
Resistance Circuit Training or Walking Training: Which Program Improves Muscle Strength and Functional Autonomy More in Older Women?


 , , and
, , and 
Abstract
:1. Introduction
2. Methods
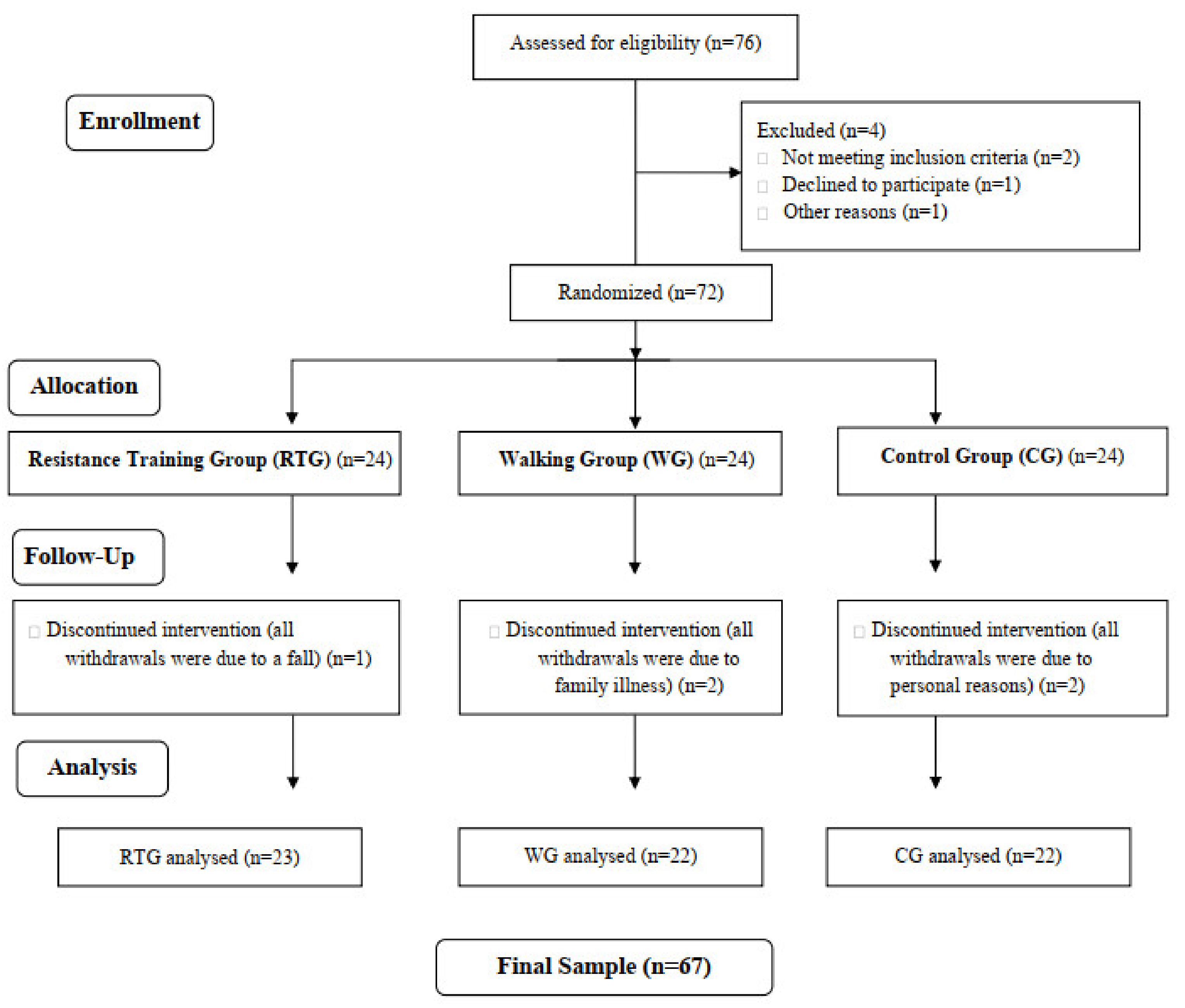
2.1. Participants
2.2. Data Collection Procedures
2.2.1. Anthropometric Measurements
Isometric Muscle Strength
Dynamic Muscle Strength
Functional Autonomy
Intervention
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marcos-Pardo, P.J.; Orquin-Castrillón, F.J.; Gea-García, G.M.; Menayo-Antúnez, R.; González-Gálvez, N.; Vale, R.G.S.; Martínez-Rodríguez, A. Effects of a moderate-to-high intensity resistance circuit training on fat mass, functional capacity, muscular strength, and quality of life in elderly: A randomized controlled trial. Sci. Rep. 2019, 9, 7830–7841. [Google Scholar] [CrossRef] [Green Version]
- Santos, J.R.; Costa, F.B.; Santos, J.L.; Oliveira, A.N.; Lima Júnior, C.M.A.; Silva Neto, A.O.; Souza, L.M.V. Avaliação da independência funcional e percepção da qualidade de vida de idosas praticantes de atividades físicas: Um estudo piloto. Motricidade 2020, 16, 64–71. [Google Scholar]
- Keating, C.J.; Cabrera-Linares, J.C.; Párraga-Montilla, J.A.; Latorre-Román, P.A.; Del Castillo, R.M.; García-Pinillos, F. Influence of resistance training on gait & balance parameters in older adults: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 1759. [Google Scholar]
- Borzuola, R.; Giombini, A.; Torre, G.; Campi, S.; Albo, E.; Bravi, M.; Borrione, P.; Fossati, C.; Macaluso, A. Central and peripheral neuromuscular adaptations to ageing. J. Clin. Med. 2020, 9, 741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Noronha Ribeiro, D.; de Souza Vale, R.G.; Giani, T.S.; Bacellar, S.; Escobar, T.; Stoutenberg, M.; Dantas, E.H.M. Correlation between static balance and functional autonomy in elderly women. Arch. Gerontol. Geriatr. 2011, 52, 111–114. [Google Scholar] [CrossRef]
- Meereis Lemos, E.C.W.; Guadagnin, E.C.; Mota, C.B. Influence of strength training and multicomponent training on the functionality of older adults: Systematic review and meta-analysis. Rev. Bras. Cineantropometria Desempenho Hum. 2020, 22, e60707. [Google Scholar] [CrossRef] [Green Version]
- Cascon, R.M.; Brown, A.D.I.; Cardozo, D.; Salermo, V.P.; Simão, R. Efeito do treinamento de força na potência muscular de membros inferiores de idosos coronariopatas. ConSci. Saúde 2017, 16, 26–32. [Google Scholar] [CrossRef]
- Brancaccio, M.; Mennitti, C.; Cesaro, A.; Fimiani, F.; Moscarella, E.; Caiazza, M.; Gragnano, F.; Ranieri, A.; D’Alicandro, G.; Tinto, N.; et al. Dietary thiols: A potential supporting strategy against oxidative stress in heart failure and muscular damage during sports activity. Int. J. Environ. Res. Public Health 2020, 17, 9424. [Google Scholar] [CrossRef]
- De Araújo, S.S.; Aidar, F.J.; Matos, D.G.d.; Santos, J.L.d.; Vieira Souza, L.M.; Silva, A.N.d.; Santos, R.M.d.; Marçal, A.C.; Mourão, D.M.; Júnior, A.L.; et al. Does Croton Argyrophyllus extract has an effect on muscle damage and lipid peroxidation in rats submitted to high intensity strength exercise? Int. J. Environ. Res. Public Health 2019, 16, 4237. [Google Scholar] [CrossRef] [Green Version]
- Resende-Neto, A.G.; Andrade, B.C.O.; Cyrino, E.S.; David, G.; De-Santana, B.M.; Silva-Grigoletto, M.E. Effects of functional and traditional training in body composition and muscle strength components in older women: A randomized controlled trial. Arch. Gerontol. Geriatr. 2019, 84, 103902. [Google Scholar] [CrossRef]
- Walker, S. Evidence of resistance training-induced neural adaptation in older adults. Exp. Gerontol. 2021, 151, 111408. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Beck, T.W. The importance of a priori sample size estimation in strength and conditioning research. J. Strength Cond. Res. 2013, 27, 2323–2337. [Google Scholar] [CrossRef] [PubMed]
- Marfell-Jones, M.; Olds, T.; Stewart, A.; Carter, L. International Standards for Anthropometric Assessment; ISAK: Potchefstroom, South Africa, 2006. [Google Scholar]
- Allen, T.J.; Jones, T.; Tsay, A.; Morgan, D.L.; Proske, U. Muscle damage produced by isometric contractions in human elbow flexors. J. Appl. Physiol. 2017, 124, 388–399. [Google Scholar] [CrossRef]
- Limonta, E.; Arienti, C.; Rampichini, S.; Venturelli, M.; Cè, E.; Veicsteinas, A.; Esposito, F. Effects of two different self-adapted occlusal splints on electromyographic and force parameters during elbow flexors isometric contraction. J. Strength Cond. Res. 2018, 32, 230–236. [Google Scholar] [CrossRef]
- Rikli, R.; Jones, C. Development and validation of a functional fitness test for community residing older adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Marcos-Pardo, P.J.; González-Gálvez, N.; Vaquero-Cristóbal, R.; Gea-García, G.M.; López-Vivancos, A.; Espeso-García, A.; Velázquez-Díaz, D.; Carbonell-Baeza, A.; Jiménez-Pavón, D.; Brandão Pinto de Castro, J.; et al. Functional autonomy evaluation levels in middle-aged and older Spanish women: On behalf of the Healthy-Age network. Sustainability 2020, 12, 9208. [Google Scholar] [CrossRef]
- Dantas, E.H.M.; Vale, R.G.S. Protocolo GDLAM de avaliação da autonomia funcional. Fit. Perform. J. 2004, 3, 175–182. [Google Scholar]
- Dantas, E.H.M.; Figueira, H.A.; Emygdio, R.F.; Vale, R.G.S. Functional autonomy GDLAM protocol classification parttern in eldely women. Indian J. Appl. Res. 2014, 4, 262–266. [Google Scholar] [CrossRef]
- Sipilã, S.; Multanen, J.; Kallinem, M.; Era, P.; Suominen, H. Effects of strength and endurance training on isometric muscle strength and walking speed in elderly women. Acta Physiol. Scand. 1996, 156, 457–464. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berk-man, L.F.; Blazer, D.G.; Sherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity fuction: Association with self-reported disability and prediction of mortality of mortality and nursing home admission. J. Gerontol. 1994, 49, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Alexander, N.B.; Ulbrich, J.; Raheja, A.; Channer, D. Rising from the floors in older adults. J. Am. Geriatr. Soc. 1997, 45, 564–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreotti, R.A.; Okuma, S.S. Validação de uma bateria de testes de atividades da vida diária para idosos fisicamente independentes. Rev. Paul. Educ. Fís. 1999, 13, 46–66. [Google Scholar] [CrossRef] [Green Version]
- Vale, R.G.S.; Pernambuco, C.S.; Novaes, J.S.; Dantas, E.H.M. Teste de autonomia funcional: Vestir e tirar uma camiseta (PTS). Rev. Bras. Ciênc. Mov. 2006, 14, 71–78. [Google Scholar] [CrossRef] [Green Version]
- American College of Sports Medicine (ACSM). Guidelines for Graded Exercise Testing and Exercise Prescription, 11th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2019. [Google Scholar]
- Kukkonen-Harjula, K.; Hiilloskorpi, H.; Mänttäri, A.; Pasanen, M.; Parkkari, J.; Suni, J.; Fogelholm, M.; Laukkanen, R. Self-guided brisk walking training with or without poles: A randomized-controlled trial in middle-aged women. Scand. J. Med. Sci. Sports 2007, 17, 316–323. [Google Scholar] [CrossRef]
- Robertson, R.; Goss, F.; Rutkowski, J.; Lenz, B.; Dixon, C.; Timmer, J.; Frazee, K.; Dube, J.; Andreacci, J. Concurrent validation of the OMNI perceived exertion scale for resistance exercise. Med. Sci. Sports Exerc. 2003, 35, 333–341. [Google Scholar] [CrossRef] [Green Version]
- Dantas, E.H.M.; Salomão, P.T.; Vale, R.G.S.; Achour Junior, A.; Simão, R.; Figueiredo, N.M.A. Scale of perceived exertion in the flexibility (PERFLEX): A dimension less tool to evaluate the intensity? Fit. Perform. J. 2008, 7, 289–294. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Bavaresco Gambassi, B.; dos Santos, C.P.; Queiroz, C.O.; Mesquita, F.O.; Santos, P.R.; Furtado Almeida, A.E.; Schwingel, P.A.; Furtado Almeida, F.D. Effects of a four-exercise resistance training protocol on functional parameters in sedentary elderly women. Sport Sci. Health 2020, 16, 99–104. [Google Scholar] [CrossRef]
- Dib, M.M.; Tomeleri, C.M.; Nunes, J.P.; Cunha, P.M.; Ribeiro, A.S.; Schiavoni, D.; Cavalcante, E.F.; Kunevaliki, G.; Teixeira, D.C.; de Oliveira, A.R.; et al. Effects of Three Resistance Exercise Orders on Muscular Function and Body Composition in Older Women. Int. J. Sports Med. 2020, 41, 1024–1031. [Google Scholar] [CrossRef]
- Suzuki, F.S.; Evangelista, A.L.; Teixeira, C.V.; Paunksnis, M.R.; Rica, R.L.; Evangelista, R.A.; João, G.A.; Doro, M.R.; Sita, D.M.; Serra, A.J.; et al. Effects of a multicomponent exercise program on the functional fitness in elderly women. Rev. Bras. Med. Esporte 2018, 24, 36–39. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, A.S.; Nunes, J.P.; Schoenfeld, B.J. Selection of Resistance Exercises for Older Individuals: The Forgotten Variable. Sports Med. 2020, 50, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Tavoian, D.; Russ, D.W.; Consitt, L.A.; Clark, B.C. Perspective: Pragmatic exercise recommendations for older adults: The case for emphasizing resistance training. Front. Physiol. 2020, 11, 799. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Garofolini, A.; Orazem, J.; Sabol, F.; Schoenfeld, B.J.; Pedisic, Z. Effects of Resistance Training on Muscle Size and Strength in Very Elderly Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sports Med. 2020, 50, 1983–1999. [Google Scholar] [CrossRef]
- Kis, O.; Buch, A.; Stern, N.; Moran, D.S. Minimally supervised home-based resistance training and muscle function in older adults: A meta-analysis. Arch. Gerontol. Geriatr. 2019, 84, 103909. [Google Scholar] [CrossRef]
- Herda, A.A.; Nabavizadeh, O. Short-term resistance training in older adults improves muscle quality: A randomized control trial. Exp. Gerontol. 2021, 145, 111195. [Google Scholar] [CrossRef]
- Skiadopoulos, A.; Stergiou, N. Risk-of-falling related outcomes improved in community-dwelling older adults after a 6-week sideways walking intervention: A feasibility and pilot study. BMC Geriatr. 2021, 21, 60. [Google Scholar] [CrossRef]
- Silva, C.D.; Oliveira, N.C.; Alfieri, F.M. Mobilidade funcional, força, medo de cair, estilo e qualidade de vida em idosos praticantes de caminhada. Acta Fisiátrica 2018, 25, 22–26. [Google Scholar] [CrossRef] [Green Version]
- Fragala, M.; Cadore, E.L.; Dorgo, S.; Esquerda, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance training for older adults: Position statement from the National Strength and Conditioning Association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- Lee, H.S.; Park, J.H. Effects of Nordic walking on physical functions and depression in frail people aged 70 years and above. J. Phys. Ther. Sci. 2015, 27, 2453–2456. [Google Scholar] [CrossRef] [Green Version]
- Marciniak, K.; Maciaszek, J.; Cyma-Wejchenig, M.; Szeklicki, R.; Maćkowiak, Z.; Sadowska, D.; Stemplewski, R. The Effect of Nordic Walking Training with Poles with an Integrated Resistance Shock Absorber on the Functional Fitness of Women over the Age of 60. Int. J. Environ. Res. Public Health 2020, 17, 2197. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Groups | Mean ± SD | p-Value (SW) |
|---|---|---|---|
| Age (years) | RTG | 64.70 ± 6.74 | 0.321 |
| WG | 65.56 ± 7.82 | 0.291 | |
| CG | 64.81 ± 4.34 | 0.435 | |
| Body mass (kg) | RTG | 63.06 ± 11.01 | 0.154 |
| WG | 68.94 ± 13.47 | 0.127 | |
| CG | 67.51 ± 6.57 | 0.173 | |
| Height (m) | RTG | 1.53 ± 0.06 | 0.451 |
| WG | 1.56 ± 0.07 | 0.428 | |
| CG | 1.58 ± 0.08 | 0.413 | |
| BMI (kg/m2) | RTG | 26.88 ± 4.43 | 0.391 |
| WG | 28.34 ± 4.72 | 0.349 | |
| CG | 27.18 ± 2.98 | 0.402 |
| Groups | Pre-Test | Pos-Test | Δ% | d | |
|---|---|---|---|---|---|
| BIS (N) | RTG | 154.24 ± 43.93 | 200.70 ± 27.81 *,#,† | 30.13% | 1.06 (s) |
| WG | 152.43 ± 37.63 | 160.89 ± 33.52 | 5.55% | 0.22 (m) | |
| CG | 151.31 ± 36.57 | 154.27 ± 34.61 | 2.0% | 0.08 (w) | |
| QIS (N) | RTG | 223.75 ± 73.15 | 371.26 ± 57.81 *,#,† | 65.92% | 2.02 (s) |
| WG | 207.65 ± 77.31 | 294.44 ± 72.68 *,† | 41.80% | 1.12 (s) | |
| CG | 202.72 ± 70.13 | 204.98 ± 67.76 | 1.1% | 0.03 (w) | |
| MULS (REP) | RTG | 14.37 ± 4.21 | 21.48 ± 2.49 *,#,† | 49.48% | 1.69 (s) |
| WG | 13.59 ± 3.41 | 14.15 ± 2.61 | 4.09% | 0.16 (w) | |
| CG | 12.89 ± 3.68 | 13.17 ± 3.41 | 2.2% | 0.07 (w) | |
| MLLS (REP) | RTG | 14.37 ± 3.34 | 22.52 ± 2.59 *,#,† | 56.70% | 2.44 (s) |
| WG | 12.81 ± 2.79 | 19.11 ± 1.65 *,† | 49.13% | 2.26 (s) | |
| CG | 11.76 ± 3.02 | 12. 23 ± 2.58 | 4.0% | 0.15 (w) |
| Groups | Pre-Test | Pos-Test | Δ% | d | |
|---|---|---|---|---|---|
| W10M (s) | RTG | 7.88 ± 3.15 | 6.57 ± 1.29 *,† | −16.63% | −0.42 (m) |
| WG | 7.95 ± 1.12 | 6.93 ± 1.05 *,† | −12.85% | −0.91 (s) | |
| CG | 8.26 ± 2.70 | 8.41 ± 2.73 | 1.8% | 0.05 (w) | |
| SSP (s) | RTG | 12.13 ± 3.08 | 10.47 ± 1.38 *,#,† | −13.68% | −0.54 (m) |
| WG | 13.06 ± 3.59 | 11.69 ± 2.40 *,† | −10.53 | −0.38 (m) | |
| CG | 12.93 ± 2.42 | 13.17 ± 2.88 | 1.9% | 0.10 (w) | |
| SVDP (s) | RTG | 5.33 ± 2.67 | 3.91 ± 1.12 *,#,† | −26.67% | −0.53 (m) |
| WG | 6.48 ± 3.60 | 6.16 ± 4.22 | −4.86% | −0.09 (w) | |
| CG | 5.86 ± 1.67 | 6.37 ± 1.81 | 8.7% | 0.30 (m) | |
| SCMH (s) | RTG | 47.37 ± 7.87 | 40.52 ± 4.11 *,#,† | −14.45% | −0.87 (s) |
| WG | 48.29 ± 5.86 | 45.46 ± 5.61 *,† | −5.87% | −0.48 (m) | |
| CG | 48.91 ± 11.93 | 49.21 ± 12.55 | 0.6% | 0.02 (w) | |
| PTS (s) | RTG | 15.11 ± 4.47 | 11.17 ± 1.69 *,#,† | −26.05% | −0.88 (s) |
| WG | 14.42 ± 3.63 | 12.66 ± 2.41 * | −12.20% | −0.48 (m) | |
| CG | 14.44 ± 4.18 | 13.82 ± 3.87 | −4.3% | −0.15 (w) | |
| GI (scores) | RTG | 32.07 ± 7.14 | 26.19 ± 2.08 *,#,† | −18.32% | −0.82 (s) |
| WG | 33.03 ± 5.73 | 30.08 ± 4.31 *,† | −8.91% | −0.51 (m) | |
| CG | 32.96 ± 5.11 | 33.19 ± 5.15 | 0.7% | 0.04 (w) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos, A.M.; Marcos-Pardo, P.J.; Vale, R.G.d.S.; Vieira-Souza, L.M.; Camilo, B.d.F.; Martin-Dantas, E.H. Resistance Circuit Training or Walking Training: Which Program Improves Muscle Strength and Functional Autonomy More in Older Women? Int. J. Environ. Res. Public Health 2022, 19, 8828. https://doi.org/10.3390/ijerph19148828
Ramos AM, Marcos-Pardo PJ, Vale RGdS, Vieira-Souza LM, Camilo BdF, Martin-Dantas EH. Resistance Circuit Training or Walking Training: Which Program Improves Muscle Strength and Functional Autonomy More in Older Women? International Journal of Environmental Research and Public Health. 2022; 19(14):8828. https://doi.org/10.3390/ijerph19148828
Chicago/Turabian StyleRamos, Ayrton Moraes, Pablo Jorge Marcos-Pardo, Rodrigo Gomes de Souza Vale, Lucio Marques Vieira-Souza, Bruno de Freitas Camilo, and Estélio Henrique Martin-Dantas. 2022. "Resistance Circuit Training or Walking Training: Which Program Improves Muscle Strength and Functional Autonomy More in Older Women?" International Journal of Environmental Research and Public Health 19, no. 14: 8828. https://doi.org/10.3390/ijerph19148828