
Factors Influencing Self-Confidence and Willingness to Perform Cardiopulmonary Resuscitation among Working Adults—A Quasi-Experimental Study in a Training Environment

 ,
, 
 ,
, 
Abstract
:1. Introduction
2. Aims
- The influence on the ability to recognize the symptoms of SCA and perform correct chest compressions was analyzed in the context of the following factors:
- Previous participation in a first aid training in general;
- The time that has elapsed since previous first aid training;
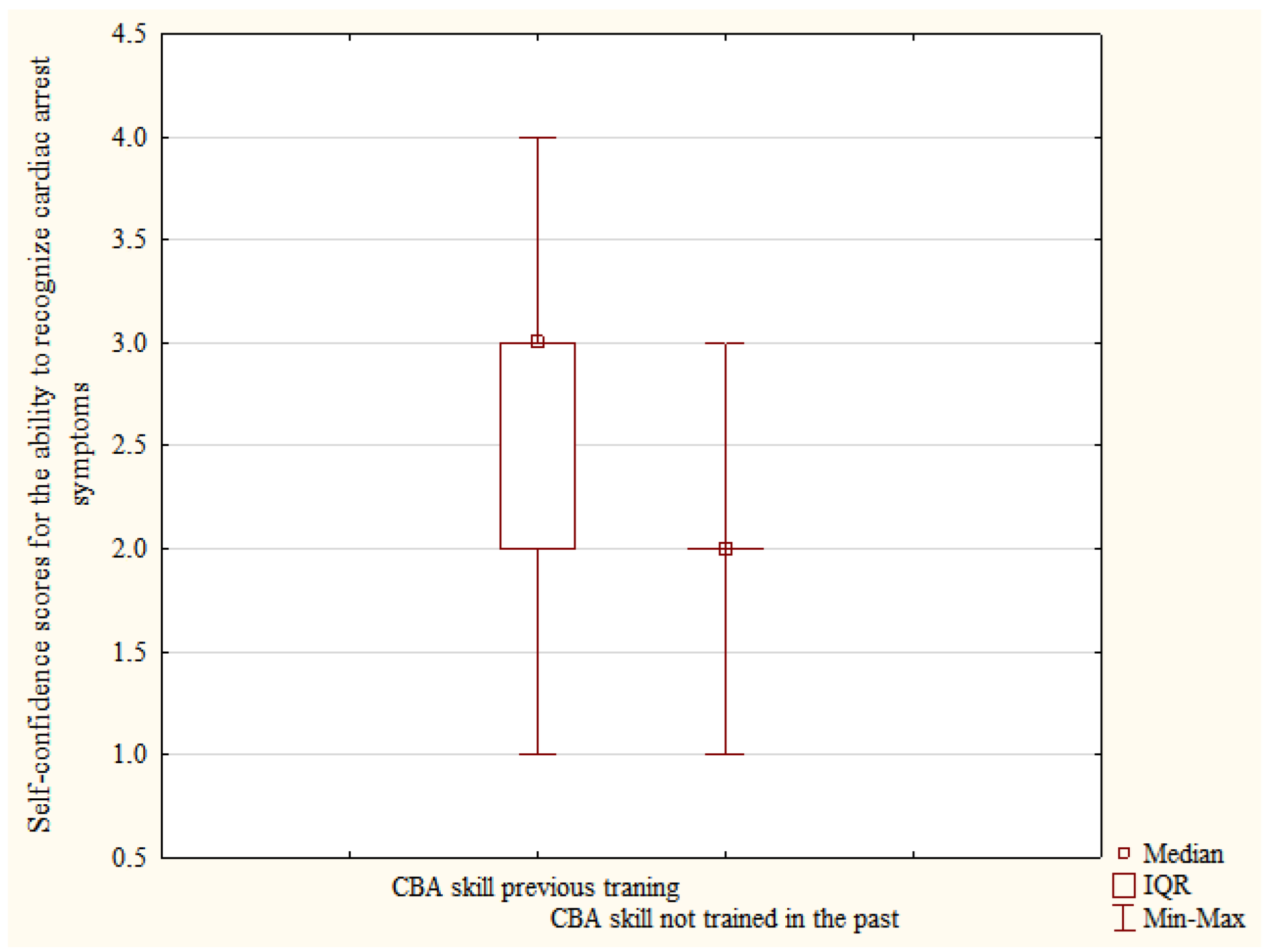
- Previous hands-on-training of checking for consciousness and the presence of normal breathing in the past (CBA skill: consciousness and breathing assessment);
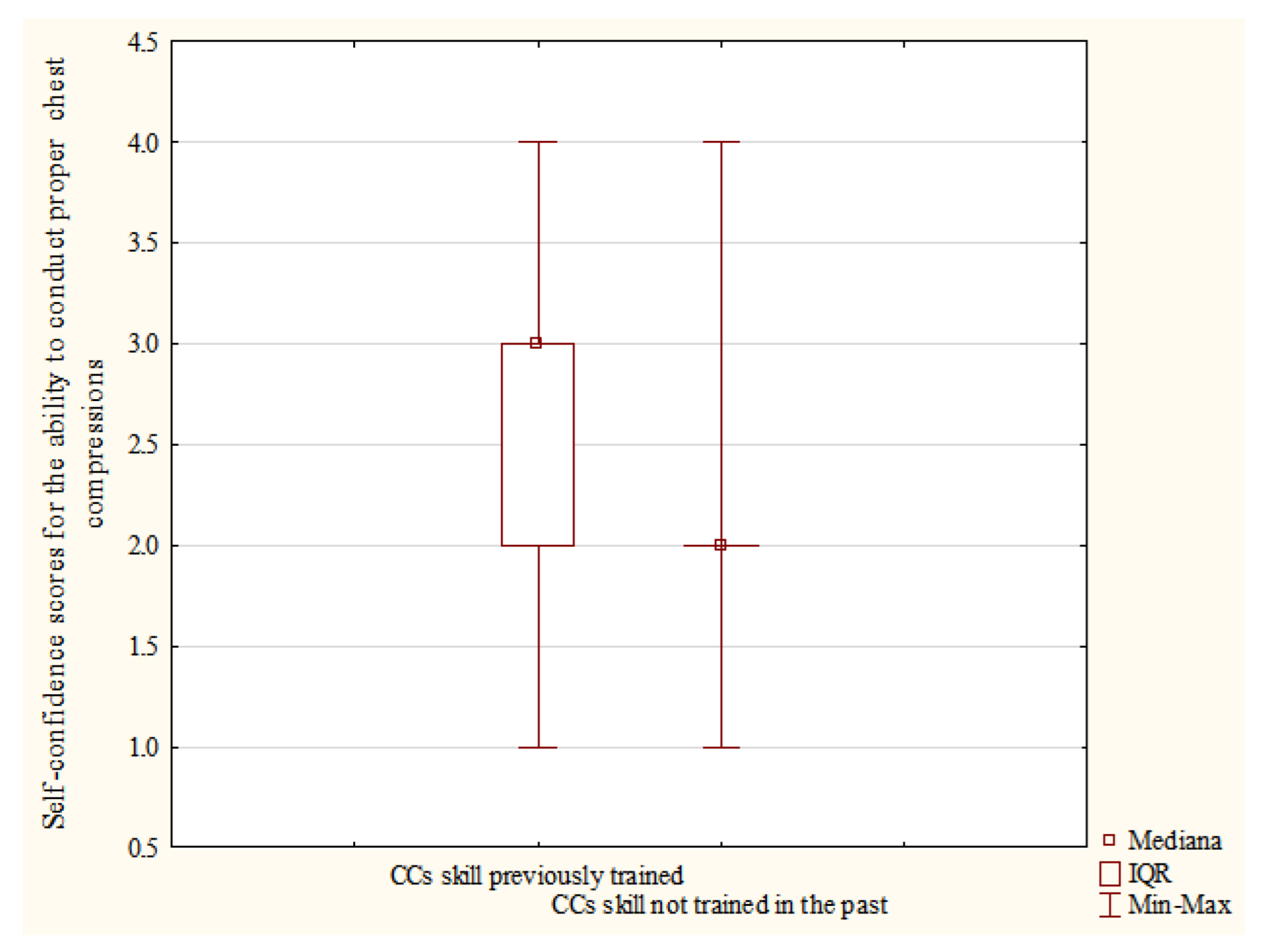
- Previous hands-on-training of chest compressions on a manikin (CCs skill: chest compressions);
- Completing the course in accordance with the planned methodology.
- Whether the willingness of participants to undertake resuscitation on individual victims depends on completing the course in accordance with the planned methodology;
- How the current training changes participants’ decision to undertake CPR on individual victims if previous training history is taken under consideration.
3. Materials and Methods
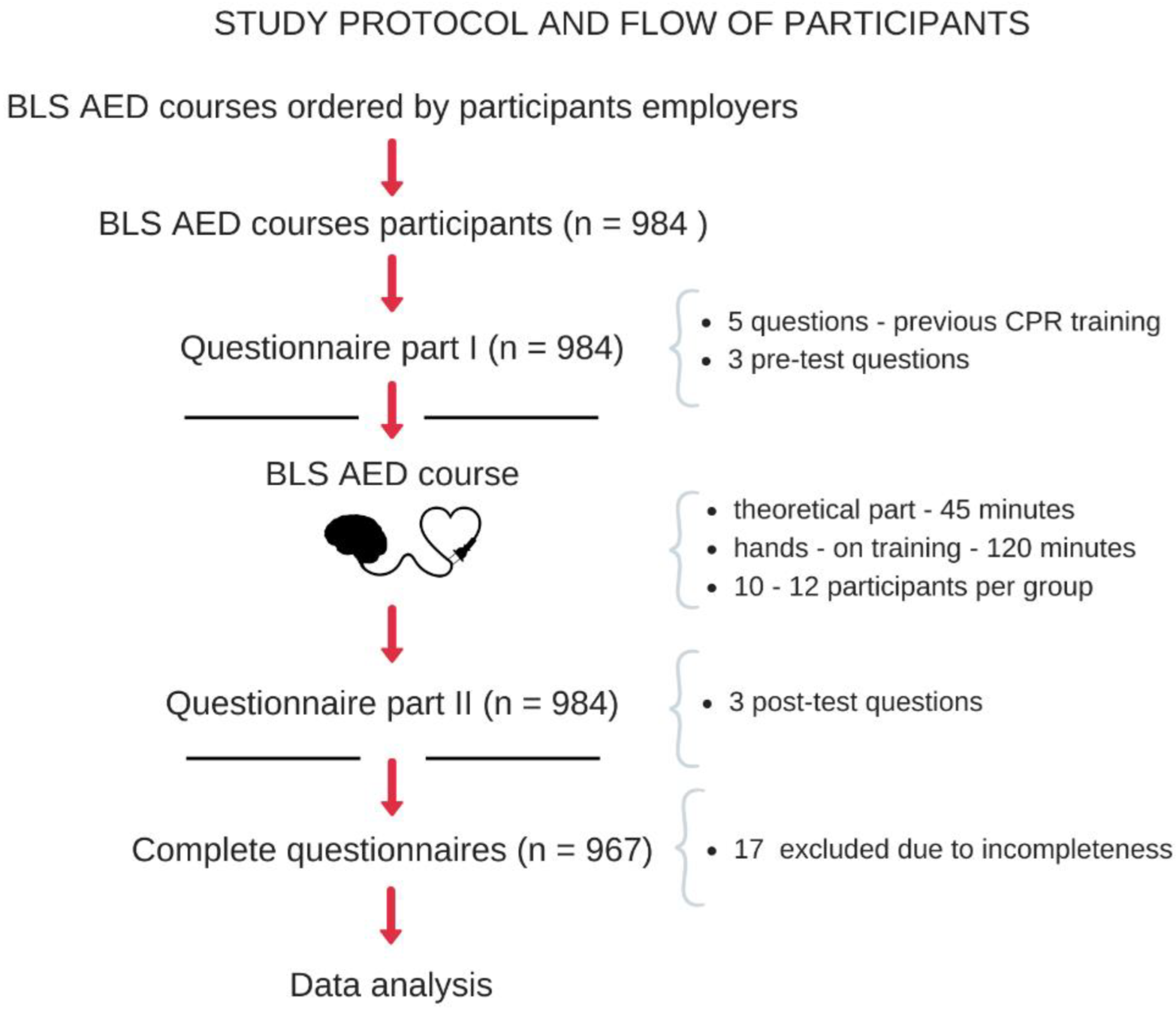
3.1. Study Design and Setting
3.2. Participants
3.3. Data Sources/Measurement
- Stage I.—Literature review to identify questions used in research on similar topics, including: literature reviews—total n = 6, (1 was rejected due to the lack of direct reference to the topic of the work); original articles, in total n = 51 (13 were rejected due to lack of direct reference to the topic of the work or to a very specific population); guidelines and international recommendations = 4—The International Liaison Committee On Resuscitation Education Implementation And Teams Task Force, American Heart Association and European Resuscitation Council Guidelines.
- Stage II.—Critical analysis of questions used in other researchers’ questionnaires and their verification in terms of consistency with the goals of the presented study.
- Stage III.—Creating a questionnaire appropriate to verify the chosen aims of the study.
- Stage IV.—Critical content evaluation by an experienced subject matter experts (n = 3)—removal of one question that was considered divergent from the chosen study aims; adding a question regarding the general characteristics of the group concerning the voivodeship of residence of the respondents.
- Stage V.—Presentation of the questionnaire in a pilot form to 30 respondents (debriefing respondents to obtain additional information about their views of the questions/concepts) participating in commercial resuscitation courses to evaluate the questionnaire in terms of whether:
- Closed questions provide at least one answer choice that would apply to every respondent;
- Questions were interpreted in the same manner by all the respondents;
- Answer choices to be selected correct;
- Questionnaire creates a positive impression, thus motivating people to respond to the question;
- Finally, whether any aspect of the questionnaire suggests any bias from the researcher.

3.4. Statistical Analysis
4. Results
5. Discussion
Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahnefeld, F.W.; Schröder, E. Preparations for disasters from a medical view (Rettungskette). Med. Hyg. 1966, 24, 1084. [Google Scholar]
- Newman, M.M. Chain of survival concept takes hold. J. Emerg. Med. Serv. 1989, 14, 11–13. [Google Scholar]
- Cummins, R.O.; Ornato, J.P.; Thies, W.H.; Pepe, P.E. Improving survival from sudden cardiac arrest: The “chain of survival” concept. A statement for health professionals from the Advanced Cardiac Life Support Subcommittee and the Emergency Cardiac Care Committee, American Heart Association. Circulation 1991, 83, 1832–1847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S366–S468. [Google Scholar] [CrossRef] [PubMed]
- Olasveengen, T.M.; Semeraro, F.; Ristagno, G.; Castren, M.; Handley, A.; Kuzovlev, A.; Monsieurs, K.G.; Raffay, V.; Smyth, M.; Soar, J.; et al. European Resuscitation Council Guidelines 2021: Basic Life Support. Resuscitation 2021, 161, 98–114. [Google Scholar] [CrossRef] [PubMed]
- Gräsner, J.-T.; Herlitz, J.; Tjelmeland, I.B.; Wnent, J.; Masterson, S.; Lilja, G.; Bein, B.; Böttiger, B.W.; Rosell-Ortiz, F.; Nolan, J.P.; et al. European Resuscitation Council Guidelines 2021: Epidemiology of cardiac arrest in Europe. Resuscitation 2021, 161, 61–79. [Google Scholar] [CrossRef]
- Park, H.J.; Jeong, W.J.; Moon, H.J.; Kim, G.W.; Cho, J.S.; Lee, K.M.; Choi, H.J.; Park, Y.J.; Lee, C.A. Factors Associated with High-Quality Cardiopulmonary Resuscitation Performed by Bystander. Emerg. Med. Int. 2020, 2020, 8356201. [Google Scholar] [CrossRef]
- Shimamoto, T.; Kiyohara, K.; Matsuyama, T.; Kitamura, T.; Kiguchi, T.; Nishiyama, C.; Kobayashi, D.; Okabayashi, S.; Kawamura, T.; Iwami, T. Impact of Bystander Cardiopulmonary Resuscitation and Dispatcher Assistance on Survival After Out-of-Hospital Cardiac Arrest Among Adult Patients by Location of Arrest. Int. Heart J. 2020, 61, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Guo, W.; Lu, X.; Kang, X.; Song, Y.; Gong, D. The effect of bystander cardiopulmonary resuscitation on the survival of out-of-hospital cardiac arrests: A systematic review and meta-analysis. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 86. [Google Scholar] [CrossRef]
- Scapigliati, A.; Zace, D.; Matsuyama, T.; Pisapia, L.; Saviani, M.; Semeraro, F.; Ristagno, G.; Laurenti, P.; Bray, J.E.; Greif, R.; et al. Community Initiatives to Promote Basic Life Support Implementation—A Scoping Review. J. Clin. Med. 2021, 10, 5719. [Google Scholar] [CrossRef]
- Greif, R.; Lockey, A.; Breckwoldt, J.; Carmona, F.; Conaghan, P.; Kuzovlev, A.; Pflanzl-Knizacek, L.; Sari, F.; Shammet, S.; Scapigliati, A.; et al. European Resuscitation Council Guidelines 2021: Education for resuscitation. Resuscitation 2021, 161, 388–407. [Google Scholar] [CrossRef] [PubMed]
- Greif, R.; Bhanji, F.; Bigham, B.L.; Bray, J.; Breckwoldt, J.; Cheng, A.; Duff, J.P.; Gilfoyle, E.; Hsieh, M.-J.; Iwami, T.; et al. Ducation, implementation, and teams: 2020 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation 2020, 156, A188–A239. [Google Scholar] [CrossRef] [PubMed]
- Case, R.; Cartledge, S.; Siedenburg, J.; Smith, K.; Straney, L.; Barger, B.; Finn, J.; Bray, J.E. Identifying barriers to the provision of bystander cardiopulmonary resuscitation (CPR) in high-risk regions: A qualitative review of emergency calls. Resuscitation 2018, 129, 43–47. [Google Scholar] [CrossRef]
- Blewer, A.L.; McGovern, S.K.; Schmicker, R.H.; May, S.; Morrison, L.J.; Aufderheide, T.P.; Daya, M.; Idris, A.H.; Callaway, C.W.; Kudenchuk, P.J.; et al. Gender Disparities Among Adult Recipients of Bystander Cardiopulmonary Resuscitation in the Public. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004710. [Google Scholar] [CrossRef]
- Matsuyama, T.; Okubo, M.; Kiyohara, K.; Kiguchi, T.; Kobayashi, D.; Nishiyama, C.; Okabayashi, S.; Shimamoto, T.; Izawa, J.; Komukai, S.; et al. Sex-Based Disparities in Receiving Bystander Car-diopulmonary Resuscitation by Location of Cardiac Arrest in Japan. Mayo Clin. Proc. 2019, 94, 577–587. [Google Scholar] [CrossRef]
- Matsui, S.; Kitamura, T.; Kiyohara, K.; Sado, J.; Ayusawa, M.; Nitta, M.; Iwami, T.; Nakata, K.; Kitamura, Y.; Sobue, T.; et al. Sex Disparities in Receipt of Bystander Interventions for Students Who Experienced Cardiac Arrest in Japan. JAMA Netw. Open 2019, 2, e195111. [Google Scholar] [CrossRef]
- Dahan, B.; Jabre, P.; Karam, N.; Misslin, R.; Tafflet, M.; Bougouin, W.; Jost, D.; Beganton, F.; Marijon, E.; Jouven, X. Impact of neighbourhood socio-economic status on bystander cardiopulmonary resuscitation in Paris. Resuscitation 2016, 110, 107–113. [Google Scholar] [CrossRef]
- Langlais, B.T.; Panczyk, M.; Sutter, J.; Fukushima, H.; Wu, Z.; Iwami, T.; Spaite, D.; Bobrow, B. Barriers to patient positioning for telephone cardiopulmonary resuscitation in out-of-hospital cardiac arrest. Resuscitation 2017, 115, 163–168. [Google Scholar] [CrossRef]
- Matsuyama, T.; Scapigliati, A.; Pellis, T.; Greif, R.; Iwami, T. Willingness to perform bystander cardiopulmonary resuscitation: A scoping review. Resusc. Plus 2020, 4, 100043. [Google Scholar] [CrossRef]
- Ro, Y.S.; Shin, S.D.; Song, K.J.; Hong, S.O.; Kim, Y.T.; Lee, D.-W.; Cho, S.-I. Public awareness and self-efficacy of cardiopulmonary resuscitation in communities and outcomes of out-of-hospital cardiac arrest: A multi-level analysis. Resuscitation 2016, 102, 17–24. [Google Scholar] [CrossRef]
- Nishiyama, C.; Sato, R.; Baba, M.; Kuroki, H.; Kawamura, T.; Kiguchi, T.; Kobayashi, D.; Shimamoto, T.; Koike, K.; Tanaka, S.; et al. Actual resuscitation actions after the training of chest compression-only CPR and AED use among new university students. Resuscitation 2019, 141, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Huang, E.P.-C.; Chiang, W.-C.; Hsieh, M.-J.; Wang, H.-C.; Yang, C.-W.; Lu, T.-C.; Wang, C.-H.; Chong, K.-M.; Lin, C.-H.; Kuo, C.-W.; et al. Public knowledge, attitudes and willingness regarding bystander cardiopulmonary resuscitation: A nationwide survey in Taiwan. J. Formos. Med. Assoc. 2018, 118, 572–581. [Google Scholar] [CrossRef]
- Yan, S.; Gan, Y.; Wang, R.; Song, X.; Zhou, N.; Lv, C. Willingness to attend cardiopulmonary resuscitation training and the associated factors among adults in China. Crit. Care 2020, 24, 457. [Google Scholar] [CrossRef] [PubMed]
- Birkun, A.; Kosova, Y. Social attitude and willingness to attend cardiopulmonary resuscitation training and perform resuscitation in the Crimea. World J. Emerg. Med. 2018, 9, 237–248. [Google Scholar] [CrossRef]
- Pivač, S.; Gradišek, P.; Skela-Savič, B. The impact of cardiopulmonary resuscitation (CPR) training on schoolchildren and their CPR knowledge, attitudes toward CPR, and willingness to help others and to perform CPR: Mixed methods research design. BMC Public Health 2020, 20, 915. [Google Scholar] [CrossRef] [PubMed]
- Abelsson, A.; Odestrand, P.; Nygårdh, A. To strengthen self-confidence as a step in improving prehospital youth laymen basic life support. BMC Emerg. Med. 2020, 20, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moriwaki, Y.; Tahara, Y.; Iwashita, M.; Kosuge, T.; Suzuki, N. Risky locations for out-of-hospital cardiopulmonary arrest in a typical urban city. J. Emergencies Trauma Shock 2014, 7, 285–294. [Google Scholar] [CrossRef]
- Bylow, H.; Rawshani, A.; Claesson, A.; Lepp, M.; Herlitz, J. Characteristics and outcome after out-of-hospital cardiac arrest with the emphasis on workplaces: An observational study from the Swedish Registry of Cardiopulmonary Resuscitation. Resusc. Plus 2021, 5, 100090. [Google Scholar] [CrossRef]
- Descatha, A.; Dumas, F.; Bougouin, W.; Cariou, A.; Geri, G. Work factors associated with return to work in out-of-hospital cardiac arrest survivors. Resuscitation 2018, 128, 170–174. [Google Scholar] [CrossRef]
- Descatha, A.; Dagrenat, C.; Cassan, P.; Jost, D.; Loeb, T.; Baer, M. Cardiac arrest in the workplace and its outcome: A systematic review and meta-analysis. Resuscitation 2015, 96, 30–36. [Google Scholar] [CrossRef]
- Shibahashi, K.; Sugiyama, K.; Kuwahara, Y.; Ishida, T.; Sakurai, A.; Kitamura, N.; Tagami, T.; Nakada, T.-A.; Takeda, M.; Hamabe, Y. Private residence as a location of cardiac arrest may have a deleterious effect on the outcomes of out-of-hospital cardiac arrest in patients with an initial non-shockable cardiac rhythm: A multicentre retrospective cohort study. Resuscitation 2020, 150, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Marino, R.; Bertocci, N.; Bernabei, M.; Bonotti, A.; Mignani, A.; Fallahi, P.; Perretta, S.; Monopoli, G.; Cristaudo, A.; Foddis, R. Analysis of survival at cardiac arrest in events occurred in work environments in the territory served by an operations center of the 118 of Tuscany. Med. Lav. 2020, 111, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Wu, B.; Long, L.; Li, J.; Jin, X. Attitudes and willingness toward out-of-hospital cardiopulmonary resuscitation: A questionnaire study among the public trained online in China. BMJ Open 2020, 10, e038712. [Google Scholar] [CrossRef] [PubMed]
- Andréll, C.; Christensson, C.; Rehn, L.; Friberg, H.; Dankiewicz, J. Knowledge and attitudes to cardiopulmonary resuscitation (CPR)–A cross-sectional population survey in Sweden. Resusc. Plus 2021, 5, 100071. [Google Scholar] [CrossRef] [PubMed]
- Luiz, T.; Dittrich, S.; Pollach, G.; Madler, C. Knowledge of the population about leading symptoms of cardiovascular emergencies and the responsibility and accessibility of medical facilities in emergencies: Results of the KZEN study in Western Palatinate. Der Anaesthesist 2017, 66, 840–849. [Google Scholar] [CrossRef]
- Bakke, H.K.; Steinvik, T.; Angell, J.; Wisborg, T. A nationwide survey of first aid training and encounters in Norway. BMC Emerg. Med. 2016, 17, 6. [Google Scholar] [CrossRef] [Green Version]
- Panchal, A.R.; Fishman, J.; Camp-Rogers, T.; Starodub, R.; Merchant, R.M. An “Intention-Focused” paradigm for improving bystander CPR performance. Resuscitation 2014, 88, 48–51. [Google Scholar] [CrossRef] [Green Version]
- Fratta, K.A.; Bouland, A.J.; Vesselinov, R.; Levy, M.J.; Seaman, K.G.; Lawner, B.J.; Hirshon, J.M. Evaluating barriers to community CPR education. Am. J. Emerg. Med. 2020, 38, 603–609. [Google Scholar] [CrossRef]
- Bouland, A.J.; Halliday, M.H.; Comer, A.C.; Levy, M.J.; Seaman, K.G.; Lawner, B.J. Evaluating Barriers to Bystander CPR among Laypersons before and after Compression-only CPR Training. Prehospital Emerg. Care 2017, 21, 662–669. [Google Scholar] [CrossRef]
- González-Salvado, V.; Rodríguez-Ruiz, E.; Abelairas-Gómez, C.; Ruano-Raviña, A.; Peña-Gil, C.; González-Juanatey, J.R.; Rodríguez-Núñez, A. Training adult laypeople in basic life support. A systematic review. Rev. Esp. Cardiol. 2019, 73, 53–68. [Google Scholar] [CrossRef]
- Chen, M.; Wang, Y.; Li, X.; Hou, L.; Wang, Y.; Liu, J.; Han, F. Public Knowledge and Attitudes towards Bystander Cardiopulmonary Resuscitation in China. BioMed Res. Int. 2017, 2017, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, I.; Kwak, Y.H.; Shin, S.D.; Ro, Y.S.; Kim, D.K. Characteristics of bystander cardiopulmonary resuscitation for paediatric out-of-hospital cardiac arrests: A national observational study from 2012 to 2014. Resuscitation 2016, 111, 26–33. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Participation in First Aid Course in the Past | Yes, <1 Year | Yes, 1–2 Years | Yes, >2 years | No Never |
|---|---|---|---|---|
| n = 220 | n = 105 | n = 408 | n = 235 | |
| PRE-TEST Recognizing the symptoms of cardiac arrest? (Scale: 1-not able, 2-not sure, 3-able, 4-definitely able) | Me, [IQR] | |||
| 2.8, [3–3] | 2.3 [2–3] | 2.3, [2–3] | 1,8, [1–2] | |
| p-value | 0.000 | |||
| Participation in the First Aid Course in the Past | Yes, <1 year | Yes, 1–2 years | Yes, >2 years | No, Never |
|---|---|---|---|---|
| n = 220 | n = 105 | n = 408 | n = 235 | |
| PRE-TEST Conducting proper chest compressions? (Scale: 1-not able, 2-not sure, 3-able, 4-definitely able) | Me, [IQR] | |||
| 3.1, [3–3] | 2.4, [2–2] | 2.3, [2–3] | 1.6, [1–2] | |
| p value | 0.000 | |||
| Victim Characteristic | Pre-Test, (%) | Post-Test, n (%) | p Value |
|---|---|---|---|
| Family member | 911 (94.2) | 933 (96.5) | 0.015 |
| Child | 833 (86.1) | 903 (93.4) | 0.000 |
| Person you know | 887 (91.7) | 927 (95.9) | <0.001 |
| Stranger | 723 (74.8) | 883 (91.3) | 0.000 |
| Victim Characteristic and Previous Training History | OR | −95%CI | +95 CI | p Value |
|---|---|---|---|---|
| Family member | ||||
| Regardless of training history | 2.1 | 1.23 | 3.58 | 0.007 |
| No never | 4 | 0.85 | 18.84 | 0.113 |
| Yes, <1 year | 0.8 | 0.32 | 2.03 | 0.813 |
| Yes, 1–2 years | 3 | 0.61 | 14.86 | 0.289 |
| Yes, >2 years | 3.33 | 1.34 | 8.3 | 0.010 |
| Child | ||||
| Regardless of training history | 4.5 | 2.77 | 7.31 | <0.001 |
| No never | 7.5 | 2.64 | 21.29 | <0.001 |
| Yes, <1 year | 1.6 | 0.73 | 3.53 | 0.326 |
| Yes, 1–2 years | 4 | 0.85 | 18.84 | 0.113 |
| Yes, >2 years | 9 | 3.2 | 25.29 | <0.001 |
| Person you know | ||||
| Regardless of training history | 3.22 | 1.9 | 5.47 | <0.001 |
| No never | NA | NA | NA | <0.001 |
| Yes, <1 year | 1 | 0.45 | 2.23 | 0.838 |
| Yes, 1–2 years | 4 | 0.85 | 18.84 | 0.113 |
| Yes, >2 years | 6 | 2.08 | 17.29 | <0.001 |
| Stranger | ||||
| Regardless of training history | 7.67 | 5.01 | 11.73 | <0.001 |
| No never | 27 | 6.58 | 110.74 | <0.001 |
| Yes, <1 year | 1.63 | 0.87 | 3.03 | 0.164 |
| Yes, 1–2 years | 7 | 1.59 | 30.08 | 0.006 |
| Yes, >2 years | 22.5 | 8.26 | 61.25 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaskiewicz, F.; Kowalewski, D.; Kaniecka, E.; Kozlowski, R.; Marczak, M.; Timler, D. Factors Influencing Self-Confidence and Willingness to Perform Cardiopulmonary Resuscitation among Working Adults—A Quasi-Experimental Study in a Training Environment. Int. J. Environ. Res. Public Health 2022, 19, 8334. https://doi.org/10.3390/ijerph19148334
Jaskiewicz F, Kowalewski D, Kaniecka E, Kozlowski R, Marczak M, Timler D. Factors Influencing Self-Confidence and Willingness to Perform Cardiopulmonary Resuscitation among Working Adults—A Quasi-Experimental Study in a Training Environment. International Journal of Environmental Research and Public Health. 2022; 19(14):8334. https://doi.org/10.3390/ijerph19148334
Chicago/Turabian StyleJaskiewicz, Filip, Dawid Kowalewski, Ewa Kaniecka, Remigiusz Kozlowski, Michal Marczak, and Dariusz Timler. 2022. "Factors Influencing Self-Confidence and Willingness to Perform Cardiopulmonary Resuscitation among Working Adults—A Quasi-Experimental Study in a Training Environment" International Journal of Environmental Research and Public Health 19, no. 14: 8334. https://doi.org/10.3390/ijerph19148334