
The Level of Fear in the Polish Police Population during the COVID-19 Pandemic with the Impact of Sociodemographic Variables

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Background
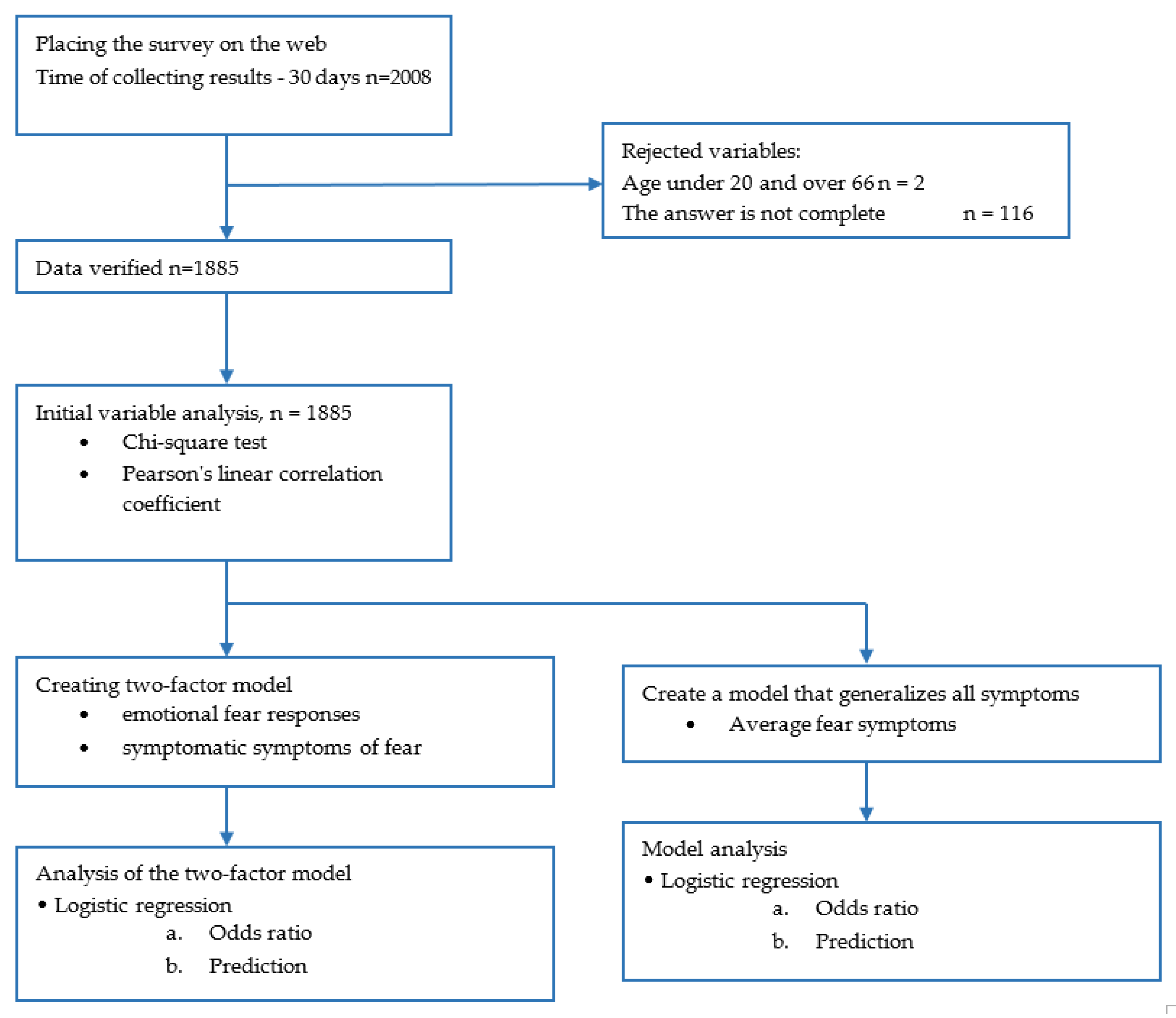
3. Materials and Methods
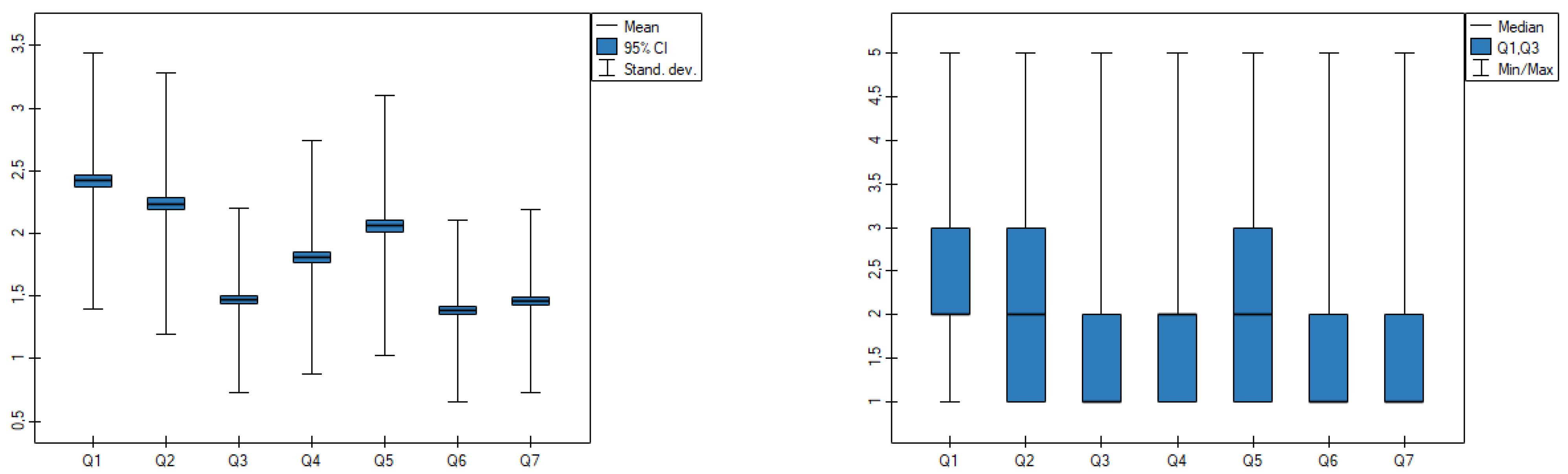
- I am afraid of the coronavirus (COVID-19) more than anything else;
- Thinking about the coronavirus (COVID-19) makes me uncomfortable;
- My palms sweat when I think about the coronavirus (COVID-19);
- I am worried that I will die from the coronavirus infection (COVID-19);
- When I hear about the coronavirus (COVID-19) in the media and on the Internet, I become nervous and worried;
- I cannot sleep because of the coronavirus (COVID-19);
- My heart starts to beat faster when I think about the coronavirus (COVID-19).
- Confidence level (α): 95%;
- Sample size (n): 1887;
- Proportion percentage (p): 50;
- Population size (N): 96,132.
4. Results
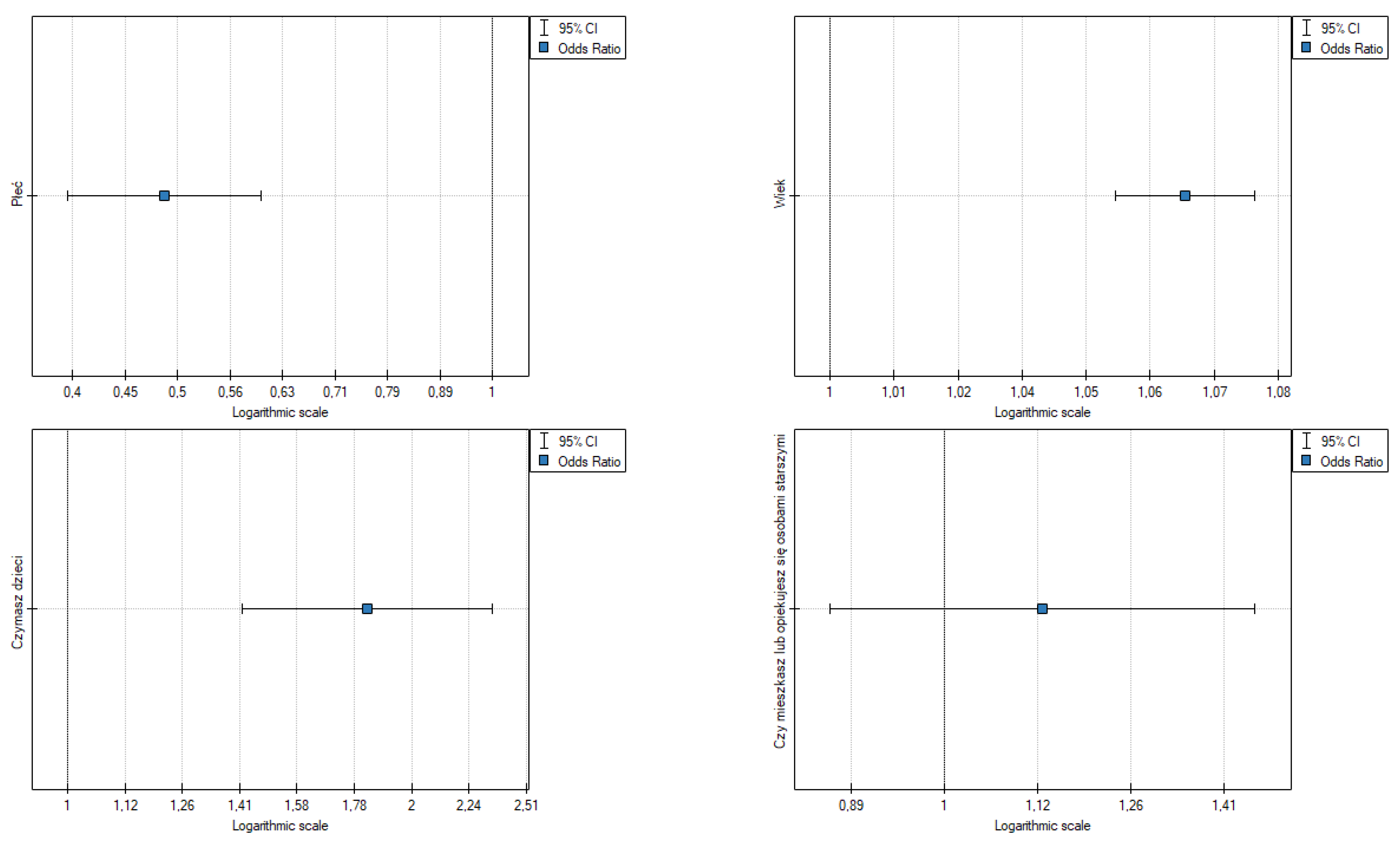
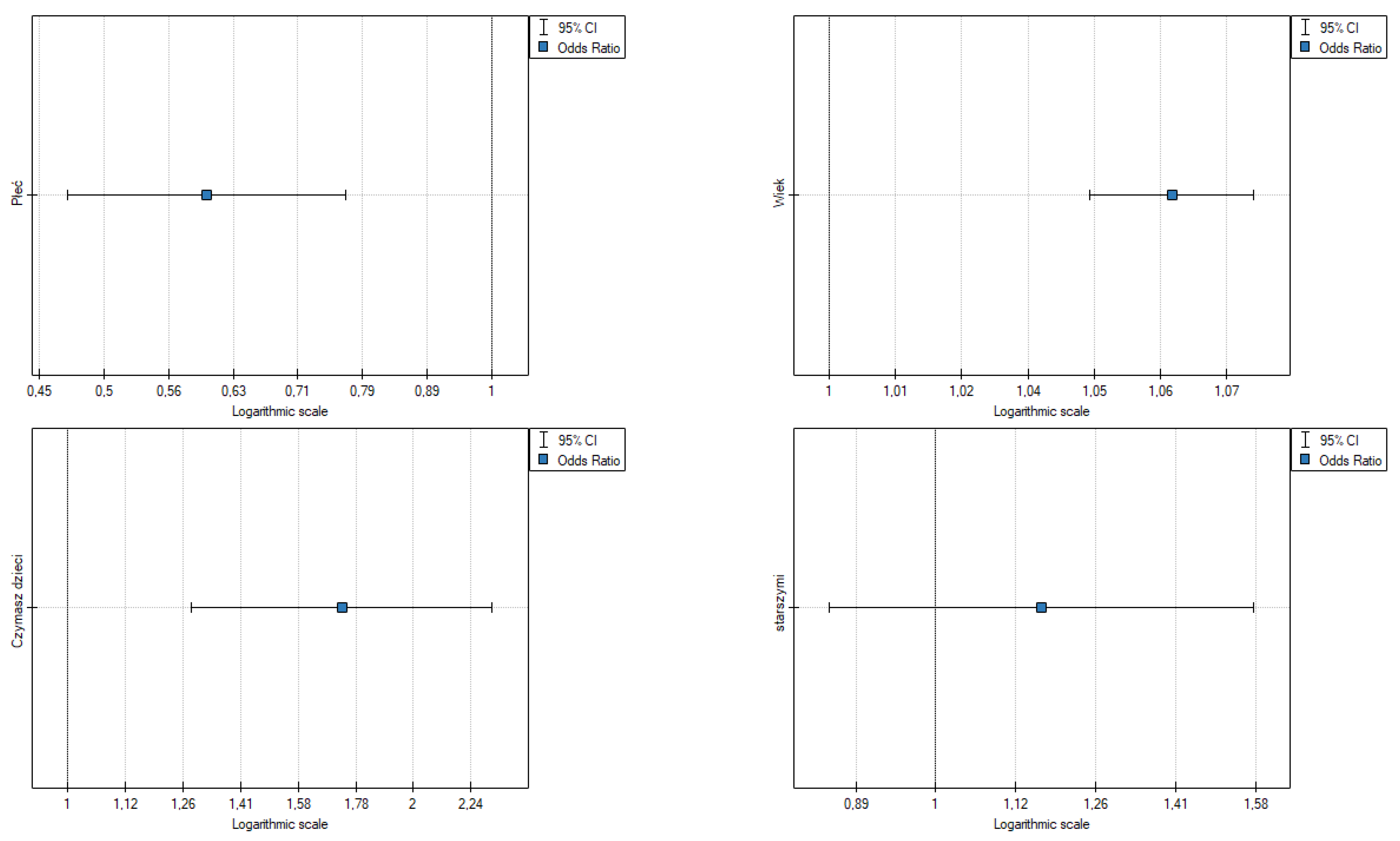
- Gender: OR [95%] = 0.49 [0.393942; 0.602288], p = 0.000, the odds of mental (emotional) symptoms in a woman are 0.5 fold higher than in a man;
- Age: OR [95%] = 1.07 [1.052602; 1.079336], p = 0.000, the odds of mental (emotional) symptoms are slightly higher in older people;
- Having children: OR [95%] = 1.83 [1.419435; 2.346546], p = 0.000, the odds of mental (emotional) symptoms in a person with children is 1.83 fold higher than in people without children;
- Caring for the elderly is not statistically significant.
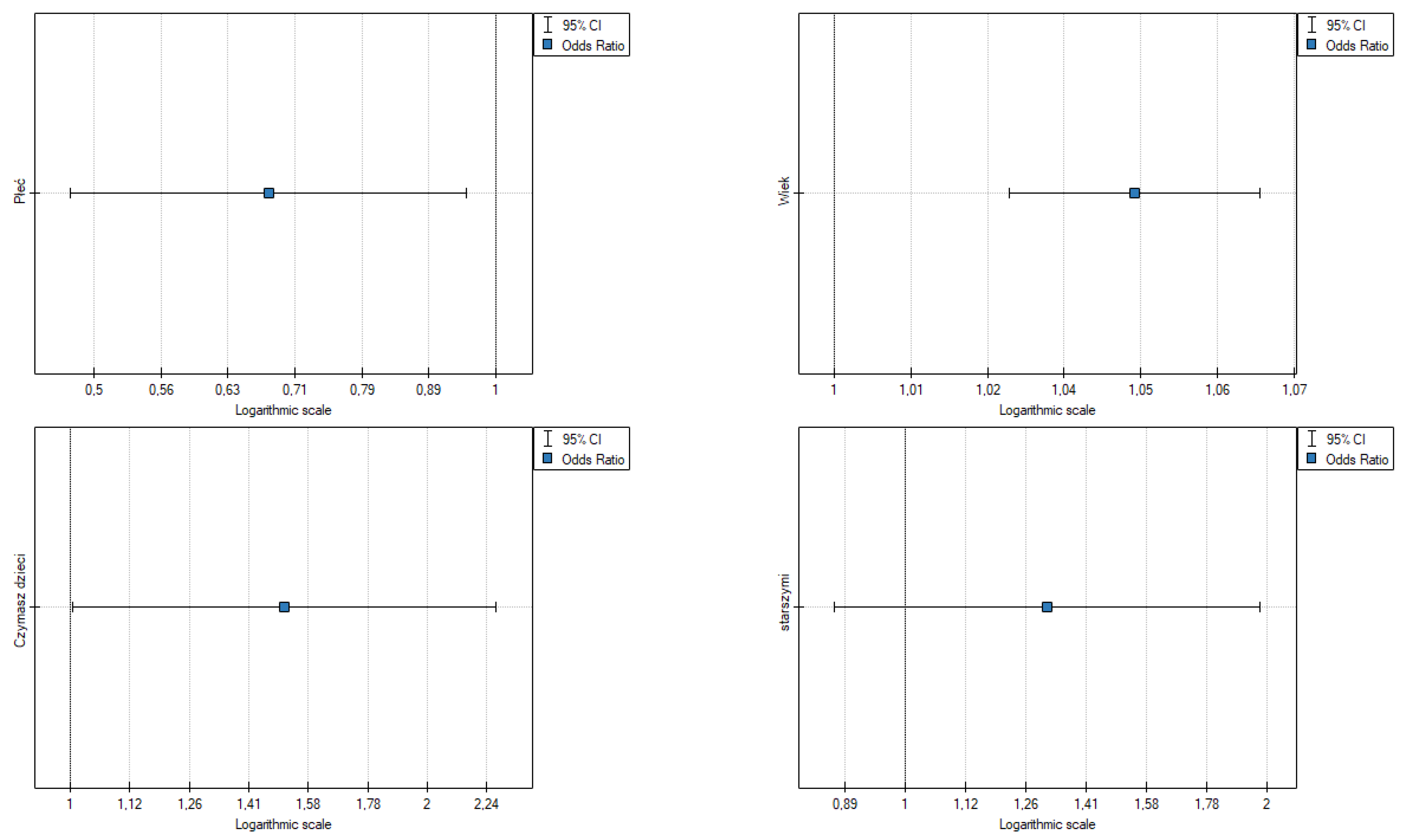
- Gender: OR [95%] = 0.68 [0.481045; 0.950956], p = 0.024, the odds of somatic symptoms in a woman are higher than in a man;
- Age: OR [95%] = 1.05 [1.026699; 1.066078], p = 0.000, the odds of somatic symptoms are slightly higher in older people;
- Having children: OR [95%] = 1.51 [1.004557; 2.277944], p = 0.048, the odds of somatic symptoms in a person with children is 1.53 fold higher than in those without children;
- Caring for the elderly is not statistically significant.
- Gender: OR [95%] = 0.60 [0.469761; 0.770796], p = 0.000, the odds of developing symptoms are slightly higher in older people;
- Age: OR [95%] = 1.06 [1.046349; 1.076548], p = 0.000, the odds of symptoms are slightly higher in older people;
- Having children: OR [95%] = 1.73 [1.280751; 2.333964], p = 0.000, the odds of having emotional symptoms in a person with children is 1.73 fold higher than in people without children;
- Caring for the elderly is not statistically significant.
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartley, T.A.; Burchfiel, C.M.; Fekedulegn, D.; Andrew, M.E.; Violanti, J.M. Health disparities in police officers: Comparisons to the U.S. general population. Int. J. Emerg. Ment. Health 2011, 13, 211. [Google Scholar]
- Mccraty, R.; Atkinson, M. Resilience Training Program Reduces Physiological and Psychological Stress in Police Officers. Glob. Adv. Health Med. 2012, 1, 44–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paoline, E.A. Taking stock: Toward a richer understanding of police culture. J. Crim. Justice 2003, 31, 199–214. [Google Scholar] [CrossRef]
- Terrill, W.; Paoline, E.A.; Manning, P.K. Police culture and coercion. Criminology 2003, 41, 1003–1034. [Google Scholar] [CrossRef]
- Mohler, G.; Bertozzi, A.L.; Carter, J.; Short, M.B.; Sledge, D.; Tita, G.E.; Uchida, C.D.; Brantingham, P.J. Impact of social distancing during COVID-19 pandemic on crime in Los Angeles and Indianapolis. J. Crim. Justice 2020, 68, 101692. [Google Scholar] [CrossRef]
- Campedelli, G.M.; Aziani, A.; Favarin, S. Exploring the effect of 2019-nCoV containment policies on crime: The case of los Angeles. arXiv 2020, arXiv:2003.11021. [Google Scholar]
- ABC. 2020. ABC News. Available online: https://abc7ny.com/nypd-coronavirus-deaths-nyc-news/6065991/ (accessed on 30 October 2021).
- Available online: https://isp.policja.pl/isp/aktualnosci/15846,Podsumowujemy-2020-rok-w-Policji.html (accessed on 30 October 2021).
- U.S. Department of Health and Human Services, Individual Resilience. Public Health and Medical Emergency Support for a National Prepared. Available online: http://www.phe.gov/Preparedness/planning/abc/Pages/individualresilience.aspx,2015 (accessed on 4 October 2020).
- Lewis-Schroeder, N.F.; Kieran, K.; Murphy, B.L.; Wolff, J.D.; Robinson, M.A.; Kaufman, M.L. Conceptualization, Assessment, and Treatment of Traumatic Stress in First Responders: A Review of Critical Issues. Harv. Rev. Psychiatry 2018, 26, 216–227. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 20, 1537–1545. [Google Scholar] [CrossRef] [Green Version]
- Wakashima, K.; Asai, K.; Kobayashi, D.; Koiwa, K.; Kamoshida, S.; Sakuraba, M. The Japanese version of the Fear of COVID-19 scale: Reliability, validity, and relation to coping behavior. PLoS ONE 2020, 15, e0241958. [Google Scholar] [CrossRef]
- Soraci, P.; Ferrari, A.; Abbiati, F.A.; Del Fante, E.; De Pace, R.; Urso, A.; Griffiths, M.D. Validation and Psychometric Evaluation of the Italian Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 4, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Lorca, M.; Martínez-Lorca, A.; Criado-Álvarez, J.J.; Armesilla, M.D.C.; Latorre, J.M. The fear of COVID-19 scale: Validation in spanish university students. Psychiatry Res. 2020, 293, 113350. [Google Scholar] [CrossRef] [PubMed]
- Alyami, M.; Henning, M.; Krägeloh, C.U.; Alyami, H. Psychometric Evaluation of the Arabic Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 19, 2219–2232. [Google Scholar] [CrossRef]
- Sakib, N.; Bhuiyan, A.K.M.I.; Hossain, S.; Al Mamun, F.; Hosen, I.; Abdullah, A.H.; Sarker, A.; Mohiuddin, M.S.; Rayhan, I.; Hossain, M.; et al. Psychometric Validation of the Bangla Fear of COVID-19 Scale: Confirmatory Factor Analysis and Rasch Analysis. Int. J. Ment. Health Addict. 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Pilch, I.; Kurasz, Z.; Turska-Kawa, A. Experiencing fear during the pandemic: Validation of the fear of COVID-19 scale in Polish. PeerJ 2021, 9, e11263. [Google Scholar] [CrossRef]
- Available online: www.dane.publiczne.pl (accessed on 30 October 2021).
- Available online: https://goodcalculators.com/margin-of-error-calculator/ (accessed on 30 October 2021).
- Taigman, M.; Liebowitz, S. Super-Charge Your Stress Management in the Age of COVID-19; Vow3 Publishing: Montecito, CA, USA, 2020. [Google Scholar]
- Lilly, M.; Curry, S. Mental Health Training and Intervention: A Critical Component of Police Reform; Ed Praetorian on Scribd: San Francisco, CA, USA, 2020. [Google Scholar]
- Nguyen, H.T.; Do, B.N.; Pham, K.M.; Kim, G.B.; Dam, H.T.B.; Nguyen, T.T.; Nguyen, T.T.P.; Nguyen, Y.H.; Sørensen, K.; Pleasant, A.; et al. Fear of COVID-19 Scale—Associations of Its Scores with Health Literacy and Health-Related Behaviors among Medical Students. Int. J. Environ. Res. Public Health 2020, 17, 4164. [Google Scholar] [CrossRef]
- Chen, R.-N.; Liang, S.-W.; Peng, Y.; Li, X.-G.; Chen, J.-B.; Tang, S.-Y.; Zhao, J.-B. Mental health status and change in living rhythms among college students in China during the COVID-19 pandemic: A large-scale survey. J. Psychosom. Res. 2020, 137, 110219. [Google Scholar] [CrossRef]
- Reznik, A.; Gritsenko, V.; Konstantinov, V.; Khamenka, N.; Isralowitz, R. COVID-19 Fear in Eastern Europe: Validation of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 19, 1903–1908. [Google Scholar] [CrossRef] [PubMed]
- Frenkel, M.O.; Giessing, L.; Egger-Lampl, S.; Hutter, V.; Oudejans, R.R.; Kleygrewe, L.; Jaspaert, E.; Plessner, H. The impact of the COVID-19 pandemic on European police officers: Stress, demands, and coping resources. J. Crim. Justice 2021, 72, 101756. [Google Scholar] [CrossRef] [PubMed]
- Stogner, J.; Miller, B.L.; McLean, K. Police stress, mental health, and resiliency during the COVID-19 pandemic. Am. J. Crim. Justice 2020, 45, 718–730. [Google Scholar] [CrossRef] [PubMed]
- Bowler, R.M.; Han, H.; Gocheva, V.; Nakagawa, S.; Alper, H.; DiGrande, L.; Cone, J.E. Gender differences in probable posttraumatic stress disorder among police responders to the 2001 world trade center terrorist attack. Am. J. Ind. Med. 2010, 53, 1186–1196. [Google Scholar] [CrossRef]
- Violanti, J.M.; Fekedulegn, D.; Hartley, T.A.; Charles, L.E.; Andrew, M.E.; Ma, C.C.; Burchfiel, C.M. Highly rated and most frequent stressors among police officers: Gender differences. Am. J. Crim. Justice 2016, 41, 645–662. [Google Scholar] [CrossRef] [Green Version]
- Landman, A.; Nieuwenhuys, A.; Oudejans, R.R.D. Decision-related action orientation predicts police officers’ shooting performance under pressure. Anxiety Stress Coping 2016, 29, 570–579. [Google Scholar] [CrossRef]
- Gray, J. Dlaczego Mars Zderza Się z Wenus; Dom Wydawniczy REBIS: Poznań, Poland, 2010; pp. 62–64. [Google Scholar]
- Drake, G.; Altheimer, I. Officer Wellness during a Global Pandemic: Long Term Recommendations for Police Leaders as They Navigate the Aftermath of COVID-19; Center for Public Safety Initiatives: New York, NY, USA, 2020. [Google Scholar]
- Patterson, G.T.; Chung, I.W.; Swan, P.W. Stress management interventions for police officers and recruits: A meta-analysis. J. Exp. Criminol. 2012, 10, 487–513. [Google Scholar] [CrossRef]
- Asghar, Z.B.; Wankhade, P.; Bell, F.; Sanderson, K.; Hird, K.; Phung, V.H.; Siriwardena, A.N. Trends, variations and prediction of staff sickness absence rates among NHS ambulance services in England: A time series study. BMJ Open 2021, 11, e053885. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cronbach’s Alpha/Split-Half | |
|---|---|
| Analyzed variables | Q1; Q2; Q3; Q4; Q5; Q6; Q7 |
| Significance level | 0.05 |
| Group size | 1885 |
| Number of items | 7 |
| Mean of scale | 12.84191 |
| Standard deviation of scale | 4.872629 |
| Cronbach’s alpha for scale | 0.88701 |
| −95% CI for Cronbach’s alpha for scale | 0.879043 |
| +95% CI for Cronbach’s alpha for scale | 0.894633 |
| Standard error of measurement | 1.637888 |
| Average correlation between pairs of items | 0.539206 |
| Standardized Cronbach’s alpha | 0.8912 |
| Demographics | Group | N (%)/Min, Max, Mean |
|---|---|---|
| Gender | Woman Man | 643 (34.1%) 1242 (65.9%) |
| Age (in years) | Min 20, max 66, mean 38.75 | |
| Do you have children? | No | 528 (28%) |
| Yes | 1357 (72%) | |
| Do you live with any elderly persons or are you taking care of them? | No | 1540 (81.7%) |
| Yes | 345 (18.3%) |
| Fear Symptoms | Group | Frequency n | Percent (%) | Mean | Std. Deviation |
|---|---|---|---|---|---|
| I am afraid of the coronavirus (COVID-19) more than anything else | 1 | 350 | 18.6 | 2.42 | 1.02 |
| 2 | 745 | 39.5 | |||
| 3 | 486 | 25.8 | |||
| 4 | 256 | 13.6 | |||
| 5 | 48 | 2.5 | |||
| Thinking about the coronavirus (COVID-19) makes me uncomfortable | 1 | 511 | 27.1 | 2.24 | 1.05 |
| 2 | 722 | 38.3 | |||
| 3 | 384 | 20.4 | |||
| 4 | 229 | 12.1 | |||
| 5 | 39 | 2.1 | |||
| My palms sweat when I think about the coronavirus (COVID-19) | 1 | 1228 | 65.1 | 1.47 | 0.74 |
| 2 | 475 | 25.2 | |||
| 3 | 145 | 7.7 | |||
| 4 | 30 | 1.6 | |||
| 5 | 7 | 0.4 | |||
| I am worried that I will die from the coronavirus (COVID-19) infection | 1 | 851 | 45.1 | 1.81 | 0.93 |
| 2 | 682 | 36.2 | |||
| 3 | 238 | 12.6 | |||
| 4 | 82 | 4.4 | |||
| 5 | 32 | 1.7 | |||
| When I hear about the coronavirus (COVID-19) in the media and on the internet, I become nervous and worried | 1 | 645 | 34.2 | 2.06 | 1.04 |
| 2 | 755 | 40.1 | |||
| 3 | 250 | 13.3 | |||
| 4 | 193 | 10.2 | |||
| 5 | 42 | 2.2 | |||
| I cannot sleep because of the coronavirus (COVID-19) | 1 | 1366 | 72.5 | 1.38 | 0.73 |
| 2 | 370 | 19.6 | |||
| 3 | 111 | 5.9 | |||
| 4 | 21 | 1.1 | |||
| 5 | 17 | 0.9 | |||
| My heart starts to beat faster when I think about the coronavirus (COVID-19) | 1 | 1237 | 65.6 | 1.46 | 0.74 |
| 2 | 484 | 25.7 | |||
| 3 | 121 | 6.4 | |||
| 4 | 36 | 1.9 | |||
| 5 | 7 | 0.3 |
| Fear Symptoms | Gender | AGE | Having Children | Taking Care of the Elderly |
|---|---|---|---|---|
| I am afraid of the coronavirus (COVID-19) more than anything else | 0.00 | Pearson Correlation R = 0.28 Sig. = 0.00 | 0.00 | 0.018 |
| Thinking about the coronavirus (COVID-19) makes me uncomfortable | 0.00 | Pearson Correlation R = 0.27 Sig. = 0.00 | 0.00 | 0.261 |
| My palms sweat when I think about the coronavirus (COVID-19) | 0.009 | Pearson Correlation R = 0.10 Sig. = 0.00 | 0.114 | 0.614 |
| I am worried that I will die from the coronavirus infection (COVID-19) | 0.00 | Pearson Correlation R = 0.23 Sig. = 0.00 | 0.00 | 0.692 |
| When I hear about the coronavirus (COVID-19) in the media and on the Internet, I become nervous and worried | 0.00 | Pearson Correlation R = 0.27 Sig. = 0.00 | 0.00 | 0.226 |
| I cannot sleep because of the coronavirus (COVID-19) | 0.022 | Pearson Correlation R = 0.15 Sig. = 0.00 | 0.00 | 0.726 |
| My heart starts to beat faster when I think about the coronavirus (COVID-19) | 0.004 | Pearson Correlation R = 0.17 Sig. = 0.00 | 0.003 | 0.099 |
| b Coeff. | b Error | −95% CI | +95% CI | Wald Stat. | p-Value | Odds Ratio | −95% CI | +95% CI | |
|---|---|---|---|---|---|---|---|---|---|
| intercept | 0.099904 | 0.179553 | −0.252014 | 0.451822 | 0.309586 | 0.577934 | 1.105065 | 0.777234 | 1.571173 |
| Gender | −0.719285 | 0.108301 | −0.931551 | −0.50702 | 44.110373 | <0.000001 | 0.4871 | 0.393942 | 0.602288 |
| intercept | −3.609458 | 0.267063 | −4.132891 | −3.086024 | 182.665665 | <0.000001 | 0.027067 | 0.016036 | 0.045683 |
| Age | 0.063806 | 0.006398 | 0.051265 | 0.076346 | 99.450684 | <0.000001 | 1.065885 | 1.052602 | 1.079336 |
| intercept | −2.118462 | 0.234419 | −2.577916 | −1.659009 | 81.668484 | <0.000001 | 0.120216 | 0.075932 | 0.190328 |
| Do you have children | 0.601602 | 0.128238 | 0.350259 | 0.852944 | 22.00805 | 0.000003 | 1.825039 | 1.419435 | 2.346546 |
| intercept | −1.208915 | 0.168249 | −1.538677 | −0.879152 | 51.627992 | <0.000001 | 0.298521 | 0.214665 | 0.415135 |
| Do you take care of the elderly | 0.120665 | 0.134059 | −0.142084 | 0.383415 | 0.810172 | 0.36807 | 1.128247 | 0.867548 | 1.467287 |
| b Coeff. | b Error | −95% CI | +95% CI | Wald Stat. | p-Value | Odds Ratio | −95% CI | +95% CI | |
|---|---|---|---|---|---|---|---|---|---|
| intercept | −1.828853 | 0.288128 | −2.393573 | −1.264132 | 40.289059 | <0.000001 | 0.160598 | 0.091303 | 0.282484 |
| Gender | −0.391041 | 0.173857 | −0.731794 | −0.050288 | 5.058962 | 0.024499 | 0.676352 | 0.481045 | 0.950956 |
| intercept | −4.2796 | 0.409519 | −5.082243 | −3.476957 | 109.208735 | <0.000001 | 0.013848 | 0.006206 | 0.030901 |
| Age | 0.045168 | 0.009602 | 0.026349 | 0.063987 | 22.129007 | 0.000003 | 1.046203 | 1.026699 | 1.066078 |
| intercept | −3.188513 | 0.382667 | −3.938526 | −2.438499 | 69.427962 | <0.000001 | 0.041233 | 0.019477 | 0.087292 |
| Do you have children | 0.41391 | 0.208863 | 0.004547 | 0.823273 | 3.927266 | 0.047509 | 1.512721 | 1.004557 | 2.277944 |
| intercept | −2.787494 | 0.266642 | −3.310103 | −2.264886 | 109.287868 | <0.000001 | 0.061575 | 0.036512 | 0.103842 |
| Taking care of the elderly | 0.270499 | 0.207137 | −0.135481 | 0.67648 | 1.705372 | 0.191587 | 1.310619 | 0.873296 | 1.966941 |
| b Coeff. | b Error | −95% CI | +95% CI | Wald Stat. | p-Value | Odds Ratio | −95% CI | +95% CI | |
|---|---|---|---|---|---|---|---|---|---|
| intercept | −0.798624 | 0.20925 | −1.208747 | −0.388501 | 14.566407 | 0.000135 | 0.449948 | 0.298571 | 0.678073 |
| Gender | −0.507932 | 0.126329 | −0.755532 | −0.260332 | 16.166097 | 0.000058 | 0.601739 | 0.469761 | 0.770796 |
| intercept | −4.017329 | 0.308811 | −4.622588 | −3.412071 | 169.234628 | <0.000001 | 0.018001 | 0.009827 | 0.032973 |
| Age | 0.059533 | 0.007258 | 0.045307 | 0.073759 | 67.272773 | <0.000001 | 1.061341 | 1.046349 | 1.076548 |
| intercept | −2.582963 | 0.281145 | −3.133996 | −2.031929 | 84.406639 | <0.000001 | 0.07555 | 0.043543 | 0.131082 |
| Do you have children | 0.547507 | 0.153095 | 0.247447 | 0.847568 | 12.789624 | 0.000349 | 1.728938 | 1.280751 | 2.333964 |
| intercept | −1.802264 | 0.196581 | −2.187555 | −1.416972 | 84.052986 | <0.000001 | 0.164925 | 0.112191 | 0.242447 |
| Caring over the elderly | 0.151746 | 0.155645 | −0.153313 | 0.456804 | 0.950521 | 0.329587 | 1.163864 | 0.857861 | 1.57902 |
| Mental | b Coeff. | b Error | −95% CI | +95% CI | Wald Stat. | p-Value | Odds Ratio | −95% CI | +95% CI |
|---|---|---|---|---|---|---|---|---|---|
| intercept | −0.920283 | 0.068274 | −1.054098 | −0.786468 | 181.689736 | <0.000001 | 0.398406 | 0.348507 | 0.455451 |
| Age of group [1] | −0.749672 | 0.124751 | −0.994179 | −0.505165 | 36.112298 | <0.000001 | 0.472522 | 0.370027 | 0.603406 |
| Age of group [3] | 0.975853 | 0.180168 | 0.622729 | 1.328976 | 29.336758 | <0.000001 | 2.653428 | 1.864009 | 3.777173 |
| OR [95%] | Value of p | |
|---|---|---|
| 20 to 35 years old | 0.472522 [0.370027 0.603406] | <0.000001 |
| 36 to 50 years old | Reference | |
| Older than 50 years | 2.653428 [1.864009 3.777173] | <0.000001 |
| Somatic | b Coeff. | b Error | −95% CI | +95% CI | Wald Stat. | p-Value | Odds Ratio | −95% CI | +95% CI |
|---|---|---|---|---|---|---|---|---|---|
| intercept | −2.432581 | 0.113127 | −2.654306 | −2.210856 | 462.381609 | <0.000001 | 0.08781 | 0.070348 | 0.109607 |
| Age of group [1] | −0.406805 | 0.201623 | −0.80198 | −0.011631 | 4.070906 | 0.043628 | 0.665774 | 0.44844 | 0.988437 |
| Age of group [3] | 0.872333 | 0.247389 | 0.38746 | 1.357206 | 12.433844 | 0.000422 | 2.392487 | 1.473235 | 3.885322 |
| OR [95%] | Value of p | |
|---|---|---|
| 20 to 35 years | 0.665774 [0.44844 0.988437] | 0.043628 |
| 36 to 50 years | Reference | |
| more than 50 years | 2.392487 [1.473235 3.885322] | 0.000422 |
| Total | b Coeff. | b Error | −95% CI | +95% CI | Wald Stat. | p-Value | Odds Ratio | −95% CI | +95% CI |
|---|---|---|---|---|---|---|---|---|---|
| intercept | −1.481605 | 0.079333 | −1.637094 | −1.326115 | 348.785239 | <0.000001 | 0.227273 | 0.194545 | 0.265507 |
| Age of group [1] | −0.728607 | 0.150375 | −1.023336 | −0.433879 | 23.476787 | 0.000001 | 0.482581 | 0.359394 | 0.647991 |
| Age of group [3] | 0.788457 | 0.193762 | 0.408691 | 1.168224 | 16.558434 | 0.000047 | 2.2 | 1.504846 | 3.216275 |
| OR [95%] | Value of p | |
|---|---|---|
| 20 to 35 years old | 0.482581 [0.359394 0.647991] | 0.000001 |
| 36 to 50 years old | Reference | |
| Older than 50 years | 2.2 [1.504846 3.216275] | 0.000047 |
| Sex | Woman | Man | Woman | Woman | Woman |
|---|---|---|---|---|---|
| Age | 51 | 51 | 51 | 50 | 55 |
| Having children | Yes | Yes | No | Yes | Yes |
| Cut-off line | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 |
| Probability prediction | 0.50625 | 0.348061 | 0.494359 | 0.491134 | 0.566323 |
| Prediction Y | 1 | 0 | 0 | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szykuła-Piec, B.; Piec, R.; Zaczyński, A.; Wójtowicz, R.; Butkiewicz, S.; Rusyan, E.; Adamczyk, K.; Walecka, I.; Dmochowska, A.; Rogula-Kozłowska, W. The Level of Fear in the Polish Police Population during the COVID-19 Pandemic with the Impact of Sociodemographic Variables. Int. J. Environ. Res. Public Health 2022, 19, 9679. https://doi.org/10.3390/ijerph19159679
Szykuła-Piec B, Piec R, Zaczyński A, Wójtowicz R, Butkiewicz S, Rusyan E, Adamczyk K, Walecka I, Dmochowska A, Rogula-Kozłowska W. The Level of Fear in the Polish Police Population during the COVID-19 Pandemic with the Impact of Sociodemographic Variables. International Journal of Environmental Research and Public Health. 2022; 19(15):9679. https://doi.org/10.3390/ijerph19159679
Chicago/Turabian StyleSzykuła-Piec, Barbara, Robert Piec, Artur Zaczyński, Rafał Wójtowicz, Sławomir Butkiewicz, Ewa Rusyan, Kamil Adamczyk, Irena Walecka, Anna Dmochowska, and Wioletta Rogula-Kozłowska. 2022. "The Level of Fear in the Polish Police Population during the COVID-19 Pandemic with the Impact of Sociodemographic Variables" International Journal of Environmental Research and Public Health 19, no. 15: 9679. https://doi.org/10.3390/ijerph19159679