
How Anti-Substance Abuse Campaigns Influence Substance Abusers’ Psychological Health in Chinese Communities: The Mediating Role of Perceived Stigma


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Sample
2.2. Measurement
2.2.1. Dependent Variables
2.2.2. Independent Variables
2.2.3. Controlled Covariates
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mak, W.W.; Poon, C.Y.; Pun, L.Y.; Cheung, S.F. Meta-Analysis of Stigma and Mental Health. Soc. Sci. Med. 2007, 65, 245–261. [Google Scholar] [CrossRef] [PubMed]
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Simon and Schuster: Delran, NJ, USA, 1963; ISBN 1-4391-8833-5. [Google Scholar]
- Jones, E.E. Social Stigma: The Psychology of Marked Relationships; WH Freeman: New York, NY, USA, 1984. [Google Scholar]
- Link, B.G.; Phelan, J.C. Conceptualizing Stigma. Annu. Rev. Sociol. 2001, 27, 363–385. [Google Scholar] [CrossRef]
- Palamar, J.J.; Halkitis, P.N.; Kiang, M.V. Perceived Public Stigma and Stigmatization in Explaining Lifetime Illicit Drug Use among Emerging Adults. Addict. Res. Theory 2013, 21, 516–525. [Google Scholar] [CrossRef]
- Schomerus, G.; Lucht, M.; Holzinger, A.; Matschinger, H.; Carta, M.G.; Angermeyer, M.C. The Stigma of Alcohol Dependence Compared with Other Mental Disorders: A Review of Population Studies. Alcohol Alcohol. Oxf. Oxfs. 2011, 46, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Hing, N.; Russell, A.M.T. How Anticipated and Experienced Stigma Can Contribute to Self-Stigma: The Case of Problem Gambling. Front. Psychol. 2017, 8, 235. [Google Scholar] [CrossRef] [Green Version]
- Pascoe, E.A.; Smart Richman, L. Perceived Discrimination and Health: A Meta-Analytic Review. Psychol. Bull. 2009, 135, 531. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.H.; Wong, L.Y.; Grivel, M.M.; Hasin, D.S. Stigma and Substance Use Disorders: An International Phenomenon. Curr. Opin. Psychiatry 2017, 30, 378–388. [Google Scholar] [CrossRef]
- Thanh, D.C.; Moland, K.M.; Fylkesnes, K. Persisting Stigma Reduces the Utilisation of HIV-Related Care and Support Services in Viet Nam. BMC Health Serv. Res. 2012, 12, 428. [Google Scholar] [CrossRef] [Green Version]
- Hammett, T.M.; Wu, Z.; Duc, T.T.; Stephens, D.; Sullivan, S.; Liu, W.; Chen, Y.; Ngu, D.; Des Jarlais, D.C. ‘Social Evils’ and Harm Reduction: The Evolving Policy Environment for Human Immunodeficiency Virus Prevention among Injection Drug Users in China and Vietnam. Addiction 2008, 103, 137–145. [Google Scholar] [CrossRef]
- Rivera, A.V.; DeCuir, J.; Crawford, N.D.; Amesty, S.; Lewis, C.F. Internalized Stigma and Sterile Syringe Use among People Who Inject Drugs in New York City, 2010–2012. Drug Alcohol Depend. 2014, 144, 259–264. [Google Scholar] [CrossRef] [Green Version]
- Latkin, C.; Davey-Rothwell, M.; Yang, J.; Crawford, N. The Relationship between Drug User Stigma and Depression among Inner-City Drug Users in Baltimore, MD. J. Urban. Health 2013, 90, 147–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelder, S.H.; Pechmann, C.; Slater, M.D.; Worden, J.K.; Levitt, A. The National Youth Anti-Drug Media Campaign. Am. J. Public Health 2002, 92, 1211–1212. [Google Scholar] [CrossRef] [PubMed]
- Luoma, J.B.; O’Hair, A.K.; Kohlenberg, B.S.; Hayes, S.C.; Fletcher, L. The Development and Psychometric Properties of a New Measure of Perceived Stigma Toward Substance Users. Subst. Use Misuse 2010, 45, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Chi, P.; Li, X.; Zhao, J.; Zhao, G. Vicious Circle of Perceived Stigma, Enacted Stigma and Depressive Symptoms Among Children Affected by HIV/AIDS in China. AIDS Behav. 2014, 18, 1054–1062. [Google Scholar] [CrossRef]
- Fortney, J.; Mukherjee, S.; Curran, G.; Fortney, S.; Han, X.; Booth, B.M. Factors Associated with Perceived Stigma for Alcohol Use and Treatment among At-Risk Drinkers. J. Behav. Health Serv. Res. 2004, 31, 418–429. [Google Scholar] [CrossRef]
- Committee on the Science of Changing Behavioral Health Social Norms; Board on Behavioral, Cognitive, and Sensory Sciences; Division of Behavioral and Social Sciences and Education; National Academies of Sciences, Engineering, and Medicine. Understanding Stigma of Mental and Substance Use Disorders; National Academies Press: Washington, DC, USA, 2016. [Google Scholar]
- Brown, S.A. Stigma towards Marijuana Users and Heroin Users. J. Psychoact. Drugs 2015, 47, 213–220. [Google Scholar] [CrossRef]
- Smith, R.; Rossetto, K.; Peterson, B.L. A Meta-Analysis of Disclosure of One’s HIV-Positive Status, Stigma and Social Support. AIDS Care 2008, 20, 1266–1275. [Google Scholar] [CrossRef]
- Decety, J.; Echols, S.; Correll, J. The Blame Game: The Effect of Responsibility and Social Stigma on Empathy for Pain. J. Cogn. Neurosci. 2010, 22, 985–997. [Google Scholar] [CrossRef]
- Dearing, R.L.; Stuewig, J.; Tangney, J.P. On the Importance of Distinguishing Shame from Guilt: Relations to Problematic Alcohol and Drug Use. Addict. Behav. 2005, 30, 1392–1404. [Google Scholar] [CrossRef] [Green Version]
- Birtel, M.D.; Wood, L.; Kempa, N.J. Stigma and Social Support in Substance Abuse: Implications for Mental Health and Well-Being. Psychiatry Res. 2017, 252, 1–8. [Google Scholar] [CrossRef]
- Keyes, K.M.; Hatzenbuehler, M.L.; McLaughlin, K.A.; Link, B.; Olfson, M.; Grant, B.F.; Hasin, D. Stigma and Treatment for Alcohol Disorders in the United States. Am. J. Epidemiol. 2010, 172, 1364–1372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crapanzano, K.A.; Hammarlund, R.; Ahmad, B.; Hunsinger, N.; Kullar, R. The Association between Perceived Stigma and Substance Use Disorder Treatment Outcomes: A Review. Subst. Abus. Rehabil. 2019, 10, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, L.; Jia, C.X. Treatments, Perceived Stigma, and Employment Outcomes among Substance Abusers in China. Healthcare 2022, 10, 130. [Google Scholar] [CrossRef] [PubMed]
- Luoma, J.B.; Nobles, R.H.; Drake, C.E.; Hayes, S.C.; O’Hair, A.; Fletcher, L.; Kohlenberg, B.S. Self-Stigma in Substance Abuse: Development of a New Measure. J. Psychopathol. Behav. Assess. 2013, 35, 223–234. [Google Scholar] [CrossRef] [Green Version]
- Steele, C.M.; Spencer, S.J.; Aronson, J. Contending with Group Image: The Psychology of Stereotype and Social Identity Threat. In Advances in Experimental Social Psychology; Elsevier: Amsterdam, The Netherlands, 2002; Volume 34, pp. 379–440. ISBN 0065-2601. [Google Scholar]
- Quinn, D.M.; Kahng, S.K.; Crocker, J. Discreditable: Stigma Effects of Revealing a Mental Illness History on Test Performance. Pers. Soc. Psychol. Bull. 2004, 30, 803–815. [Google Scholar] [CrossRef]
- Schmader, T.; Johns, M.; Forbes, C. An Integrated Process Model of Stereotype Threat Effects on Performance. Psychol. Rev. 2008, 115, 336. [Google Scholar] [CrossRef] [Green Version]
- Chawla, N.; Ostafin, B. Experiential Avoidance as a Functional Dimensional Approach to Psychopathology: An Empirical Review. J. Clin. Psychol. 2007, 63, 871–890. [Google Scholar] [CrossRef]
- Deng, Q.; Hu, M.; Yu, F.; Liu, Q.; Hao, W.; Wu, Q.; Luo, T. A Community-Based Investigation of Stigma Toward Individuals Receiving Methadone Maintenance Treatment in China: A Randomized Case Vignette Study. Front. Psychiatry 2020, 11, 1277. [Google Scholar] [CrossRef]
- Li, L.; Liang, L.-J.; Lin, C.; Feng, N.; Wu, Z. Comparison Between Urinalysis Results and Self-Reported Heroin Use Among Patients Undergoing Methadone Maintenance Treatment in China. Subst. Use Misuse 2017, 52, 1307–1314. [Google Scholar] [CrossRef] [Green Version]
- Luo, T.; Wang, J.; Li, Y.; Wang, X.; Tan, L.; Deng, Q.; Thakoor, J.P.D.; Hao, W. Stigmatization of People with Drug Dependence in China: A Community-Based Study in Hunan Province. Drug Alcohol Depend. 2014, 134, 285–289. [Google Scholar] [CrossRef]
- Zhang, C.; Li, X.; Liu, Y.; Zhou, Y.; Shen, Z.; Chen, Y. Impacts of HIV Stigma on Psychosocial Well-Being and Substance Use Behaviors Among People Living With HIV/AIDS In China: Across the Life Span. AIDS Educ. Prev. 2018, 30, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Yu, C.; Chen, X.; Hao, Y.; Ding, Y.; Wu, Z.; Wang, X. A Quasi-Experimental Study on the Effectiveness of Compulsory and Voluntary Treatment Settings for 1,299 Drug Abusers in Hunan, China. Front. Psychiatry 2021, 12, 613665. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Zhang, Y. Risk Control and Rational Recreation: A Qualitative Analysis of Synthetic Drug Use among Young Urbanites in China. Int. J. Drug Policy 2014, 25, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Duan, S.; Jin, Z.; Liu, X.; Yang, Y.; Ye, R.; Tang, R.; Gao, M.; Ding, Y.; He, N. Tobacco and Alcohol Use among Drug Users Receiving Methadone Maintenance Treatment: A Cross-Sectional Study in a Rural Prefecture of Yunnan Province, Southwest China. BMJ Open 2017, 7, e014643. [Google Scholar] [CrossRef]
- Zhang, L.; Zou, X.; Xu, Y.; Medland, N.; Deng, L.; Liu, Y.; Su, S.; Ling, L. The Decade-Long Chinese Methadone Maintenance Therapy Yields Large Population and Economic Benefits for Drug Users in Reducing Harm, HIV and HCV Disease Burden. Front. Public Health 2019, 7, 327. [Google Scholar] [CrossRef]
- Li, Y.; Zeng, X.; Zhou, H. Relationship between Anxiety and Drug Abstention Motivation in Men with Substance Use Disorders: A Cross-Sectional Study of Compulsory Isolation Rehabilitation in China. J. Ethn. Subst. Abuse 2021, 39, 171. [Google Scholar] [CrossRef]
- Yang, J.; Giummarra, M.J. Compulsory and Voluntary Drug Treatment Models in China: A Need for Improved Evidence-Based Policy and Practice to Reduce the Loaded Burden of Substance Use Disorders. Int. J. Drug Policy 2021, 92, 103063. [Google Scholar] [CrossRef]
- Blume, A.W. Advances in Substance Abuse Prevention and Treatment Interventions among Racial, Ethnic, and Sexual Minority Populations. Alcohol Res. Curr. Rev. 2016, 38, 47. [Google Scholar]
- Bobrova, N.; Rhodes, T.; Power, R.; Alcorn, R.; Neifeld, E.; Krasiukov, N.; Latyshevskaia, N.; Maksimova, S. Barriers to Accessing Drug Treatment in Russia: A Qualitative Study among Injecting Drug Users in Two Cities. Drug Alcohol Depend. 2006, 82, S57–S63. [Google Scholar] [CrossRef]
- Sun, H.; Bao, Y.; Zhou, S.; Meng, S.; Lu, L. The New Pattern of Drug Abuse in China. Curr. Opin. Psychiatry 2014, 27, 251–255. [Google Scholar] [CrossRef]
- Lu, L.; Fang, Y.; Wang, X. Drug Abuse in China: Past, Present and Future. Cell. Mol. Neurobiol. 2008, 28, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Shi, R.; Hazen, M.D. Applying the Extended Parallel Process Model to Examine Posters in the 2008 Chinese Annual Anti-Drug Campaign. J. Asian Pac. Commun. 2012, 22, 60–77. [Google Scholar] [CrossRef]
- Brockner, J.; Chen, Y.-R. The Moderating Roles of Self-Esteem and Self-Construal in Reaction to a Threat to the Self: Evidence from the People’s Republic of China and the United States. J. Pers. Soc. Psychol. 1996, 71, 603. [Google Scholar] [CrossRef] [PubMed]
- Mak, W.W.S.; Ho, C.Y.Y.; Wong, V.U.T.; Law, R.W.; Chan, R.C.H. Cultural Model of Self-Stigma among Chinese with Substance Use Problems. Drug Alcohol Depend. 2015, 155, 83–89. [Google Scholar] [CrossRef]
- Conner, K.O.; Rosen, D. “You’re Nothing but a Junkie”: Multiple Experiences of Stigma in an Aging Methadone Maintenance Population. J. Soc. Work Pract. Addict. 2008, 8, 244–264. [Google Scholar] [CrossRef]
- Gunn, A.; Guarino, H. “Not Human, Dead Already”: Perceptions and Experiences of Drug-Related Stigma among Opioid-Using Young Adults from the Former Soviet Union Living in the US. Int. J. Drug Policy 2016, 38, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Notley, C.; Maskrey, V.; Holland, R. The Needs of Problematic Drug Misusers Not in Structured Treatment–a Qualitative Study of Perceived Treatment Barriers and Recommendations for Services. Drugs Educ. Prev. Policy 2012, 19, 40–48. [Google Scholar] [CrossRef]
- Gilchrist, G.; Moskalewicz, J.; Nutt, R.; Love, J.; Germeni, E.; Valkova, I.; Kantchelov, A.; Stoykova, T.; Bujalski, M.; Poplas-Susic, T. Understanding Access to Drug and Alcohol Treatment Services in Europe: A Multi-Country Service Users’ Perspective. Drugs Educ. Prev. Policy 2014, 21, 120–130. [Google Scholar] [CrossRef]
- Lin, W.; Zhou, W. Factors Associated with the Physical and Mental Health of Drug Users Participating in Community-Based Drug Rehabilitation Programmes in China. Health Soc. Care Community 2020, 28, 584–590. [Google Scholar] [CrossRef]
- Chen, L.Y.; Strain, E.C.; Crum, R.M.; Mojtabai, R. Gender Differences in Substance Abuse Treatment and Barriers to Care among Persons with Substance Use Disorders with and without Comorbid Major Depression. J. Addict. Med. 2013, 7, 325. [Google Scholar] [CrossRef] [Green Version]
- Derogatis, L.R. BSI Brief Symptom Inventory. In Administration, Scoring, and Procedures Manual; National Computer Systems: Minneapolis, MN, USA, 1993. [Google Scholar]
- Calabrese, S.K.; Burke, S.E.; Dovidio, J.F.; Levina, O.S.; Uusküla, A.; Niccolai, L.M.; Heimer, R. Internalized HIV and Drug Stigmas: Interacting Forces Threatening Health Status and Health Service Utilization among People with HIV Who Inject Drugs in St. Petersburg, Russia. AIDS Behav. 2016, 20, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Mattoo, S.K.; Sarkar, S.; Gupta, S.; Nebhinani, N.; Parakh, P.; Basu, D. Stigma Towards Substance Use: Comparing Treatment Seeking Alcohol and Opioid Dependent Men. Int. J. Ment. Health Addict. 2015, 13, 73–81. [Google Scholar] [CrossRef]
- Ohrnberger, J.; Fichera, E.; Sutton, M. The Relationship between Physical and Mental Health: A Mediation Analysis. Soc. Sci. Med. 2017, 195, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.A.; Kramer, K.; Lewno, B.; Dumas, L.; Sacchetti, G.; Powell, E. Correlates of Self-Stigma among Individuals with Substance Use Problems. Int. J. Ment. Health Addict. 2015, 13, 687–698. [Google Scholar] [CrossRef]
- Meyers, S.A.; Earnshaw, V.A.; D’Ambrosio, B.; Courchesne, N.; Werb, D.; Smith, L.R. The Intersection of Gender and Drug Use-Related Stigma: A Mixed Methods Systematic Review and Synthesis of the Literature. Drug Alcohol Depend. 2021, 223, 108706. [Google Scholar] [CrossRef]
- Salkind, N. Encyclopedia of Research Design; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2010; ISBN 978-1-4129-6127-1. [Google Scholar]
- Preacher, K.J.; Selig, J.P. Advantages of Monte Carlo Confidence Intervals for Indirect Effects. Commun. Methods Meas. 2012, 6, 77–98. [Google Scholar] [CrossRef] [Green Version]
- Yzerbyt, V.; Muller, D.; Batailler, C.; Judd, C.M. New Recommendations for Testing Indirect Effects in Mediational Models: The Need to Report and Test Component Paths. J. Pers. Soc. Psychol. 2018, 115, 929–943. [Google Scholar] [CrossRef] [Green Version]
- Eichhorn, B.R. Common Method Variance Techniques; Cleveland State University: Cleveland, OH, USA, 2014; pp. 1–11. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics, 7th ed.; Pearson: New York, NY, USA, 2019; ISBN 978-0-13-479054-1. [Google Scholar]
- Joseph, F.; Tomas, M.G.; Christian, M.; Marko, S. (Eds.) A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM), 2nd ed.; Sage: Los Angeles, CA, USA, 2017; ISBN 978-1-4833-7744-5. [Google Scholar]
- Kenny, D.A. MEDIATION 2021. Available online: https://davidakenny.net/cm/mediate.htm (accessed on 4 March 2022).
- Beaudoin, C.E. Exploring Antismoking Ads: Appeals, Themes, and Consequences. J. Health Commun. 2002, 7, 123–137. [Google Scholar] [CrossRef]
- Achar, C.; Dunn, L.H.; Agrawal, N. Tainted by Stigma: The Interplay of Stigma and Moral Identity in Health Persuasion. J. Mark. Res. 2022, 59, 392–410. [Google Scholar] [CrossRef]
- Lewis, N.; Sznitman, S.R. You Brought It on Yourself: The Joint Effects of Message Type, Stigma, and Responsibility Attribution on Attitudes Toward Medical Cannabis: Narratives and Medical Cannabis Policy. J. Commun. 2017, 67, 181–202. [Google Scholar] [CrossRef]
- Dietz-Uhler, B.; Murrell, A. Effects of Social Identity and Threat on Self-Esteem and Group Attributions. Group Dyn. Theory Res. Pract. 1998, 2, 24. [Google Scholar] [CrossRef]
- Crockett, K.B.; Kalichman, S.C.; Kalichman, M.O.; Cruess, D.G.; Katner, H.P. Experiences of HIV-Related Discrimination and Consequences for Internalised Stigma, Depression and Alcohol Use. Psychol. Health 2019, 34, 796–810. [Google Scholar] [CrossRef] [PubMed]
- Luoma, J.B.; Kohlenberg, B.S.; Hayes, S.C.; Bunting, K.; Rye, A.K. Reducing Self-Stigma in Substance Abuse through Acceptance and Commitment Therapy: Model, Manual Development, and Pilot Outcomes. Addict. Res. Theory 2008, 16, 149–165. [Google Scholar] [CrossRef]
- Mittal, D.; Sullivan, G.; Chekuri, L.; Allee, E.; Corrigan, P.W. Empirical Studies of Self-Stigma Reduction Strategies: A Critical Review of the Literature. Psychiatr. Serv. 2012, 63, 974–981. [Google Scholar] [CrossRef] [Green Version]
- Fishbein, M.; Hall-Jamieson, K.; Zimmer, E.; von Haeften, I.; Nabi, R. Avoiding the Boomerang: Testing the Relative Effectiveness of Antidrug Public Service Announcements Before a National Campaign. Am. J. Public Health 2002, 92, 238–245. [Google Scholar] [CrossRef]
- Dillard, J.P.; Shen, L.; Vail, R.G. Does Perceived Message Effectiveness Cause Persuasion or Vice Versa? 17 Consistent Answers. Hum. Commun. Res. 2007, 33, 467–488. [Google Scholar] [CrossRef]
- Worden, J.K.; Slater, M.D. Theory and Practice in the National Youth Anti-Drug Media Campaign. Soc. Mark. Q. 2004, 10, 13–27. [Google Scholar] [CrossRef]


{kind=link}
| Female | Male | Total | |
|---|---|---|---|
| N | 301 | 3156 | 3457 |
| (8.71%) | (91.29%) | (100.00%) | |
| N of employed | 210 | 2387 | 2597 |
| (69.77%) | (75.63%) | (75.12%) | |
| N of married | 137 | 1771 | 1908 |
| (45.97%) | (56.42%) | (55.51%) | |
| N of using Heroin | 52 | 1042 | 1094 |
| (17.28%) | (33.02%) | (31.56%) | |
| N of using Methamphetamine | 182 | 1712 | 1894 |
| (60.47%) | (54.25%) | (54.65%) | |
| N of using other types of substances | 42 | 455 | 497 |
| (14.24%) | (14.67%) | (14.34%) | |
| M physical unhealth (days per week) | 0.55 | 0.64 | 0.63 |
| (0.08) | (0.03) | (1.48) | |
| M of personal monthly income (1000 CNY) | 2.37 | 2.75 | 2.72 |
| (0.10) | (0.03) | (1.61) | |
| M of abstinence duration (months) | 3.26 | 3.29 | 3.29 |
| (0.06) | (0.02) | (1.04) | |
| M of years of education | 8.76 | 8.54 | 8.56 |
| (0.17) | (0.05) | (2.80) | |
| M of years of age | 34.38 | 38.15 | 37.82 |
| (0.50) | (0.16) | (9.07) |
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Anxiety | — | |||||
| 2. Depression | 0.88 *** | — | ||||
| 3. Somatization | 0.87 *** | 0.84 *** | — | |||
| 4. Perceived stigma | 0.18 *** | 0.18 *** | 0.18 *** | — | ||
| 5. POH-SA | 0.14 *** | 0.13 *** | 0.13 *** | 0.86 *** | — | |
| 6. POH-S | 0.07 *** | 0.08 *** | 0.09 *** | 0.01 | −0.01 | — |
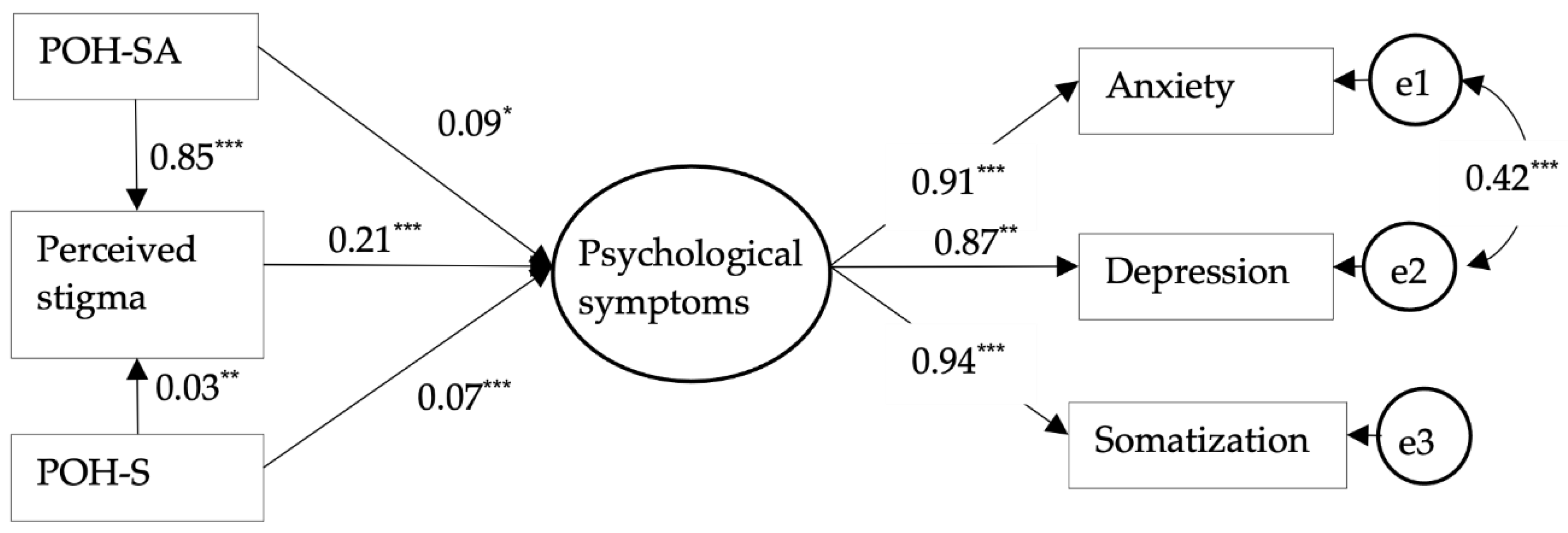
| Variables | →POH-SA | →POH-S | →Perceived Stigma | →Psychological Symptoms | |||
|---|---|---|---|---|---|---|---|
| POH-SA | 0.85 *** | 0.09 * | |||||
| POH-S | 0.03 ** | 0.07 *** | |||||
| Perceived stigma | 0.21 *** | ||||||
| Controlled Covariates | |||||||
| Type of substance | |||||||
| (Base = no usage) | |||||||
| -Heroin | −0.03 | 0.03 | 0.01 | −0.01 | |||
| -Methamphetamines | 0.06 ** | 0.06 ** | 0.02 * | −0.01 | |||
| -Other | 0.00 | 0.11 *** | 0.01 | 0.06 ** | |||
| Abstinence (months) | −0.06 *** | 0.02 | −0.03 ** | −0.05 ** | |||
| Physical unhealth | 0.06 ** | 0.04 | 0.01 | 0.34 *** | |||
| Demographics | |||||||
| Employment status | −0.03 | −0.05 * | 0.03 ** | −0.07 ** | |||
| Monthly income (CNY) | −0.03 | 0.05 * | −0.04 ** | −0.07 *** | |||
| Male (Base = female) | 0.02 | 0.01 | 0.02 | −0.06 | |||
| Married (Base = others) | 0.06 ** | −0.04 | −0.04 | 0.03 | |||
| Age (years) | −0.02 | 0.06 ** | 0.03 * | 0.04 | |||
| Education (years) | 0.01 | 0.01 | −0.01 | −0.02 | |||
| Factor loadings for indicators of the latent variable | |||||||
| Psychological symptoms -> | Anxiety | Depression | Somatization | ||||
| Factor Loading | 0.91 *** | 0.87 *** | 0.94 *** | ||||
| Model-fit index | |||||||
| = 3.57; CFI = 0.99; TLI = 0.98; RMSEA = 0.03, with 90% CI = [0.02–0.04] | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeng, Y.; Han, L.; Cheng, Y.; Jia, C.X. How Anti-Substance Abuse Campaigns Influence Substance Abusers’ Psychological Health in Chinese Communities: The Mediating Role of Perceived Stigma. Int. J. Environ. Res. Public Health 2022, 19, 6687. https://doi.org/10.3390/ijerph19116687
Zeng Y, Han L, Cheng Y, Jia CX. How Anti-Substance Abuse Campaigns Influence Substance Abusers’ Psychological Health in Chinese Communities: The Mediating Role of Perceived Stigma. International Journal of Environmental Research and Public Health. 2022; 19(11):6687. https://doi.org/10.3390/ijerph19116687
Chicago/Turabian StyleZeng, Yonghui, Li Han, Yu Cheng, and Cindy Xinshan Jia. 2022. "How Anti-Substance Abuse Campaigns Influence Substance Abusers’ Psychological Health in Chinese Communities: The Mediating Role of Perceived Stigma" International Journal of Environmental Research and Public Health 19, no. 11: 6687. https://doi.org/10.3390/ijerph19116687