
Cancer Survivors’ Long-Term Health Service Costs in Queensland, Australia: Results of a Population-Level Data Linkage Study (Cos-Q)

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Extraction & Linkage
2.1.1. Study Cohort
2.1.2. Ethics Approval
2.1.3. Healthcare in Australia and Data Linkage
2.2. Data Preparation and Analyses
2.2.1. Definition of Cancer Types
2.2.2. Cost Calculations
2.3. Data Cleaning and Statistical Analyses
3. Results
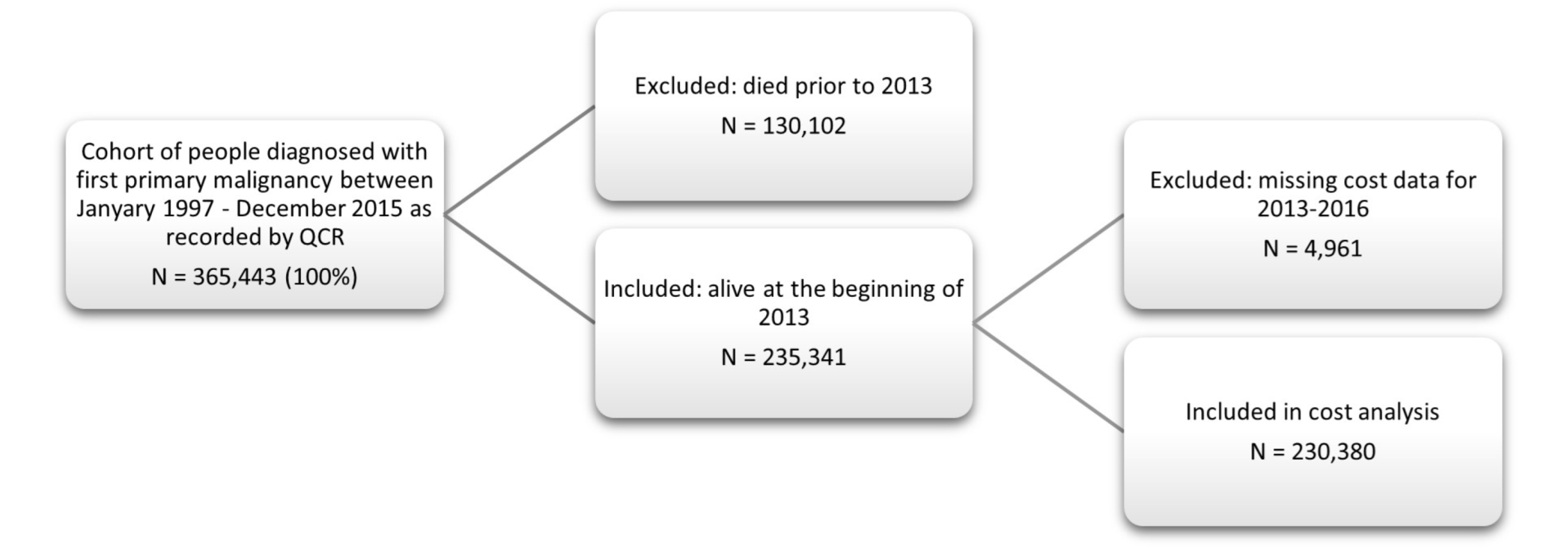
3.1. Patient Cohort Selection
3.2. Demographic Overview of Cancer Cohort
3.3. Mean Annual Healthcare Cost on Patient-Level
3.3.1. Costs by Age Group and Vital Status
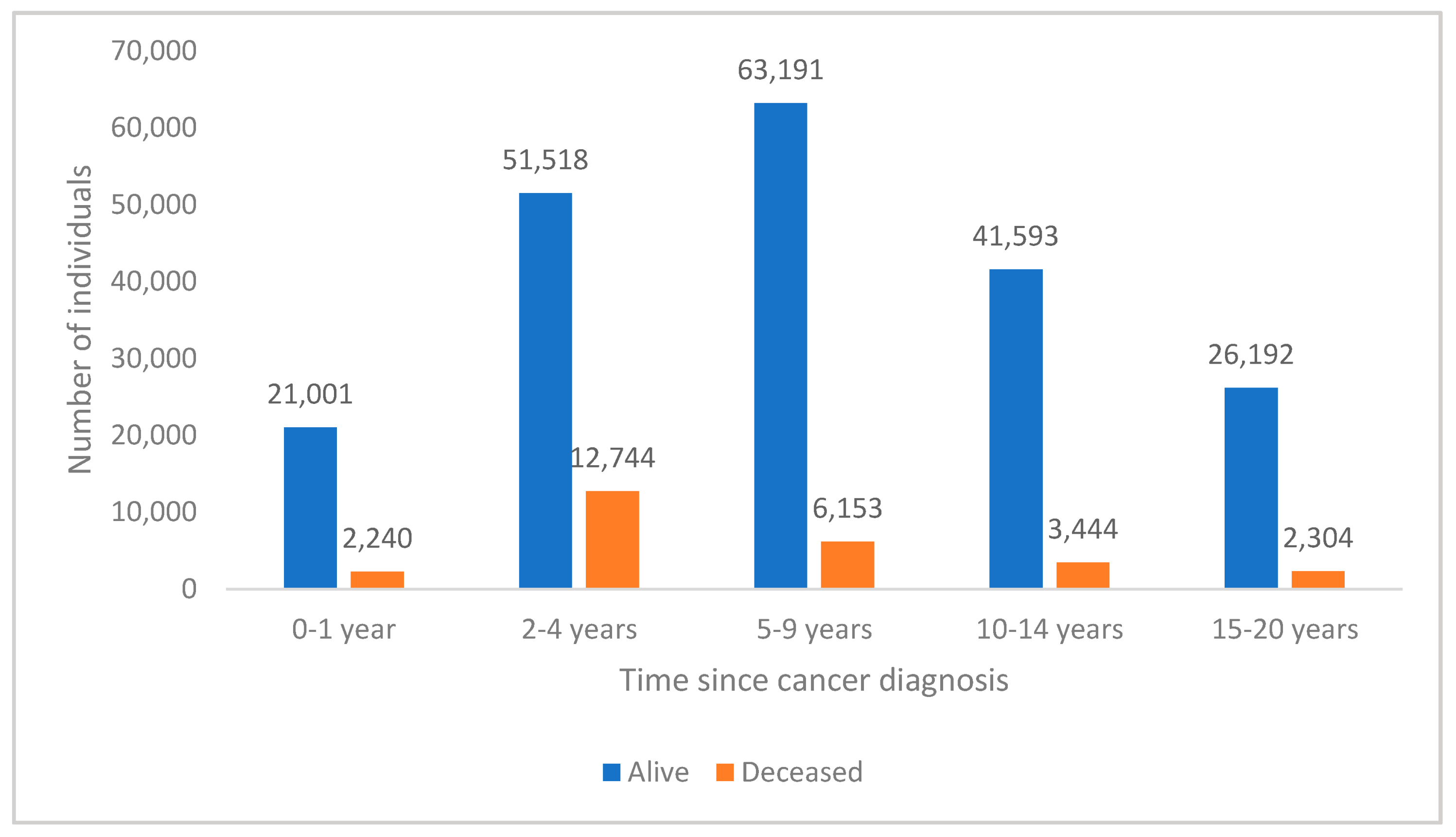
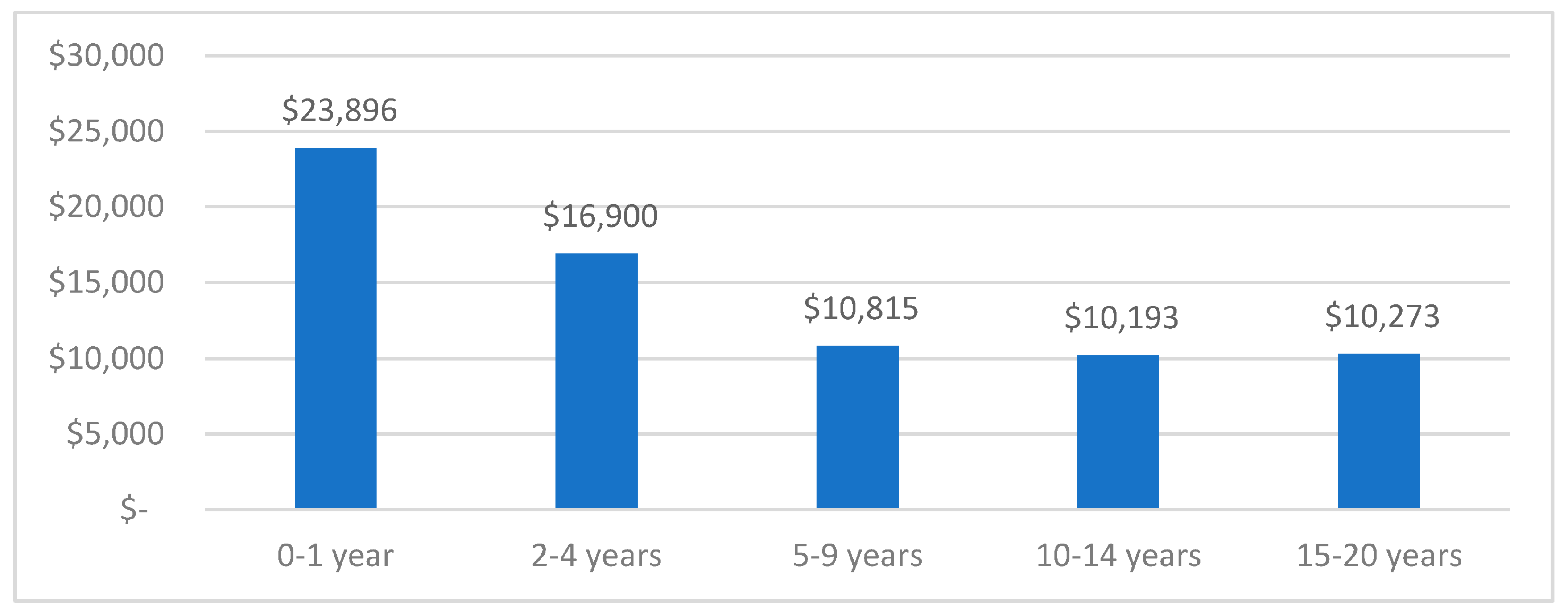
3.3.2. Costs by Time since Diagnosis
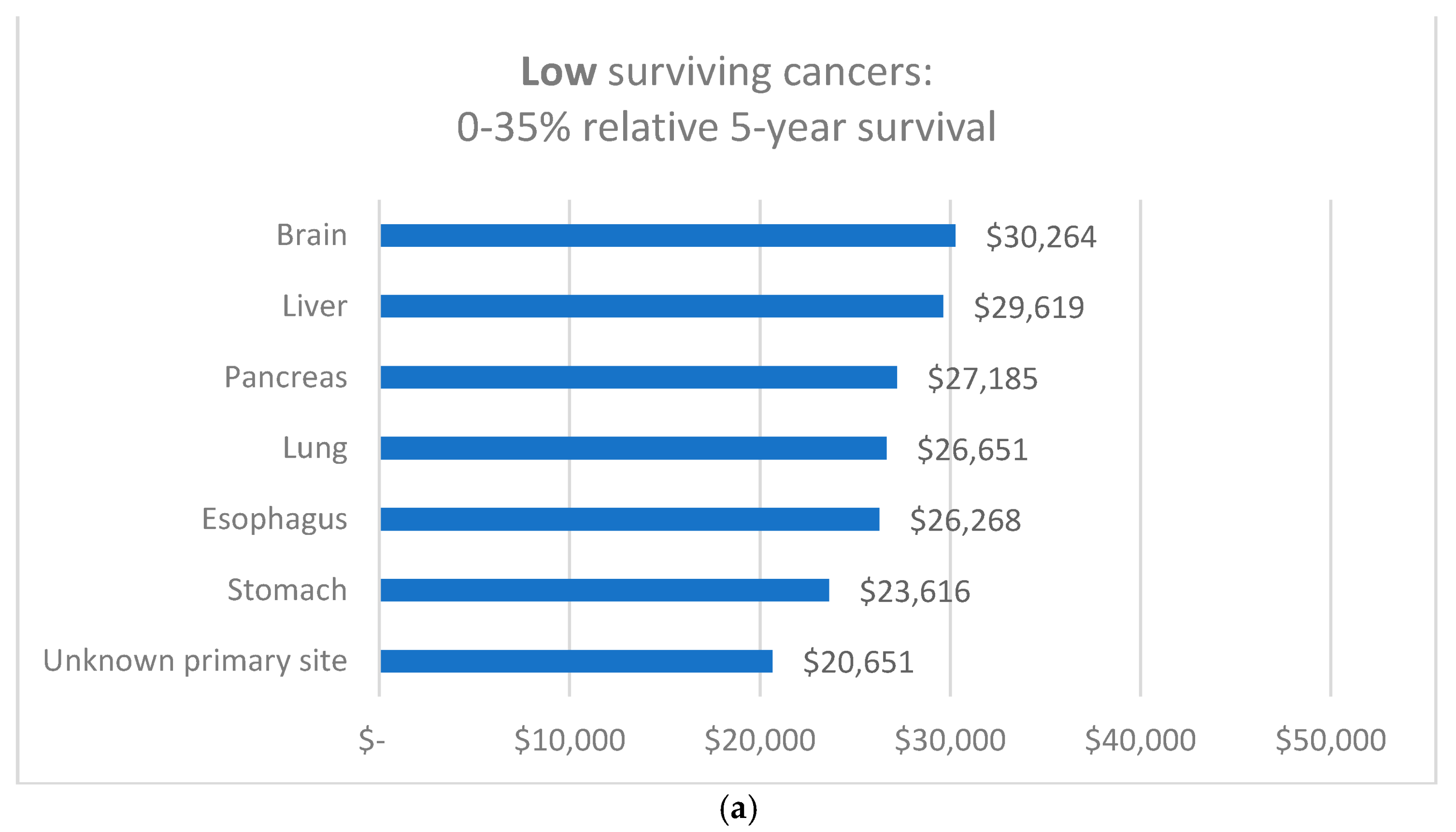
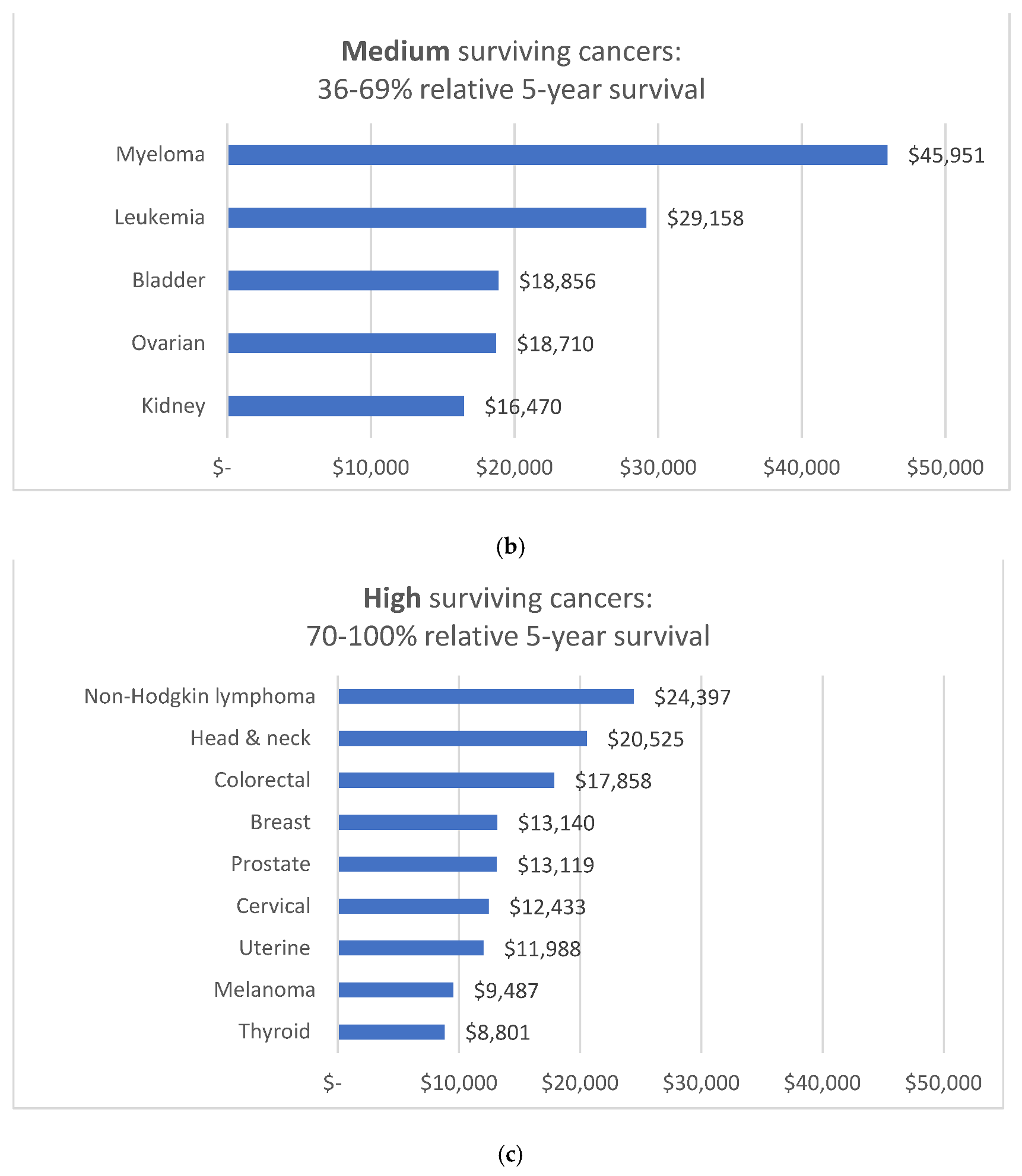
3.3.3. Costs by Type of Cancer and Relative 5-Year Survival Group
3.3.4. Costs by Type of Cancer and Health Service Component
3.4. Mean Annual Healthcare Cost on Cohort-Level
3.4.1. By Age Group in Proportion to Total Cost
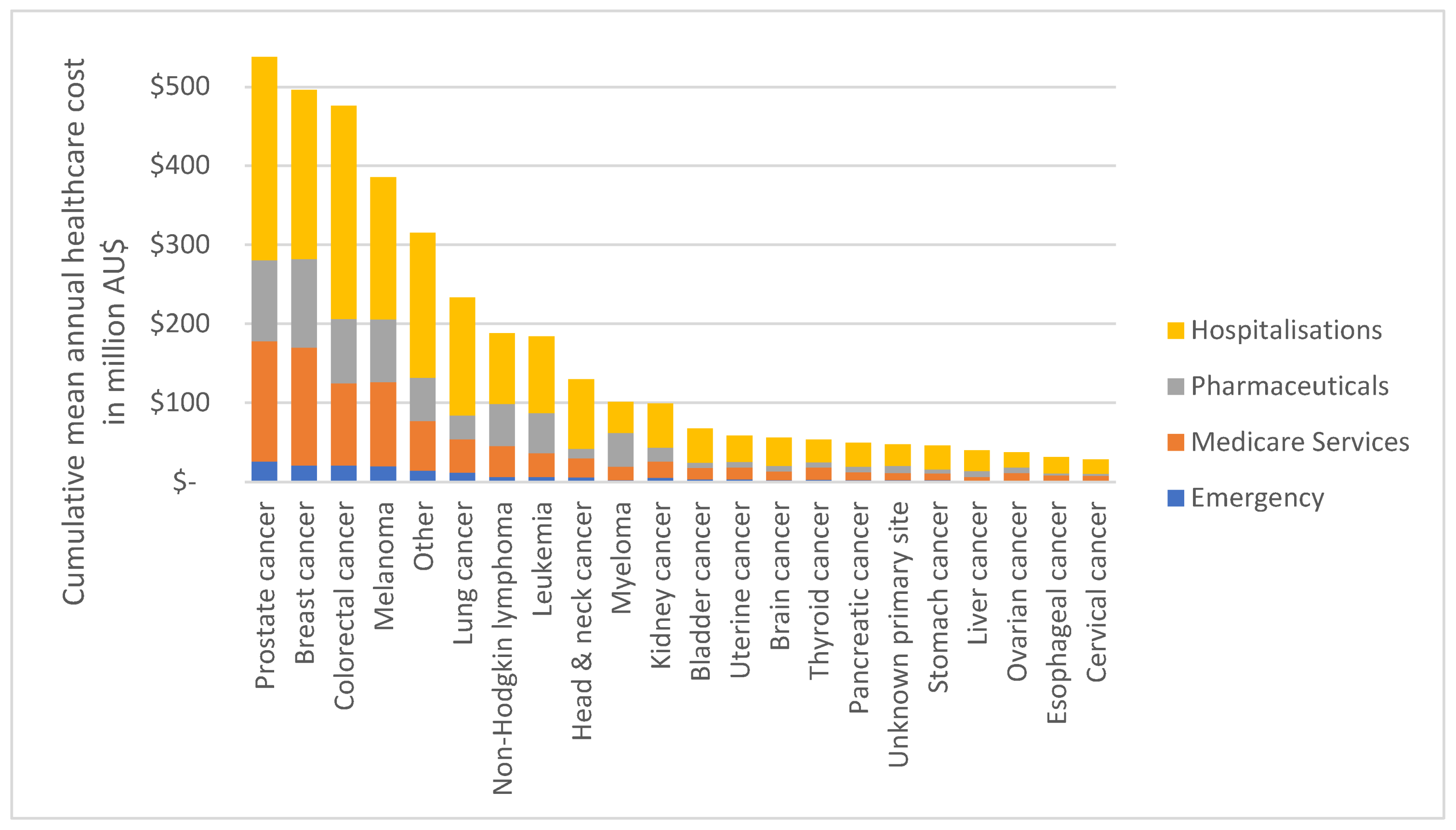
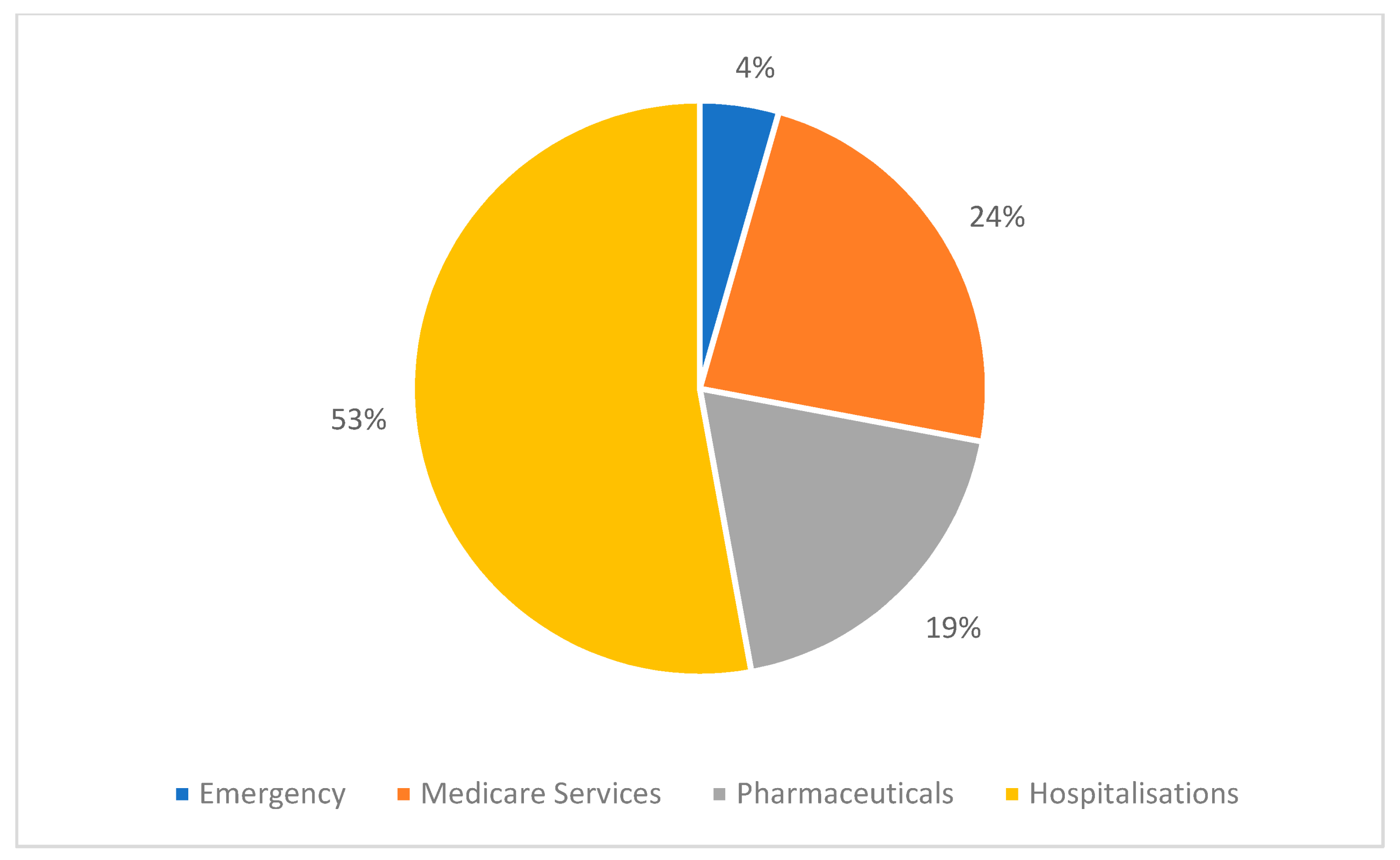
3.4.2. By Type of Cancer and Health Service Component
4. Discussion
4.1. Main Findings in Context of Recent Literature
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Denlinger, C.S.; Carlson, R.W.; Are, M.; Baker, K.S.; Davis, E.; Edge, S.B.; Friedman, D.L.; Goldman, M.; Jones, L.; King, A.; et al. Survivorship: Introduction and definition. Clinical practice guidelines in oncology. J. Natl. Compr. Canc Netw. 2014, 12, 34–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surbone, A.; Tralongo, P. Categorization of Cancer Survivors: Why We Need It. J. Clin. Oncol. 2016, 34, 3372–3374. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease Cancer, C.; Kocarnik, J.M.; Compton, K.; Dean, F.E.; Fu, W.; Gaw, B.L.; Harvey, J.D.; Henrikson, H.J.; Lu, D.; Pennini, A.; et al. Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022, 8, 420–444. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Cancer in Australia 2021. In Cancer Series No. 133 (Cat. No. CAN 144), AIHW, ed.; Australian Government: Canberra, Australia, 2021. [Google Scholar]
- Australian Institute of Health and Welfare. Disease Expenditure in Australia 2018-19, v23.0 (Last Updated 18/02/22) ed.; Australian Government, Ed. AIHW: Darlinghurst, Australia, 2021. [Google Scholar]
- Australian Institute of Health and Welfare. Health and Welfare. Health system expenditure on cancer and other neoplasms in Australia, 2015–2016. In Cancer Series No. 131 (Cat. No. CAN 142), AIHW, ed.; Australian Government: Canberra, Australia, 2021. [Google Scholar]
- American Cancer Society. Cancer Treatment & Survivorship: Facts & Figures 2019–2021; American Cancer Society: Atlanta, GA, USA, 2019. [Google Scholar]
- Caruso, R.; Breitbart, W. Mental health care in oncology. Contemporary perspective on the psychosocial burden of cancer and evidence-based interventions. Epidemiol. Psychiatr Sci. 2020, 29, e86. [Google Scholar] [CrossRef] [Green Version]
- Basaria, S.; Lieb, J., 2nd; Tang, A.M.; DeWeese, T.; Carducci, M.; Eisenberger, M.; Dobs, A.S. Long-term effects of androgen deprivation therapy in prostate cancer patients. Clin. Endocrinol. 2002, 56, 779–786. [Google Scholar] [CrossRef]
- Brook, I. Late side effects of radiation treatment for head and neck cancer. Radiat. Oncol. J. 2020, 38, 84–92. [Google Scholar] [CrossRef]
- Helou, J.; Charas, T. Acute and late side-effects after low dose-rate brachytherapy for prostate cancer; incidence, management and technical considerations. Brachytherapy 2021, 20, 956–965. [Google Scholar] [CrossRef]
- Rim, S.H.; Guy, G.P., Jr.; Yabroff, K.R.; McGraw, K.A.; Ekwueme, D.U. The impact of chronic conditions on the economic burden of cancer survivorship: A systematic review. Expert Rev. Pharm. Outcomes Res. 2016, 16, 579–589. [Google Scholar] [CrossRef] [Green Version]
- Guy, G.P., Jr.; Ekwueme, D.U.; Yabroff, K.R.; Dowling, E.C.; Li, C.; Rodriguez, J.L.; de Moor, J.S.; Virgo, K.S. Economic burden of cancer survivorship among adults in the United States. J. Clin. Oncol. 2013, 31, 3749–3757. [Google Scholar] [CrossRef] [Green Version]
- Iragorri, N.; de Oliveira, C.; Fitzgerald, N.; Essue, B. The Indirect Cost Burden of Cancer Care in Canada: A Systematic Literature Review. Appl. Health Econ. Health Policy 2021, 19, 325–341. [Google Scholar] [CrossRef]
- Callander, E.; Bates, N.; Lindsay, D.; Larkins, S.; Preston, R.; Topp, S.M.; Cunningham, J.; Garvey, G. The patient co-payment and opportunity costs of accessing healthcare for Indigenous Australians with cancer: A whole of population data linkage study. Asia Pac. J. Clin. Oncol. 2019, 15, 309–315. [Google Scholar] [CrossRef]
- Bates, N.; Callander, E.; Lindsay, D.; Watt, K. Correction to: CancerCostMod: A model of the healthcare expenditure, patient resource use, and patient co-payment costs for Australian cancer patients. Health Econ. Rev. 2019, 9, 2. [Google Scholar] [CrossRef] [Green Version]
- Callander, E.; Bates, N.; Lindsay, D.; Larkins, S.; Topp, S.M.; Cunningham, J.; Sabesan, S.; Garvey, G. Long-term out of pocket expenditure of people with cancer: Comparing health service cost and use for indigenous and non-indigenous people with cancer in Australia. Int. J. Equity Health 2019, 18, 32. [Google Scholar] [CrossRef] [Green Version]
- Goldsbury, D.E.; Yap, S.; Weber, M.F.; Veerman, L.; Rankin, N.; Banks, E.; Canfell, K.; O’Connell, D.L. Health services costs for cancer care in Australia: Estimates from the 45 and Up Study. PLoS ONE 2018, 13, e0201552. [Google Scholar] [CrossRef]
- Brodszky, V.; Varga, P.; Gimesi-Orszagh, J.; Fadgyas-Freyler, P.; Boncz, I.; Nyirady, P.; Riesz, P.; Baji, P.; Pentek, M.; Rencz, F.; et al. Long-term costs and survival of prostate cancer: A population-based study. Int. Urol. Nephrol. 2017, 49, 1707–1714. [Google Scholar] [CrossRef]
- Williams, S.B.; Howard, L.E.; Foster, M.L.; Klaassen, Z.; Sieluk, J.; De Hoedt, A.M.; Freedland, S.J. Estimated Costs and Long-term Outcomes of Patients With High-Risk Non-Muscle-Invasive Bladder Cancer Treated With Bacillus Calmette-Guerin in the Veterans Affairs Health System. JAMA Netw Open 2021, 4, e213800. [Google Scholar] [CrossRef]
- Grady, I.; Grady, S.; Chanisheva, N. Long-term cost of breast cancer treatment to the United States Medicare Program by stage at diagnosis. Eur. J. Health Econ. 2021, 22, 1365–1370. [Google Scholar] [CrossRef]
- Bermejo de Las Heras, B.; Cortes Ramon, Y.C.J.; Galve Calvo, E.; de la Haba Rodriguez, J.; Garcia Mata, J.; Moreno Anton, F.; Pelaez Fernandez, I.; Rodriguez-Lescure, A.; Rodriguez Sanchez, C.A.; Ruiz-Borrego, M.; et al. The economic burden of metastatic breast cancer in Spain. Eur. J. Hosp. Pharm. 2020, 27, 19–24. [Google Scholar] [CrossRef]
- de Oliveira, C.; Weir, S.; Rangrej, J.; Krahn, M.D.; Mittmann, N.; Hoch, J.S.; Chan, K.K.W.; Peacock, S. The economic burden of cancer care in Canada: A population-based cost study. CMAJ Open 2018, 6, E1–E10. [Google Scholar] [CrossRef] [Green Version]
- Cicin, I.; Oksuz, E.; Karadurmus, N.; Malhan, S.; Gumus, M.; Yilmaz, U.; Cansever, L.; Cinarka, H.; Cetinkaya, E.; Kiyik, M.; et al. Economic burden of lung cancer in Turkey: A cost of illness study from payer perspective. Health Econ. Rev. 2021, 11, 22. [Google Scholar] [CrossRef]
- Henderson, R.H.; French, D.; Maughan, T.; Adams, R.; Allemani, C.; Minicozzi, P.; Coleman, M.P.; McFerran, E.; Sullivan, R.; Lawler, M. The economic burden of colorectal cancer across Europe: A population-based cost-of-illness study. Lancet Gastroenterol. Hepatol. 2021, 6, 709–722. [Google Scholar] [CrossRef]
- Leal, J.; Luengo-Fernandez, R.; Sullivan, R.; Witjes, J.A. Economic Burden of Bladder Cancer Across the European Union. Eur. Urol. 2016, 69, 438–447. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, T.; Goto, R.; Yamamoto, Y.; Ichinose, Y.; Higashi, T. First-Year Healthcare Resource Utilization Costs of Five Major Cancers in Japan. Int. J. Environ. Res. Public Health 2021, 18, 9447. [Google Scholar] [CrossRef]
- Delgado-Ortega, L.; Gonzalez-Dominguez, A.; Borras, J.M.; Oliva-Moreno, J.; Gonzalez-Haba, E.; Menjon, S.; Perez, P.; Vicente, D.; Cordero, L.; Jimenez, M.; et al. The economic burden of disease of epithelial ovarian cancer in Spain: The OvarCost study. Eur. J. Health Econ. 2019, 20, 135–147. [Google Scholar] [CrossRef] [Green Version]
- Tan, S.S.; Rutten, F.F.; van Ineveld, B.M.; Redekop, W.K.; Hakkaart-van Roijen, L. Comparing methodologies for the cost estimation of hospital services. Eur. J. Health Econ. 2009, 10, 39–45. [Google Scholar] [CrossRef]
- Eakin, E.G.; Youlden, D.R.; Baade, P.D.; Lawler, S.P.; Reeves, M.M.; Heyworth, J.S.; Fritschi, L. Health behaviors of cancer survivors: Data from an Australian population-based survey. Cancer Causes Control. 2007, 18, 881–894. [Google Scholar] [CrossRef]
- Wong, W.; Yim, Y.M.; Kim, A.; Cloutier, M.; Gauthier-Loiselle, M.; Gagnon-Sanschagrin, P.; Guerin, A. Assessment of costs associated with adverse events in patients with cancer. PLoS ONE 2018, 13, e0196007. [Google Scholar] [CrossRef]
- Merollini, K.M.D.; Gordon, L.G.; Aitken, J.F.; Kimlin, M.G. Lifetime Costs of Surviving Cancer-A Queensland Study (COS-Q): Protocol of a Large Healthcare Data Linkage Study. Int. J. Environ. Res. Public Health 2020, 17, 2831. [Google Scholar] [CrossRef] [Green Version]
- Australian Bureau of Statistics. National, State and Territory Population. Available online: https://www.abs.gov.au/statistics/people/population/national-state-and-territory-population/latest-release (accessed on 21 June 2022).
- Pulok, M.H.; van Gool, K.; Hall, J. Horizontal inequity in the utilisation of healthcare services in Australia. Health Policy 2020, 124, 1263–1271. [Google Scholar] [CrossRef]
- Duckett, S. The Australian Health Care System; Oxford University Press: Melbourne, Australia, 2004. [Google Scholar]
- World Health Organisation. International Classification of Diseases for Oncology, 3rd ed.; (ICD-O3); WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Australian Government, C.A. National Cancer Control Indicator: 5-Year Relative Survival. Available online: https://ncci.canceraustralia.gov.au/outcomes/relative-survival-rate/5-year-relative-survival (accessed on 1 December 2021).
- Nuffield Trust. Cancer Survival Rates. Available online: https://www.nuffieldtrust.org.uk/resource/cancer-survival-rates (accessed on 1 December 2021).
- Australian Bureau of Statistics. Standard Australian Classification of Countries (SACC); Australian Bureau of Statistics: Canberra, Australia, 2016. [Google Scholar]
- Cancer Council NSW; Understanding Myeloma. A Guide for People with Cancer, Their Families and Friends; Cancer Council NSW: Wooloomooloo, Australia, 2020. [Google Scholar]
- Bates, N.; Callander, E.; Lindsay, D.; Watt, K. Cancer Cost Mod: A model of the healthcare expenditure, patient resource use, and patient co-payment costs for Australian cancer patients. Health Econ. Rev. 2018, 8, 28. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, C.; Pataky, R.; Bremner, K.E.; Rangrej, J.; Chan, K.K.; Cheung, W.Y.; Hoch, J.S.; Peacock, S.; Krahn, M.D. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer 2016, 16, 809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sam, D.; Cheung, W.Y. A population-level comparison of cancer-related and non-cancer-related health care costs using publicly available provincial administrative data. Curr. Oncol. 2019, 26, 94–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Essue, B.M.; Iragorri, N.; Fitzgerald, N.; de Oliveira, C. The psychosocial cost burden of cancer: A systematic literature review. Psychooncology 2020, 29, 1746–1760. [Google Scholar] [CrossRef] [PubMed]
- Luengo-Fernandez, R.; Leal, J.; Gray, A.; Sullivan, R. Economic burden of cancer across the European Union: A population-based cost analysis. Lancet Oncol. 2013, 14, 1165–1174. [Google Scholar] [CrossRef]
- Wiersma, M.; Ghinea, N.; Kerridge, I.; Lipworth, W. ‘Treat them into the grave’: Cancer physicians’ attitudes towards the use of high-cost cancer medicines at the end of life. Sociol. Health Illn. 2019, 41, 343–359. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (N) | Percent (%) |
|---|---|---|
| Total number of individuals | 230,380 | 100 |
| Gender ¹ | ||
| Male | 119,137 | 51.8 |
| Female | 105,062 | 46.9 |
| Age at diagnosis in years | N | % |
| 0–14 | 1905 | 0.9 |
| 15–24 | 3383 | 1.4 |
| 25–34 | 8708 | 3.7 |
| 35–44 | 18,708 | 8.1 |
| 45–54 | 38,068 | 16.5 |
| 55–64 | 60,018 | 26.1 |
| 65–74 | 59,979 | 26.0 |
| 75–84 | 30,872 | 13.4 |
| 85+ | 8739 | 3.8 |
| Mean age (SD) | 60.5 (15.4) | |
| Geographic location of birth | N | % |
| Australia | 176,994 | 76.8 |
| Northwest Europe | 25,210 | 10.9 |
| Oceania except Australia | 11,260 | 4.9 |
| Southeast Europe | 5611 | 2.4 |
| Southeast Asia | 2513 | 1.1 |
| Sub Saharan Africa | 2108 | 0.9 |
| America | 1814 | 0.8 |
| Northeast Asia | 1519 | 0.7 |
| South and Central Asia | 903 | 0.4 |
| North Africa and Middle East | 654 | 0.3 |
| Other | 1794 | 0.8 |
| Marital status | ||
| Married/De facto | 152,427 | 66.2 |
| Widowed | 26,181 | 11.4 |
| Divorced/Separated | 25,580 | 11.1 |
| Never married | 22,521 | 9.8 |
| Unknown | 3671 | 1.6 |
| Type of cancer | ||
| Prostate | 40,988 | 17.8 |
| Melanoma | 40,655 | 17.6 |
| Breast | 37,745 | 16.4 |
| Colorectal | 26,646 | 11.6 |
| Lung | 8750 | 3.8 |
| Non-Hodgkin lymphoma | 7700 | 3.3 |
| Head & neck | 6323 | 2.7 |
| Leukemia | 6308 | 2.7 |
| Thyroid | 6098 | 2.6 |
| Kidney | 6016 | 2.6 |
| Uterine | 4893 | 2.1 |
| Bladder | 3574 | 1.6 |
| Unknown primary site | 2303 | 1.0 |
| Cervical | 2266 | 1.0 |
| Myeloma | 2201 | 1.0 |
| Ovarian | 1997 | 0.9 |
| Stomach | 1941 | 0.8 |
| Brain | 1849 | 0.8 |
| Pancreatic | 1819 | 0.8 |
| Liver | 1342 | 0.6 |
| Esophageal | 1200 | 0.5 |
| All other cancers combined | 17,766 | 7.7 |
| Survivorship status by 2016 | ||
| Alive | 203,495 | 88.3% |
| Deceased (between 2013–15) | 26,885 | 11.7% |
| Age at death | ||
| Mean (SD) | 74.7 (13.5) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merollini, K.M.D.; Gordon, L.G.; Ho, Y.M.; Aitken, J.F.; Kimlin, M.G. Cancer Survivors’ Long-Term Health Service Costs in Queensland, Australia: Results of a Population-Level Data Linkage Study (Cos-Q). Int. J. Environ. Res. Public Health 2022, 19, 9473. https://doi.org/10.3390/ijerph19159473
Merollini KMD, Gordon LG, Ho YM, Aitken JF, Kimlin MG. Cancer Survivors’ Long-Term Health Service Costs in Queensland, Australia: Results of a Population-Level Data Linkage Study (Cos-Q). International Journal of Environmental Research and Public Health. 2022; 19(15):9473. https://doi.org/10.3390/ijerph19159473
Chicago/Turabian StyleMerollini, Katharina M. D., Louisa G. Gordon, Yiu M. Ho, Joanne F. Aitken, and Michael G. Kimlin. 2022. "Cancer Survivors’ Long-Term Health Service Costs in Queensland, Australia: Results of a Population-Level Data Linkage Study (Cos-Q)" International Journal of Environmental Research and Public Health 19, no. 15: 9473. https://doi.org/10.3390/ijerph19159473