
How Do Patients Understand Questions about Lower Urinary Tract Symptoms? A Qualitative Study of Problems in Completing Urological Questionnaires

 ,
,
Abstract
:1. Introduction
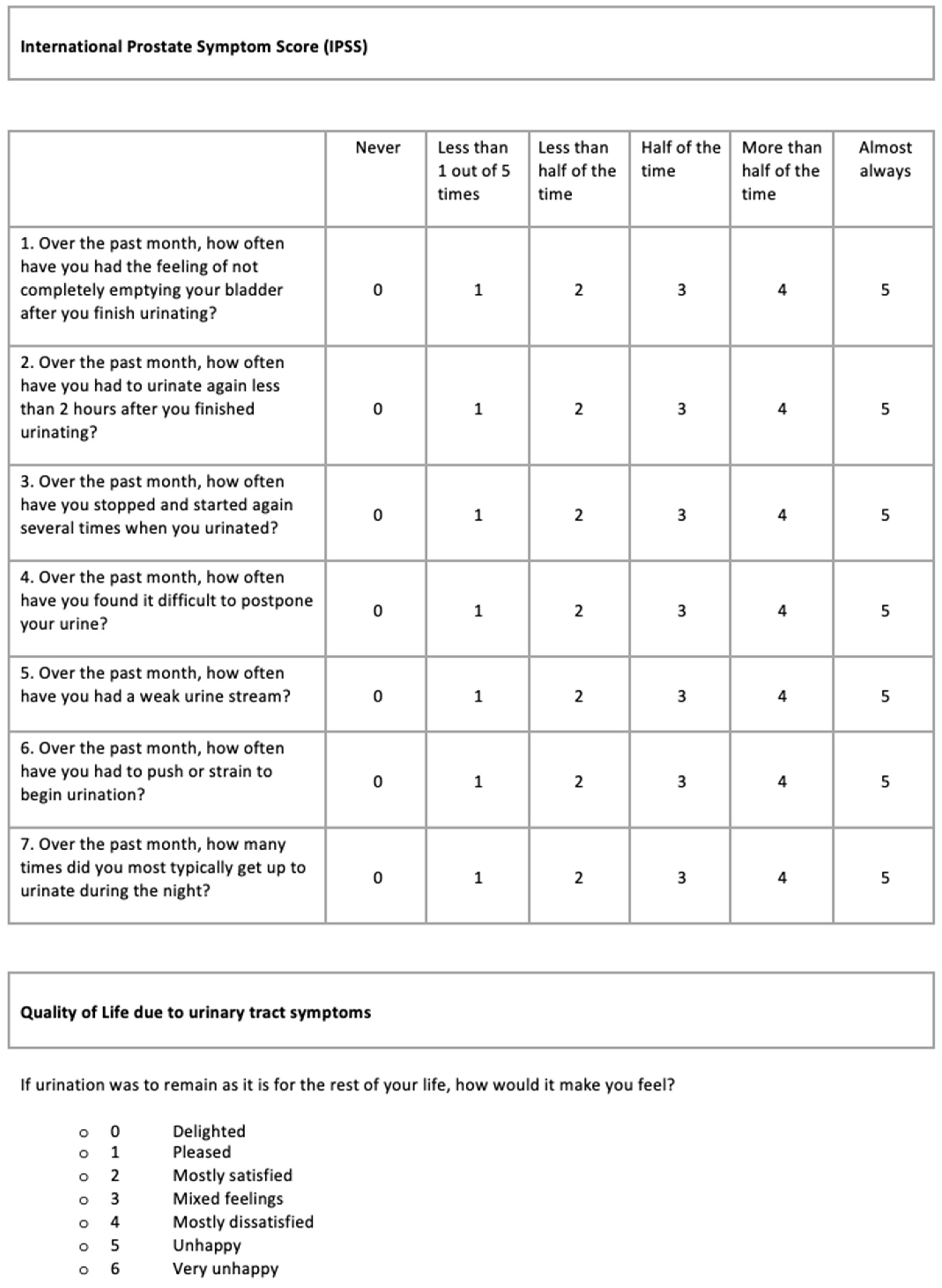
1.1. The International Prostate Symptom Score (IPSS)
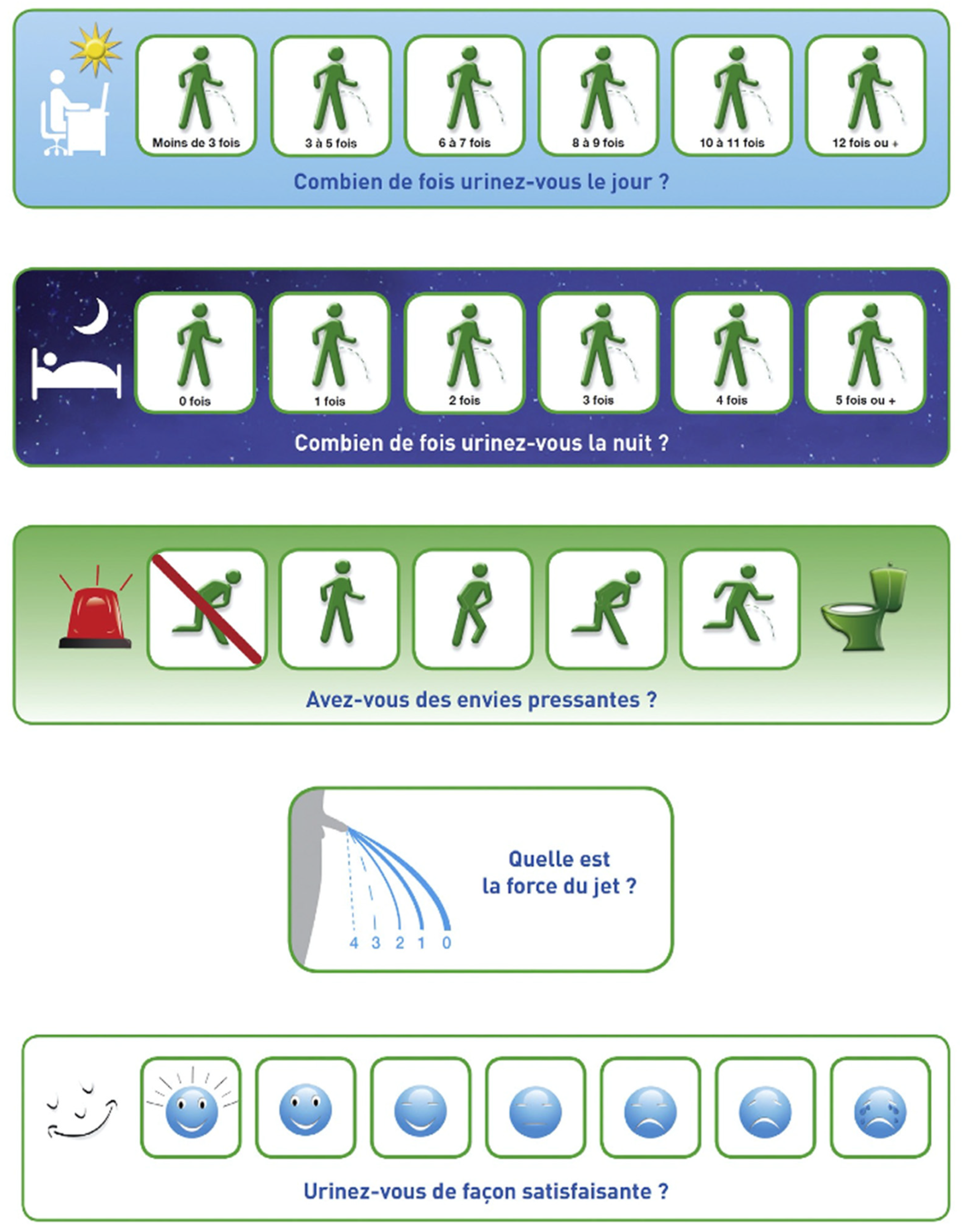
1.2. The Visual Prostate Symptom Score (VPSS)
1.3. The Score Visuel Prostatique en Image (SVPI)
1.4. Research Questions
- What kind of problems do men face when trying to complete an existing LUTS questionnaire?
- What causes can be identified for these problems?
- What is the relationship between these problems and the causes thereof on the one hand, and the level of health literacy of the participants on the other hand?
2. Materials and Methods
2.1. Design
2.2. Participants and Setting
2.3. Procedure
- What did you think of the questionnaire?
- Is the layout of the questionnaire clear, and if not, what could be improved?
- Is the questionnaire more difficult or easier compared to other forms you are familiar with?
- Did you miss any general information, such as an introduction at the top of the questionnaire?
- How did you experience this test?
- Should you have completed this questionnaire for yourself at home, would you have proceeded in the same way as you have done now?
2.4. LUTS Questionnaires
2.5. Working-Aloud Method
2.5.1. Techniques
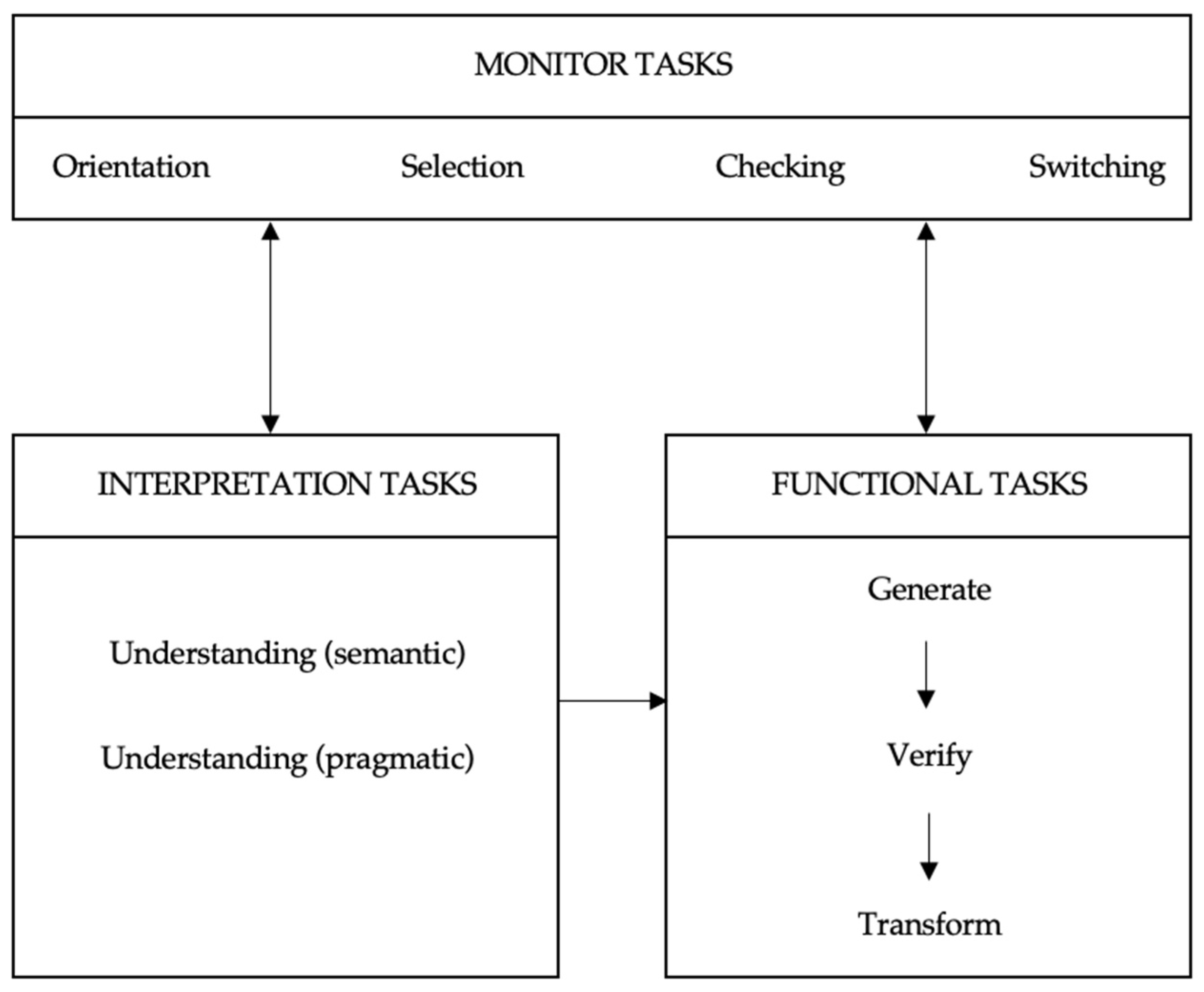
2.5.2. Task Analysis
- generating data: producing the requested information;
- verifying: checking whether an item of information fits into a particular category;
- transforming: converting an item of information into a code, such as a graphic sign (check a box, for instance).
- orientation: obtaining an overview of the document and its various parts, and of the overall task and the various steps that it comprises;
- selection: deciding which functional tasks and which interpretation tasks should or should not be carried out given the form filler’s individual situation;
- checking: ascertaining whether the task performance is proceeding correctly and making corrections where necessary;
- switching: interrupting the performance of interpretation tasks to carry out functional tasks and vice versa.
2.6. Measuring Level of Health Literacy: SBSQ
2.7. Data Collection and Analysis
2.8. Characteristics of the Investigators
3. Results
3.1. Problems with Interpretation Tasks
3.1.1. IPSS
“First thing I think: So did I only pee 5 times in a month? Or 5 times a day?”
“In the beginning it was difficult to connect the X and Y axes”.
“The answer options are tricky. In the beginning, it seemed that the answer most to the left meant ‘never’ and the one most to the right meant ‘almost always’. Then when my reaction to a question was ‘pretty good’, I filled out the box next to ‘almost always’.”
3.1.2. VPSS
“I thought it was about how often I pee during my work.”
“I filled out the frequency during the morning because I always work in the garden in the morning only.”
“I miss the question or text, I don’t really know what is expected of me.”
3.1.3. SVPI
“The flashing light is on the left, while the answer on the left actually indicates ‘no need’. Also, the answer option on the left with the red stripe represents ‘emergency’ to me, while this is precisely the answer without emergency. Red stands for alarm!”
“You would think the stronger the stream the higher the number. That made me doubt for a moment.”
“Clear questionnaire, despite the fact that Dutch is not my mother tongue”.
3.2. Problems with Functional Tasks
3.2.1. IPSS
3.2.2. VPSS
3.2.3. SVPI
3.3. Problems with Monitor Tasks
3.3.1. IPSS
“Not so clear that this question belongs there too, because it is separate from the table with all other questions.”
3.3.2. VPSS
3.3.3. SVPI
3.4. Results from the Retrospective Interviews
4. Discussion
4.1. Problems of Various Nature
4.2. Underlying Causes
4.3. Differences between Groups with Various Levels of Health Literacy
4.4. Relationship with the Results of Previous Studies
4.5. Strengths and Limitations
4.6. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Participants | IPSS Tot vs. VPSS Tot | IPSS Tot vs. Qmax | IPSS Tot vs. Qave | VPSS Tot vs. Qmax | VPSS Tot vs. Qave | FREQ VPSS Q1 vs. IPSS Q2 | NOCT VPSS Q2 vs. IPSS Q7 | WEAK VPSS Q3 vs. IPSS Q5 | IPSS Q5 vs. Qmax | IPSS Q5 vs. Qave | VPSS Q3 vs. Qmax | VPSS Q3 vs. Qave | IPSS QOL vs. VPSS QOL | IPSS Tot vs. IPSS QOL | VPSS Tot vs. VPSS QOL | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abiola (2016) [45] | n = 90 | .775 | - | - | - | - | .524 | .873 | .639 | - | - | - | - | .533 | - | - |
| <0.001 | - | - | - | - | <0.001 | <0.001 | <0.001 | - | - | - | - | <0.001 | - | - | ||
| Afriansya(2014) [46] | n = 103 | .675 | - | - | - | - | .494 | .952 | .572 | - | - | - | - | .823 | 0.666 | .470 |
| <0.001 | - | - | - | - | <0.001 | <0.001 | <0.001 | - | - | - | - | <0.001 | <0.001 | <0.001 | ||
| Bhomi (2017) [43] | n = 66 | .822 | −.701 | −.612 | −.729 | −.643 | .41 | .907 | .478 | −.321 | - | −.518 | - | .762 | - | - |
| <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | - | <0.01 | - | <0.01 | - | - | ||
| Ceylan (2015) [11] | n = 191 | .72 | −.52 | −.434 | −.3 | −.317 | .6 | .94 | .56 | −.44 | - | −.26 | - | .67 | 0.62 | .85 |
| <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | - | <0.001 | - | <0.001 | <0.001 | <0.001 | ||
| Els (2019) [47] | n = 100 | .802 | −.308 | −.310 | −.311 | −.344 | - | - | - | - | - | - | - | - | - | - |
| <0.0001 | 0.002 | 0.002 | 0.002 | <0.001 | - | - | - | - | - | - | - | - | - | - | ||
| Guzelsoy (2017) [48] | n = 309 | .694 | - | - | - | - | .340 | .848 | .468 | - | - | −.196 | −.173 | .460 | - | - |
| 0.0001 | - | - | - | - | 0.0001 | 0.001 | 0.0001 | - | - | 0.001 | 0.003 | 0.0001 | - | - | ||
| Heyns a (2012) [19] | n = 66 | .73 | −.30 | −.29 | −.38 | −.37 | - | - | - | −.15 | −0.11 | −.37 | −.31 | - | - | - |
| <0.001 | 0.016 | 0.018 | 0.002 | 0.003 | - | - | - | 0.219 | 0.370 | 0.002 | 0.011 | - | - | - | ||
| Heyns a (2014) [49] | n = 57 | .934 | −.284 | −.441 | −.174 | −.334 | .525 | .913 | .775 | −.365 | −0.507 | −.456 | −.572 | .902 | - | - |
| <0.0001 | 0.038 | 0.0006 | 0.208 | 0.011 | <0.0001 | <0.0001 | <0.0001 | 0.007 | <0.0001 | 0.0005 | <0.0001 | <0.0001 | - | - | ||
| Memon (2016) [44] | n = 67 | - | - | - | −.848 | - | - | - | - | - | - | - | - | - | - | - |
| - | - | - | <0.001 | - | - | - | - | - | - | - | - | - | - | - | ||
| Olcücü (2020) [3] | n = 342 | .677 | −.414 | −.447 | −.621 | −.565 | .494 | .862 | .780 | −.523 | - | −.483 | - | .550 | .726 | .709 |
| <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | - | <0.001 | - | <0.001 | <0.001 | <0.001 | ||
| Onowa (2019) [50] | n = 85 | .684 | −.328 | - | −.222 | - | - | - | - | - | - | - | - | .570 | .589 | .898 |
| 0.001 | 0.002 | - | 0.041 | - | - | - | - | - | - | - | - | <0.001 | <0.001 | <0.001 | ||
| Park (2014) [51] | n = 240 | .632 | - | - | - | - | - | - | - | - | - | −.269 | −.239 | .799 | - | - |
| <0.001 | - | - | - | - | - | - | - | - | - | <0.001 | <0.001 | <0.001 | - | - | ||
| Putra (2019) [52] | n = 252 | .57 | −.08 | - | −.19 | - | .39 | .72 | .50 | −.17 | - | −.26 | - | .76 | .67 | .45 |
| <0.001 | 0.252 | - | 0.002 | - | <0.001 | <0.001 | <0.001 | 0.006 | - | <0.001 | - | <0.001 | <0.001 | <0.001 | ||
| Roy (2016) [4] | n = 100 | - | −.433 | −.368 | −.719 | −.497 | .645 | .536 | .266 | −.159 | −0.103 | −.636 | −.538 | - | .693 | .430 |
| - | 0.000 | 0.000 | 0.000 | 0.000 | <0.01 | <0.01 | 0.007 | 0.114 | 0.306 | 0.000 | 0.000 | - | <0.01 | <0.01 | ||
| Selekman (2015) [53] | n = 121 | .71 | - | - | - | - | .47 | .69 | .65 | - | - | - | - | .73 | - | .69 |
| <0.001 | - | - | - | - | <0.001 | <0.001 | <0.001 | - | - | - | - | <0.001 | - | <0.001 | ||
| Setthawong (2018) [17] | n = 200 | .493 | −.046 | −.048 | −.159 | −.158 | - | - | - | - | - | - | - | - | - | - |
| <0.05 | 0.548 | 0.528 | 0.035 | 0.037 | - | - | - | - | - | - | - | - | - | - | ||
| Stothers (2017) [20] | n = 33 | - | - | - | - | - | .81 | .66 | .73 | - | - | - | - | - | - | - |
| - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | ||
| Taneja (2017) [12] | n = 121 | .724 | −.629 | −.479 | −.578 | −.5 | .508 | .886 | .761 | −.713 | - | −.753 | - | .841 | .656 | .708 |
| <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | - | <0.001 | - | <0.001 | <0.001 | <0.001 | ||
| Van der Walt (2011) [9] | n = 96 | - | −.280 | −.290 | −.421 | −.414 | .542 | .805 | .590 | −.110 | - | −.370 | - | .681 | .642 | .276 |
| - | 0.0068 | 0.0051 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.2936 | - | 0.0003 | - | <0.001 | <0.001 | 0.0065 | ||
| Wessels b (2014) [54] | n = 100 | .845 | −.587 | - | −.575 | - | - | - | - | - | - | −.595 | - | - | - | - |
| <0.001 | <0.001 | - | <0.001 | - | - | - | - | - | - | <0.0001 | - | - | - | - |
Appendix B. Introduction to the Aims of This Study
- Are you 40 years or older?
- Have you ever filled out this questionnaire about urinary problems before?
- If you agree to participate, please put your signature at the bottom of the permission letter.
Appendix C
| Questions | Problems | |||||||
|---|---|---|---|---|---|---|---|---|
| + | ± | - | 0 | |||||
| IPSS 1 Emptying | 14 (88) | 2 (29) | 2 (13) | 1 (14) | - | 4 (57) | - | - |
| IPSS 2 Frequency | 15 (94) | 1 (14) | 1 (6) | - | - | 5 (71) | - | 1 (14) |
| IPSS 3 Intermittency | 14 (88) | - | 2 (13) | - | - | 6 (86) | - | 1 (14) |
| IPSS 4 Urgency | 14 (88) | 1 (14) | 1 (6) | - | 1 (6) | 3 (43) | - | 3 (43) |
| IPSS 5 Stream | 13 (81) | 1 (14) | - | - | 2 (13) | 2 (29) | 1 (6) | 4 (57) |
| IPSS 6 Straining | 13 (81) | 2 (29) | 1 (6) | - | 1 (6) | 3 (43) | 1 (6) | 2 (29) |
| IPSS 7 Nocturia | 13 (81) | 4 (57) | 3 (19) | 1 (14) | - | 2 (29) | - | - |
| IPSS QOL | 9 (56) | 4 (57) | 6 (38) | - | - | - | 1 (6) | 3 (43) |
| VPSS 1 Frequency day | 7 (47) | 1 (17) | 6 (40) | - | 1 (7) | 2 (33) | 1 (7) | 3 (50) |
| VPSS 2 Frequency night | 10 (67) | 3 (50) | 5 (33) | - | - | - | - | 3 (50) |
| VPSS 3 Stream | 12 (80) | 4 (67) | 2 (13) | 1 (17) | 1 (7) | - | - | 1 (17) |
| VPSS 4 QOL | 8 (53) | 2 (33) | 5 (33) | - | 2 (13) | 2 (33) | - | 2 (33) |
| SVPI 1 Frequency night | 16 (100) | 4 (80) | - | 1 (20) | - | - | - | - |
| SVPI 2 Frequency night | 16 (100) | 5 (100) | - | - | - | - | - | - |
| SVPI 3 Urgency | 14 (88) | 4 (80) | 1 (6) | - | 1 (6) | - | - | 1 (20) |
| SVPI 4 Stream | 15 (94) | 4 (80) | - | 1 (20) | 1 (6) | - | - | - |
| SVPI 5 QOL | 15 (94) | 5 (100) | 1 (6) | - | - | - | - | - |
References
- European Association of Urology. Guideline Management of Non-Neurogenic Male LUTS 2022. Available online: https://uroweb.org/guidelines/management-of-non-neurogenic-male-luts (accessed on 20 May 2022).
- American Urological Association. Guideline Management of Benign Prostatic Hyperplasia/Lower Urinary Tract Symptoms 2021. Available online: https://www.auanet.org/guidelines/guidelines/benign-prostatic-hyperplasia-(bph)-guideline (accessed on 20 May 2022).
- Olcücü, M.T.; Aydın, M.E.; Avcı, S.; Koras, Ö.; Eren, A.E.; Yılmaz, K.; Ates, M. Comparison of a Visual Prostate Symptom Score and International Prostate Symptom Score: A Prospective Multicenter Study and Literature Review. Urology 2020, 146, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.; Singh, A.; Sidhu, D.S.; Jindal, R.P.; Malhotra, M.; Kaur, H. New Visual Prostate Symptom Score versus International Prostate Symptom Score in Men with Lower Urinary Tract Symptoms: A Prospective Comparision in Indian Rural Population. Niger. J. Surg. 2016, 22, 111–117. [Google Scholar] [PubMed]
- Barry, M.J.; Fowler, F.J.; O’Leary, M.P.; Bruskewitz, R.C.; Holtgrewe, H.L.; Mebust, W.K.; Cocket, A.T.K. The American Urological Association Symptom Index for benign prostatic hyperplasia. J. Urol. 1992, 148, S189–S197. [Google Scholar] [CrossRef]
- Burnett, A.L.; Wein, A.J. Benign Prostatic Hyperplasia in Primary Care: What You Need to Know. J. Urol. 2006, 175, S19–S24. [Google Scholar] [CrossRef]
- Morgantini, L.; Acar, O.; Tirapegui, F.; Ghafoor, S.; Naha, U.; Flores Martinez, J.; Madurga Patuel, B.; Kocjancic, E. Development and pilot testing of a simplified version of the International Prostate Symptom Score. Abstract 2080. ICS 2020 Online. Available online: https://www.ics.org/2020/abstract/280 (accessed on 20 May 2022).
- Cam, K.; Senel, F.; Akman, Y.; Erol, A. The efficacy of an abbreviated model of the International Prostate Symptom Score in evaluating benign prostatic hyperplasia. BJU Int. 2003, 91, 186–189. [Google Scholar] [CrossRef] [PubMed]
- Van der Walt, C.L.; Groeneveld, A.E.; Heyns, C.F.; Edlin, R.S.; van Vuuren, S.P. Prospective Comparison of a New Visual Prostate Symptom Score Versus the International Prostate Symptom Score in Men With Lower Urinary Tract Symptoms. Urology 2011, 78, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Netto Júnior, N.R.; de Lima, M.L. The influence of patiënt education level on the International Prostatic Symptom Score. J. Urol. 1995, 154, 97–99. [Google Scholar] [CrossRef]
- Ceylan, Y.; Gunlucoy, B.; Degirmency, T.; Kozacioglu, Z.; Bolat, D.; Minareci, S. Is new visual prostate symptom score useful as International Prostate Symptom Score in the evaluation of men with lower urinary tract symptoms? A prospective comparison of 2 symptom scores in Turkish society. Urology 2015, 85, 653–657. [Google Scholar] [CrossRef]
- Taneja, Y.; Ram, P.; Kumar, S.; Raj, K.; Singh, C.K.; Dhaked, S.K.; Jaipuria, J. Comparison of Visual Prostate Symptom Score and International Prostate Symptom Score in the evaluation of men with benign prostatic hyperplasia: A prospective study from an Indian population. Prostate Int. 2017, 5, 158–161. [Google Scholar] [CrossRef]
- Johnson, T.V.; Goodman, M.; Master, V.A. The efficacy of written screening tools in an inner city hospital: Literacy based limitations on patient access to appropriate care. J. Urol. 2007, 178, 623–629. [Google Scholar] [CrossRef]
- Johnson, T.V.; Abbasi, A.; Ehrlich, S.S.; Kleris, R.S.; Schoenberg, E.D.; Owen-Smith, A.; Goodman, M.; Master, V.A. Patient misunderstanding of the individual questions of the American Urological Association symptom score. J. Urol. 2008, 179, 2291–2294. [Google Scholar] [CrossRef] [PubMed]
- MacDiarmid, S.A.; Goodson, T.C.; Holmes, T.M.; Martin, P.R.; Doyle, R.B. An assessment of the comprehension of the American Urological Association Symptom Index. J. Urol. 1998, 159, 873–874. [Google Scholar] [CrossRef]
- Santos Silva, C.S.; de Araujo, U.M.; Alvaia, M.A.; Freitas, K.S.; Tiraboschi, T.L.; Gomes, C.M.; de Bessa Júnior, J. Luts-V: A new simplified score for assessing lower urinary tract symptoms in men. Int. Braz. J. Urol. 2021, 47, 525–532. [Google Scholar] [CrossRef]
- Setthawong, V.; Mahawong, P.; Pattanachindakun, N.; Amnattrakul, P.; Dar, F.M.; Thanavongvibul, S. To investigate the correlation between the visual prostate symptom score, the international prostate symptom score, and uroflowmetry parameters in adult Thai males of different educational levels. Prostate Int. 2018, 6, 115–118. [Google Scholar] [CrossRef]
- Van der Walt, C.; Groeneveld, A.; van Vuuren, S.; Edlin, R.; Heyns, C. Visual Prostate Symptom Score versust the International Prostate Symptom Score in men with lower urinary tract symptoms. Urology 2010, 76 (Suppl. S3A), S10. [Google Scholar] [CrossRef]
- Heyns, C.F.; van der Walt, C.L.E.; Groeneveld, A.E. Correlation between a new visual prostate symptom score (VPSS) and uroflowmetry parameters in men with lower urinary tract symptoms. Afr. Med. J. 2012, 102, 237–240. [Google Scholar]
- Stothers, L.; Macnab, A.; Bajunirwe, F.; Mutabazi, S.; Lobatt, C. Comprehension and construct validity of the Visual Prostate Symptom Score (VPSS) by men with obstructive lower urinary tract symptoms in rural Africa. Can. Urol. Assoc. J. 2017, 11, E405–E408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Descazeaud, A.; Coloby, P.; Davin, J.L.; De La Taille, A.; Karsenty, G.; Kouri, G.; Rossi, D.; Pouteau, J.C.; Zerbib, M. Validation of visual prostate symptom score, VPSS, in the evaluation of lower urinary tract symptoms associated with benign prostatic hyperplasia (550 patients). Urology 2017, 27, 176–183. [Google Scholar]
- Descazeaud, A.; Coloby, P.; Taille, A.; Karsenty, G.; Kouri, G.; Rossi, D.; Carrois, F.; Zerbib, M. The visual prostate symptom score is a simple tool to identify and follow up in general practice patients with lower urinary tract symptoms associated with benign prostatic hyperplasia (a study with 1359 patients). Presse Med. 2018, 47 Pt 1, e91–e98. [Google Scholar] [CrossRef]
- Balstad, T.R.; Bye, A.; Jenssen, C.R.S.; Solheim, T.S.; Thoresen, L.; Sand, K. Patient interpretation of the patient-generated subjective global assessment (PG-SGA) short form. Patient Prefer. Adherence 2019, 13, 1391–1400. [Google Scholar] [CrossRef] [Green Version]
- Jansen, C.J.M.; Steehouder, M. Taalverkeersproblemen Tussen Overheid en Burger. Ph.D. Dissertation, SDU, Den Haag, The Netherlands, 1989. [Google Scholar]
- Chew, L.D.; Bradley, K.A.; Boyko, E.J. Brief questions to identify patients with inadequate health literacy. Fam. Med. 2004, 36, 588–594. [Google Scholar] [PubMed]
- Guillemin, F.; Bombardier, C.; Beaton, D. Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines. J. Clin. Epidemiol. 1993, 46, 1417–1432. [Google Scholar] [CrossRef]
- Jansen, C.J.M.; Steehouder, M. Forms as a Source of Communication Problems. J. Tech. Writ. 1992, 22, 179–194. [Google Scholar] [CrossRef] [Green Version]
- Frohlich, D.M. On the organization of form-filling behaviour. Inf. Des. J. 1986, 5, 43–59. [Google Scholar]
- Frohlich, D.M. On the re-organisation of form-filling behaviour in an electronic medium. Inf. Des. J. 1987, 5, 111–128. [Google Scholar] [CrossRef]
- Fan, M.; Shi, S.; Truong, K.N. Practices and Challenges of Using Think-Aloud Protocols in Industry: An International Survey. JUS 2020, 15, 85–102. [Google Scholar]
- Van den Haak, M.J.; De Jong, M.D.T.; Schellens, P.J. Evaluating municipal websites: A methodological comparison of three think-aloud variants. Gov. Inf. Q. 2009, 26, 193–220. [Google Scholar] [CrossRef] [Green Version]
- Cooke, L. Assessing Concurrent Think-Aloud Protocol as a Usability Test Method: A Technical Communication Approach. IEEE Trans. Prof. Commun. 2010, 53, 202–215. [Google Scholar] [CrossRef]
- Van Someren, M.W.; Barnard, Y.F.; Sandberg, J.A.C. The Think Aloud Method. A Practical Guide to Modelling Cognitive Processes, 1st ed.; Academic Press: London, UK, 1994. [Google Scholar]
- Chew, L.D.; Griffin, J.M.; Partin, M.R.; Noorbaloochi, S.; Grill, J.P.; Snyder, A.; Bradley, K.A.; Nugent, S.M.; Baines, A.D.; Vanryn, M. Validation of screening questions for limited health literacy in a large VA outpatient population. J. Gen. Intern. Med. 2008, 23, 561–566. [Google Scholar] [CrossRef] [Green Version]
- Fransen, M.P.; Van Schaik, T.M.; Twickler, T.B.; Essink-Bot, M.L. Applicability of Internationally Available Health Literacy Measures in the Netherlands. J. Health Commun. 2011, 16 (Suppl. S3), 134–149. [Google Scholar] [CrossRef]
- Watanebe, S.; Nekolaichuk, C.; Beaumont, C.; Mawani, A. The Edmonton symptom assessment system: What do patients think? Support. Care Cancer 2009, 17, 675–683. [Google Scholar] [CrossRef]
- Bergh, I.; Ludlin Kvalem, I.; Aass, N.; Jensen Hjermstad, M. What does the answer mean? A qualitative study of how palliative cancer patients interpret and respond to the Edmonton Symptom Assessment System. Palliat. Med. 2011, 25, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Elling, S.; Lentz, L.; De Jong, M. Combining Concurrent Think-Aloud Protocols and Eye-Tracking Observations: An Analysis of Verbalizations and Silences. IEEE Trans. Prof. Commun. 2012, 55, 206–220. [Google Scholar] [CrossRef] [Green Version]
- Dowse, R.; Ehlers, S. Pictograms in Pharmacy. Int. J. Pharm. Pract. 1998, 6, 109–118. [Google Scholar] [CrossRef]
- Hafner, C.; Schneider, J.; Schindler, M.; Braillard, O. Visual aids in ambulatory clinical practice: Experiences, perceptions and needs of patients and healthcare professionals. PLoS ONE 2022, 17, e0263041. [Google Scholar] [CrossRef] [PubMed]
- Mbanda, N.; Dada, S.; Bastable, K.; Ingalill, G.B.; Ralf, W.S. A scoping review of the use of visual aids in health education materials for persons with low-literacy levels. Patient Educ. Couns. 2021, 104, 998–1017. [Google Scholar] [CrossRef]
- Van Beusekom, M.M.; Land-Zandstra, A.M.; Bos, M.J.W.; Van den Broek, J.M.; Guchelaar, H.J. Pharmaceutical pictograms for low-literate patients: Understanding, risk of false confidence, and evidence-based design strategies. Patient Educ. Couns. 2017, 100, 966–973. [Google Scholar] [CrossRef] [Green Version]
- Bhomi, K.; Subedi, N.; Panta, P. Correlation of Visual Prostate Symptom Score with International Prostate Symptom Score and Uroflowmetry Parameters in Nepalese Male Patients with Lower Urinary Tract Symptoms. JNMA J. Nepal Med. Assoc. 2017, 56, 217–220. [Google Scholar]
- Memon, M.; Ather, M. Relationship between visual prostate score (VPSS) and maximum flow rate (Qmax) in men with urinary tract symptoms. Int. Braz. J. Urol. 2016, 42, 321–326. [Google Scholar] [CrossRef]
- Abiola, O.; Ajape, A.; Adeniyi, S.; Ayeni, S. Use and ease of self-administered International Prostate Symptoms Score (IPSS) and Visual Prostate Symptoms Score (VPSS) questionnaires for the assessment of lower urinary tract symptoms in Nigerian men. Afr. Jf. Urol. 2016, 22, 121–126. [Google Scholar] [CrossRef]
- Afriansyah, A.; Gani, Y.; Nusali, H. Comparison between visual prostate symptom score and international prostate symptom score in males older than 40 years in rural Indonesia. Prostate Int. 2014, 2, 176–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Els, M.; Heyns, C.; van der Merwe, A.; Zarrabi, A. Prospective comparison of the novel visual prostate symptom score (VPSS) versus the international prostate symptom score (IPSS), and assessment of patient pain perception with regard to transrectal ultrasound guided prostate biopsy. Int. Braz. J. Urol. 2019, 45, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Guzelsoy, M.; Aydos, M.; Coban, S.; Turkoglu, A.; Acibucu, K.; Demirci, H. Comparison of the effectiveness of IPSS and VPSS without any help in LUTS patients: A prospective study. Aging Male 2018, 21, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Heyns, C.; Steenkamp, B.; Chiswo, J.; Stellmacher, G.; Förtsch, H.; van der Merwe, A. Evaluation of the visual prostate symptom score in a male population with great language diversity and limited education: A study from Namibia. S. Afr. Med. J. 2014, 26, 353–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onowa, V.; Shuaibu, S.; Akpayak, I.; Ofoha, C.; Agbo, C.; Nabasu, L.; Galam, Z.; Ramyil, V.; Dakum, N. Value of the visual prostate symptom score in evaluation of symptomatic benign prostatic enlargement: Prospective study in a Nigerian population. Int. J. Res. Med. Sci. 2019, 7, 1658–1664. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.; Lee, J. Correlation Between the Visual Prostate Symptom Score and International Prostate Symptom Score in Patients With Lower Urinary Tract Symptoms. Int. Neurourol. J. 2014, 18, 37–41. [Google Scholar] [CrossRef] [Green Version]
- Putra, I.; Hamid, A.; Rasyid, N.; Mochtar, C.; Umbas, R. Comparison of Visual Prostate Symptom Score with the International Prostate Symptom Score and uroflowmetry parameters in assessing men with lower urinary tract symptoms in Dr. Cipto Mangunkusumo National General Hospital, Indonesia. Prostate Int. 2019, 7, 91–95. [Google Scholar] [CrossRef]
- Selekman, R.; Harris, C.; Filippou, P.; Chi, T.; Alwaal, A.; Blaschko, S.; Breyer, B. Validation of a Visual Prostate Symptom Score in Men With Lower Urinary Tract Symptoms in a Health Safety Net Hospital. Urology 2015, 86, 354–358. [Google Scholar] [CrossRef] [Green Version]
- Wessels, S.; Heyns, C. Prospective Evaluation of a New Visual Prostate Symptom Score, the International Prostate Symptom Score, and Uroflowmetry in Men With Urethral Stricture Disease. Urology 2014, 83, 220–224. [Google Scholar] [CrossRef]




| IPSS | VPSS | SVPI | Total | |
|---|---|---|---|---|
| Participants (n) | ||||
| AHL | 16 | 15 | 16 | 47 |
| IHL | 7 | 6 | 5 | 18 |
| Total | 23 | 21 | 21 | 65 |
| Med. age (years) | ||||
| AHL | 75.5 (48–82) | 75 (43–84) | 65 (40–78) | 65 (40–84) |
| IHL | 52 (41–64) | 61.5 (57–65) | 64 (61–68) | 61 (41–68) |
| Total | 72 (41–82) | 69 (43–85) | 65 (40–78) | 65 (40–85) |
| Language | ||||
| AHL | ||||
| (near) native | 16 | 15 | 16 | 47 |
| non-native | 0 | 0 | 0 | 0 |
| IHL | ||||
| (near) native | 5 | 5 | 4 | 14 |
| non-native | 2 | 1 | 1 | 4 |
| Total | ||||
| (near) native | 21 | 20 | 20 | 61 |
| non-native | 2 | 1 | 1 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schlatmann, F.W.M.; van Balken, M.R.; de Winter, A.F.; de Jong, I.-J.; Jansen, C.J.M. How Do Patients Understand Questions about Lower Urinary Tract Symptoms? A Qualitative Study of Problems in Completing Urological Questionnaires. Int. J. Environ. Res. Public Health 2022, 19, 9650. https://doi.org/10.3390/ijerph19159650
Schlatmann FWM, van Balken MR, de Winter AF, de Jong I-J, Jansen CJM. How Do Patients Understand Questions about Lower Urinary Tract Symptoms? A Qualitative Study of Problems in Completing Urological Questionnaires. International Journal of Environmental Research and Public Health. 2022; 19(15):9650. https://doi.org/10.3390/ijerph19159650
Chicago/Turabian StyleSchlatmann, Florine W. M., Michael R. van Balken, Andrea F. de Winter, Igle-Jan de Jong, and Carel J. M. Jansen. 2022. "How Do Patients Understand Questions about Lower Urinary Tract Symptoms? A Qualitative Study of Problems in Completing Urological Questionnaires" International Journal of Environmental Research and Public Health 19, no. 15: 9650. https://doi.org/10.3390/ijerph19159650