
The Effects of a Dance and Music-Based Intervention on Parkinson’s Patients’ Well-Being: An Interview Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Procedure
2.3. Data Analysis–Content Analysis
2.4. Data Analysis–Quantitative Content Analysis
3. Results
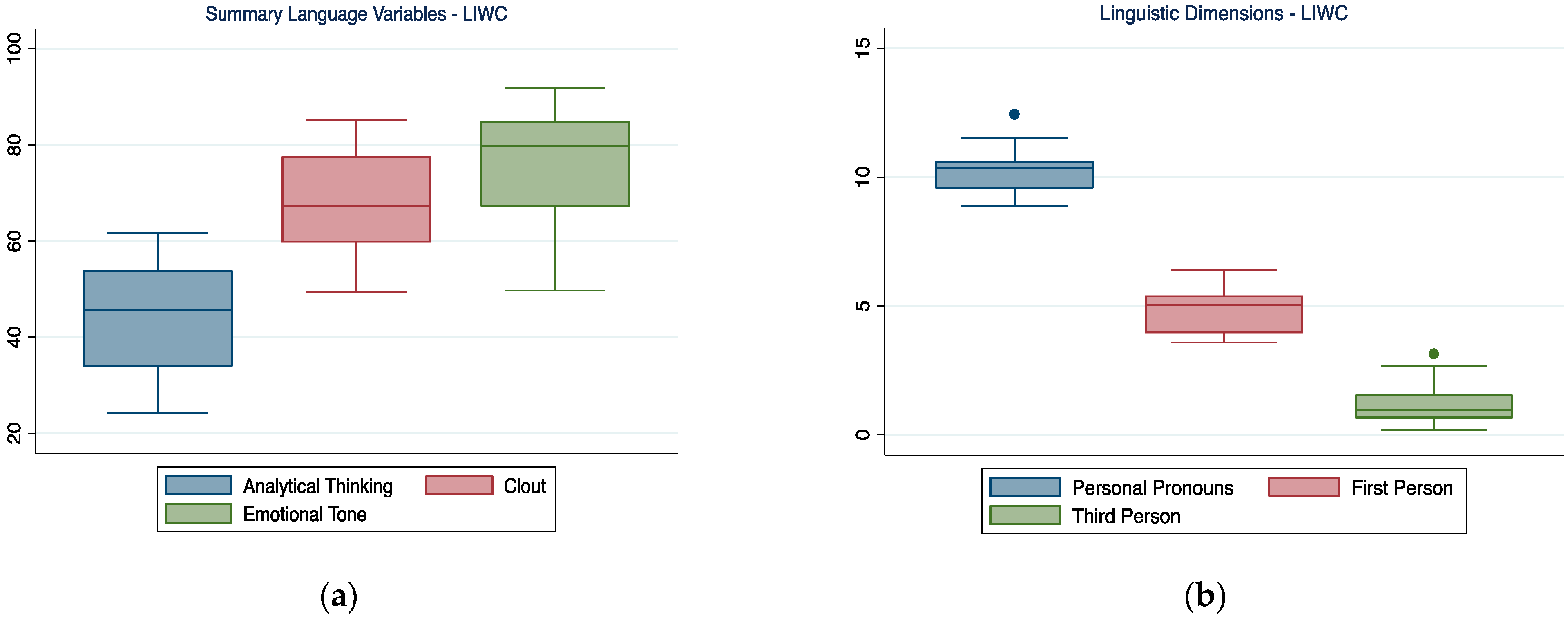
3.1. Summary Language Variables and Linguistic Dimensions
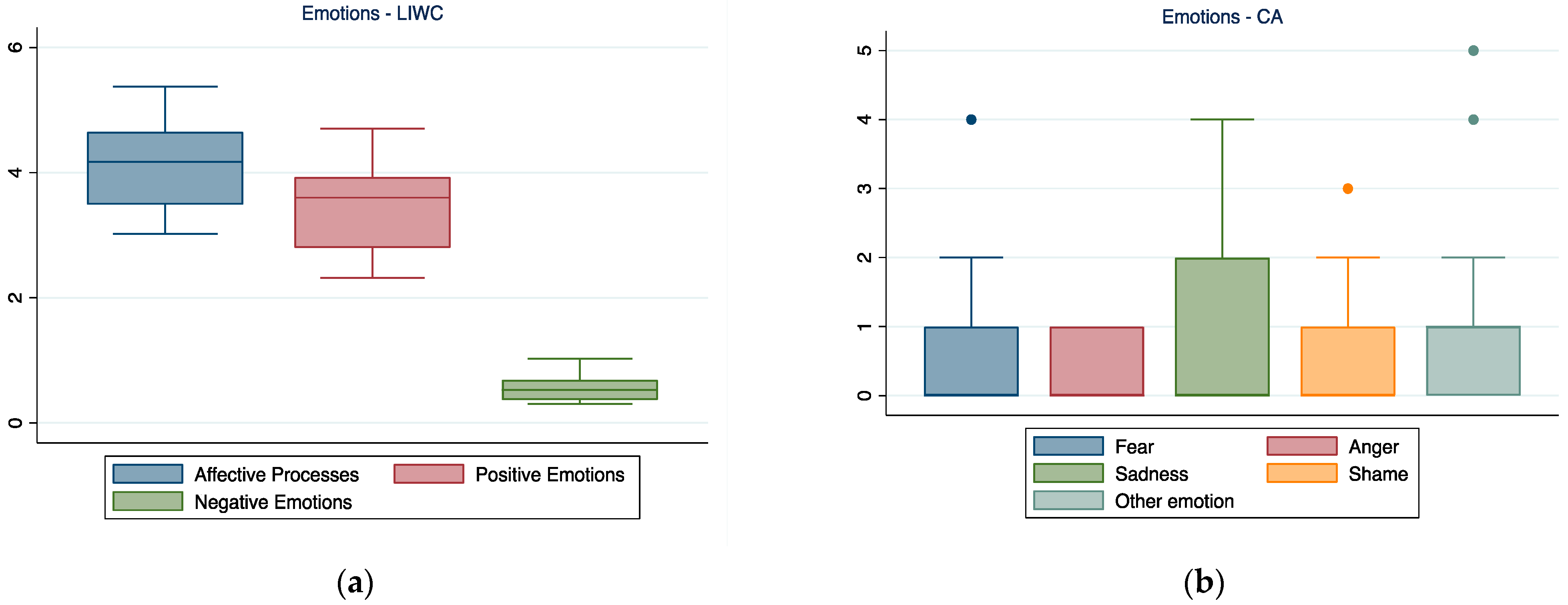
3.2. Emotions
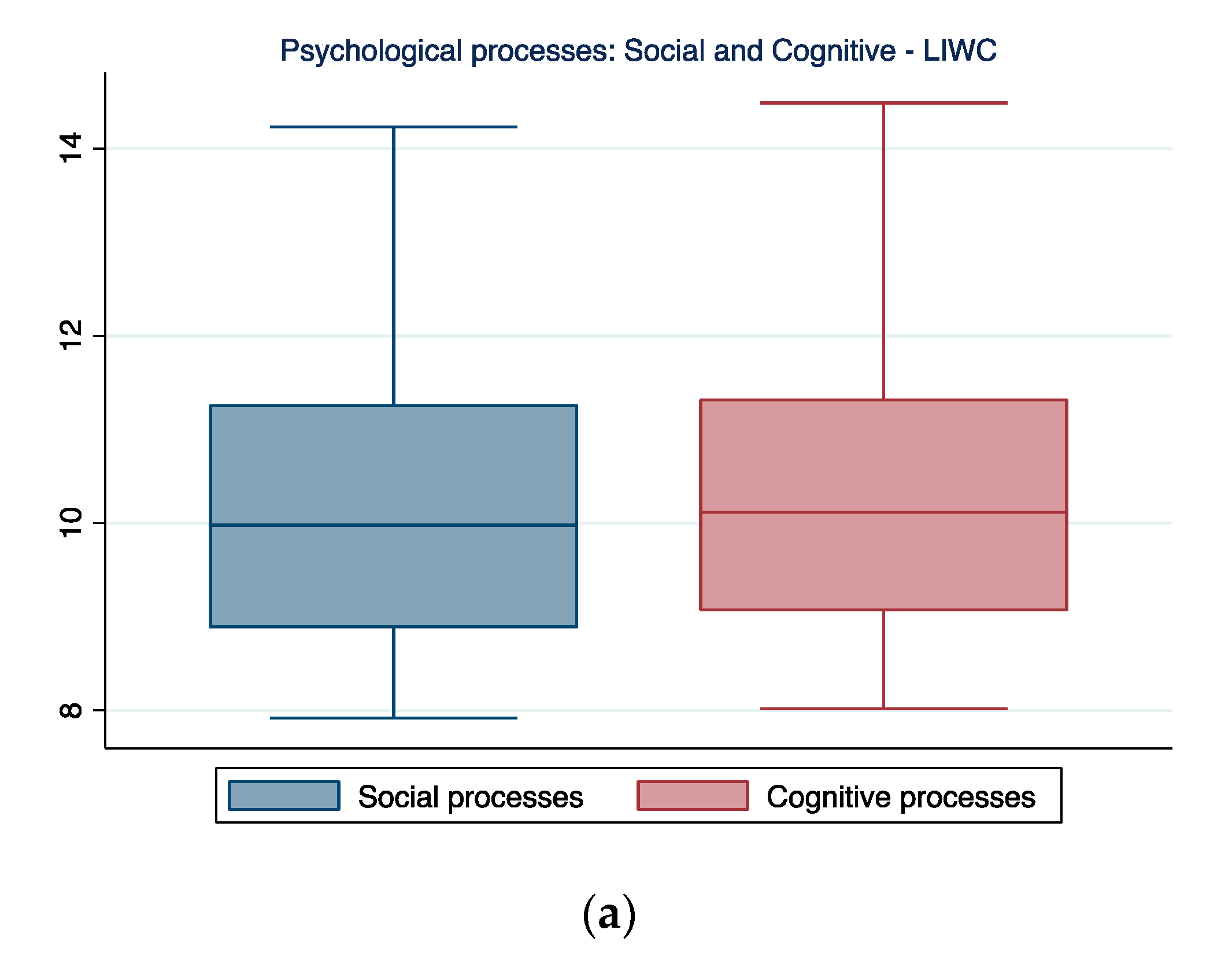
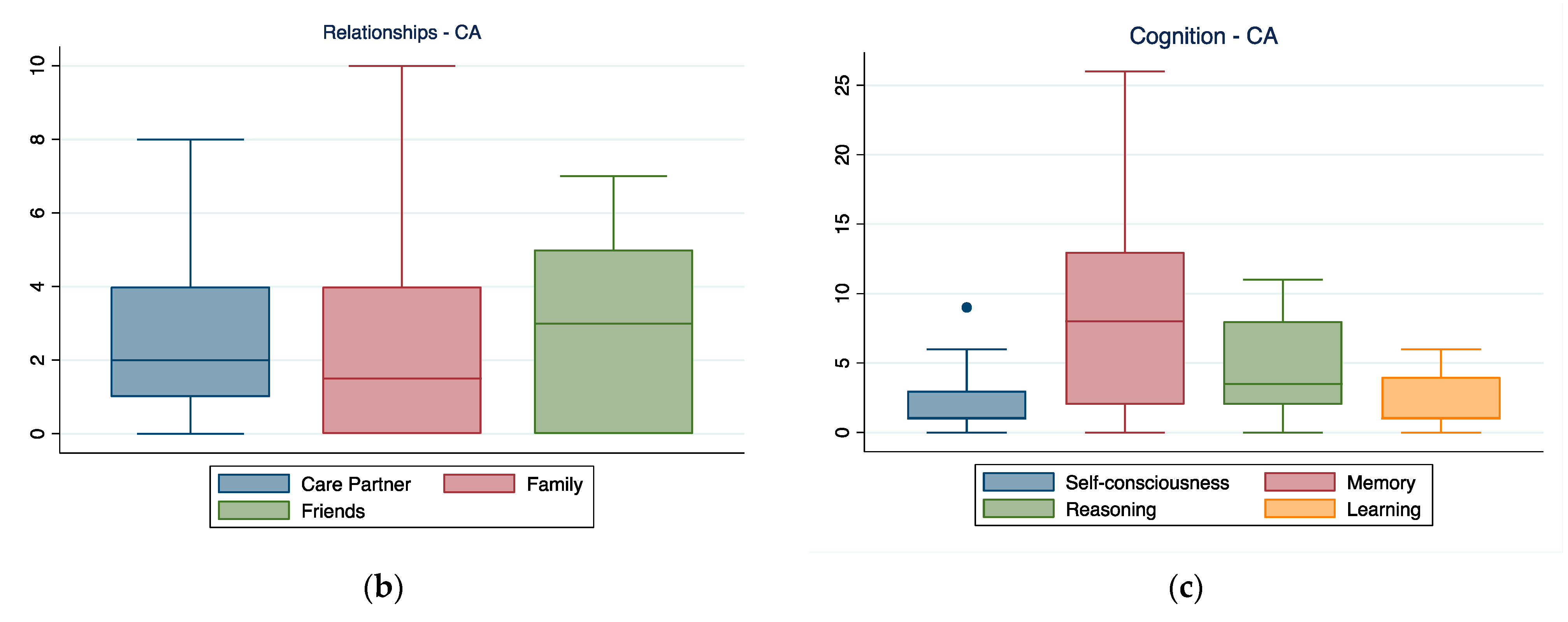
3.3. Social and Cognitive Processes
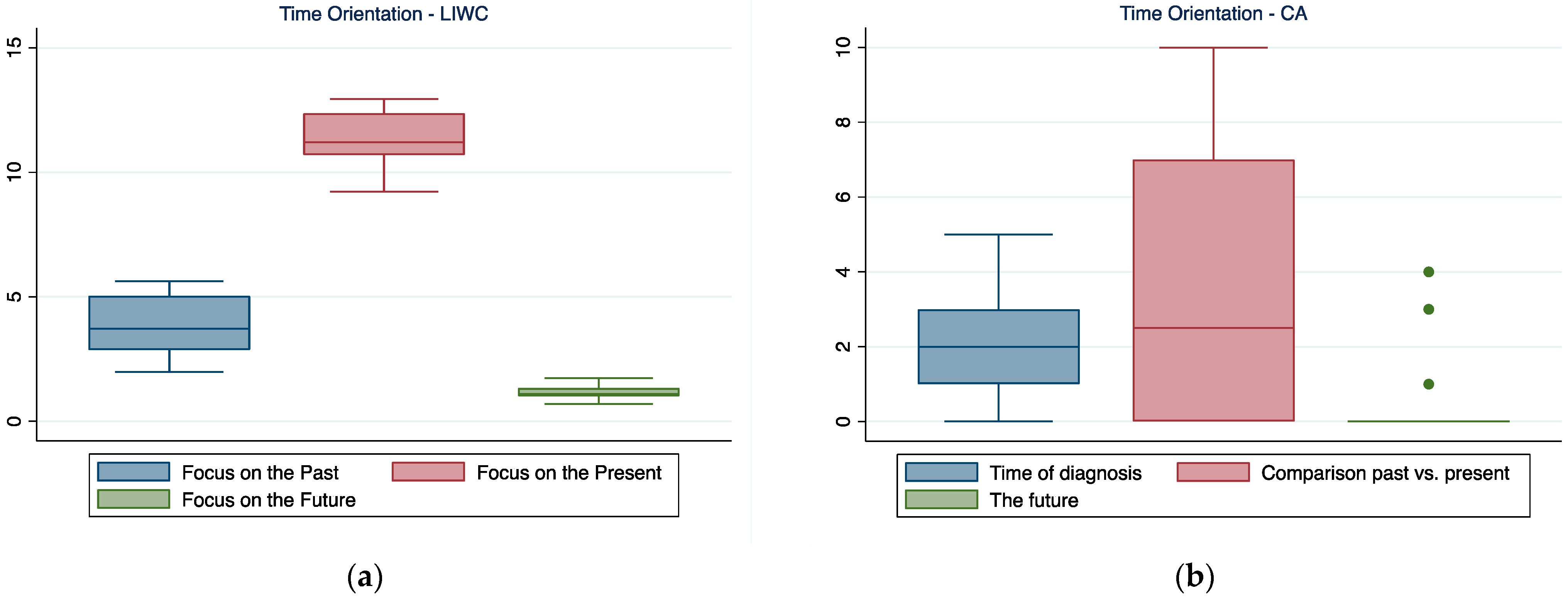
3.4. Time Orientation
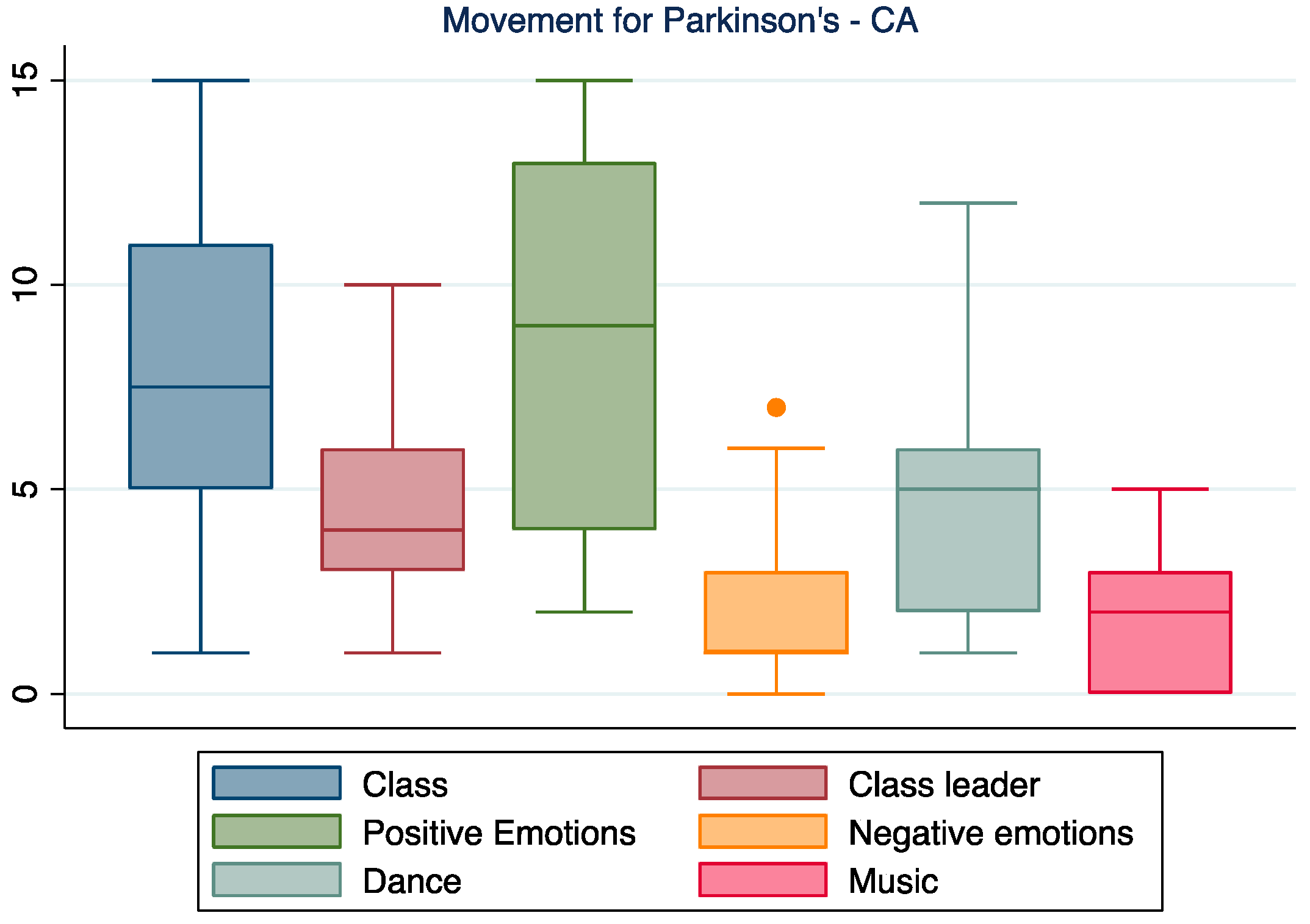
3.5. Movement for Parkinson’s
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dorsey, E.R.; Holloway, R.G.; Ravina, B.M. Biomarkers in Parkinson’s disease. Expert Rev. Neurother. 2006, 6, 823–831. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Berger, K.; Chen, H.; Leslie, D.; Mailman, R.B.; Huang, X. Projection of the prevalence of Parkinson’s disease in the coming decades: Revisited. Mov. Disord. 2018, 33, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Marras, C.; Beck, J.; Bower, J.; Roberts, E.; Ritz, B.; Ross, G.; Abbott, R.; Savica, R.; Van Den Eeden, S.; Willis, A. Prevalence of Parkinson’s disease across North America. Npj Parkinson’s Dis. 2018, 4, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foltynie, T.; Langston, J.W. Therapies to slow, stop, or reverse Parkinson’s disease. J. Parkinson’s Dis. 2018, 8, S115–S121. [Google Scholar] [CrossRef] [Green Version]
- Witt, K.; Kalbe, E.; Erasmi, R.; Ebersbach, G. Nonpharmacological treatment procedures for Parkinson’s disease. Der. Nervenarzt. 2017, 88, 383–390. [Google Scholar] [CrossRef]
- Šumec, R.; Filip, P.; Sheardová, K.; Bareš, M. Psychological benefits of nonpharmacological methods aimed for improving balance in Parkinson’s disease: A systematic review. Behav. Neurol. 2015, 2015, 620674. [Google Scholar] [CrossRef] [Green Version]
- Fancourt, D.; Finn, S. What Is the Evidence on the Role of the Arts in Improving Health and Well-Being? A Scoping Review; World Health Organization, Regional Office for Europe: Geneva, Switzerland, 2019. [Google Scholar]
- Koch, S.; Kunz, T.; Lykou, S.; Cruz, R. Effects of dance movement therapy and dance on health-related psychological outcomes: A meta-analysis. Arts Psychother. 2014, 41, 46–64. [Google Scholar] [CrossRef]
- Bearss, K.A.; DeSouza, J.F. Parkinson’s Disease Motor Symptom Progression Slowed with Multisensory Dance Learning over 3-Years: A Preliminary Longitudinal Investigation. Brain Sci. 2021, 11, 895. [Google Scholar] [CrossRef]
- Biassoni, F.; Gnerre, M.; Malaspina, E.; Di Tella, S.; Anzuino, I.; Baglio, F.; Silveri, M.C. How does prosodic deficit impact naïve listeners recognition of emotion? An analysis with speakers affected by Parkinson’s disease. Psychol. Lang. Commun. 2022, 26, 102–125. [Google Scholar] [CrossRef]
- Park, A.; Stacy, M. Non-motor symptoms in Parkinson’s disease. J. Neurol. 2009, 256, 293–298. [Google Scholar] [CrossRef]
- Zhang, Q.; Hu, J.; Wei, L.; Jia, Y.; Jin, Y. Effects of dance therapy on cognitive and mood symptoms in people with Parkinson’s disease: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2019, 36, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Alpert, P.T. The health benefits of dance. Home Health Care Manag. Pract. 2011, 23, 155–157. [Google Scholar] [CrossRef]
- Westbrook, B.K.; McKibben, H. Dance/movement therapy with groups of outpatients with Parkinson’s disease. Am. J. Danc. Ther. 1989, 11, 27–38. [Google Scholar] [CrossRef]
- Earhart, G.M. Dance as therapy for individuals with Parkinson disease. Eur. J. Phys. Rehabil. Med. 2009, 45, 231. [Google Scholar]
- McNeely, M.; Duncan, R.; Earhart, G. A comparison of dance interventions in people with Parkinson disease and older adults. Maturitas 2015, 81, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Pereira, A.P.S.; Marinho, V.; Gupta, D.; Magalhães, F.; Ayres, C.; Teixeira, S. Music therapy and dance as gait rehabilitation in patients with Parkinson disease: A review of evidence. J. Geriatr. Psychiatry Neurol. 2019, 32, 49–56. [Google Scholar] [CrossRef]
- Hackney, M.E.; Kantorovich, S.; Levin, R.; Earhart, G.M. Effects of tango on functional mobility in Parkinson’s disease: A preliminary study. J. Neurol. Phys. Ther. 2007, 31, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Hackney, M.E.; Earhart, G.M. Backward walking in Parkinson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2009, 24, 218–223. [Google Scholar] [CrossRef]
- Li, F.; Harmer, P.; Fitzgerald, K.; Eckstrom, E.; Stock, R.; Galver, J.; Maddalozzo, G.; Batya, S.S. Tai chi and postural stability in patients with Parkinson’s disease. N. Engl. J. Med. 2012, 366, 511–519. [Google Scholar] [CrossRef] [Green Version]
- Aguiar, L.P.C.; da Rocha, P.A.; Morris, M. Therapeutic dancing for Parkinson’s disease. Int. J. Gerontol. 2016, 10, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Kiepe, M.-S.; Stöckigt, B.; Keil, T. Effects of dance therapy and ballroom dances on physical and mental illnesses: A systematic review. Arts Psychother. 2012, 39, 404–411. [Google Scholar] [CrossRef]
- Batson, G. Feasibility of an intensive trial of modern dance for adults with Parkinson disease. Complement. Health Pract. Rev. 2010, 15, 65–83. [Google Scholar] [CrossRef]
- Heiberger, L.; Maurer, C.; Amtage, F.; Mendez-Balbuena, I.; Schulte-Mönting, J.; Hepp-Reymond, M.-C.; Kristeva, R. Impact of a weekly dance class on the functional mobility and on the quality of life of individuals with Parkinson’s disease. Front. Aging Neurosci. 2011, 3, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eyigor, S.; Karapolat, H.; Durmaz, B.; Ibisoglu, U.; Cakir, S. A randomized controlled trial of Turkish folklore dance on the physical performance, balance, depression and quality of life in older women. Arch. Gerontol. Geriatr. 2009, 48, 84–88. [Google Scholar] [CrossRef]
- Duncan, R.P.; Earhart, G.M. Are the effects of community-based dance on Parkinson disease severity, balance, and functional mobility reduced with time? A 2-year prospective pilot study. J. Altern. Complement. Med. 2014, 20, 757–763. [Google Scholar] [CrossRef] [Green Version]
- Lee, N.-Y.; Lee, D.-K.; Song, H.-S. Effect of virtual reality dance exercise on the balance, activities of daily living, and depressive disorder status of Parkinson’s disease patients. J. Phys. Ther. Sci. 2015, 27, 145–147. [Google Scholar] [CrossRef] [Green Version]
- McGill, A.; Houston, S.; Lee, R.Y. Dance for Parkinson’s: A new framework for research on its physical, mental, emotional, and social benefits. Complement. Ther. Med. 2014, 22, 426–432. [Google Scholar] [CrossRef]
- Shanahan, J.; Morris, M.E.; Bhriain, O.N.; Volpe, D.; Lynch, T.; Clifford, A.M. Dancing for Parkinson disease: A randomized trial of Irish set dancing compared with usual care. Arch. Phys. Med. Rehabil. 2017, 98, 1744–1751. [Google Scholar] [CrossRef] [Green Version]
- McKee, K.E.; Hackney, M.E. The effects of adapted tango on spatial cognition and disease severity in Parkinson’s disease. J. Mot. Behav. 2013, 45, 519–529. [Google Scholar] [CrossRef]
- Warburton, E.C.; Wilson, M.; Lynch, M.; Cuykendall, S. The cognitive benefits of movement reduction: Evidence from dance marking. Psychol. Sci. 2013, 24, 1732–1739. [Google Scholar] [CrossRef]
- Kalyani, H.; Sullivan, K.; Moyle, G.; Brauer, S.; Jeffrey, E.R.; Kerr, G. Impacts of dance on cognition, psychological symptoms and quality of life in Parkinson’s disease. NeuroRehabilitation 2019, 45, 273–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGarry, L.M.; Russo, F.A. Mirroring in dance/movement therapy: Potential mechanisms behind empathy enhancement. Arts Psychother. 2011, 38, 178–184. [Google Scholar] [CrossRef]
- Behrends, A.; Müller, S.; Dziobek, I. Moving in and out of synchrony: A concept for a new intervention fostering empathy through interactional movement and dance. Arts Psychother. 2012, 39, 107–116. [Google Scholar] [CrossRef]
- Kattenstroth, J.-C.; Kolankowska, I.; Kalisch, T.; Dinse, H.R. Superior sensory, motor, and cognitive performance in elderly individuals with multi-year dancing activities. Front. Aging Neurosci. 2010, 2, 31. [Google Scholar] [CrossRef] [Green Version]
- Hobeika, L.; Samson, S. Why do music-based interventions benefit persons with neurodegenerative disease? In Music and the Aging Brain; Elsevier: Amsterdam, The Netherlands, 2020; pp. 333–349. [Google Scholar]
- Zhang, M.Y. Dance for AD: A Multicomponent Intervention to Mitigate the Negative Effects of Alzheimer’s Disease; Mailman School of Public Health, Columbia University: New York, NY, USA, 2022. [Google Scholar]
- Lazarou, I.; Parastatidis, T.; Tsolaki, A.; Gkioka, M.; Karakostas, A.; Douka, S.; Tsolaki, M. International ballroom dancing against neurodegeneration: A randomized controlled trial in Greek community-dwelling elders with mild cognitive impairment. Am. J. Alzheimers Dis. Dement. 2017, 32, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Barnish, M.S.; Barran, S.M. A systematic review of active group-based dance, singing, music therapy and theatrical interventions for quality of life, functional communication, speech, motor function and cognitive status in people with Parkinson’s disease. BMC Neurol. 2020, 20, 371. [Google Scholar] [CrossRef]
- Rocha, P.A.; Slade, S.C.; McClelland, J.; Morris, M.E. Dance is more than therapy: Qualitative analysis on therapeutic dancing classes for Parkinson’s. Complement. Ther. Med. 2017, 34, 1–9. [Google Scholar] [CrossRef]
- Diaz Abrahan, V.; Justel, N.; Shifres, F. Musical improvisation: A mixed methods study on social interactions in younger and older adults. Nord. J. Music. Ther. 2022, 1–19. [Google Scholar] [CrossRef]
- Boster, J.B.; Spitzley, A.M.; Castle, T.W.; Jewell, A.R.; Corso, C.L.; McCarthy, J.W. Music improves social and participation outcomes for individuals with communication disorders: A systematic review. J. Music Ther. 2021, 58, 12–42. [Google Scholar] [CrossRef]
- Prewitt, C.M.; Charpentier, J.C.; Brosky, J.A.; Urbscheit, N.L. Effects of dance classes on cognition, depression, and self-efficacy in Parkinson’s disease. Am. J. Danc. Ther. 2017, 39, 126–141. [Google Scholar] [CrossRef]
- Iannello, P.; Biassoni, F.; Bertola, L.; Antonietti, A.; Caserta, V.A.; Panella, L. The role of autobiographical story-telling during rehabilitation among hip-fracture geriatric patients. Eur. J. Psychol. 2018, 14, 424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, M. Narrating stroke: The life-writing and fiction of brain damage. Med. Humanit. 2012, 38, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.C.; Watts, J.; List, J.-M.; Puryear, C.; Drabble, R.; Lindquist, K.A. From text to thought: How analyzing language can advance psychological science. Perspect. Psychol. Sci. 2021, 17, 805–826. [Google Scholar] [CrossRef] [PubMed]
- Tausczik, Y.R.; Pennebaker, J.W. The psychological meaning of words: LIWC and computerized text analysis methods. J. Lang. Soc. Psychol. 2010, 29, 24–54. [Google Scholar] [CrossRef]
- Renz, S.M.; Carrington, J.M.; Badger, T.A. Two strategies for qualitative content analysis: An intramethod approach to triangulation. Qual. Health Res. 2018, 28, 824–831. [Google Scholar] [CrossRef]
- Pennebaker, J.W.; Boyd, R.L.; Jordan, K.; Blackburn, K. The Development and Psychometric Properties of LIWC2015. 2015. Available online: https://repositories.lib.utexas.edu/bitstream/handle/2152/31333/LIWC2015_LanguageManual.pdf (accessed on 23 April 2022).
- Mergenthaler, E.; Bucci, W. Linking verbal and non-verbal representations: Computer analysis of referential activity. Br. J. Med. Psychol. 1999, 72, 339–354. [Google Scholar] [CrossRef] [PubMed]
- Viney, L.L. The assessment of psychological states through content analysis of verbal communications. Psychol. Bull. 1983, 94, 542. [Google Scholar] [CrossRef]
- Weintraub, W. Verbal Behavior in Everyday Life; Springer Publishing Co.: Berlin/Heidelberg, Germany, 1989. [Google Scholar]
- Mehl, M.R. Quantitative Text Analysis. In Handbook of Multimethod Measurement in Psychology; Eid, M., Diener, E., Eds.; American Psychological Association: Washington, DC, USA, 2006; pp. 141–156. [Google Scholar] [CrossRef]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef]
- Morse, J. The changing face of qualitative inquiry. Int. J. Qual. Methods 2020, 19, 1609406920909938. [Google Scholar] [CrossRef] [Green Version]
- Pennebaker, J.W. The secret life of pronouns. New Sci. 2011, 211, 42–45. [Google Scholar] [CrossRef]
- Pennebaker, J.W.; Francis, M.E. Cognitive, emotional, and language processes in disclosure. Cogn. Emot. 1996, 10, 601–626. [Google Scholar] [CrossRef]
- Barrett, D. Dreams about COVID-19 versus normative dreams: Trends by gender. Dreaming 2020, 30, 216. [Google Scholar] [CrossRef]
- Coe, K.; Scacco, J.M. Content analysis, quantitative. Int. Encycl. Commun. Res. Methods 2017, 1–11. [Google Scholar]
- Roberts, C.W. A conceptual framework for quantitative text analysis. Qual. Quant. 2000, 34, 259–274. [Google Scholar] [CrossRef]
- Kuopio, A.M.; Marttila, R.J.; Helenius, H.; Toivonen, M.; Rinne, U.K. The quality of life in Parkinson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2000, 15, 216–223. [Google Scholar] [CrossRef]
- Opara, J.; Brola, W.; Leonardi, M.; Błaszczyk, B. Quality of life in Parkinsons Disease. J. Med. Life 2012, 5, 375. [Google Scholar]
- Rutten, S.; van den Heuvel, O.A.; de Kruif, A.; Schoonmade, L.J.; Schumacher, E.I.; Vermunt, K.; Hagen, R.; van Wegen, E.E.; Rutten, K. The subjective experience of living with Parkinson’s disease: A meta-ethnography of qualitative literature. J. Parkinson’s Dis. 2021, 11, 139–151. [Google Scholar] [CrossRef]
- Hanff, A.-M.; Leist, A.K.; Fritz, J.V.; Pauly, C.; Krüger, R.; Halek, M.; Consortium, N.-P. Determinants of Self-Stigma in People with Parkinson’s Disease: A Mixed Methods Scoping Review. J. Parkinson’s Dis. 2022, 12, 509–522. [Google Scholar] [CrossRef]
- Cohn, M.A.; Mehl, M.R.; Pennebaker, J.W. Linguistic markers of psychological change surrounding September 11, 2001. Psychol. Sci. 2004, 15, 687–693. [Google Scholar] [CrossRef]
- Sotgiu, I.; Rusconi, M.L. Investigating emotions in Parkinson’s disease: What we know and what we still don’t know. Front. Psychol. 2013, 4, 336. [Google Scholar] [CrossRef] [Green Version]
- Nègre-Pagès, L.; Grandjean, H.; Lapeyre-Mestre, M.; Montastruc, J.L.; Fourrier, A.; Lépine, J.P.; Rascol, O.; Group, D.S. Anxious and depressive symptoms in Parkinson’s disease: The French cross-sectionnal DoPaMiP study. Mov. Disord. 2010, 25, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Siri, C.; Cilia, R.; De Gaspari, D.; Villa, F.; Goldwurm, S.; Marco, C.; Pezzoli, G.; Antonini, A. Psychiatric symptoms in Parkinson’s disease assessed with the SCL-90R self-reported questionnaire. Neurol. Sci. 2010, 31, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Dara, C.; Monetta, L.; Pell, M.D. Vocal emotion processing in Parkinson’s disease: Reduced sensitivity to negative emotions. Brain Res. 2008, 1188, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Lubomski, M.; Davis, R.L.; Sue, C.M. Depression in Parkinson’s disease: Perspectives from an Australian cohort. J. Affect. Disord. 2020, 277, 1038–1044. [Google Scholar] [CrossRef]
- Oguru, M.; Tachibana, H.; Toda, K.; Okuda, B.; Oka, N. Apathy and depression in Parkinson disease. J. Geriatr. Psychiatry Neurol. 2010, 23, 35–41. [Google Scholar] [CrossRef]
- Van Swol, L.M.; Ahn, P.H.; Prahl, A.; Gong, Z. Language Use in Group Discourse and Its Relationship to Group Processes. SAGE Open 2021, 11, 21582440211001852. [Google Scholar] [CrossRef]
- Perepezko, K.; Hinkle, J.T.; Shepard, M.D.; Fischer, N.; Broen, M.P.; Leentjens, A.F.; Gallo, J.J.; Pontone, G.M. Social role functioning in Parkinson’s disease: A mixed-methods systematic review. Int. J. Geriatr. Psychiatry 2019, 34, 1128–1138. [Google Scholar] [CrossRef]
- Sheppard, A.; Broughton, M.C. Promoting wellbeing and health through active participation in music and dance: A systematic review. Int. J. Qual. Stud. Health Well-Being 2020, 15, 1732526. [Google Scholar] [CrossRef] [Green Version]
- Busetto, L.; Wick, W.; Gumbinger, C. How to use and assess qualitative research methods. Neurol. Res. Pract. 2020, 2, 14. [Google Scholar] [CrossRef]
- Flick, U. Design and process in qualitative research. Companion Qual. Res. 2004, 146–152. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Examples |
|---|---|
| Summary Language Variables | |
| Analytical Thinking | / |
| Clout | / |
| Emotional tone | / |
| Linguistic dimensions | |
| Personal pronouns | |
| 1st person | I, me, mine, we, us |
| 3rd person | she, her, him, they, them |
| Psychological processes | |
| Affective processes | Happy, cried |
| Positive emotion | Love, nice, sweet |
| Negative emotion | Hurt, ugly, nasty |
| Social processes | Mate, talk, daughter, buddy |
| Cognitive processes | Cause, know, ought |
| Time orientation | |
| Past focus | Ago, did, talked |
| Present Focus | Today, is, now |
| Future Focus | May, will, soon |
| Theme | Subcategories |
|---|---|
| Relationships |
|
| Cognition |
|
| Emotions |
|
| Time |
|
| Movement for Parkinson’s |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colombo, B.; Rigby, A.; Gnerre, M.; Biassoni, F. The Effects of a Dance and Music-Based Intervention on Parkinson’s Patients’ Well-Being: An Interview Study. Int. J. Environ. Res. Public Health 2022, 19, 7519. https://doi.org/10.3390/ijerph19127519
Colombo B, Rigby A, Gnerre M, Biassoni F. The Effects of a Dance and Music-Based Intervention on Parkinson’s Patients’ Well-Being: An Interview Study. International Journal of Environmental Research and Public Health. 2022; 19(12):7519. https://doi.org/10.3390/ijerph19127519
Chicago/Turabian StyleColombo, Barbara, Alison Rigby, Martina Gnerre, and Federica Biassoni. 2022. "The Effects of a Dance and Music-Based Intervention on Parkinson’s Patients’ Well-Being: An Interview Study" International Journal of Environmental Research and Public Health 19, no. 12: 7519. https://doi.org/10.3390/ijerph19127519