
How Diabetes and Other Comorbidities of Elderly Patients and Their Treatment Influence Levels of Glycation Products

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Analysis of Pentosidine Content Using Fluorometric Method
2.2. Assessment of Content of Compounds with Thiol Groups (Glutathione)
2.3. Assessment of Lipid Peroxidation on the Basis of Determination of Malondialdehyde (MDA) in Serum
2.4. Reactive Free Amine Content
2.5. Analysis of GAL3 and LOX1 Protein Content
2.6. Analysis of sRAGE, SCRAB1, and MSR1 Protein Content
2.7. Statistical Analysis
3. Results
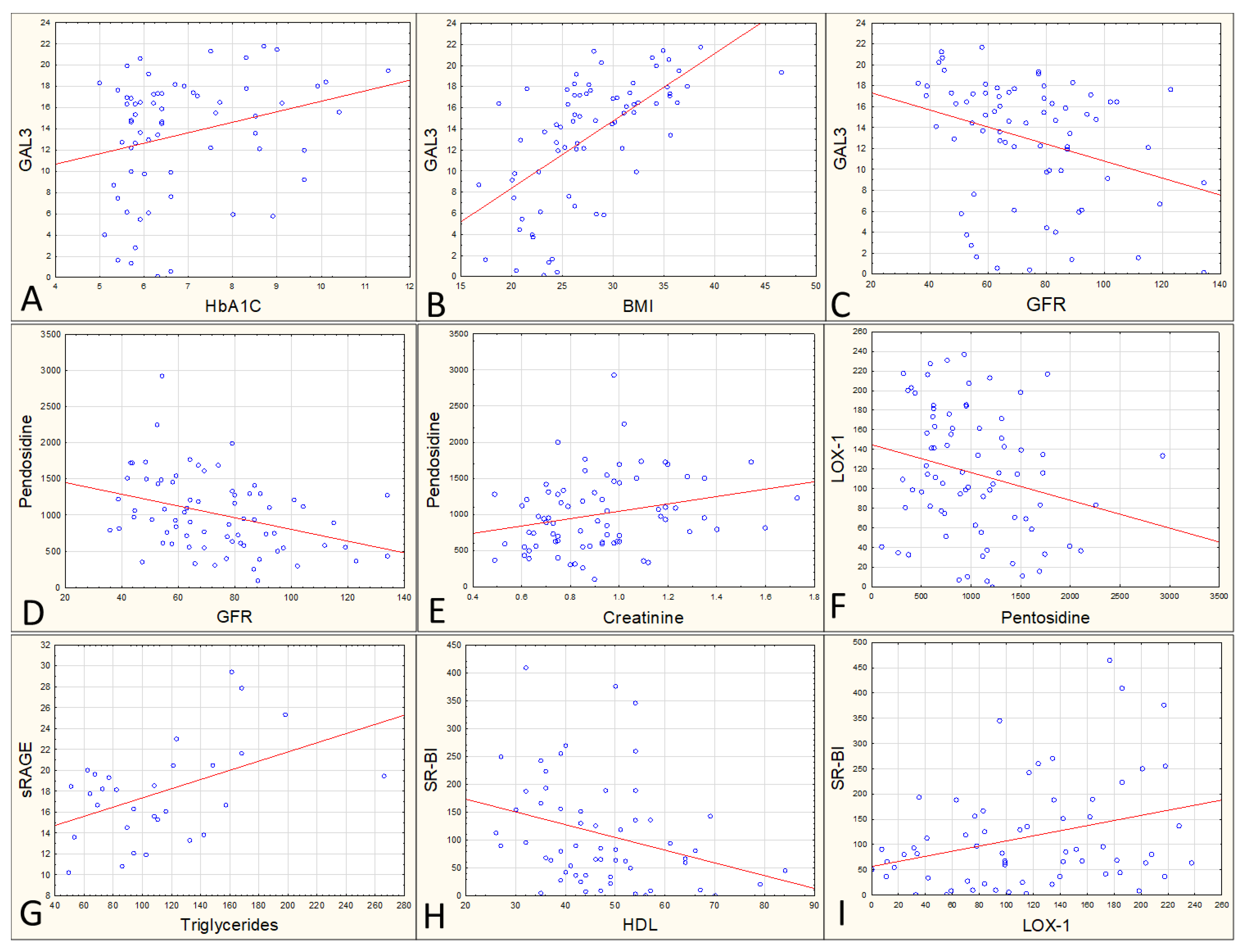
3.1. Average Values and Correlations between Variables
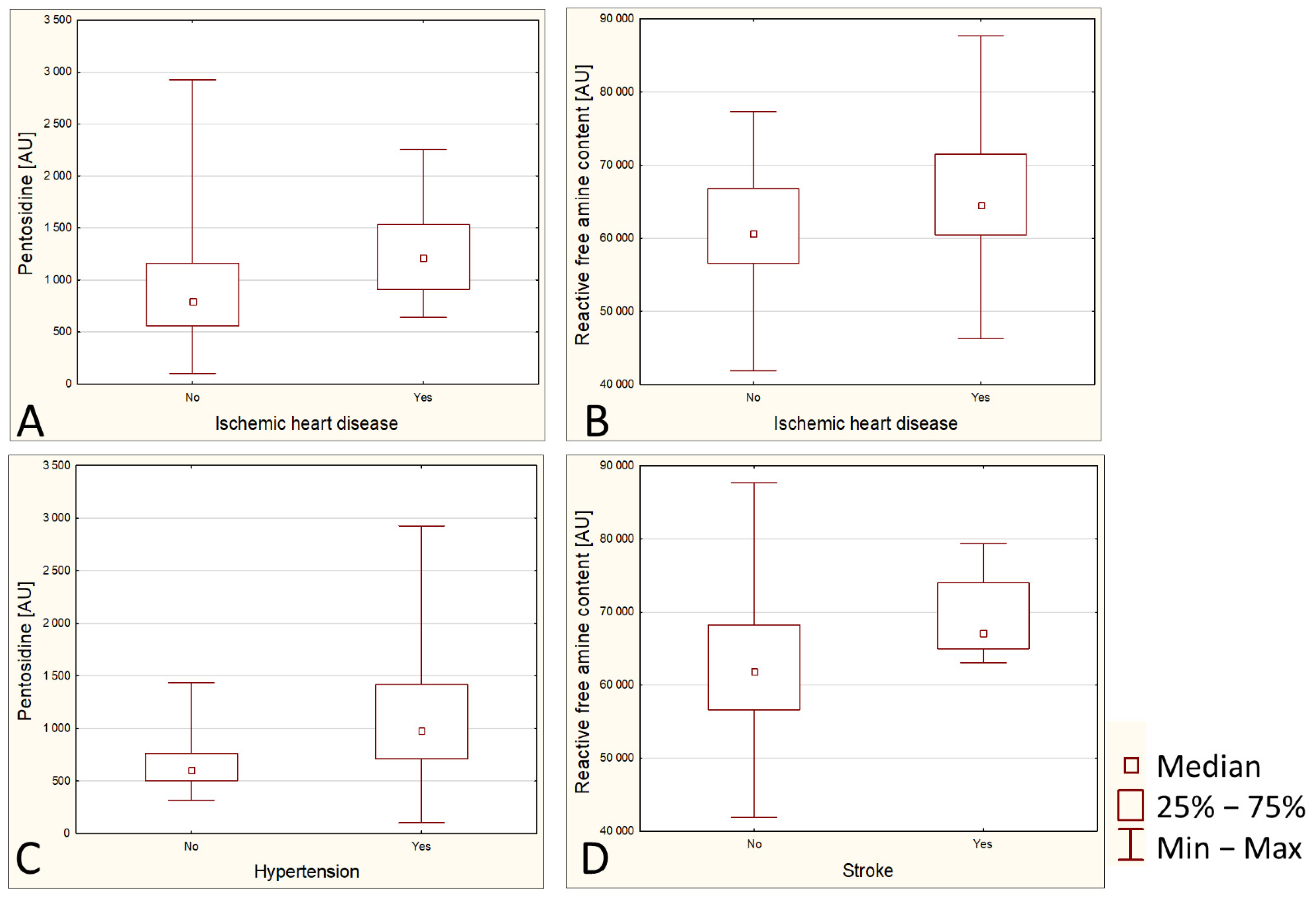
3.2. Relationships between Diseases and Biochemical Parameters
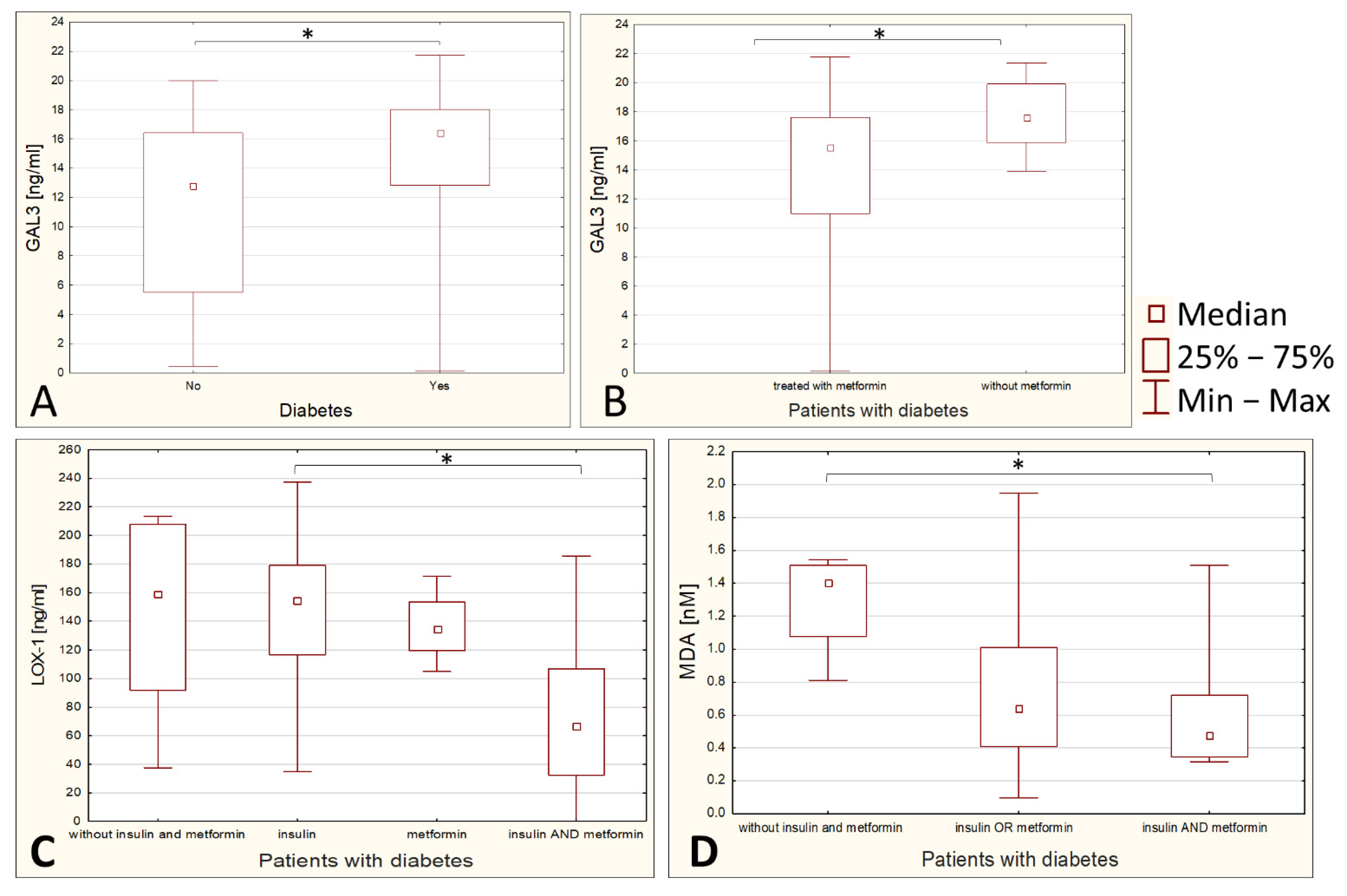
3.3. Influence of Diabetes Therapy on Parameters Related to Glycation and Peroxidation
3.4. Statistical Modeling Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nascher, I.L. Geriatrics. N. Y. Med. J. 1909, 21, 358–359. [Google Scholar] [CrossRef]
- Nascher, I.L. Geriatrics: The Diseases of Old Age and Their Treatment, including Physiological Old Age, Home and Institutional Care, and Medico-Legal Relations; P. Blakiston’s Son & Company: Philadelphia, PA, USA, 1914. [Google Scholar]
- Derejczyk, J.; Bień, B.; Kokoszka-Paszkot, J.; Szczygieł, J. Gerontologia i geriatria w Polsce na tle Europy—Czy należy inwestować w ich rozwój w naszym kraju? Gerontol. Pol. 2008, 16, 149–159. [Google Scholar]
- Jaul, E.; Barron, J. Age-Related Diseases and Clinical and Public Health Implications for the 85 Years Old and Over Population. Front. Public Heal. 2017, 5, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leszko, M.; Zając-Lamparska, L.; Trempala, J. Aging in Poland. Gerontologist 2015, 55, 707–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cybulski, M.; Krajewska-Kułak, E.; Sowa, P.; Shpakau, A.; Theodosopoulou, E.; Chadzopulu, A. Most common health problems of elderly in the opinion of health sciences students in Poland, Belarus and Greece. Prog. Health Sci. 2016, 6, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Bautmans, I.; Salimans, L.; Njemini, R.; Beyer, I.; Lieten, S.; Liberman, K. The effects of exercise interventions on the inflammatory profile of older adults: A systematic review of the recent literature. Exp. Gerontol. 2021, 146, 111236. [Google Scholar] [CrossRef]
- Chentli, F.; Azzoug, S.; Mahgoun, S. Diabetes mellitus in elderly. Indian J. Endocrinol. Metab. 2015, 19, 744–752. [Google Scholar] [CrossRef]
- Sinclair, A.; Morley, J.E.; Rodriguez-Mañas, L.; Paolisso, G.; Bayer, T.; Zeyfang, A.; Bourdel-Marchasson, I.; Vischer, U.; Woo, J.; Chapman, I. Diabetes mellitus in older people: Position statement on behalf of the International Association of Gerontology and Geriatrics (IAGG), the European Diabetes Working Party for Older People (EDWPOP), and the International Task Force of Experts in Diabetes. J. Am. Med. Dir. Assoc. 2012, 13, 497–502. [Google Scholar] [CrossRef]
- Boyle, J.P.; Thompson, T.J.; Gregg, E.W.; Barker, L.E.; Williamson, D.F. Projection of the year 2050 burden of diabetes in the US adult population: Dynamic modeling of incidence, mortality, and prediabetes prevalence. Popul. Health Metr. 2010, 8, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Gentile, S.; Strollo, F.; Ceriello, A. COVID-19 infection in Italian people with diabetes: Lessons learned for our future (an experience to be used). Diabetes Res. Clin. Pract. 2020, 162, 108137. [Google Scholar] [CrossRef]
- Cuschieri, S.; Grech, S. COVID-19 and diabetes: The why, the what and the how. J. Diabetes Complicat. 2020, 34, 107637. [Google Scholar] [CrossRef] [PubMed]
- Yanase, T.; Yanagita, I.; Muta, K.; Nawata, H. Frailty in elderly diabetes patients. Endocr. J. 2018, 65, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, K.H.; Godin, D.V. Micronutrients and antioxidants in the progression of diabetes. Nutr. Res. 1995, 15, 1377–1410. [Google Scholar] [CrossRef]
- Newsholme, P.; Cruzat, V.F.; Keane, K.N.; Carlessi, R.; de Bittencourt, P.I.H.J. Molecular mechanisms of ROS production and oxidative stress in diabetes. Biochem. J. 2016, 473, 4527–4550. [Google Scholar] [CrossRef] [PubMed]
- Nowotny, K.; Jung, T.; Höhn, A.; Weber, D.; Grune, T. Advanced glycation end products and oxidative stress in type 2 diabetes mellitus. Biomolecules 2015, 5, 194–222. [Google Scholar] [CrossRef] [Green Version]
- Newlaczyl, A.U.; Yu, L.G. Galectin-3—A jack-of-all-trades in cancer. Cancer Lett. 2011, 313, 123–128. [Google Scholar] [CrossRef]
- Böhme, R.; Becker, C.; Keil, B.; Damm, M.; Rasch, S.; Beer, S.; Schneider, R.; Kovacs, P.; Bugert, P.; Riedel, J.; et al. Serum levels of advanced glycation end products and their receptors sRAGE and Galectin-3 in chronic pancreatitis. Pancreatology 2020, 20, 187–192. [Google Scholar] [CrossRef]
- Stephen, S.L.; Freestone, K.; Dunn, S.; Twigg, M.W.; Homer-Vanniasinkam, S.; Walker, J.H.; Wheatcroft, S.B.; Ponnambalam, S. Scavenger Receptors and Their Potential as Therapeutic Targets in the Treatment of Cardiovascular Disease. Int. J. Hypertens. 2010, 2010, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Neviere, R.; Yu, Y.; Wang, L.; Tessier, F.; Boulanger, E. Implication of advanced glycation end products (Ages) and their receptor (Rage) on myocardial contractile and mitochondrial functions. Glycoconj. J. 2016, 33, 607–617. [Google Scholar] [CrossRef]
- Hamasaki, S.; Kobori, T.; Yamazaki, Y.; Kitaura, A.; Niwa, A.; Nishinaka, T.; Nishibori, M.; Mori, S.; Nakao, S.; Takahashi, H. Effects of scavenger receptors-1 class A stimulation on macrophage morphology and highly modified advanced glycation end product-protein phagocytosis. Sci. Rep. 2018, 8, 1–11. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Leszek, J.; Małyszczak, K.; Bartyś, A.; Staniszewska, M.; Gamian, A. Analysis of Serum of Patients With Alzheimer’s Disease for the Level of Advanced Glycation End Products. Am. J. Alzheimer’s Dis. Other Dement. 2006, 21, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Diplock, A.T.; Symons, M.C.R.; Rice-Evans, C.A. Techniques in Free Radical Research; Elsevier: Amsterdam, The Netherlands, 1991; ISBN 0080858910. [Google Scholar]
- Shetty, S.; Babu, S.; Kumari, S.; Shetty, P.; Hegde, S.; Castelino, R. Status of salivary lipid peroxidation in oral cancer and precancer. Indian J. Med. Paediatr. Oncol. 2014, 35, 156–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fracasso, B.D.M.; Rangel, J.O.; Machado, A.G.; Curuja, F.S.; Lopes, A.; Olsen, V.; Clausell, N.; Biolo, A.; Rohde, L.E.; Andrades, M. Characterization of advanced glycation end products and their receptor (RAGE) in an animal model of myocardial infarction. PLoS ONE 2019, 14, e0209964. [Google Scholar] [CrossRef] [PubMed]
- Pashchenko, Y.; Clausing, D.H.; Ablah, E.; Okut, H.; Elhomsy, G.C. Glycemic Control and Awareness of Insulin Therapy. Kans. J. Med. 2021, 14, 249. [Google Scholar] [CrossRef] [PubMed]
- Masuch, A.; Friedrich, N.; Roth, J.; Nauck, M.; Müller, U.A.; Petersmann, A. Preventing misdiagnosis of diabetes in the elderly: Age-dependent HbA1c reference intervals derived from two population-based study cohorts. BMC Endocr. Disord. 2019, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Zhang, Q. Glycated Plasma Proteins as More Sensitive Markers for Glycemic Control in Type 1 Diabetes. Proteom. Clin. Appl. 2020, 14, 1900104. [Google Scholar] [CrossRef]
- Hashimoto, K.; Kunikata, H.; Yasuda, M.; Ito, A.; Aizawa, N.; Sawada, S.; Kondo, K.; Satake, C.; Takano, Y.; Nishiguchi, K.M.; et al. The relationship between advanced glycation end products and ocular circulation in type 2 diabetes. J. Diabetes Complicat. 2016, 30, 1371–1377. [Google Scholar] [CrossRef] [Green Version]
- Sato, E.; Nagaoka, T.; Yokota, H.; Takahashi, A.; Yoshida, A. Correlation between plasma pentosidine concentrations and retinal hemodynamics in patients with type 2 diabetes. Am. J. Ophthalmol. 2012, 153, 903–909.e1. [Google Scholar] [CrossRef]
- Hrynchyshyn, N.; Jourdain, P.; Desnos, M.; Diebold, B.; Funck, F. Galectin-3: A new biomarker for the diagnosis, analysis and prognosis of acute and chronic heart failure. Arch. Cardiovasc. Dis. 2013, 106, 541–546. [Google Scholar] [CrossRef] [Green Version]
- Kanukurti, J.; Mohammed, N.; Sreedevi, N.N.; Khan, S.A.; Baba, K.S.S.S.; Bhaskar, M.V.; Satish, O.S.; Naushad, S.M.; Mohan, I.K. Evaluation of Galectin-3 as a Novel Diagnostic Biomarker in Patients with Heart Failure with Preserved Ejection Fraction. J. Lab. Physicians 2020, 12, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Atalar, M.N.; Abuşoğlu, S.; Ünlü, A.; Tok, O.; İpekçi, S.H.; Baldane, S.; Kebapcılar, L. Assessment of serum galectin-3, methylated arginine and Hs-CRP levels in type 2 diabetes and prediabetes. Life Sci. 2019, 231, 116577. [Google Scholar] [CrossRef] [PubMed]
- King, D.R.; Salako, D.C.; Arthur-Bentil, S.K.; Rubin, A.E.; Italiya, J.B.; Tan, J.S.; Macris, D.G.; Neely, H.K.; Palka, J.M.; Grodin, J.L.; et al. Relationship between novel inflammatory biomarker galectin-3 and depression symptom severity in a large community-based sample. J. Affect. Disord. 2021, 281, 384–389. [Google Scholar] [CrossRef]
- Pang, J.; Nguyen, V.T.; Rhodes, D.H.; Sullivan, M.E.; Braunschweig, C.; Fantuzzi, G. Relationship of galectin-3 with obesity, IL-6, and CRP in women. J. Endocrinol. Investig. 2016, 39, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Kang, X.; Guo, Y.; Zhang, J.; Xie, J.; Shao, S.; Xiang, Y.; Chen, G.; Yu, X. Association of circulating galectin-3 with gestational diabetes mellitus, progesterone, and insulin resistance. J. Diabetes 2021, 13, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Alves, M.T.; de Souza, I.D.P.; Ferreira, C.N.; Cândido, A.L.; Bizzi, M.F.; Oliveira, F.R.; Reis, F.M.; Gomes, K.B. Galectin-3 is a potential biomarker to insulin resistance and obesity in women with polycystic ovary syndrome. Gynecol. Endocrinol. 2020, 36, 760–763. [Google Scholar] [CrossRef]
- Sattar Taha, A.; Zahraei, Z.; Al-Hakeim, H.K. Serum apelin and galectin-3 in preeclampsia in Iraq. Hypertens. Pregnancy 2020, 39, 379–386. [Google Scholar] [CrossRef]
- Dikker, O.; Akarsu, M. Evaluation of serum galectin-3 concentrations in patients with hypothyroidism. Scand. J. Clin. Lab. Invest. 2019, 79, 354–358. [Google Scholar] [CrossRef]
- O’Seaghdha, C.M.; Hwang, S.J.; Ho, J.E.; Vasan, R.S.; Levy, D.; Fox, C.S. Elevated galectin-3 precedes the development of CKD. J. Am. Soc. Nephrol. 2013, 24, 1470–1477. [Google Scholar] [CrossRef] [Green Version]
- Tang, W.H.W.; Shrestha, K.; Shao, Z.; Borowski, A.G.; Troughton, R.W.; Thomas, J.D.; Klein, A.L. Usefulness of plasma galectin-3 levels in systolic heart failure to predict renal insufficiency and survival. Am. J. Cardiol. 2011, 108, 385–390. [Google Scholar] [CrossRef] [Green Version]
- Asensio-Lopez, M.D.C.; Lax, A.; Fernandez del Palacio, M.J.; Sassi, Y.; Hajjar, R.J.; Pascual-Figal, D.A. Pharmacological inhibition of the mitochondrial NADPH oxidase 4/PKCα/Gal-3 pathway reduces left ventricular fibrosis following myocardial infarction. Transl. Res. 2018, 199, 4–23. [Google Scholar] [CrossRef] [PubMed]
- Weigert, J.; Neumeier, M.; Wanninger, J.; Bauer, S.; Farkas, S.; Scherer, M.N.; Schnitzbauer, A.; Schäffler, A.; Aslanidis, C.; Schölmerich, J.; et al. Serum Galectin-3 Is Elevated in Obesity and Negatively Correlates with Glycosylated Hemoglobin in Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2010, 95, 1404–1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Fu, W.; Zheng, Y.; Yang, J.; Liu, Y.; Qi, Z.; Wu, M.; Fan, Z.; Yin, K.; Chen, Y.; et al. Galectin 3 enhances platelet aggregation and thrombosis via Dectin-1 activation: A translational study. Eur. Heart J. 2022. [Google Scholar] [CrossRef]
- Jakobs, K.; Rauch, U. Galectin-3 inhibitors as novel antithrombotic drugs with almost no bleeding risk: Wishful thinking or a realistic vision? Eur. Heart J. 2022. [Google Scholar] [CrossRef] [PubMed]
- Witkowski, M.; Friebel, J.; Tabaraie, T.; Grabitz, S.; Dörner, A.; Taghipour, L.; Jakobs, K.; Stratmann, B.; Tschoepe, D.; Landmesser, U.; et al. Metformin Is Associated with Reduced Tissue Factor Procoagulant Activity in Patients with Poorly Controlled Diabetes. Cardiovasc. Drugs Ther. 2021, 35, 809–813. [Google Scholar] [CrossRef] [PubMed]
- Marsche, G.; Weigle, B.; Sattler, W.; Malle, E. Soluble RAGE blocks scavenger receptor CD36-mediated uptake of hypochlorite-modified low-density lipoprotein. FASEB J. 2007, 21, 3075–3082. [Google Scholar] [CrossRef] [PubMed]
- Barreto, J.; Karathanasis, S.K.; Remaley, A.; Sposito, A.C. Role of LOX-1 (Lectin-Like Oxidized Low-Density Lipoprotein Receptor 1) as a Cardiovascular Risk Predictor: Mechanistic Insight and Potential Clinical Use. Arterioscler. Thromb. Vasc. Biol. 2020, 41, 153–166. [Google Scholar] [CrossRef]
- Akhmedov, A.; Sawamura, T.; Chen, C.-H.; Kraler, S.; Vdovenko, D.; Lüscher, T.F. Lectin-like oxidized low-density lipoprotein receptor-1 (LOX-1): A crucial driver of atherosclerotic cardiovascular disease. Eur. Heart J. 2020, 42, 1797–1807. [Google Scholar] [CrossRef]
- Mentrup, T.; Cabrera-Cabrera, F.; Schröder, B. Proteolytic Regulation of the Lectin-Like Oxidized Lipoprotein Receptor LOX-1. Front. Cardiovasc. Med. 2021, 7, 594441. [Google Scholar] [CrossRef]
- West, M.; Greason, E.; Kolmakova, A.; Jahangiri, A.; Asztalos, B.; Pollin, T.I.; Rodriguez, A. Scavenger receptor class B type i protein as an independent predictor of high-density lipoprotein cholesterol levels in subjects with hyperalphalipoproteinemia. J. Clin. Endocrinol. Metab. 2009, 94, 1451–1457. [Google Scholar] [CrossRef] [Green Version]
- Bailey, C.J. Metformin: Historical overview. Diabetologia 2017, 60, 1566–1576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruggiero-Lopez, D.; Lecomte, M.; Moinet, G.; Patereau, G.; Lagarde, M.; Wiernsperger, N. Reaction of metformin with dicarbonyl compounds. possible implication in the inhibition of advanced glycation end product formation. Biochem. Pharmacol. 1999, 58, 1765–1773. [Google Scholar] [CrossRef]
- Beisswenger, P.; Ruggiero-Lopez, D. Metformin inhibition of glycation processes. Diabetes Metab. 2003, 29, 6S95–6S103. [Google Scholar] [CrossRef]
- Ahmad, S.; Shahab, U.; Baig, M.H.; Khan, M.S.; Khan, M.S.; Srivastava, A.K.; Saeed, M. Moinuddin Inhibitory Effect of Metformin and Pyridoxamine in the Formation of Early, Intermediate and Advanced Glycation End-Products. PLoS ONE 2013, 8, e72128. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.H.; Chan, S.H.; Chu, P.M.; Lin, H.C.; Tsai, K.L. Metformin regulates oxLDL-facilitated endothelial dysfunction by modulation of SIRT1 through repressing LOX-1-modulated oxidative signaling. Oncotarget 2016, 7, 10773–10787. [Google Scholar] [CrossRef] [Green Version]
- Shiu, S.W.M.; Wong, Y.; Tan, K.C.B. Effect of advanced glycation end products on lectin-like oxidized low density lipoprotein receptor-1 expression in endothelial cells. J. Atheroscler. Thromb. 2012, 19, 1083–1092. [Google Scholar] [CrossRef] [Green Version]
- Ouslimani, N.; Mahrouf, M.; Peynet, J.; Bonnefont-Rousselot, D.; Cosson, C.; Legrand, A.; Beaudeux, J.L. Metformin reduces endothelial cell expression of both the receptor for advanced glycation end products and lectin-like oxidized receptor 1. Metabolism 2007, 56, 308–313. [Google Scholar] [CrossRef]
- Valencia, J.V.; Weldon, S.C.; Quinn, D.; Kiers, G.H.; DeGroot, J.; TeKoppele, J.M.; Hughes, T.E. Advanced glycation end product ligands for the receptor for advanced glycation end products: Biochemical characterization and formation kinetics. Anal. Biochem. 2004, 324, 68–78. [Google Scholar] [CrossRef]
- Yoshida, N.; Okumura, K.I.; Aso, Y. High serum pentosidine concentrations are associated with increased arterial stiffness and thickness in patients with type 2 diabetes. Metabolism 2005, 54, 345–350. [Google Scholar] [CrossRef]
- Guerin-Dubourg, A.; Cournot, M.; Planesse, C.; Debussche, X.; Meilhac, O.; Rondeau, P.; Bourdon, E. Association between Fluorescent Advanced Glycation End-Products and Vascular Complications in Type 2 Diabetic Patients. Biomed. Res. Int. 2017, 2017, 7989180. [Google Scholar] [CrossRef]
- Bodiga, V.L.; Eda, S.R.; Bodiga, S. Advanced glycation end products: Role in pathology of diabetic cardiomyopathy. Heart Fail. Rev. 2014, 19, 49–63. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, S.; Miyata, T.; Ueda, Y.; Tanaka, H.; Maeda, K.; Kawashima, S.; Van Ypersele de Strihou, C.; Kurokawa, K. Plasma levels of pentosidine in diabetic patients: An advanced glycation end product. J. Am. Soc. Nephrol. 1998, 9, 1681–1688. [Google Scholar] [CrossRef] [PubMed]
- Kerkeni, M.; Weiss, I.S.; Jaisson, S.; Dandana, A.; Addad, F.; Gillery, P.; Hammami, M. Increased serum concentrations of pentosidine are related to presence and severity of coronary artery disease. Thromb. Res. 2014, 134, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Kerkeni, M.; Saïdi, A.; Bouzidi, H.; Letaief, A.; Ben Yahia, S.; Hammami, M. Pentosidine as a biomarker for microvascular complications in type 2 diabetic patients. Diabetes Vasc. Dis. Res. 2013, 10, 239–245. [Google Scholar] [CrossRef]
- Nakano, M.; Nakamura, Y.; Suzuki, T.; Miyazaki, A.; Takahashi, J.; Saito, M.; Shiraki, M. Pentosidine and carboxymethyl-lysine associate differently with prevalent osteoporotic vertebral fracture and various bone markers. Sci. Rep. 2020, 10, 22090. [Google Scholar] [CrossRef]
- Munenori, K.; Kitazawa, R.; Makita, K.; Yoshida, K.; Takeji, M.; Soga, Y.; Kurata, M.; Haraguchi, R.; Kitazawa, S. Pulmonary hypertension associated with diffuse deposition of pentosidine in pulmonary arterioles. Diabetes Res. Clin. Pract. 2013, 100, e59–e62. [Google Scholar] [CrossRef]
- Dozio, E.; Vettoretti, S.; Caldiroli, L.; Nerini-Molteni, S.; Tacchini, L.; Ambrogi, F.; Messa, P.; Corsi Romanelli, M.M. Advanced glycation end products (Age) and soluble forms of age receptor: Emerging role as mortality risk factors in CKD. Biomedicines 2020, 8, 638. [Google Scholar] [CrossRef]
- Schalkwijk, C.G.; Ter Wee, P.M.; Stehouwer, C.D.A. Plasma levels of AGE peptides in type 1 diabetic patients are associated with serum creatinine and not with albumin excretion rate: Possible role of AGE peptide-associated endothelial dysfunction. Ann. N. Y. Acad. Sci. 2005, 1043, 662–670. [Google Scholar] [CrossRef]
- Nooshi-Nedamani, S.; Habibi-Rezaei, M.; Farzadfard, A.; Moosavi-Movahedi, A.A. Intensification of serum albumin amyloidogenesis by a glycation-peroxidation loop (GPL). Arch. Biochem. Biophys. 2019, 668, 54–60. [Google Scholar] [CrossRef]
- Kocer, D.; Bayram, F.; Diri, H. The effects of metformin on endothelial dysfunction, lipid metabolism and oxidative stress in women with polycystic ovary syndrome. Gynecol. Endocrinol. 2014, 30, 367–371. [Google Scholar] [CrossRef]
- Sotoudeh, R.; Hadjzadeh, M.-A.-R.; Gholamnezhad, Z.; Aghaei, A. The anti-diabetic and antioxidant effects of a combination of Commiphora mukul, Commiphora myrrha and Terminalia chebula in diabetic rats. Avicenna J. Phytomedicine 2019, 9, 454–464. [Google Scholar] [CrossRef]
- ALrefai, A.A.; Alsalamony, A.M.; Fatani, S.H.; Kamel, H.F.M. Effect of variable antidiabetic treatments strategy on oxidative stress markers in obese patients with T2DM. Diabetol. Metab. Syndr. 2017, 9, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Q.; Li, J.; Gao, F. New insights into insulin: The anti-inflammatory effect and its clinical relevance. World J. Diabetes 2014, 5, 89. [Google Scholar] [CrossRef] [PubMed]
- Monnier, L.; Colette, C.; Michel, F.; Cristol, J.P.; Owens, D.R. Insulin therapy has a complex relationship with measure of oxidative stress in type 2 diabetes: A case for further study. Diabetes. Metab. Res. Rev. 2011, 27, 348–353. [Google Scholar] [CrossRef]
- Bunck, M.C.; Cornér, A.; Eliasson, B.; Heine, R.J.; Shaginian, R.M.; Wu, Y.; Yan, P.; Smith, U.; Yki-Järvinen, H.; Diamant, M.; et al. One-year treatment with exenatide vs. Insulin Glargine: Effects on postprandial glycemia, lipid profiles, and oxidative stress. Atherosclerosis 2010, 212, 223–229. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, Y.; Xiong, D.; Xie, C. Insulin combined with Chinese medicine improves glycemic outcome through multiple pathways in patients with type 2 diabetes mellitus. J. Diabetes Investig. 2015, 6, 708–715. [Google Scholar] [CrossRef]
- Koenig, R.J.; Peterson, C.M.; Jones, R.L.; Saudek, C.; Lehrman, M.; Cerami, A. Correlation of Glucose Regulation and Hemoglobin AIc in Diabetes Mellitus. N. Engl. J. Med. 2009, 295, 417–420. [Google Scholar] [CrossRef]
- Kuzan, A.; Chwiłkowska, A.; Kobielarz, M.; Pezowicz, C.; Gamian, A. Glycation of extracellular matrix proteins and its role in atherosclerosis. Postepy Hig. Med. Dosw. 2012, 66, 804–809. [Google Scholar] [CrossRef]
- Caniglia, J.L.; Guda, M.R.; Asuthkar, S.; Tsung, A.J.; Velpula, K.K. A potential role for Galectin-3 inhibitors in the treatment of COVID-19. PeerJ 2020, 8, e9392. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Without Diabetes 0 (N = 38) | With Diabetes 1 (N = 41) | p | |
|---|---|---|---|
| Age (Max-Min) | 79.65 (64.0–92.0) | 78.7 (64.0–94.0) | 0.52 |
| Sex (Women/Men) | 29/9 | 30/11 | 0.7480 |
| BMI (Max-Min) | 26.21 (17.4–46.6) | 29.43 (18.7–38.6) | 0.003 |
| Ischemic heart disease 0/1 * | 27/9 | 25/12 | 0.4831 |
| Myocardial infarction 0/1 * | 37/1 | 35/6 | 0.0667 |
| Stroke 0/1 * | 32/5 | 36/5 | 0.5634 |
| Hypertension 0/1 * | 11/27 | 6/35 | 0.1014 |
| Peripheral artery disease 0/1 * | 34/3 | 37/4 | 0.5582 |
| Atherosclerosis 0/1 * | 13/25 | 9/32 | 0.2245 |
| Hyperlipidemia 0/1 * | 18/19 | 28/12 | 0.0563 |
| Fatty liver disease 0/1 * | 32/6 | 30/11 | 0.2329 |
| HbA1c (%) | 5.81 ± 0.39 | 7.69 ± 1.54 | <0.001 |
| Glucose (mg/dL) | 98.39 ± 17.35 | 155.85 ± 71.59 | <0.001 |
| Hemoglobin (g/dL) | 12.64 ± 1.54 | 12.72 ± 1.31 | 0.8365 |
| Cholesterol (mg/dL) | 202.08 ± 54.04 | 151.18 ± 41.88 | <0.001 |
| HDL (mg/dL) | 53.69 ± 10.75 | 41.05 ± 1.68 | <0.001 |
| LDL (mg/dL) | 124.94 ± 44.57 | 81.54 ± 32.68 | <0.001 |
| Triglycerides (mg/dL) | 114.32 ± 47.84 | 135.42 ± 57.45 | 0.0971 |
| Total protein (g/dL) | 6.98 ± 0.57 | 7.18 ± 0.78 | 0.2056 |
| CRP (mg/L) | 3.44 ± 9.02 | 4.37 ± 5.91 | 0.5916 |
| Creatinine (mg/dL) | 0.90 ± 0.22 | 0.93 ± 0.28 | 0.5572 |
| Uric acid (mg/dL) | 5.58 ± 1.38 | 6.29 ± 1.99 | 0.0975 |
| GFR (mL/min/1.73 m2) | 72.95 ± 20.34 | 72.44 ± 22.67 | 0.9210 |
| Parameter (N) | Mean | SD |
|---|---|---|
| Pentosidine (AU) (81) | 1015.26 | 513.17 |
| Free amine content (AU) (82) | 62,838.79 | 8247.55 |
| GAL3 (ng/mL) (82) | 13.23 | 5.77 |
| LOX1 (ng/mL) (78) | 115.47 | 64.51 |
| sRAGE (pg/mL) (32) | 17.98 | 4.74 |
| SR-BI (SCRAB1) (pg/mL) (63) | 116.96 | 103.34 |
| SR-A (MSR1) (ng/mL) (75) | 2.58 | 4.04 |
| MDA (nM) (78) | 0.75 | 0.51 |
| Glutathione (mM) (81) | 0.15 | 0.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuzan, A.; Królewicz, E.; Kustrzeba-Wójcicka, I.; Lindner-Pawłowicz, K.; Sobieszczańska, M. How Diabetes and Other Comorbidities of Elderly Patients and Their Treatment Influence Levels of Glycation Products. Int. J. Environ. Res. Public Health 2022, 19, 7524. https://doi.org/10.3390/ijerph19127524
Kuzan A, Królewicz E, Kustrzeba-Wójcicka I, Lindner-Pawłowicz K, Sobieszczańska M. How Diabetes and Other Comorbidities of Elderly Patients and Their Treatment Influence Levels of Glycation Products. International Journal of Environmental Research and Public Health. 2022; 19(12):7524. https://doi.org/10.3390/ijerph19127524
Chicago/Turabian StyleKuzan, Aleksandra, Emilia Królewicz, Irena Kustrzeba-Wójcicka, Karolina Lindner-Pawłowicz, and Małgorzata Sobieszczańska. 2022. "How Diabetes and Other Comorbidities of Elderly Patients and Their Treatment Influence Levels of Glycation Products" International Journal of Environmental Research and Public Health 19, no. 12: 7524. https://doi.org/10.3390/ijerph19127524