1. Introduction
Fall-related accidents are a key national UK public health priority with fragility fractures estimated an annual cost of GBP 4.4 billion [
1]. Furthermore, the impact of fall-related accidents may lead to injury, pain, fear of falling, loss of independence and confidence, mobility limitations, and mortality [
2]. Age-related declines in both the sensory (vision, vestibular, and proprioception) and neuromuscular (strength, power, range of motion) systems negatively affect postural stability, which is an important factor for older adults to perform usual activities of daily life such as walking, turning, moving, and functioning independently [
3]. Impaired balance control increases the risk of falls in older adults due to the difficulty in controlling balance recovery reactions, e.g., swaying around the ankles or hips, and taking steps beyond the base of support [
4,
5]. Therefore, developing physical activity (PA) interventions to improve/maintain postural control is important not only for overall health and psychological benefits but also for daily functioning and independence [
6]. Understanding the key facilitators and barriers that older adults may face when adopting and maintaining PA is crucial when developing feasible, accessible, appropriate, affordable, and enjoyable interventions [
7], including those centred on fall prevention.
The determinants for participation in PA by older adults have been identified in the development of the social ecological model (SEM) [
7], which highlights enjoyment, sociable, affordable, accessible, and flexible as important aspects of a PA program for older adults [
7]. Additionally, the self-determination theory of human motivation supports the concept of psychological needs, autonomy competence, and enjoyment as influences on behavioural motivation for participation in PA [
8,
9]. These findings emphasise the importance of obtaining feedback on newly designed PA interventions to ensure that they meet the needs of older adults. Many PA interventions examine task-specific reactive balance, which is recommended as an optimal intervention for improving reactive balance in older adults [
5,
10]. Perturbation-based balance training aims to incorporate repeated postural perturbations to evoke instantaneous rapid balance reactions to reduce falls in older adults [
11,
12,
13] with the potential of producing quicker adaptations to improve balance compared to conventional balance training [
13]. Furthermore, perturbation-based balance training is an approach used in fall prevention with improved balance, confidence [
14], resilience, and balance reactive control to respond to real-life circumstances such as trips that occur in daily life [
15]. Such interventions are often performed in clinical settings and are not always accessible to all older adults as part of a regular exercise regime.
Muscular strength is another important factor for maintaining balance, which is recommended in PA guidelines for older adults [
16]. Strength reductions in ageing have been associated with muscle changes, leading to increased risk of falls and difficulty in performing daily tasks such as climbing stairs, rising from a chair, and household chores. The importance of muscular strength highlights the need to include strengthening exercises in PA interventions for older adults, which can be achieved using elastic band resistance [
17]. Studies documenting the use of elastic band resistance versus conventional resistance training using weight machines have shown similar improvements in strength [
18], isometric force [
19], peripheral muscle force [
17], functional exercise capacity [
20], and improvements in health-related quality of life in older adults [
19]. Elastic band resistance is a useful, cost-effective, and safe intervention in the rehabilitation of balance impairments in older adults [
21]. When used in a full-body training program, elastic band resistance has been shown to improve postural control in older adults [
22,
23], and in targeted lower limb strengthening training has been shown to influence balance, gait function, flexibility, and fall efficacy [
24]. However, the importance of involving and engaging older adults in the development of interventions that meet their needs and preferences is a critical factor for a successful PA intervention [
7,
25]. Furthermore, to our knowledge, the use of elastic band resistance to challenge balance using this methodology within the individual’s base of support (similar to that of perturbation-based balance training) has not been previously examined. Given the above, this study aimed to develop a novel PA intervention using elastic band resistance training to challenge balance and utilise the perspectives of older adults to shape an accessible, appropriate, and acceptable intervention for older adults to meet their needs.
4. Discussion
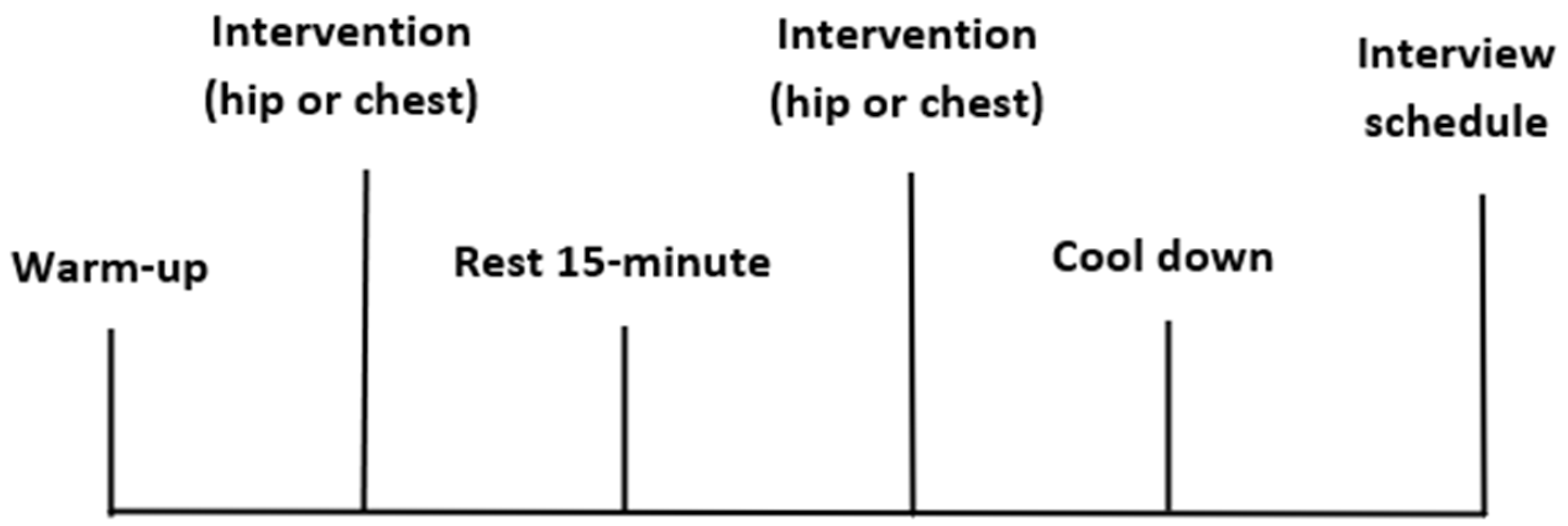
In the current study, the feasibility of a novel PA intervention using elastic band resistance at the hip and chest to challenge balance in older adults was evaluated. The study was designed to include multiple data sets to inform the design of the PA intervention by using interviews to investigate their personal preferences, difficulty, comfort, suitability, perceived benefits, safety, exercise equipment, and the environment. Additionally, quantitative data of HR and RPE were used to determine the PA intensity. These multiple data sets were combined with the feedback from older adults as a unique aspect to the study, which contributes to informing the process of designing PA interventions that are feasible for older adults [
1,
32,
33]. The benefits of involving older adults in the development of such interventions has been shown to encourage older adults to be physically active [
34].
The present study identified the feasibility of a novel elastic band resistance PA intervention and the importance of delivery to make older adults feel comfortable and safe, including a sense of enjoyment and considering the environment as well as the preferences and physical abilities of each individual. Therefore, it is important to discuss the outcomes of the study, which include considerations that may be useful for future PA interventions to meet the needs of older adults.
4.1. Perceptions of the Exercises
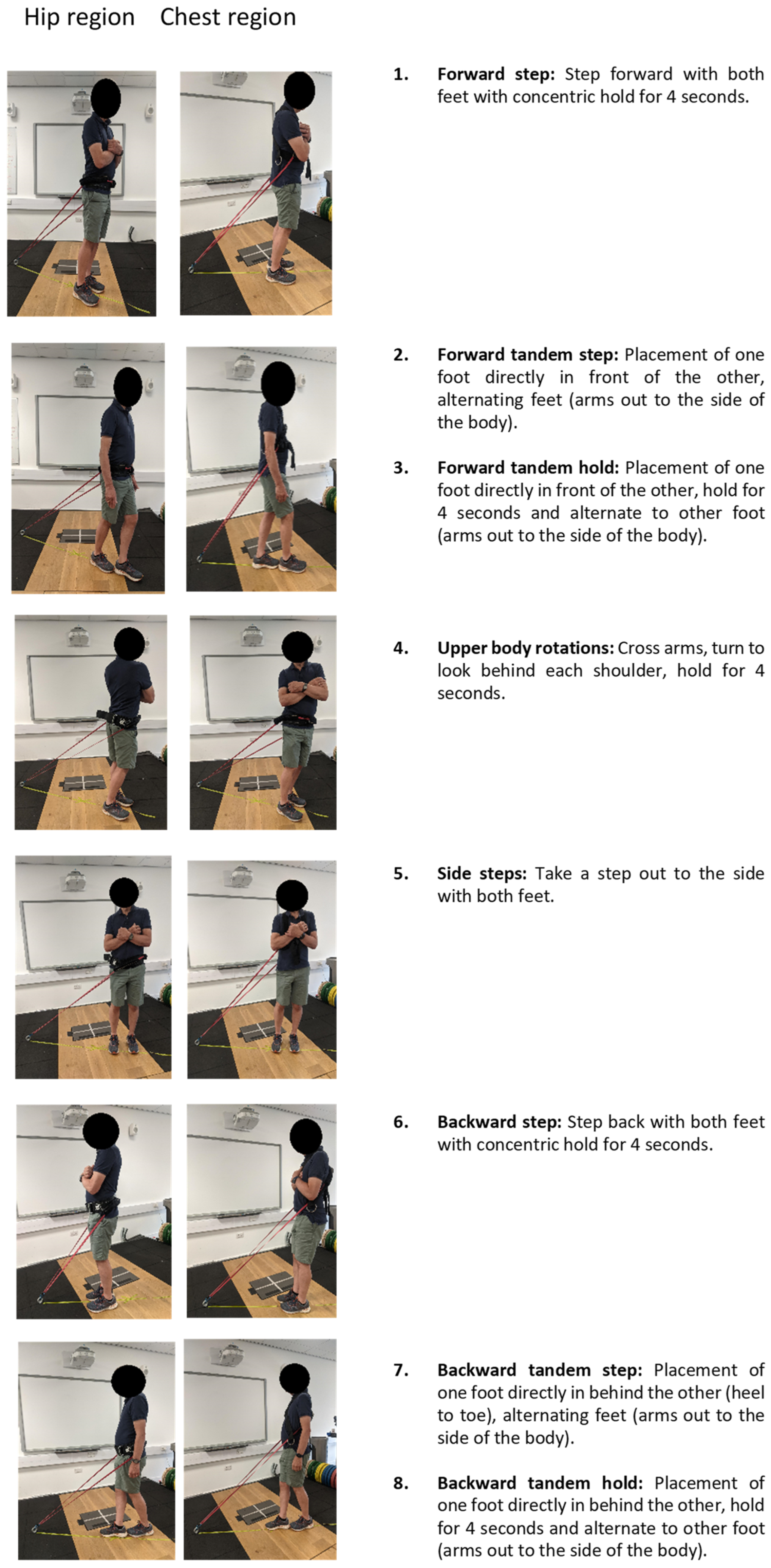
Participants varied in their perceptions of how challenging the PA intervention was regarding balance. However, exercises including the upper-body rotations and the side steps were perceived to be less challenging. These exercises were performed with a wider base of support, which is a likely explanation for the greater stability experienced, influencing participants’ perception that they insufficiently challenged balance [
35].
In terms of difficulty, participants suggested that the chest exercises were easier to perform as they could use the force of their whole body to lean against the resistance band to maintain balance, whereas hip exercises were restricted to using the force of the lower body only and were perceived to be more difficult. Furthermore, this may be due to activation of additional muscles, including those in the trunk/core area, which may provide greater benefit to balance performance compared to hip exercises [
36].
Holding the arms out to each side of the body during the tandem exercises (
Figure 1 (Images 2,3,7,8)) was perceived to increase exercise difficulty. This may be due to the additional cognitive demand of performing two tasks simultaneously, requiring greater coordination [
36]. Previous studies have highlighted an increase in perceived difficulty in dual-task exercises and a decrease in balance performance [
37,
38,
39]. Providing the option of a dual-task element in the PA intervention would therefore provide an additional challenge to increase difficulty for people who require it, allowing greater individualisation of the training prescription and potentially improving intervention effectiveness.
4.1.1. Perceptions of Age and Balance Capacity
According to the verbal feedback, participants who perceived themselves to be older also tended to view their balance as poorer (
Section 3.3.4,
Section 3.3.6). As ageing is associated with a reduction in physical function, including reduced muscle strength, coordination, and balance [
40], this is likely explained by age-related fear of falling [
41,
42].
4.1.2. Psychological and Motivational Considerations
The participants’ perception of their ability to perform the exercises was related to confidence, self-efficacy, and comfort (
Section 3.3.9), which are determinants of PA for older adults [
43]. Participants expressed that they felt less comfortable performing the exercises that most challenged balance (i.e., tandem steps, tandem holds, and performed exercises backwards ), and this likely placed increased demand on postural control and coordination due to the narrow base of support. Most participants did not report anxiousness whilst performing the exercises, possibly due to the close supervision by staff, with whom the participants were well-acquainted [
44]. Furthermore, other factors that likely contributed to participants’ confidence levels were the clear verbal instruction for how to perform the exercises and a detailed safety briefing on the PA equipment to provide everyone with the confidence to perform the exercises (
Section 3.5.1). Previous research has highlighted benefits of providing both verbal and written instructions to increase compliance and motivation regarding PA in younger adults [
44,
45], which provides a sense of security and safety during the intervention. The current intervention considered this aspect within the design with older adults and highlighted the importance of this aspect when creating PA interventions for this age group.
4.1.3. Perceptions of the Elastic Band Placement
Participants perceived the chest placement of the elastic band to provide a greater sense of security in terms of safety whilst performing the exercises compared to the hip placement. This perception may be related to the points addressed previously with the chest intervention being less challenging in terms of the balance required to perform the exercises compared to that with band placement at the hip. Sex was a factor associated with the perceived comfort of the exercise selection, with females expressing how the chest harness felt uncomfortable due to the placement of the elastic band high on the anatomical position of the chest, whereas this was not a concern for males. This suggests that the chest intervention may not be feasible, or at least less preferred, than the hip intervention for some females. Regardless, both locations of the elastic band placement (chest and hip) were reported to be challenging with regard to balance. Thus, the exercise equipment and the elastic band placement should be taken into consideration or be modified to suit individuals in future interventions.
4.1.4. Perceptions of Intervention
The personal preferences reported for the exercise selection were associated with the ability to perform the exercises, with participants preferring to perform the exercises that were less difficult and at which they therefore felt more capable and confident to perform. This ease provided participants with a greater sense of enjoyment due to being able to perform the selected exercises [
46]. The importance of enjoyment in PA is recognised as an essential aspect of engagement for older adults, which should be considered in PA interventions for older adults [
46]. Additionally, enjoyment is highlighted in the SEM as a factor that makes activities accessible and appealing [
7]. The PA interventions have the potential to provide a graded challenge to allow individuals to become proficient and efficacious in the exercises over time, which has previously been highlighted as a motivational factor, and should thus be considered for older adults [
44].
4.1.5. Perceptions of Exercise Intensity
The PA intervention was delivered at a low/moderate intensity, which can be altered to gradually increase the intensity over time to provide a continuously challenging program as the neuromuscular system adapts [
47]. The adaptability of the exercises would allow participants to progress at their own pace with the activity, which has been highlighted as an important aspect in engaging older adults in PA within the SEM [
7,
48]. Including this aspect of adaptability in PA interventions for older adults enables individuals with varying needs to participate in PA and allows older adults to exercise within the limits of their own abilities [
44].
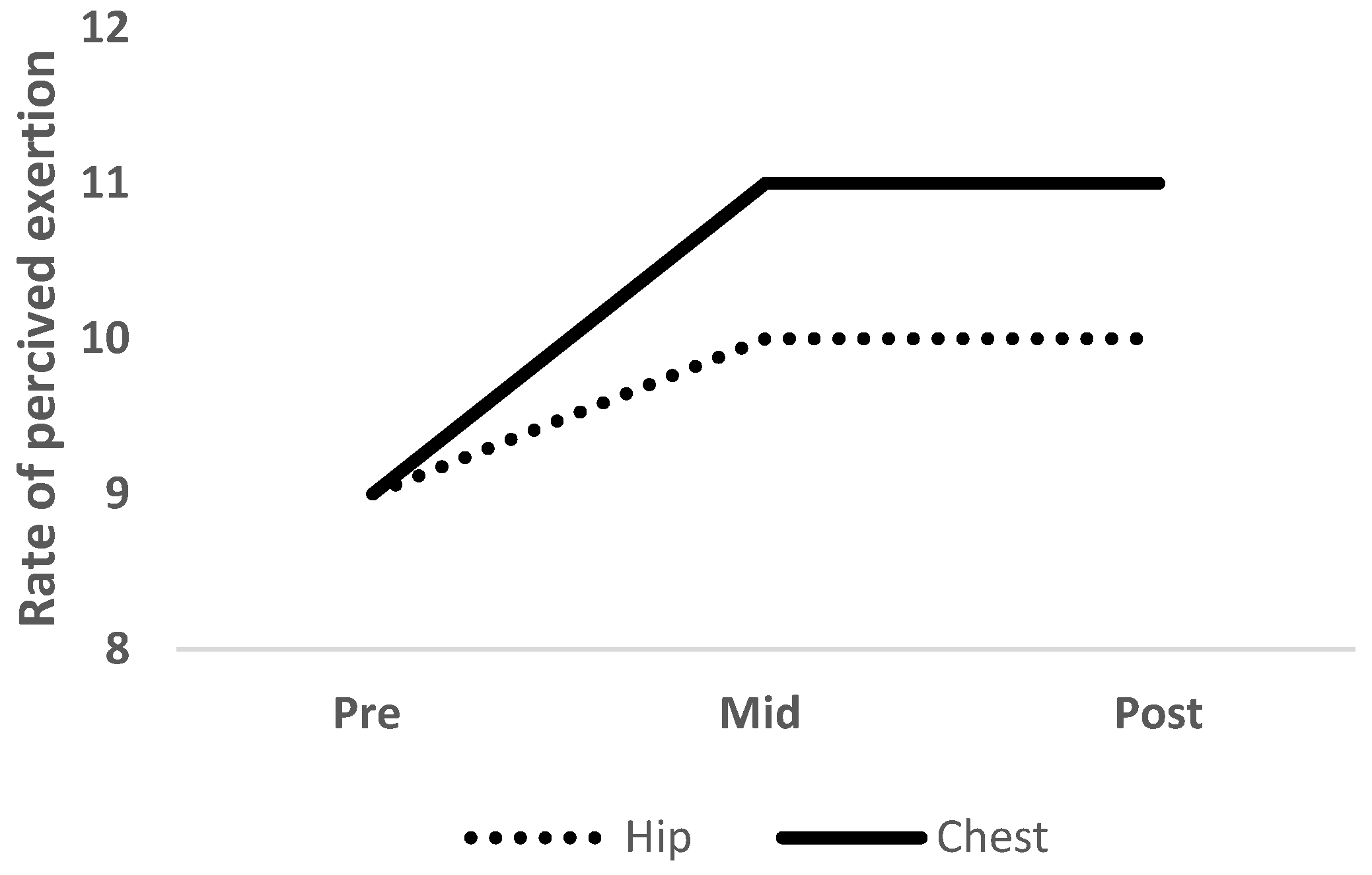
4.1.6. Exercise Intensity: Heart Rate (HR) and Perceived Exertion (RPE)
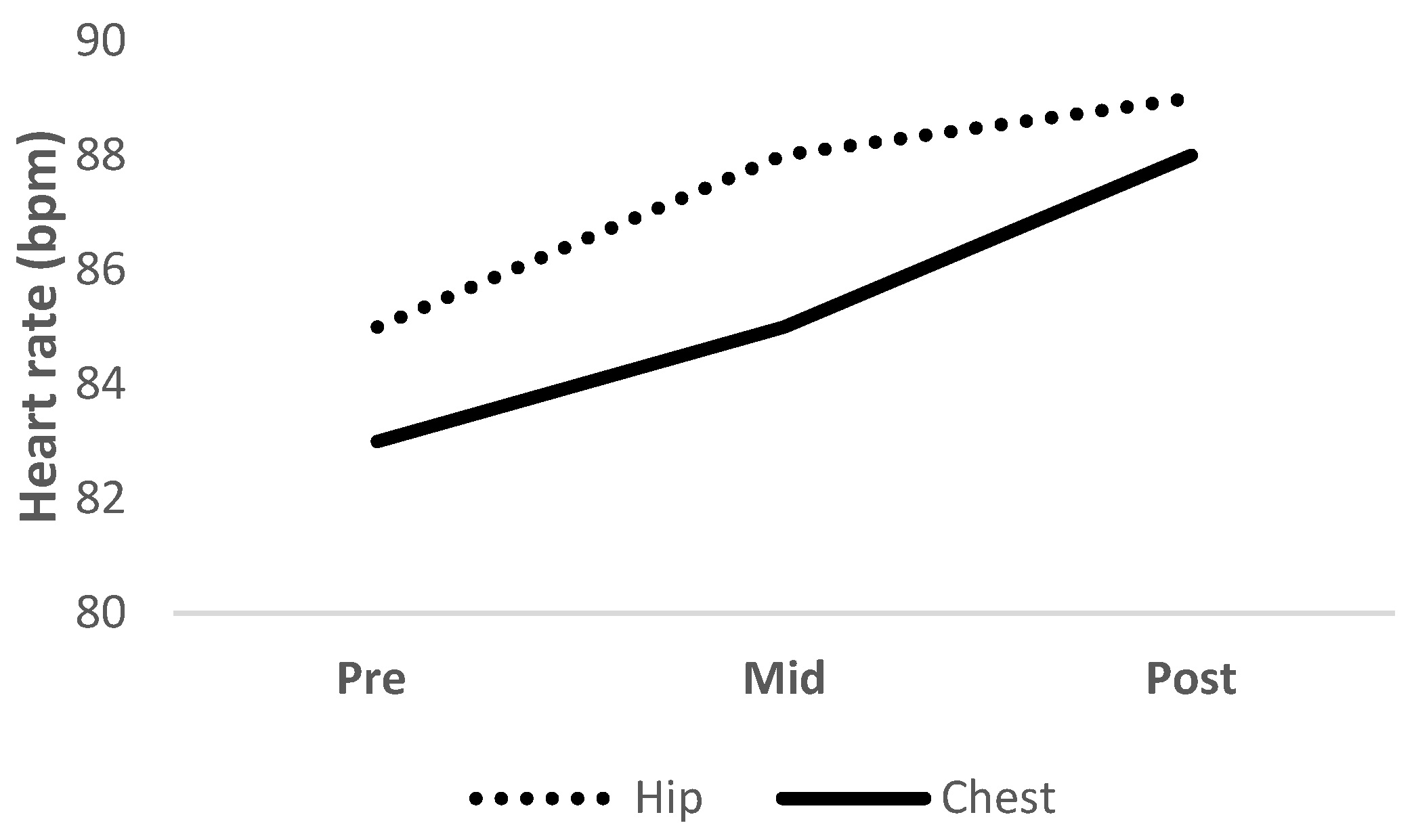
Heart rate and RPE measures indicated that the intensity of the PA intervention increased to a low-to-moderate level. Although moderate-to-vigorous levels of PA are recommended in the PA guidelines for older adults [
16], the physical and mental health benefits of increasing sedentary levels of PA may be overlooked. The importance of providing older adults with the confidence to engage in PA to be more active is essential to promote behaviour changes and leads to increased PA levels over time [
44,
45]. The current PA interventions can be tailored for varying physical abilities and can be modified to increase the difficulty and therefore intensity of the exercises over time to meet individual needs.
4.1.7. Reflection on Aspects of Socialisation
Within this study, all participants reported a positive experience from engaging in the PA. A contributing factor was the social interaction aspect, which emerged as a general theme (
Section 3.5.2). The interaction with the researchers/supervisors was a facilitator of engagement in the intervention. The importance of the social element has previously been identified in the self-determination theory [
10,
11] as a facilitator that motivates behaviour, which may promote behaviour change in PA engagement [
49]. A prominent theme was that the group setting/supervision was the preferred environment of participants to engage and perform the PA intervention, which is consistent with previous research indicating the importance of the social aspect in providing participants with motivation, enjoyment, and social interaction. Other studies have shown that theses aspects are important factors to be considered in PA interventions to make them appealing and engaging for older adults [
50]. The SEM demonstrates the importance of this social element in activities as an essential motivator for older adults to adhere to PA [
7]. Furthermore, as this research was conducted during COVID-19 restrictions, group contact may have been a concern. However, some of the participants wanted the group contact, which may explain the personal preference for a preferred group setting [
27]. As older adults may be at high risk of social isolation [
51], the opportunity for social engagement is an important aspect to be considered in PA interventions to influence relationships and improve social connectedness to provide a positive experience [
52]. Future considerations of a group setting for the current PA interventions would be advantageous to make the intervention accessible for older adults [
7,
53].
4.1.8. Organisation and Tailoring
The opinion about the exercise organisation in terms of the sets and repetitions varied for each participant. This was likely a result of each participants’ previous experience of PA [
44]. This further enhances the importance of individual tailoring and meeting individual needs, which has previously been stated to be a safe and effective approach to improving physical outcomes in older adults [
54,
55]. The perceived suitability of the intervention was considered to ensure that the intervention was suitable for older adults. Participants revealed that they felt the intervention was suitable for themselves and others in their age group as they were aware of the deterioration of balance control in ageing. The participants in the older age group (65–84 years) reported perceived benefits of performing the exercises, associated with their own abilities to perform the exercises. However, participants in the younger age bracket (50–64 years) thought that the exercises would be beneficial at a later age when their balance control would be decreased, although at this age (50–64 years), this could possibly be considered as too late. Providing the opportunity for an early preventative PA intervention in middle-aged adults to improve and maintain balance performance may be key to delaying declines in daily functioning and falls later in life [
56,
57].
Importantly, the opinions and ideas of older adults have contributed to shaping the design of the intervention. This included ways in which the equipment can be altered to provide comfort and ways to progress the intervention to make it more challenging, such as incorporating weights, incorporating the exercises in a multicomponent intervention, and increasing the resistance of the elastic band to further challenge balance. The inclusion of progressively challenging balancing exercises is essential in such interventions as the body’s sensory systems are highly adaptive [
58]. Modifications should be considered to suit individual preferences in PA interventions for older adults, for example, by altering the resistance of the elastic band and having participants stand out further from the anchor point to increase the resistance and instability and therefore make the exercises progressively more challenging to improve and adapt balance control strategies [
59]. The practice of postural control strategies helps to improve and challenge balance, supporting the ideology of the PA intervention [
35].
4.2. Strengths and Limitations
An important strength of the present study is that it provided rich information about the perceptions of the PA design of older adults and utilised the participants’ perceptions/feedback to shape the intervention. This is useful for directing future PA interventions for older adults to make them accessible, enjoyable, and appropriate. Further, the present study shares the process of how to undertake this research, involving older adults in the development of shaping and designing interventions to meet their needs, as called for in the literature [
7]. This will be helpful for other stakeholders seeking to identify the preferences for the exercise section, safety, social, and enjoyment factors. These research findings will be disseminated to older adults and the providers of services for older adults through local PA networks in Derbyshire and the East Midlands (UK). Furthermore, whilst this study evaluated the perceptions of older adults, participants’ balance performances were not measured directly using a balance performance measure. This research was conducted during COVID-19 restrictions with safety precautions, although the recruitment to the study was limited to those individuals who felt confident in the university setting during this time.
5. Conclusions
In this study, the insights, opinions, and preferences regarding the novel elastic band resistance PA protocol provided valuable information for designing and shaping future PA interventions suitable for older adults. The importance of including security, safety, and the option of regressions and progressions in PA tailored to individual needs/abilities should be considered within such interventions. The enjoyment, socialisation, and perceived benefits of performing PA are important aspects and motivating factors in older adults’ decision to engage in PA. Given the outcomes, it would suggest that the PA intervention is feasible and appropriate for older adults to perform at a low-to-moderate exercise intensity. Ongoing efforts to involve and include older adults in the intervention design to meet the needs and preferences of older adults are of significance to enable PA interventions to be successful. This study contributes to the development of a novel PA intervention using elastic band resistance training to challenge balance and utilised the perspectives of older adults in shaping an accessible, appropriate, and acceptable intervention to meet their needs. Furthermore, the current intervention has the potential to improve balance in older adults and therefore prevent falls and mitigate fall occurrences, although further research is required to identify the effects on balance and postural sway patterns to confirm the efficacy of the program in mitigating common fall risk characteristics.

 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}