
Associations between Lifestyle Changes and Adherence to COVID-19 Restrictions in Older Adults with Hypertension

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Demographic and Clinical Indicators
2.3. Physical Activity
2.4. Diet
2.5. Alcohol Consumption
2.6. Cigarette Smoking
2.7. Adherence to Behavioral Indications and National Restrictions
2.8. Statistical Analyses
3. Results
3.1. Preliminary Analyses: Lifestyles Stability during the Prepandemic Period
3.2. Participants’ Health Condition
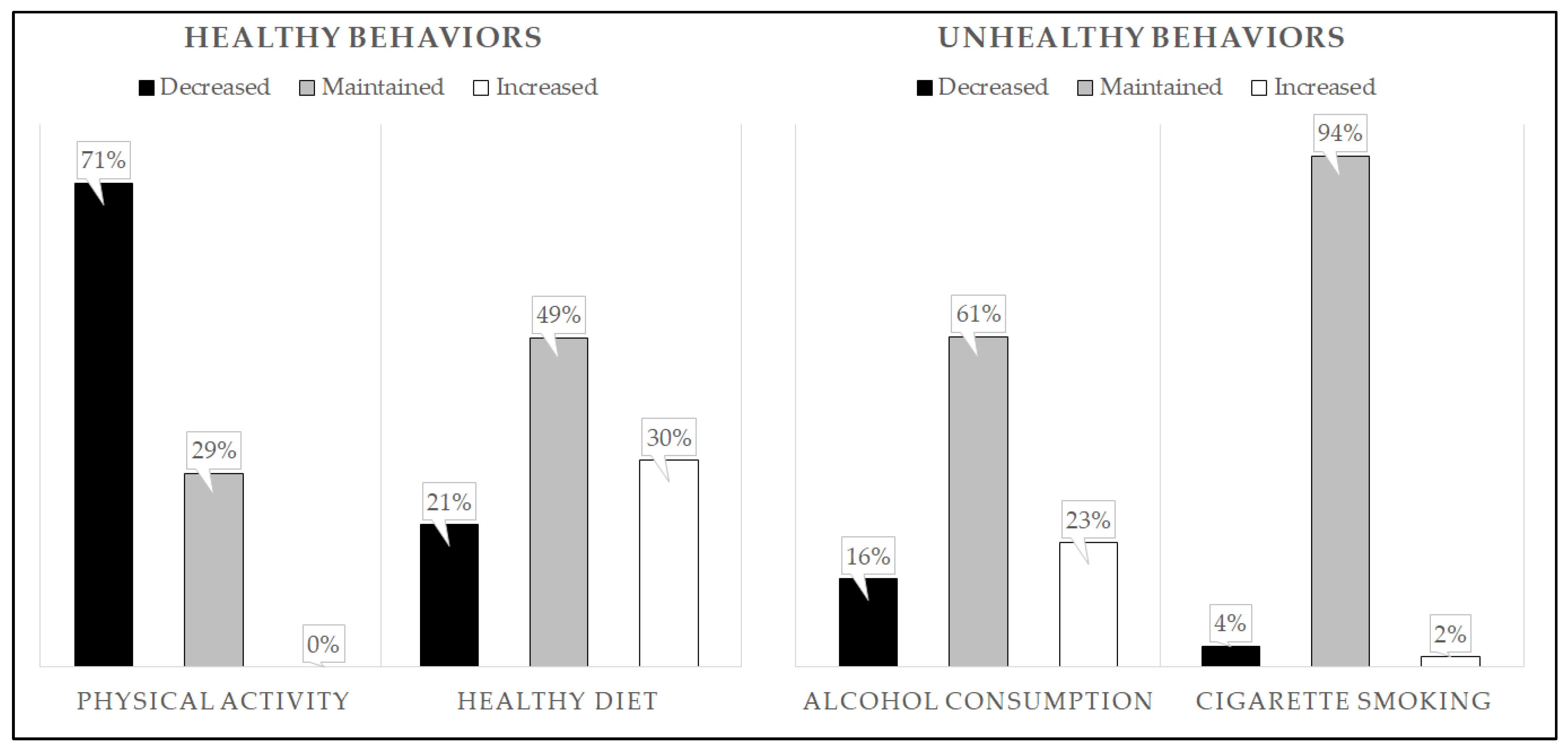
3.3. Lifestyles Change
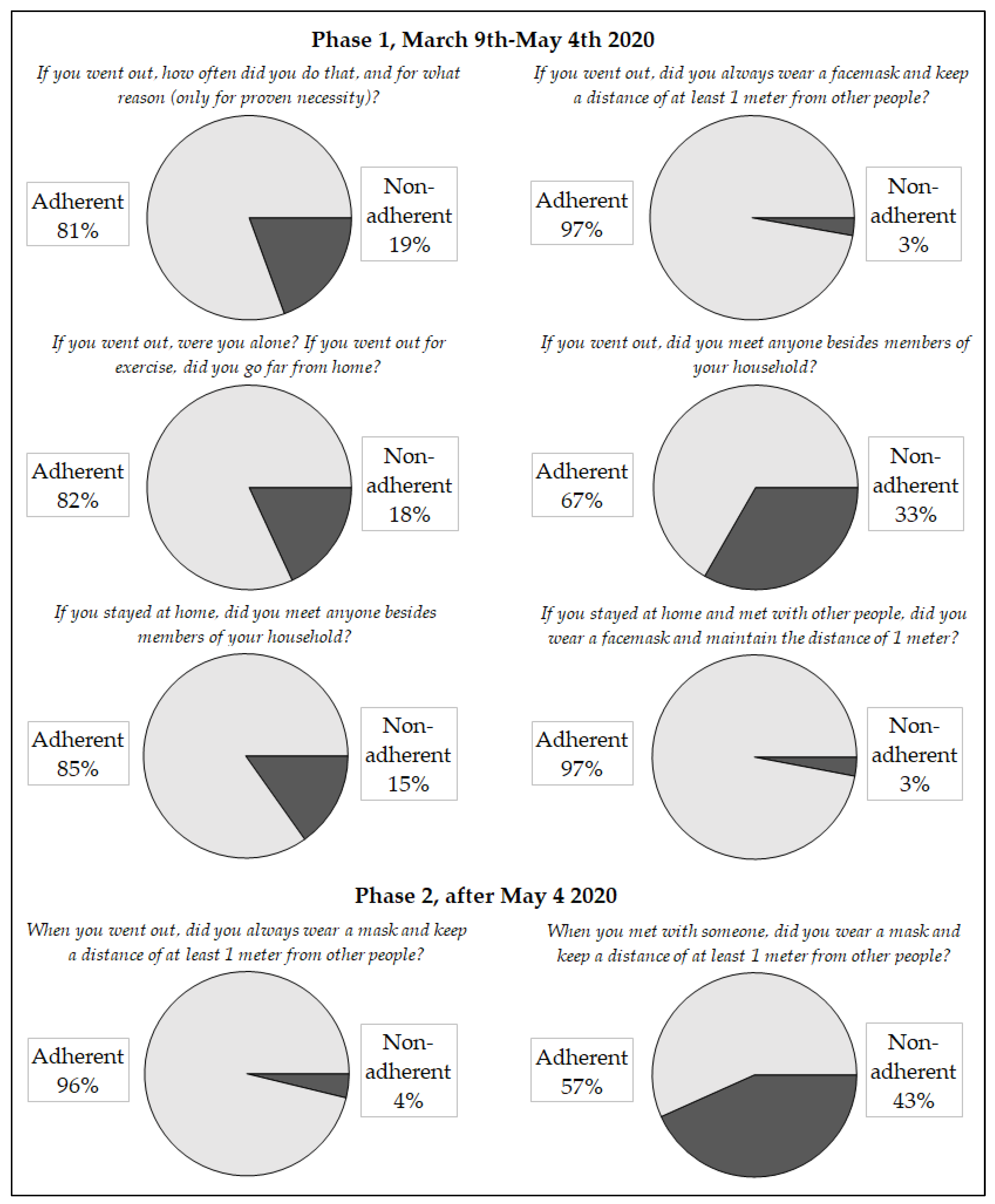
3.4. Adherence to Government Restrictions
3.5. Prediction of Adherence to Restrictions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Domain of Investigation | Specific Questions |
| General health information | How is your health in general? (Coded on a 5-point Likert scale) Have you developed any other cardiovascular or other diseases since we last spoke? (Interviewer annotated which one and when) |
| Lifestyle changes | Have you struggled to maintain healthy habits in the past few months? (Interviewer collected information about physical activity, diet, alcohol consumption, and smoke) |
| COVID information | Have you ever tested positive for the virus? If so, the interviewer asked how he/she found out, if he/she had been hospitalized and for how long, and how long the illness had lasted overall. Has anyone close to you tested positive for the virus? Who? |
| Adherence to national restrictions during phase 1 (from 9 March to 4 May 2020) | If you went out, how often did you do that, and why? If you went out, did you always wear a facemask, and did you always keep a distance of at least 1 m from other people? If you went out, were you alone? If you went out for exercise, did you go far from home? If you went out, did you meet anyone besides members of your household? If you stayed at home, did you meet anyone besides members of your household? If you stayed at home and met other people, did you always wear a facemask and maintain a minimum distance of 1 m from them? |
| Adherence to national restrictions during phase 2 (after 4 May 2020) | When you met someone, did you always wear a mask, and keep a distance of at least 1 m from other people? When you went out, did you always wear a mask, and keep a distance of at least 1 m from other people? |
Appendix B
| Lifestyle | Baseline Mean (SD) | 6-Months Mean (SD) | 12-Months Mean (SD) | 24-Months Mean (SD) | 36-Months Mean (SD) | F | p |
| Physical Activity | 4.71 (1.80) | 4.58 (1.50) | 4.84 (1.49) | 4.71 (1.74) | 4.76 (2.00) | 0.38 | 0.79 |
| Diet | 1.31 (0.79) | 1.38 (0.62) | 1.42 (0.74) | 1.26 (0.70) | 1.31 (0.81) | 0.93 | 0.43 |
| Alcohol Consumption | 2.15 (0.73) | 2.25 (0.70) | 2.16 (0.69) | 2.31 (0.61) | 2.07 (0.80) | 3.43 | 0.01 |
| Cigarette Smoking | 4.16 (1.30) | 4.15 (1.30) | 4.15 (1.30) | 4.24 (1.15) | 4.36 (1.00) | 3.00 | 0.06 |
Appendix C

References
- Coronavirus Disease (COVID-19)–World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 24 March 2022).
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What Next? Lancet Lond. Engl. 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Lim, J.M.; Tun, Z.M.; Kumar, V.; Quaye, S.E.D.; Offeddu, V.; Cook, A.R.; Lwin, M.O.; Jiang, S.; Tam, C.C. Population Anxiety and Positive Behaviour Change during the COVID-19 Epidemic: Cross-sectional Surveys in Singapore, China and Italy. Influenza Other Respir. Viruses 2021, 15, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Gazzetta Ufficiale. Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/09/20A01558/sg (accessed on 24 March 2022).
- Degli Esposti, L.; Buda, S.; Nappi, C.; Paoli, D.; Perrone, V. Implications of COVID-19 Infection on Medication Adherence with Chronic Therapies in Italy: A Proposed Observational Investigation by the Fail-to-Refill Project. Risk Manag. Healthc. Policy 2020, 13, 3179–3185. [Google Scholar] [CrossRef] [PubMed]
- Gazzetta Ufficiale. Available online: https://www.gazzettaufficiale.it/eli/id/2020/04/27/20A02352/sg (accessed on 24 March 2022).
- Nochaiwong, S.; Ruengorn, C.; Thavorn, K.; Hutton, B.; Awiphan, R.; Phosuya, C.; Ruanta, Y.; Wongpakaran, N.; Wongpakaran, T. Global Prevalence of Mental Health Issues among the General Population during the Coronavirus Disease-2019 Pandemic: A Systematic Review and Meta-Analysis. Sci. Rep. 2021, 11, 10173. [Google Scholar] [CrossRef] [PubMed]
- Bailey, B.; Whelen, M.L.; Strunk, D.R. Adhering to COVID-19 Health Guidelines: Examining Demographic and Psychological Predictors of Adherence. Appl. Psychol. Health Well-Being 2021, 13, 968–985. [Google Scholar] [CrossRef]
- Qeadan, F.; Akofua Mensah, N.; Tingey, B.; Bern, R.; Rees, T.; Talboys, S.; Pal Singh, T.; Lacey, S.; Shoaf, K. What Protective Health Measures Are Americans Taking in Response to COVID-19? Results from the COVID Impact Survey. Int. J. Environ. Res. Public Health 2020, 17, 6295. [Google Scholar] [CrossRef]
- Carlucci, L.; D’Ambrosio, I.; Balsamo, M. Demographic and Attitudinal Factors of Adherence to Quarantine Guidelines During COVID-19: The Italian Model. Front. Psychol. 2020, 11, 559288. [Google Scholar] [CrossRef]
- Moran, C.; Campbell, D.J.T.; Campbell, T.S.; Roach, P.; Bourassa, L.; Collins, Z.; Stasiewicz, M.; McLane, P. Predictors of Attitudes and Adherence to COVID-19 Public Health Guidelines in Western Countries: A Rapid Review of the Emerging Literature. J. Public Health Oxf. Engl. 2021, 43, 739–753. [Google Scholar] [CrossRef]
- Smith, L.E.; Amlȏt, R.; Lambert, H.; Oliver, I.; Robin, C.; Yardley, L.; Rubin, G.J. Factors Associated with Adherence to Self-Isolation and Lockdown Measures in the UK: A Cross-Sectional Survey. Public Health 2020, 187, 41–52. [Google Scholar] [CrossRef]
- Szwarcwald, C.L.; de Souza Júnior, P.R.B.; Malta, D.C.; de Azevedo Barros, M.B.; de Avelar Figueiredo Mafra Magalhães, M.; Xavier, D.R.; de Freitas Saldanha, R.; Damacena, G.N.; Azevedo, L.O.; Lima, M.G.; et al. Adherence to Physical Contact Restriction Measures and the Spread of COVID-19 in Brazil. Epidemiol. E Serviços Saúde 2020, 29, e2020432. [Google Scholar] [CrossRef]
- Coroiu, A.; Moran, C.; Campbell, T.; Geller, A.C. Barriers and Facilitators of Adherence to Social Distancing Recommendations during COVID-19 among a Large International Sample of Adults. PLoS ONE 2020, 15, e0239795. [Google Scholar] [CrossRef] [PubMed]
- Reinders Folmer, C.P.; Brownlee, M.A.; Fine, A.D.; Kooistra, E.B.; Kuiper, M.E.; Olthuis, E.H.; de Bruijn, A.L.; van Rooij, B. Social Distancing in America: Understanding Long-Term Adherence to COVID-19 Mitigation Recommendations. PLoS ONE 2021, 16, e0257945. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in Physical Activity and Sedentary Behaviours from before to during the COVID-19 Pandemic Lockdown: A Systematic Review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef] [PubMed]
- Rossi, L.; Behme, N.; Breuer, C. Physical Activity of Children and Adolescents during the COVID-19 Pandemic—A Scoping Review. Int. J. Environ. Res. Public. Health 2021, 18, 11440. [Google Scholar] [CrossRef] [PubMed]
- López-Valenciano, A.; Suárez-Iglesias, D.; Sanchez-Lastra, M.A.; Ayán, C. Impact of COVID-19 Pandemic on University Students’ Physical Activity Levels: An Early Systematic Review. Front. Psychol. 2021, 11, 624567. [Google Scholar] [CrossRef]
- Wunsch, K.; Kienberger, K.; Niessner, C. Changes in Physical Activity Patterns Due to the Covid-19 Pandemic: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public. Health 2022, 19, 2250. [Google Scholar] [CrossRef]
- González-Monroy, C.; Gómez-Gómez, I.; Olarte-Sánchez, C.M.; Motrico, E. Eating Behaviour Changes during the COVID-19 Pandemic: A Systematic Review of Longitudinal Studies. Int. J. Environ. Res. Public. Health 2021, 18, 11130. [Google Scholar] [CrossRef]
- Mignogna, C.; Costanzo, S.; Ghulam, A.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; Bonaccio, M. Impact of Nationwide Lockdowns Resulting from the First Wave of the COVID-19 Pandemic on Food Intake, Eating Behaviors, and Diet Quality: A Systematic Review. Adv. Nutr. 2021, 13, 388–423. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Vanderbruggen, N.; Matthys, F.; Van Laere, S.; Zeeuws, D.; Santermans, L.; Van den Ameele, S.; Crunelle, C.L. Self-Reported Alcohol, Tobacco, and Cannabis Use during COVID-19 Lockdown Measures: Results from a Web-Based Survey. Eur. Addict. Res. 2020, 26, 309–315. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating Habits and Lifestyle Changes during COVID-19 Lockdown: An Italian Survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Gallè, F.; Sabella, E.A.; Roma, P.; Ferracuti, S.; Da Molin, G.; Diella, G.; Montagna, M.T.; Orsi, G.B.; Liguori, G.; Napoli, C. Knowledge and Lifestyle Behaviors Related to COVID-19 Pandemic in People over 65 Years Old from Southern Italy. Int. J. Environ. Res. Public. Health 2021, 18, 10872. [Google Scholar] [CrossRef] [PubMed]
- Andualem, A.; Gelaye, H.; Damtie, Y. Adherence to Lifestyle Modifications and Associated Factors Among Adult Hypertensive Patients Attending Chronic Follow-Up Units of Dessie Referral Hospital, North East Ethiopia, 2020. Integr. Blood Press. Control 2020, 13, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Cransac-Miet, A.; Zeller, M.; Chagué, F.; Faure, A.S.; Bichat, F.; Danchin, N.; Boulin, M.; Cottin, Y. Impact of COVID-19 Lockdown on Lifestyle Adherence in Stay-at-Home Patients with Chronic Coronary Syndromes: Towards a Time Bomb. Int. J. Cardiol. 2021, 323, 285–287. [Google Scholar] [CrossRef]
- Mattioli, A.V.; Ballerini Puviani, M. Lifestyle at Time of COVID-19: How Could Quarantine Affect Cardiovascular Risk. Am. J. Lifestyle Med. 2020, 14, 240–242. [Google Scholar] [CrossRef]
- de Vries, H.; van ’t Riet, J.; Spigt, M.; Metsemakers, J.; van den Akker, M.; Vermunt, J.K.; Kremers, S. Clusters of Lifestyle Behaviors: Results from the Dutch SMILE Study. Prev. Med. 2008, 46, 203–208. [Google Scholar] [CrossRef]
- Steca, P.; Monzani, D.; Greco, A.; Franzelli, C.; Magrin, M.E.; Miglioretti, M.; Sarini, M.; Scrignaro, M.; Vecchio, L.; Fattirolli, F.; et al. Stability and Change of Lifestyle Profiles in Cardiovascular Patients after Their First Acute Coronary Event. PLoS ONE 2017, 12, e0183905. [Google Scholar] [CrossRef] [Green Version]
- Nudelman, G.; Peleg, S.; Shiloh, S. The Association Between Healthy Lifestyle Behaviours and Coronavirus Protective Behaviours. Int. J. Behav. Med. 2021, 28, 779–787. [Google Scholar] [CrossRef]
- Berg-Beckhoff, G.; Dalgaard Guldager, J.; Tanggaard Andersen, P.; Stock, C.; Smith Jervelund, S. What Predicts Adherence to Governmental COVID-19 Measures among Danish Students? Int. J. Environ. Res. Public. Health 2021, 18, 1822. [Google Scholar] [CrossRef]
- Muto, K.; Yamamoto, I.; Nagasu, M.; Tanaka, M.; Wada, K. Japanese Citizens’ Behavioral Changes and Preparedness against COVID-19: An Online Survey during the Early Phase of the Pandemic. PLoS ONE 2020, 15, e0234292. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A.; Axfors, C.; Contopoulos-Ioannidis, D.G. Population-Level COVID-19 Mortality Risk for Non-Elderly Individuals Overall and for Non-Elderly Individuals without Underlying Diseases in Pandemic Epicenters. Environ. Res. 2020, 188, 109890. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet Lond. Engl. 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Cappelletti, E.R.; Greco, A.; Maloberti, A.; Giannattasio, C.; Steca, P.; D’Addario, M. What Hypertensive Patients Want to Know [and from Whom] about Their Disease: A Two-Year Longitudinal Study. BMC Public Health 2020, 20, 308. [Google Scholar] [CrossRef] [PubMed]
- Steca, P.; Adorni, R.; Greco, A.; Zanatta, F.; Fattirolli, F.; Franzelli, C.; Giannattasio, C.; D’Addario, M. Impulsivity Assessed Ten Years Earlier and Sociodemographic Factors Predict Adherence to COVID-19 Related Behavioral Restrictions in Old Individuals with Hypertension. BMC Public Health 2022, 22, 185. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Cook, A.R.; Lim, J.T.; Sun, Y.; Dickens, B.L. A Systematic Review of COVID-19 Epidemiology Based on Current Evidence. J. Clin. Med. 2020, 9, 967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laslett, L.J.; Alagona, P.; Clark, B.A.; Drozda, J.P.; Saldivar, F.; Wilson, S.R.; Poe, C.; Hart, M. The Worldwide Environment of Cardiovascular Disease: Prevalence, Diagnosis, Therapy, and Policy Issues: A Report From the American College of Cardiology. J. Am. Coll. Cardiol. 2012, 60, S1–S49. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; ISBN 978-0-203-77158-7. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Topolski, T.D.; LoGerfo, J.; Patrick, D.L.; Williams, B.; Walwick, J.; Patrick, M.M.B. The Rapid Assessment of Physical Activity (RAPA) Among Older Adults. Prev. Chronic. Dis. 2006, 3, A118. [Google Scholar]
- Strath, S.J.; Kaminsky, L.A.; Ainsworth, B.E.; Ekelund, U.; Freedson, P.S.; Gary, R.A.; Richardson, C.R.; Smith, D.T.; Swartz, A.M.; American Heart Association Physical Activity Committee of the Council on Lifestyle; et al. Guide to the Assessment of Physical Activity: Clinical and Research Applications: A Scientific Statement from the American Heart Association. Circulation 2013, 128, 2259–2279. [Google Scholar] [CrossRef]
- Steca, P.; Pancani, L.; Greco, A.; D’Addario, M.; Magrin, M.E.; Miglioretti, M.; Sarini, M.; Scrignaro, M.; Vecchio, L.; Cesana, F.; et al. Changes in Dietary Behavior among Coronary and Hypertensive Patients: A Longitudinal Investigation Using the Health Action Process Approach. Appl. Psychol. Health Well-Being 2015, 7, 316–339. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greco, A.; Brugnera, A.; D’Addario, M.; Compare, A.; Franzelli, C.; Maloberti, A.; Giannattasio, C.; Fattirolli, F.; Steca, P. A Three-Year Longitudinal Study of Healthy Lifestyle Behaviors and Adherence to Pharmacological Treatments in Newly Diagnosed Patients with Acute Coronary Syndrome: Hierarchical Linear Modeling Analyses. J. Public Health 2022, 30, 931–942. [Google Scholar] [CrossRef]
- Rimm, E.B.; Giovannucci, E.L.; Willett, W.C.; Colditz, G.A.; Ascherio, A.; Rosner, B.; Stampfer, M.J. Prospective Study of Alcohol Consumption and Risk of Coronary Disease in Men. Lancet Lond. Engl. 1991, 338, 464–468. [Google Scholar] [CrossRef]
- Shek, D.T. Family Environment and Adolescent Psychological Well-Being, School Adjustment, and Problem Behavior: A Pioneer Study in a Chinese Context. J. Genet. Psychol. 1997, 158, 113–128. [Google Scholar] [CrossRef]
- Baker, T.B.; Breslau, N.; Covey, L.; Shiffman, S. DSM Criteria for Tobacco Use Disorder and Tobacco Withdrawal: A Critique and Proposed Revisions for DSM-5. Addict. Abingdon Engl. 2012, 107, 263–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greco, A.; Brugnera, A.; Adorni, R.; D’Addario, M.; Fattirolli, F.; Franzelli, C.; Giannattasio, C.; Maloberti, A.; Zanatta, F.; Steca, P. Protein Intake and Physical Activity in Newly Diagnosed Patients with Acute Coronary Syndrome: A 5-Year Longitudinal Study. Nutrients 2021, 13, 634. [Google Scholar] [CrossRef] [PubMed]
- Gitlow, L. Technology Use by Older Adults and Barriers to Using Technology. Phys. Occup. Ther. Geriatr. 2014, 32, 271–280. [Google Scholar] [CrossRef]
- Seifert, A. The Digital Exclusion of Older Adults during the COVID-19 Pandemic. J. Gerontol. Soc. Work 2020, 63, 674–676. [Google Scholar] [CrossRef]
- Górnicka, M.; Drywień, M.E.; Zielinska, M.A.; Hamułka, J. Dietary and Lifestyle Changes During COVID-19 and the Subsequent Lockdowns among Polish Adults: A Cross-Sectional Online Survey PLifeCOVID-19 Study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef]
- Stay Physically Active during Self-Quarantine. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/publications-and-technical-guidance/noncommunicable-diseases/stay-physically-active-during-self-quarantine (accessed on 24 March 2022).
- Bertrand, L.; Shaw, K.A.; Ko, J.; Deprez, D.; Chilibeck, P.D.; Zello, G.A. The Impact of the Coronavirus Disease 2019 (COVID-19) Pandemic on University Students’ Dietary Intake, Physical Activity, and Sedentary Behaviour. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2021, 46, 265–272. [Google Scholar] [CrossRef]
- Rodriguez, L.M.; Litt, D.M.; Stewart, S.H. Drinking to Cope with the Pandemic: The Unique Associations of COVID-19-Related Perceived Threat and Psychological Distress to Drinking Behaviors in American Men and Women. Addict. Behav. 2020, 110, 106532. [Google Scholar] [CrossRef] [PubMed]
- Webster, R.K.; Brooks, S.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Rubin, G.J. How to Improve Adherence with Quarantine: Rapid Review of the Evidence. Public Health 2020, 182, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Byrnes, J.P.; Miller, D.C.; Schafer, W.D. Gender Differences in Risk Taking: A Meta-Analysis. Psychol. Bull. 1999, 125, 367–383. [Google Scholar] [CrossRef]
- Ory, M.G.; Towne, S.D.; Won, J.; Forjuoh, S.N.; Lee, C. Social and Environmental Predictors of Walking among Older Adults. BMC Geriatr. 2016, 16, 155. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Pavón, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical Exercise as Therapy to Fight against the Mental and Physical Consequences of COVID-19 Quarantine: Special Focus in Older People. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef]
- Füzéki, E.; Groneberg, D.A.; Banzer, W. Physical Activity during COVID-19 Induced Lockdown: Recommendations. J. Occup. Med. Toxicol. Lond. Engl. 2020, 15, 25. [Google Scholar] [CrossRef]
- Daoust, J.-F.; Nadeau, R.; Dassonneville, R.; Lachapelle, E.; Bélanger, É.; Savoie, J.; Linden, C. van der How to Survey Citizens’ Compliance with COVID-19 Public Health Measures: Evidence from Three Survey Experiments. J. Exp. Polit. Sci. 2021, 8, 310–317. [Google Scholar] [CrossRef]
- Gollwitzer, A.; McLoughlin, K.; Martel, C.; Marshall, J.; Höhs, J.M.; Bargh, J.A. Linking Self-Reported Social Distancing to Real-World Behavior During the COVID-19 Pandemic. Soc. Psychol. Sci. 2022, 13, 656–668. [Google Scholar] [CrossRef]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Connor Gorber, S.; Tremblay, M. A Comparison of Direct versus Self-Report Measures for Assessing Physical Activity in Adults: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [Green Version]
- Hammami, A.; Harrabi, B.; Mohr, M.; Krustrup, P. Physical Activity and Coronavirus Disease 2019 (COVID-19): Specific Recommendations for Home-Based Physical Training. Manag. Sport Leis. 2022, 27, 20–25. [Google Scholar] [CrossRef]
- Hoseini, R. How to Exercise During Coronavirus Quarantine? Casp. J. Intern. Med. 2020, 11, 479–483. [Google Scholar] [CrossRef]
- PersonalParker, K.; Uddin, R.; Ridgers, N.D.; Brown, H.; Veitch, J.; Salmon, J.; Timperio, A.; Sahlqvist, S.; Cassar, S.; Toffoletti, K.; et al. The Use of Digital Platforms for Adults’ and Adolescents’ Physical Activity During the COVID-19 Pandemic (Our Life at Home): Survey Study. J. Med. Internet Res. 2021, 23, e23389. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Predictor | B | SE | p | OR | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Gender | 1.06 | 0.50 | 0.036 | 2.88 | 0.13 | 0.93 |
| Living condition | 1.29 | 0.90 | 0.154 | 3.62 | 0.62 | 21.26 |
| Occupation | 1.34 | 0.61 | 0.027 | 3.84 | 1.16 | 12.64 |
| Change in physical activity | ||||||
| Decreased—stable | 1.36 | 0.59 | 0.022 | 3.90 | 1.22 | 12.49 |
| Change in dietary routines | ||||||
| Decreased—stable | 1.09 | 0.62 | 0.080 | 2.98 | 0.88 | 10.16 |
| Increased—stable | 0.17 | 0.59 | 0.772 | 1.19 | 0.37 | 3.76 |
| Change in alcohol consumption | ||||||
| Decreased—stable | −1.21 | 0.74 | 0.104 | 0.30 | 0.07 | 1.28 |
| Increased—stable | −0.22 | 0.62 | 0.719 | 0.80 | 0.24 | 2.70 |
| Change in smoking behaviors | ||||||
| Decreased—stable | −17.19 | 1975.65 | 0.993 | 0.00 | 0.00 | Inf |
| Increased—stable | −17.44 | 2443.74 | 0.994 | 0.00 | 0.00 | Inf |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Addario, M.; Adorni, R.; Steca, P.; Capelli, R.; Zanatta, F.; Fattirolli, F.; Franzelli, C.; Giannattasio, C.; Greco, A. Associations between Lifestyle Changes and Adherence to COVID-19 Restrictions in Older Adults with Hypertension. Int. J. Environ. Res. Public Health 2022, 19, 7853. https://doi.org/10.3390/ijerph19137853
D’Addario M, Adorni R, Steca P, Capelli R, Zanatta F, Fattirolli F, Franzelli C, Giannattasio C, Greco A. Associations between Lifestyle Changes and Adherence to COVID-19 Restrictions in Older Adults with Hypertension. International Journal of Environmental Research and Public Health. 2022; 19(13):7853. https://doi.org/10.3390/ijerph19137853
Chicago/Turabian StyleD’Addario, Marco, Roberta Adorni, Patrizia Steca, Roberto Capelli, Francesco Zanatta, Francesco Fattirolli, Cristina Franzelli, Cristina Giannattasio, and Andrea Greco. 2022. "Associations between Lifestyle Changes and Adherence to COVID-19 Restrictions in Older Adults with Hypertension" International Journal of Environmental Research and Public Health 19, no. 13: 7853. https://doi.org/10.3390/ijerph19137853