
Impact of Different Isokinetic Movement Patterns on Shoulder Rehabilitation Outcome


 and
and
Abstract
:1. Introduction
2. Materials and Methods:
2.1. Study Design
2.2. Study Participants
2.3. Dash Questionnaire
2.4. BTE-Settings
2.5. Statistical Analysis
3. Results
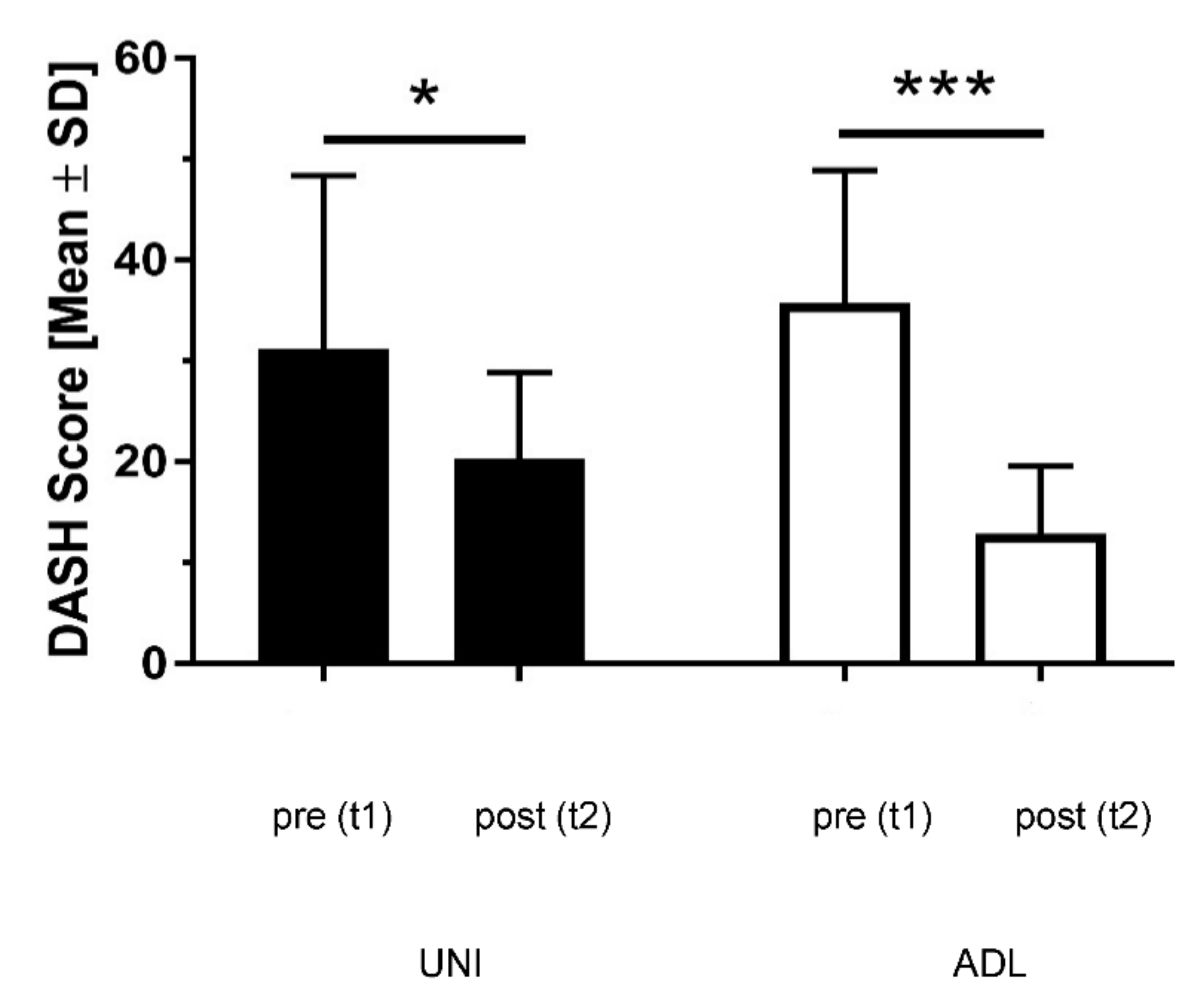
3.1. DASH Results
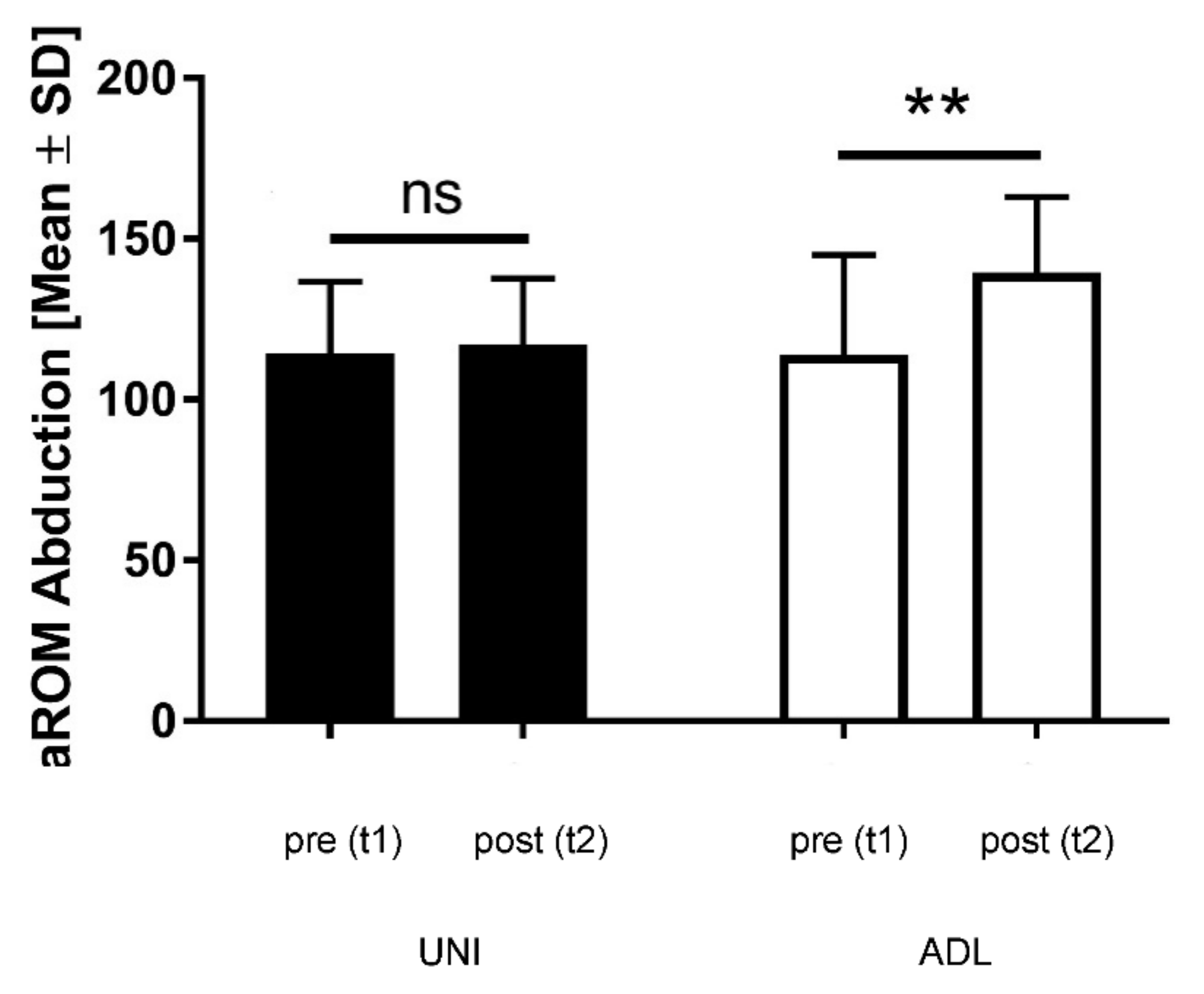
3.2. Results Active Range of Motion (aROM)
3.3. Pain (NPRS) Results
3.4. Results Grip Strength
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ingwersen, K.G.; Christensen, R.; Sørensen, L.; Jørgensen, H.R.; Jensen, S.L.; Rasmussen, S.; Søgaard, K.; Juul-Kristensen, B. Progressive high-load strength training compared with general low-load exercises in patients with rotator cuff tendinopathy: Study protocol for a randomised controlled trial. Trials 2015, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.L.; Fu, B.M.; Ngai, G.; Yung, P. Effect of isokinetic training on shoulder impingement. Genet. Mol. Res. 2014, 13, 744–757. [Google Scholar] [CrossRef] [PubMed]
- Von der Heyde, R.L. Occupational therapy interventions for shoulder conditions: A systematic review. Am. J. Occup. Ther. 2011, 65, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Walker, C.R.; Belisario, J.C.Y.; Vasudevan, J.M. Suprascapular Neuropathy in Collegiate Tennis Player: A Case Report. Cureus 2021, 13, e20824. [Google Scholar] [CrossRef]
- Chua, M.M.J.; Hayes, M.T.; Cosgrove, R. Parsonage-Turner syndrome following COVID-19 vaccination and review of the literature. Surg. Neurol. Int. 2022, 13, 152. [Google Scholar] [CrossRef]
- Brown, R.; O’Callaghan, J.; Peter, N. Parsonage Turner syndrome caused by Staphylococcus aureus spondylodiscitis. BMJ Case Rep. 2020, 13, e233073. [Google Scholar] [CrossRef]
- Maselli, F.; Storari, L.; Lorusso, M.; Mourad, F.; Pennella, D.; Barbari, V.; Salomon, M.; Brindisino, F. Osteoid Osteoma in an Adult Wheelchair Basketball Player Mimicking Musculoskeletal Shoulder Pain: Red Flag or a Red Herring? Tomography 2022, 8, 389–401. [Google Scholar] [CrossRef]
- Alotaibi, A.A.; Albaqami, F.S.; Almushayqih, A.K.; Alotaibi, G.N.; Aldakkan, N.F.; Muammar, J.M.; Alsulaimani, A.A.; Alrowathi, K.I.; Almansour, A.A.; Alrushud, S.S.; et al. Large Pleural Lipoma Manifesting with Chronic Shoulder Pain. Cureus 2022, 14, e21113. [Google Scholar]
- Wang, J.; Zhao, B.; Song, T.; Sun, J. Lung cancer combined with diffuse peritoneal and mesenteric amyloidosis detected on 18F-FDG PET/CT: A case report. Medicine 2021, 100, e25961. [Google Scholar] [CrossRef]
- Mohamud, S.; Oyawusi, M.; Weir, R.L.; Halbert, E.O.; Millis, R.M.; Gebremedhin, T.; Dehkordi, O. Pancoast tumor presenting with multiple joint pains: A case report. J. Med. Case Rep. 2022, 16, 109. [Google Scholar] [CrossRef]
- Izuka, S.; Komai, T.; Natsumoto, B.; Shoda, H.; Fujio, K. Self-limited Polymyalgia Rheumatica-like Syndrome Following mRNA-1273 SARS-CoV-2 Vaccination. Intern. Med. 2022, 61, 903–906. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liu, J.; Wang, X.; Liu, X.; Sun, Q.; Du, Y.; Yin, L. Bilateral vertebral artery dissection complicated by posterior circulation stroke in a young man: A case report. Medicine 2020, 99, e22822. [Google Scholar] [CrossRef] [PubMed]
- Kuo, F.Y.; Chen, K.L.; Yen, C.C. Idiopathic humeral head osteonecrosis mimicking rotator cuff disorders: Two challenging diagnostic case reports. Medicine 2020, 99, e18766. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Borchgrevink, P.C.; Allen, S.M.; Rosseland, L.A.; Romundstad, L.; Hals, E.K.; Kvarstein, G.; Stubhaug, A. Assessment of pain. Br. J. Anaesth. 2008, 101, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of four pain intensity rating scales. Pain 2011, 152, 2399–2404. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Grip Strength: An Indispensable Biomarker For Older Adults. Review. Clin. Interv. Aging 2019, 14, 1681–1691. [Google Scholar] [CrossRef]
- Steiber, N. Strong or Weak Handgrip? Normative Reference Values for the German Population across the Life Course Stratified by Sex, Age, and Body Height. PLoS ONE 2016, 11, e0163917. [Google Scholar] [CrossRef]
- Willems, S.M.; Wright, D.J.; Day, F.R.; Trajanoska, K.; Joshi, P.K.; Morris, J.A.; Matteini, A.M.; Garton, F.C.; Grarup, N.; Oskolkov, N.; et al. Large-scale GWAS identifies multiple loci for hand grip strength providing biological insights into muscular fitness. Nat. Commun. 2017, 8, 16015. [Google Scholar] [CrossRef]
- Manickaraj, N.; Bisset, L.M.; Kavanagh, J.J. Lateral epicondylalgia exhibits adaptive muscle activation strategies based on wrist posture and levels of grip force: A case-control study. J. Musculoskelet. Neuronal Interact. 2018, 18, 323–332. [Google Scholar]
- Beumer, A.; Lindau, T.R. Grip strength ratio: A grip strength measurement that correlates well with DASH score in different hand/wrist conditions. BMC Musculoskelet. Disord. 2014, 15, 336. [Google Scholar] [CrossRef] [PubMed]
- Cronin, J.; Lawton, T.; Harris, N.; Kilding, A.; McMaster, D.T. A brief review of handgrip strength and sport performance. J. Strength Cond. Res. 2017, 31, 3187–3217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nussbaumer, S.; Leunig, M.; Glatthorn, J.F.; Stauffacher, S.; Gerber, H.; Maffiuletti, N.A. Validity and test-retest reliability of manual goniometers for measuring passive hip range of motion in femoroacetabular impingement patients. BMC Musculoskelet. Disord. 2010, 11, 194. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.G.; Kim, E.K. Test-retest reliability of an active range of motion test for the shoulder and hip joints by unskilled examiners using a manual goniometer. J. Phys. Ther. Sci. 2016, 28, 722–724. [Google Scholar] [CrossRef] [PubMed]
- Hayes, K.; Walton, J.R.; Szomor, Z.L.; Murrell, G.A. Reliability of five methods for assessing shoulder range of motion. Aust. J. Physiother. 2001, 47, 289–294. [Google Scholar] [CrossRef]
- Kolber, M.J.; Hanney, W.J. The reliability and concurrent validity of shoulder mobility measurements using a digital inclinometer and goniometer: A technical report. Int. J. Sports Phys. Ther. 2012, 7, 306–313. [Google Scholar]
- Gajdosik, R.L.; Bohannon, R.W. Clinical measurement of range of motion: Review of goniometry emphasizing reliability and validity. Phys. Ther. 1987, 67, 1867–1872. [Google Scholar] [CrossRef]
- Mullaney, M.J.; McHugh, M.P.; Johnson, C.P.; Tyler, T.F. Reliability of shoulder range of motion comparing a goniometer to a digital level. Physiother. Theory Pract. 2010, 26, 327–333. [Google Scholar] [CrossRef]
- Kent, B.E. Functional anatomy of the shoulder complex: A review. Phys. Ther. 1971, 51, 947. [Google Scholar] [CrossRef]
- Greenberg, D.L. Evaluation and treatment of shoulder pain. Review. Med. Clin. N. Am. 2014, 98, 487–504. [Google Scholar] [CrossRef]
- Klintberg, I.H.; Cools, A.M.; Holmgren, T.M.; Holzhausen, A.C.; Johansson, K.; Maenhout, A.G.; Moser, J.S.; Spunton, V.; Ginn, K. Consensus for physiotherapy for shoulder pain. Int. Orthop. 2015, 39, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Marik, T.L.; Roll, S.C. Effectiveness of Occupational Therapy Interventions for Musculoskeletal Shoulder Conditions: A Systematic Review. Am. J. Occup. Ther. 2017, 71, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Levanon, Y. The advantages and disadvantages of using high technology in hand rehabilitation. J. Hand Ther. 2013, 26, 179–183. [Google Scholar] [CrossRef]
- Raven, E.E.; Haverkamp, D.; Sierevelt, I.N.; van Montfoort, D.O.; Pöll, R.G.; Blankevoort, L.; Tak, P.P. Construct validity and reliability of the disability of arm, shoulder and hand questionnaire for upper extremity complaints in rheumatoid arthritis. J. Rheumatol. 2008, 35, 2334–2338. [Google Scholar] [CrossRef] [PubMed]
- Hudak, P.L.; Amadio, P.C.; Bombardier, C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder, and head) [corrected]. Am. J. Ind. Med. 1996, 29, 602–608. [Google Scholar] [CrossRef]
- Franchignoni, F.; Vercelli, S.; Giordano, A.; Sartorio, F.; Bravini, E.; Ferriero, G. Minimal clinically important difference of the disabilities of the arm, shoulder and hand outcome measure (DASH) and its shortened version (QuickDASH). J. Orthop. Sports Phys. Ther. 2014, 44, 30–39. [Google Scholar] [CrossRef]
- Gummesson, C.; Atroshi, I.; Ekdahl, C. The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: Longitudinal construct validity and measuring self-rated health change after surgery. BMC Musculoskelet. Disord. 2003, 4, 11. [Google Scholar] [CrossRef]
- Beaton, D.E.; Katz, J.N.; Fossel, A.H.; Wright, J.G.; Tarasuk, V.; Bombardier, C. Measuring the whole or the parts? Validity, reliability, and responsiveness of the Disabilities of the Arm, Shoulder and Hand outcome measure in different regions of the upper extremity. J. Hand Ther. 2001, 14, 128–146. [Google Scholar] [CrossRef]
- Kennedy, L.E.; Bhambhani, Y.N. The Baltimore Therapeutic Equipment Work Simulator: Reliability and validity at three work intensities. Arch. Phys. Med. Rehabil. 1991, 72, 511–516. [Google Scholar]
- Bhambhani, Y.; Esmail, S.; Brintnell, S. The Baltimore Therapeutic Equipment work simulator: Biomechanical and physiological norms for three attachments in healthy men. Am. J. Occup. Ther. 1994, 48, 19–25. [Google Scholar] [CrossRef]
- Ting, W.; Wessel, J.; Brintnell, S.; Maikala, R.; Bhambhani, Y. Validity of the baltimore therapeutic equipment work simulator in the measurement of lifting endurance in healthy men. Am. J. Occup. Ther. 2001, 55, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Kibler, W.B.; Ludewig, P.M.; McClure, P.W.; Michener, L.A.; Bak, K.; Sciascia, A.D. Clinical implications of scapular dyskinesis in shoulder injury: The 2013 consensus statement from the ‘Scapular Summit’. Br. J. Sports Med. 2013, 47, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Cools, A.M.; Dewitte, V.; Lanszweert, F.; Notebaert, D.; Roets, A.; Soetens, B.; Cagnie, B.; Witvrouw, E.E. Rehabilitation of scapular muscle balance: Which exercises to prescribe? Am. J. Sports Med. 2007, 35, 1744–1751. [Google Scholar] [CrossRef]
- Lefèvre-Colau, M.M.; Nguyen, C.; Palazzo, C.; Srour, F.; Paris, G.; Vuillemin, V.; Poiraudeau, S.; Roby-Brami, A.; Roren, A. Kinematic patterns in normal and degenerative shoulders. Part II: Review of 3-D scapular kinematic patterns in patients with shoulder pain, and clinical implications. Ann. Phys. Rehabil. Med. 2018, 61, 46–53. [Google Scholar] [CrossRef]
- Ashton, M.L.; Savage-Elliott, I.; Granruth, C.; Michael, J.; O’Brien, M.J. What Are We Measuring? A Systematic Review of Outcome Measurements Used in Shoulder Surgery. Arthrosc. Sports Med. Rehabil. 2020, 2, e429–e434. [Google Scholar] [CrossRef] [PubMed]
- Riebel, M.; Crowell, M.; Dolbeer, J.; Szymanek, E.; Goss, D. Correlation of self-reported outcome measures and the selective functional movement assessment (SFMA): An exploration of validity. Int. J. Sports Phys. Ther. 2017, 12, 931–947. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Chung, S.W.; Lee, S.J.; Lee, J.W.; Oh, K.S. Evaluation of the Electromyographic Amplitude-to-Work Ratio in the Infraspinatus Muscle During External Shoulder Rotation Exercises: A Comparison of Concentric Isotonic and Isokinetic Exercises. Orthop. J. Sports Med. 2020, 8, 2325967120932459. [Google Scholar] [CrossRef] [PubMed]
- Ratamess, N.A.; Beller, N.A.; Gonzalez, A.M.; Spatz, G.E.; Hoffman, J.R.; Ross, R.E.; Faigenbaum, A.D.; Kang, J. The Effects of Multiple-Joint Isokinetic Resistance Training on Maximal Isokinetic and Dynamic Muscle Strength and Local Muscular Endurance. J. Sports Sci. Med. 2016, 15, 34–40. [Google Scholar]
- Bélaise, C.; Michaud, B.; Boucher, M.; Begon, M. Do relevant shear forces appear in isokinetic shoulder testing to be implemented in biomechanical models? J. Biomech. 2018, 2, 241–246. [Google Scholar] [CrossRef]
- Wilk, K.E.; Macrina, L.C. Nonoperative and postoperative rehabilitation for injuries of the throwing shoulder. Sports Med. Arthrosc. 2014, 22, 137–150. [Google Scholar] [CrossRef]
- Zinke, F.; Warnke, T.; Gäbler, M.; Granacher, U. Effects of Isokinetic Training on Trunk Muscle Fitness and Body Composition in World-Class Canoe Sprinters. Front. Physiol. 2019, 10, 21. [Google Scholar] [CrossRef] [PubMed]
- Moeller, C.R.; Bliven, K.C.; Valier, A.R. Scapular muscle-activation ratios in patients with shoulder injuries during functional shoulder exercises. J. Athl. Train. 2014, 49, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Michener, L.A.; Snyder, A.R.; Leggin, B.G. Responsiveness of the numeric pain rating scale in patients with shoulder pain and the effect of surgical status. J. Sport Rehabil. 2020, 20, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Stien, N.; Pedersen, H.; Ravnøy, A.H.; Andersen, V.; Saeterbakken, A.H. Training specificity performing single-joint vs. multi-joint resistance exercises among physically active females: A randomized controlled trial. PLoS ONE 2020, 15, e0233540. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable (SD, Median) | UNI-Group (n = 9) | ADL-Group (n = 10) | Total (n = 19) | |||
|---|---|---|---|---|---|---|
| Male (%) | 11 | 40 | 26 | |||
| Female (%) | 89 | 60 | 74 | |||
| BMI | 26.6 | (±5.1, 27.0) | 31.9 | (±5.4, 32.7) | 29.39 | (±5.9, 28.5) |
| Age | 57.6 | (±5.9, 57.0) | 54.3 | (±9.5, 54.4) | 55.1 | (±8.1, 55.0) |
| DASH | 31.2 | (±2.2, 30.0) | 35.8 | (±1.9, 35.8) | 33.6 | (±2.4, 34.1) |
| NPRS at rest | 1.8 | (±2.5, 3.5) | 2.6 | (±1.6, 2.0) | 2.2 | (±1.2, 3.0) |
| NPRS in movement | 5.2 | (±1.9, 5.0) | 7.3 | (±2.0, 7.5) | 6.3 | (±2.1, 7.0) |
| HGS (N × 10) | 29.7 | (±12.1, 25.8) | 20.9 | (±8.3, 21.0) | 25.5 | (±11.36, 22.6) |
| RGHS | 1.10 | (±0.4, 1.0) | 0.65 | (±8.3, 0.4) | 0.89 | (±11.3, 0.9) |
| aROM abduction (degrees) | 114.4 | (±21.1, 120) | 114.0 | (±29.3, 105.0) | 114.2 | (±25.8, 110.0) |
| DASH | NPRS Move | Handgrip | aROM Abduction | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Group | UNI | ADL | UNI | ADL | UNI | ADL | UNI | ADL | |
| DASH | r | 1.000 | 1.000 | 0.551 | 0.555 | 0.286 | −0.567 | −0.775 | 0.211 |
| p | - | - | 0.124 | 0.096 | 0.456 | 0.087 | 0.014 * | 0.559 | |
| NPRS move | r | 1.000 | 1.000 | 0.790 | −0.611 | −0.470 | −0.133 | ||
| p | - | - | 0.011 * | 0.061 | 0.201 | 0.714 | |||
| Hand grip | r | 1.000 | 1.000 | −0.462 | −0.238 | ||||
| p | - | - | 0.210 | 0.507 | |||||
| aROM abduction | r | 1.000 | 1.000 | ||||||
| p | - | - | |||||||
| Pain in Either Group. | Beginning of Rehabilitation (t1) | End of Rehabilitation (t2) | Relative Change (t1 − t2) | Significance of Change (p) | |
|---|---|---|---|---|---|
| NPRS at rest | |||||
| UNI-group | Mean (SD) | 1.78 (2.49) | 1.11 (1.27) | −0.67 (2.50) | 0.447 |
| Median (IQR) | 0.0 (3.5) | 1.0 (2.5) | 0.0 (4.0) | ||
| ADL-group | Mean (SD) | 2.60 (1.58) | 0.90 (1.29) | −1.70 (1.34) | 0.003 ** |
| Median (IQR) | 2.0 (2.3) | 0.5 (1.3) | −1.5 (2.3) | ||
| NPRS in movement | |||||
| UNI-group | Mean (SD) | 5.22 (1.92) | 4.11 (2.57) | −1.11 (2.37) | 0.197 |
| Median (IQR) | 5.0 (3.5) | 4.0 (4.0) | 0.0 (4.5) | ||
| ADL-group | Mean (SD) | 7.30 (2.00) | 3.60 (2.55) | −3.70 (2.00) | 0.000 *** |
| Media (IQR)n | 7.5 (2.8) | 3.0 (4.3) | −4.5 (3.5) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Missmann, M.; Gollner, K.; Schroll, A.; Pirchl, M.; Grote, V.; Fischer, M.J. Impact of Different Isokinetic Movement Patterns on Shoulder Rehabilitation Outcome. Int. J. Environ. Res. Public Health 2022, 19, 10623. https://doi.org/10.3390/ijerph191710623
Missmann M, Gollner K, Schroll A, Pirchl M, Grote V, Fischer MJ. Impact of Different Isokinetic Movement Patterns on Shoulder Rehabilitation Outcome. International Journal of Environmental Research and Public Health. 2022; 19(17):10623. https://doi.org/10.3390/ijerph191710623
Chicago/Turabian StyleMissmann, Martin, Katrin Gollner, Andrea Schroll, Michael Pirchl, Vincent Grote, and Michael J. Fischer. 2022. "Impact of Different Isokinetic Movement Patterns on Shoulder Rehabilitation Outcome" International Journal of Environmental Research and Public Health 19, no. 17: 10623. https://doi.org/10.3390/ijerph191710623