
Conjunctional Relationship between Serum Uric Acid and Serum Nickel with Non-Alcoholic Fatty Liver Disease in Men: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
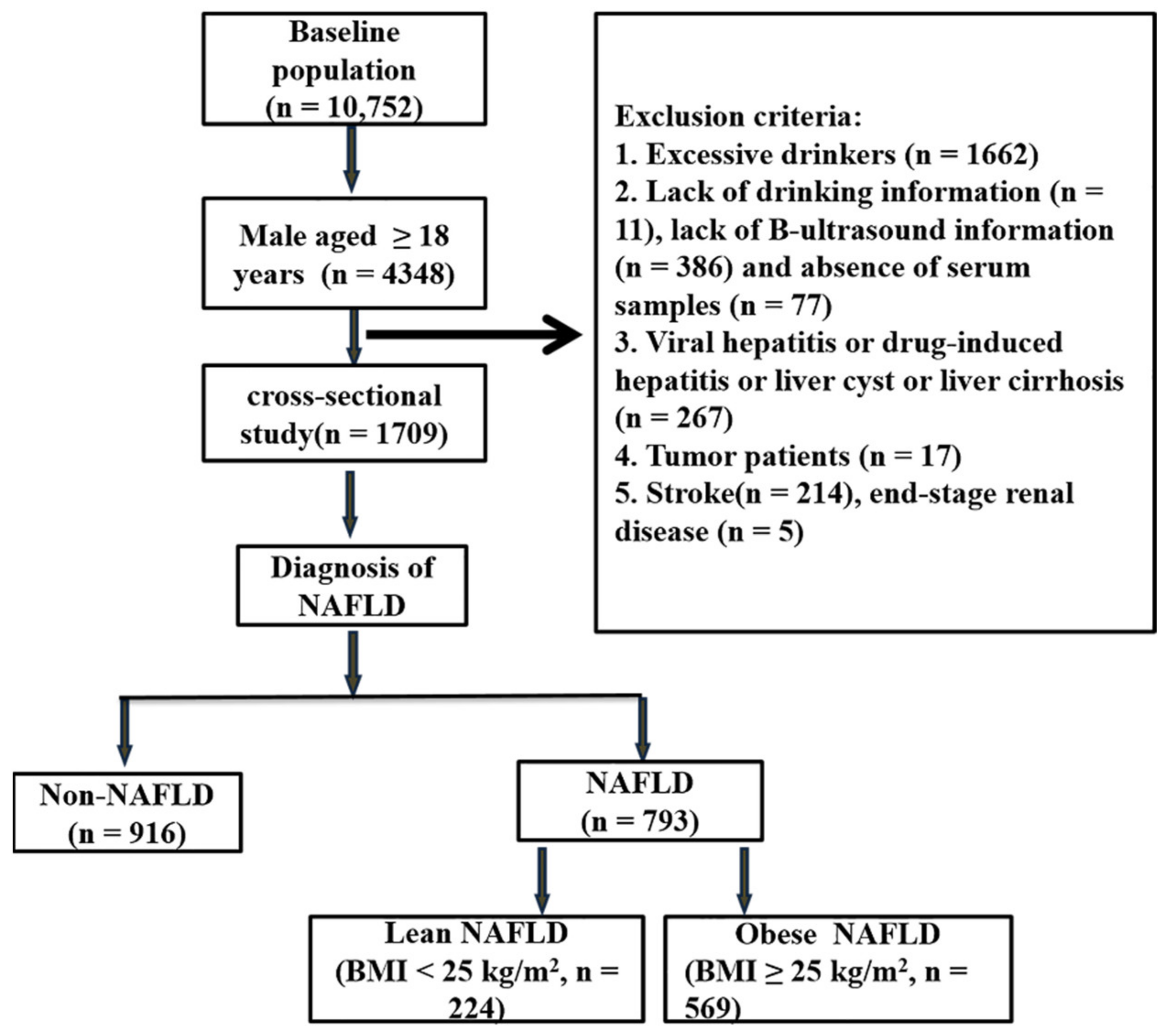
2.1. Study Design and Subjects
2.2. Data Collection and Definitions
2.3. Diagnosis of NAFLD
2.4. Assessment of Serum Ni
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Men Participants
3.2. Basic Characteristics after Quartile of SUA and Serum Nickel
3.3. Binary Logistic Regression Analysis of the Association between SUA and Serum Ni with NAFLD
3.4. Comparison of SUA and Serum Ni in Lean NAFLD, Obese NAFLD, and Control Group
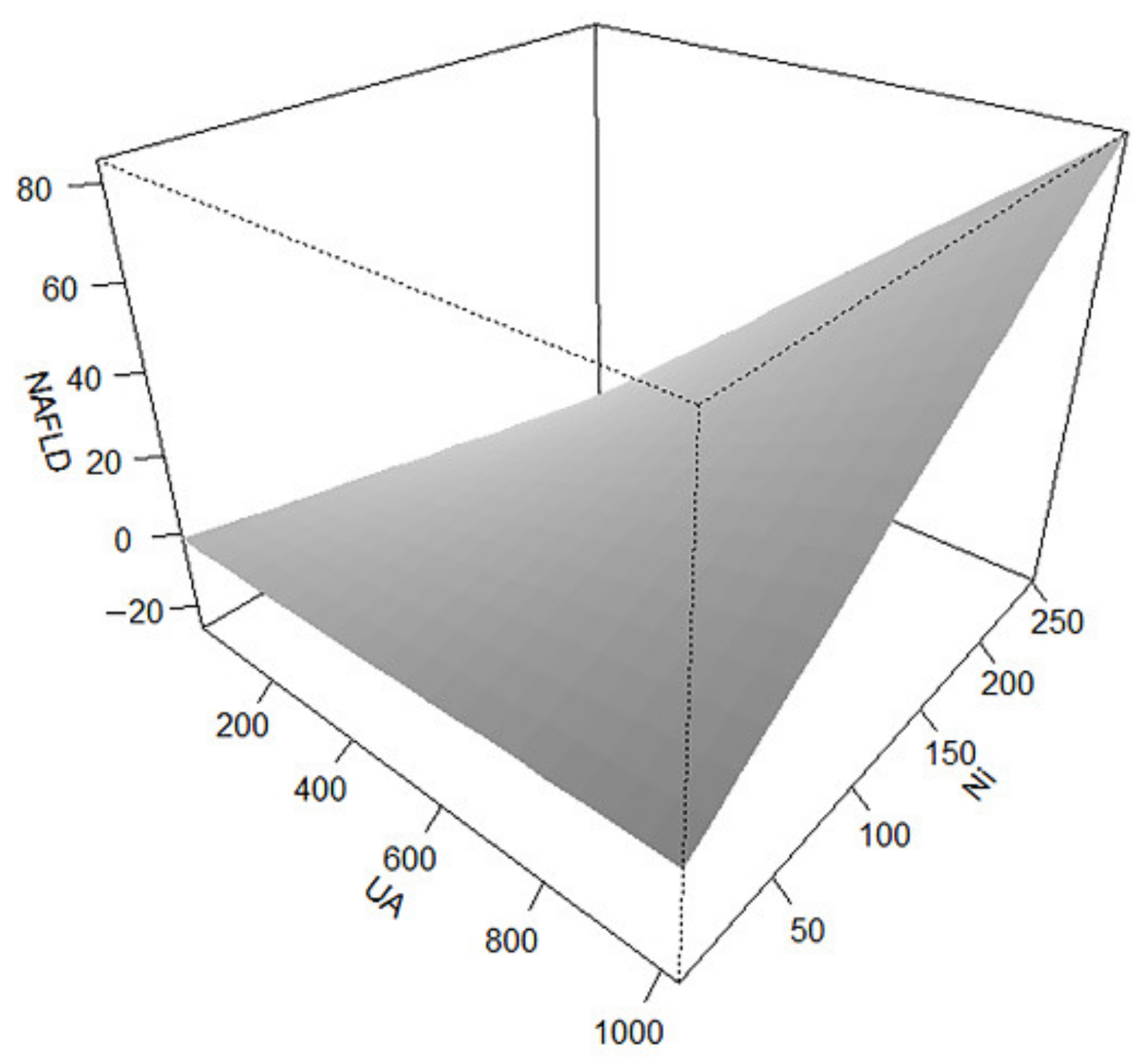
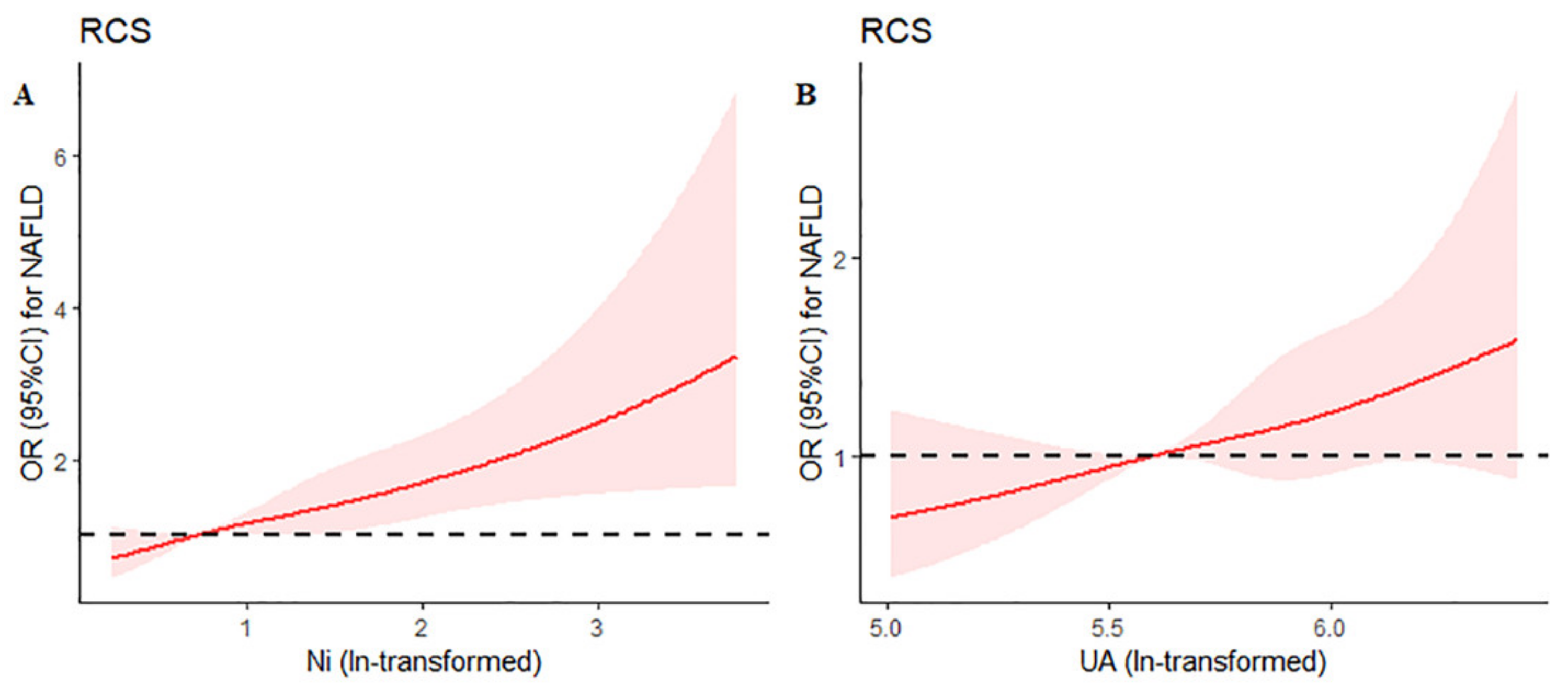
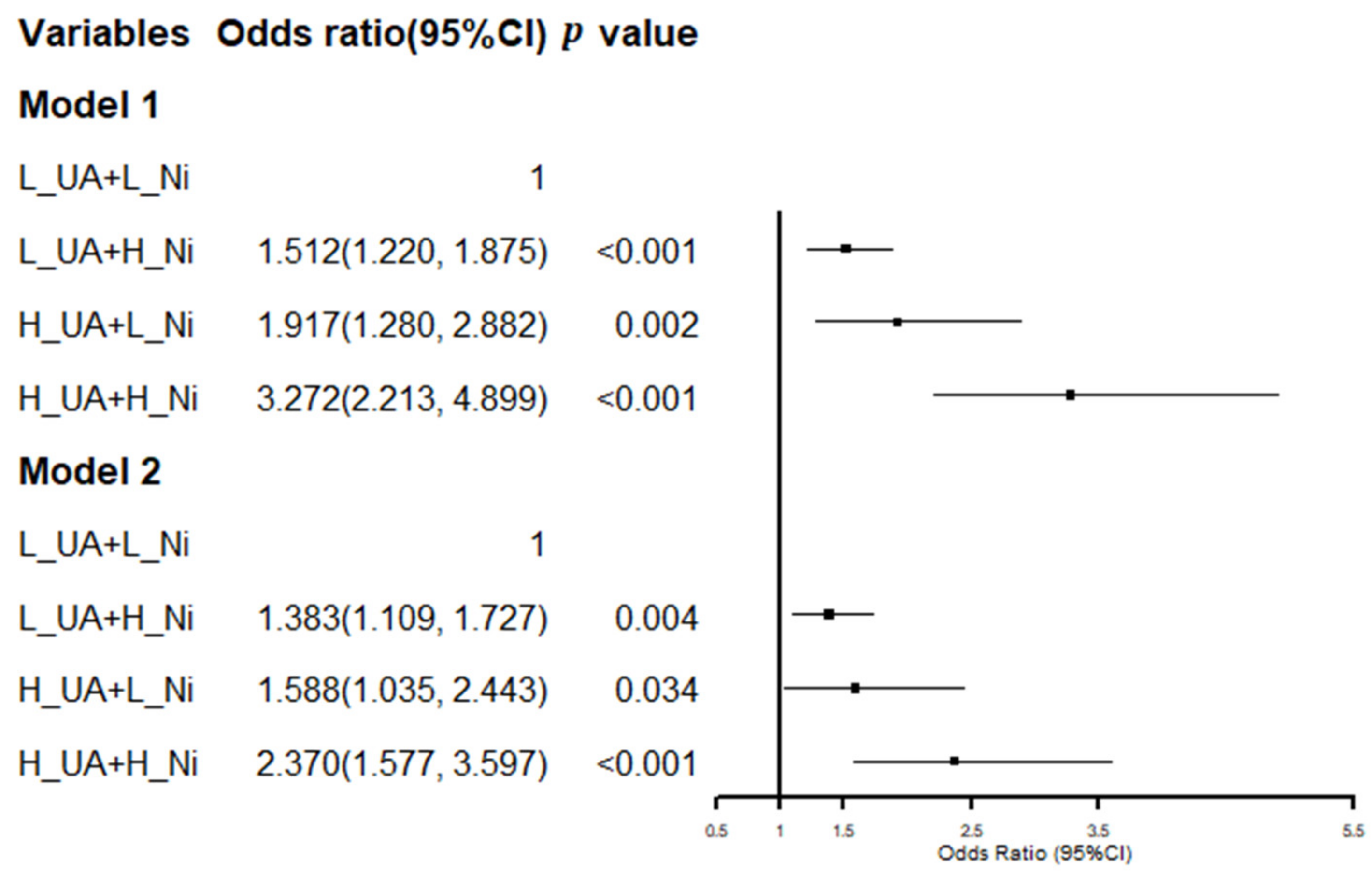
3.5. Conjunctional Relationship of SUA and Serum Ni on NAFLD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, F.; Zhou, J.; Wang, W.; Zhang, X.J.; Ji, Y.X.; Zhang, P.; She, Z.G.; Zhu, L.; Cai, J.; Li, H. Unexpected Rapid Increase in the Burden of NAFLD in China From 2008 to 2018: A Systematic Review and Meta-Analysis. Hepatology 2019, 70, 119–133. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, J.G. Epidemiology of alcoholic and nonalcoholic fatty liver disease in China. J. Gastroenterol. Hepatol. 2013, 28 (Suppl. 1), 11–17. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhou, F.; Wang, W.; Zhang, X.J.; Ji, Y.X.; Zhang, P.; She, Z.G.; Zhu, L.; Cai, J.; Li, H. Epidemiological Features of NAFLD From 1999 to 2018 in China. Hepatology 2020, 71, 1851–1864. [Google Scholar] [CrossRef]
- Li, X.D.; Qiu, B.H.; Su, F.C.; Sun, S.X. Gender impacts on the correlations between nonalcoholic fatty liver disease and hypertension in a Chinese population aged 45–60 y. Clin. Exp. Hypertens. 2016, 38, 639–643. [Google Scholar] [CrossRef]
- Nozaki, Y.; Petersen, M.C.; Zhang, D.; Vatner, D.F.; Perry, R.J.; Abulizi, A.; Haedersdal, S.; Zhang, X.M.; Butrico, G.M.; Samuel, V.T.; et al. Metabolic control analysis of hepatic glycogen synthesis in vivo. Proc. Natl. Acad. Sci. USA 2020, 117, 8166–8176. [Google Scholar] [CrossRef] [Green Version]
- Younossi, Z.M.; Stepanova, M.; Younossi, Y.; Golabi, P.; Mishra, A.; Rafiq, N.; Henry, L. Epidemiology of chronic liver diseases in the USA in the past three decades. Gut 2020, 69, 564–568. [Google Scholar] [CrossRef]
- Ma, Z.; Zhang, J.; Kang, X.; Xu, C.; Sun, C.; Tao, L.; Zheng, D.; Han, Y.; Li, Q.; Guo, X.; et al. Hyperuricemia precedes non-alcoholic fatty liver disease with abdominal obesity moderating this unidirectional relationship: Three longitudinal analyses. Atherosclerosis 2020, 311, 44–51. [Google Scholar] [CrossRef]
- Lin, Y.C.; Lian, I.B.; Kor, C.T.; Chang, C.C.; Su, P.Y.; Chang, W.T.; Liang, Y.F.; Su, W.W.; Soon, M.S. Association between soil heavy metals and fatty liver disease in men in Taiwan: A cross sectional study. BMJ Open 2017, 7, e014215. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Zhao, L.; Liu, L.; Li, Y.; Sun, J.; Liu, Y. Relationship between serum uric acid level and nonalcoholic fatty liver disease in type 2 diabetes patients. Medicine 2021, 100, e26946. [Google Scholar] [CrossRef]
- Syamala, S.; Li, J.; Shankar, A. Association between serum uric acid and prehypertension among US adults. J. Hypertens. 2007, 25, 1583–1589. [Google Scholar] [CrossRef]
- Yuan, H.; Yu, C.; Li, X.; Sun, L.; Zhu, X.; Zhao, C.; Zhang, Z.; Yang, Z. Serum Uric Acid Levels and Risk of Metabolic Syndrome: A Dose-Response Meta-Analysis of Prospective Studies. J. Clin. Endocrinol. Metab. 2015, 100, 4198–4207. [Google Scholar] [CrossRef] [Green Version]
- Lanaspa, M.A.; Sanchez-Lozada, L.G.; Choi, Y.J.; Cicerchi, C.; Kanbay, M.; Roncal-Jimenez, C.A.; Ishimoto, T.; Li, N.; Marek, G.; Duranay, M.; et al. Uric acid induces hepatic steatosis by generation of mitochondrial oxidative stress: Potential role in fructose-dependent and -independent fatty liver. J. Biol. Chem. 2012, 287, 40732–40744. [Google Scholar] [CrossRef] [Green Version]
- Ballestri, S.; Nascimbeni, F.; Romagnoli, D.; Lonardo, A. The independent predictors of non-alcoholic steatohepatitis and its individual histological features, Insulin resistance, serum uric acid, metabolic syndrome, alanine aminotransferase and serum total cholesterol are a clue to pathogenesis and candidate targets for treatment. Hepatol. Res. 2016, 46, 1074–1087. [Google Scholar]
- Wan, X.; Xu, C.; Lin, Y.; Lu, C.; Li, D.; Sang, J.; He, H.; Liu, X.; Li, Y.; Yu, C. Uric acid regulates hepatic steatosis and insulin resistance through the NLRP3 inflammasome-dependent mechanism. J. Hepatol. 2016, 64, 925–932. [Google Scholar] [CrossRef]
- Lonardo, A.; Loria, P.; Leonardi, F.; Borsatti, A.; Neri, P.; Pulvirenti, M.; Verrone, A.M.; Bagni, A.; Bertolotti, M.; Ganazzi, D.; et al. Fasting insulin and uric acid levels but not indices of iron metabolism are independent predictors of non-alcoholic fatty liver disease: A case-control study. Dig. Liver Dis. 2002, 34, 204–211. [Google Scholar] [CrossRef]
- Seo, Y.B.; Han, A.L. Association of the Serum Uric Acid-to-Creatinine Ratio with Nonalcoholic Fatty Liver Disease Diagnosed by Computed Tomography. Metab. Syndr. Relat. Disord. 2021, 19, 70–75. [Google Scholar] [CrossRef]
- Wu, S.J.; Zhu, G.Q.; Ye, B.Z.; Kong, F.Q.; Zheng, Z.X.; Zou, H.; Shi, K.Q.; Lin, L.; Braddock, M.; Huang, W.J.; et al. Association between sex-specific serum uric acid and non-alcoholic fatty liver disease in Chinese adults: A large population-based study. Medicine 2015, 94, e802. [Google Scholar] [CrossRef]
- Fan, N.; Zhang, L.; Xia, Z.; Peng, L.; Wang, Y.; Peng, Y. Sex-Specific Association between Serum Uric Acid and Nonalcoholic Fatty Liver Disease in Type 2 Diabetic Patients. J. Diabetes Res. 2016, 2016, 3805372. [Google Scholar] [CrossRef] [Green Version]
- Ali, H.; Khan, E. Bioaccumulation of Cr, Ni, Cd and Pb in the Economically Important Freshwater Fish Schizothorax plagiostomus from Three Rivers of Malakand Division, Pakistan: Risk Assessment for Human Health. Bull. Environ. Contam. Toxicol. 2019, 102, 77–83. [Google Scholar] [CrossRef]
- Ronda, O.; Grządka, E.; Ostolska, I.; Orzeł, J.; Cieślik, B.M. Accumulation of radioisotopes and heavy metals in selected species of mushrooms. Food Chem. 2022, 367, 13067. [Google Scholar] [CrossRef]
- Babaahmadifooladi, M.; Jacxsens, L. Chronic dietary exposure to nickel from selected foods consumed in Belgium. Food Addit. Contam. Part A Chem. Anal Control Expo Risk Assess. 2021, 38, 95–112. [Google Scholar] [CrossRef]
- Genchi, G.; Carocci, A.; Lauria, G.; Sinicropi, M.S.; Catalano, A. Nickel: Human Health and Environmental Toxicology. Int. J. Environ. Res. Public Health 2020, 17, 679. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, M.S.; Ashraf, M. Essential roles and hazardous effects of nickel in plants. Rev. Environ. Contam. Toxicol. 2011, 214, 125–167. [Google Scholar]
- Adjroud, O. The toxic effects of nickel chloride on liver, erythropoiesis, and development in Wistar albino preimplanted rats can be reversed with selenium pretreatment. Environ. Toxicol. 2013, 28, 290–298. [Google Scholar] [CrossRef]
- Owumi, S.E.; Olayiwola, Y.O.; Alao, G.E.; Gbadegesin, M.A.; Odunola, O.A. Cadmium and nickel co-exposure exacerbates genotoxi-city and not oxido-inflammatory stress in liver and kidney of rats: Protective role of omega-3 fatty acid. Environ. Toxicol. 2020, 35, 231–241. [Google Scholar] [CrossRef]
- Buzzetti, E.; Pinzani, M.; Tsochatzis, E.A. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabo-lism 2016, 65, 1038–1048. [Google Scholar] [CrossRef]
- Wen, W.L.; Wang, C.W.; Wu, D.W.; Chen, S.C.; Hung, C.H.; Kuo, C.H. Associations of Heavy Metals with Metabolic Syndrome and Anthropometric Indices. Nutrients 2020, 12, 2666. [Google Scholar] [CrossRef]
- Liu, X.; Mao, Z.; Li, Y.; Wu, W.; Zhang, X.; Huo, W.; Yu, S.; Shen, L.; Li, L.; Tu, R.; et al. Cohort Profile: The Henan Rural Cohort: A prospective study of chronic non-communicable diseases. Int. J. Epidemiol. 2019, 48, 1756–1756j. [Google Scholar] [CrossRef]
- Mei, Y.X.; Zhang, Z.X.; Wu, H.; Hou, J.; Liu, X.T.; Sang, S.X.; Mao, Z.X.; Zhang, W.H.; Yang, D.B.; Wang, C.J. Health-Related Quality of Life and Its Related Factors in Survivors of Stroke in Rural China: A Large-Scale Cross-Sectional Study. Front. Public Health 2022, 10, 810185. [Google Scholar] [CrossRef]
- Chinese Nutrition Society. The Dietary Guidelines for Chinese Residents; The Tibet People’s Publishing House: Lhasa, China, 2011; pp. 97–197, 198. [Google Scholar]
- VanWagner, L.B.; Armstrong, M.J. Lean NAFLD: A not so benign condition? Hepatol. Commun. 2018, 2, 5–8. [Google Scholar] [CrossRef]
- Lin, J.W.; Tsai, K.Z.; Chen, K.W.; Su, F.Y.; Li, Y.H.; Lin, Y.P.; Han, C.L.; Lin, F.; Lin, Y.K.; Hsieh, C.B.; et al. Sex-Specific Association Between Serum Uric Acid and Elevated Alanine Aminotransferase in a Military Cohort: The CHIEF Study. Endocr. Metab. Immune Disord. Drug Targets 2019, 19, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Christensen, O.B.; Möller, H.; Andrasko, L.; Lagesson, V. Nickel concentration of blood, urine and sweat after oral administration. Contact Dermatitis. 1979, 5, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Templeton, D.M.; Sunderman, F.W., Jr.; Herber, R.F. Tentative reference values for nickel concentrations in human serum, plasma, blood, and urine: Evaluation according to the TRACY protocol. Sci. Total Environ. 1994, 148, 243–251. [Google Scholar] [CrossRef]
- Fatty Liver and Alcoholic Liver Disease Group, Hepatology Branch, Chinese Medical Association; Fatty Liver Disease Expert Committee, Chinese Medical Association. Guidelines for the Prevention and Treatment of Non-Alcoholic Fatty Liver Disease (2018 Update). J. Pract. Hepatol. 2018, 21, 177–186. [Google Scholar]
- Li, H.; Guo, M.; An, Z.; Meng, J.; Jiang, J.; Song, J.; Wu, W. Prevalence and Risk Factors of Metabolic Associated Fatty Liver Disease in Xinxiang, China. Int. J. Environ. Res. Public Health 2020, 17, 1818. [Google Scholar] [CrossRef] [Green Version]
- Zheng, X.; Gong, L.; Luo, R.; Chen, H.; Peng, B.; Ren, W.; Wang, Y. Serum uric acid and non-alcoholic fatty liver disease in non-obesity Chinese adults. Lipids Health Dis. 2017, 16, 202. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.L.; Wu, F.Z.; Lin, K.H.; Chen, Y.H.; Wu, P.C.; Chen, Y.H.; Chen, C.S.; Wang, W.H.; Mar, G.Y.; Yu, H.C. Role of Fatty Liver Index and Metabolic Factors in the Prediction of Nonalcoholic Fatty Liver Disease in a Lean Population Receiving Health Checkup. Clin. Transl. Gastroenterol. 2019, 10, e00042. [Google Scholar] [CrossRef]
- Eshraghian, A.; Nikeghbalian, S.; Geramizadeh, B.; Kazemi, K.; Shamsaeefar, A.; Malek-Hosseini, S.A. Characterization of biopsy proven non-alcoholic fatty liver disease in healthy non-obese and lean population of living liver donors: The impact of uric acid. Clin. Res. Hepatol. Gastroenterol. 2020, 44, 572–578. [Google Scholar] [CrossRef]
- Oyabambi, A.O.; Olaniyi, K.S.; Soladoye, A.O.; Olatunji, L.A. Suppression of uric acid and lactate production by sodium acetate ameliorates hepatic triglyceride accumulation in fructose-insulin resistant pregnant rats. Environ. Toxicol. Pharmacol. 2020, 80, 103452. [Google Scholar] [CrossRef]
- Liu, C.Q.; He, C.M.; Chen, N.; Wang, D.; Shi, X.; Liu, Y.; Zeng, X.; Yan, B.; Liu, S.; Yang, S.; et al. Serum uric acid is independently and linearly associated with risk of nonalcoholic fatty liver disease in obese Chinese adults. Sci. Rep. 2016, 6, 38605. [Google Scholar] [CrossRef] [Green Version]
- Mosca, A.; Nobili, V.; Vito, R.; Crudele, A.; Scorletti, E.; Villani, A.; Alisi, A.; Byrne, C.D. Serum uric acid concentrations and fructose consumption are independently associated with NASH in children and adolescents. J. Hepatol. 2017, 66, 1031–1036. [Google Scholar] [CrossRef] [Green Version]
- Wei, F.; Li, J.; Chen, C.; Zhang, K.; Cao, L.; Wang, X.; Ma, J.; Feng, S.; Li, W.D. Higher Serum Uric Acid Level Predicts Non-alcoholic Fatty Liver Disease: A 4-Year Prospective Cohort Study. Front. Endocrinol. 2020, 11, 179. [Google Scholar] [CrossRef] [Green Version]
- Hwang, I.C.; Suh, S.Y.; Suh, A.R.; Ahn, H.Y. The relationship between normal serum uric acid and nonalcoholic fatty liver disease. J. Korean Med. Sci. 2011, 26, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Li, D.; Song, X.; Liu, F.; Wang, X.; Ma, Q.; Zhang, X.; Li, X. Joint associations of serum uric acid and ALT with NAFLD in elderly men and women: A Chinese cross-sectional study. J. Transl. Med. 2018, 16, 285. [Google Scholar] [CrossRef]
- Yu, X.L.; Shu, L.; Shen, X.M.; Zhang, X.Y.; Zheng, P.F. Gender difference on the relationship between hyperuricemia and nonal-coholic fatty liver disease among Chinese: An observational study. Medicine 2017, 96, e8164. [Google Scholar] [CrossRef]
- Das, K.K.; Gupta, A.D.; Dhundasi, S.A.; Patil, A.M.; Das, S.N.; Ambekar, J.G. Effect of L-ascorbic acid on nickel-induced alterations in serum lipid profiles and liver histopathology in rats. J. Basic Clin. Physiol. Pharmacol. 2006, 17, 29–44. [Google Scholar] [CrossRef]
- Varga, I.; Szebeni, A.; Szoboszlai, N. Determination of trace elements in human liver biopsy samples by ICP-MS and TXRF: Hepatic steatosis and nickel accumulation. J. Basic Clin. Physiol. Pharmacol. 2006, 17, 29–44. [Google Scholar] [CrossRef]
- Lusi, E.A.; Di Ciommo, V.M.; Patrissi, T.; Guarascio, P. High prevalence of nickel allergy in an overweight female population: A pilot observational analysis. PLoS ONE 2015, 10, e0123265. [Google Scholar] [CrossRef]
- Cortés, S.; Zúñiga-Venegas, L.; Pancetti, F.; Covarrubias, A.; Ramírez-Santana, M.; Adaros, H.; Muñoz, L. A Positive Relationship between Exposure to Heavy Metals and Development of Chronic Diseases: A Case Study from Chile. Int. J. Environ. Res. Public Health 2021, 18, 1419. [Google Scholar] [CrossRef]
- Rizwan, M.; Imtiaz, M.; Dai, Z.; Mehmood, S.; Adeel, M.; Liu, J.; Tu, S. Nickel stressed responses of rice in Ni subcellular distribution, antioxidant production, and osmolyte accumulation. Environ. Sci. Pollut. Res. Int. 2017, 24, 20587–20598. [Google Scholar] [CrossRef]
- Filatova, D.; Cherpak, C. Mechanisms of Nickel-Induced Cell Damage in Allergic Contact Dermatitis and Nutritional Intervention Strategies. Endocr. Metab. Immune Disord. Drug Targets 2020, 20, 1010–1014. [Google Scholar] [CrossRef]
- Dahmen-Ben Moussa, I.; Bellassoued, K.; Athmouni, K.; Naifar, M.; Chtourou, H.; Ayadi, H.; Makni-Ayadi, F.; Sayadi, S.; El Feki, A.; Dhouib, A. Protective effect of Dunaliella sp., lipid extract rich in polyunsaturated fatty acids, on hepatic and renal toxicity induced by nickel in rats. Toxicol. Mech. Methods 2016, 26, 221–230. [Google Scholar] [CrossRef]
- Kadi, I.E.; Dahdouh, F. Vitamin C pretreatment protects from nickel-induced acute nephrotoxicity in mice. Arh. Hig. Rada Toksikol. 2016, 67, 210–215. [Google Scholar] [CrossRef] [Green Version]
- Hasanein, P.; Felegari, Z. Chelating effects of carnosine in ameliorating nickel-induced nephrotoxicity in rats. Can. J. Physiol. Pharmacol. 2017, 95, 1426–1432. [Google Scholar] [CrossRef]
- Ali, A.A. Evaluation of some biological, biochemical, and hematological aspects in male albino rats after acute exposure to the nano-structured oxides of nickel and cobalt. Environ. Sci. Pollut. Res. Int. 2019, 26, 17407–17417. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 1709) | NAFLD (n = 793) | Non-NAFLD (n = 916) | p3 |
|---|---|---|---|---|
| Prevalence (%) | 46.4 | 100 | 0 | |
| age (y) (median; IQR) 2 | 55 (45, 65) | 53 (43, 64) | 58.5 (47, 66) | <0.001 |
| age (y) n (%) 1 | <0.001 | |||
| 18 ≤ age ≤ 44 | 410 (24.0) | 220 (53.7) | 190 (46.3) | |
| 45 ≤ age ≤ 59 | 573 (33.5) | 284 (49.6) | 289 (50.4) | |
| age ≥ 60 | 726 (42.5) | 289 (39.8) | 437 (60.2) | |
| BMI (kg/m2) n (%) 1 | <0.001 | |||
| BMI < 18.50 | 25 (1.6) | 2 (8.0) | 23 (92.0) | |
| 18.50 ≤ BMI < 24 | 559 (32.6) | 145 (25.9) | 414 (74.1) | |
| BMI ≥ 24 | 1125 (65.8) | 646 (57.4) | 479 (42.6) | |
| SBP, mmHg (median; IQR) 2 | 129.7 (118.3, 143.0) | 131.3 (119.7, 143.0) | 128.0 (117.7, 142.7) | 0.028 |
| DBP, mmHg (median; IQR) 2 | 82.0 (74.7, 89.7) | 82.7 (75.3, 91.0) | 81.0 (73.9, 89.0) | 0.001 |
| ALT, U/L (median; IQR) 2 | 21.0 (15.5, 29.0) | 23.4 (18.0, 33.0) | 19.0 (14.0, 25.0) | <0.001 |
| AST, U/L (median; IQR) 2 | 22.0 (19.0, 25.0) | 22.0 (19.0, 26.0) | 22.0 (19.0, 25.0) | 0.450 |
| ALP, U/L (median; IQR) 2 | 84.0 (71.0, 98.2) | 82.0 (68.0, 96.0) | 85.0 (72.0, 100.0) | 0.001 |
| TBIL, mmol/L (median; IQR) 2 | 16.8 (12.9, 22.2) | 16.89 (13.0, 22.1) | 16.7 (12.8, 22.2) | 0.491 |
| SUA, mmol/L (median; IQR) 2 | 323.0 (274.0, 380.6) | 341.0 (289.0, 400.0) | 310.0 (265.0, 360.0) | <0.001 |
| Serum nickel, µg/L (median; IQR) 2 | 2.5 (2.0, 3.5) | 2.8 (2.1, 4.0) | 2.4 (1.9, 3.2) | <0.001 |
| Total cholesterol, mg/dL (median; IQR) 2 | 5.0 (4.3, 5.6) | 5.1 (4.4, 5.7) | 4.9 (4.2, 5.5) | <0.001 |
| Triglycerides, mg/dL (median; IQR) 2 | 1.4 (1.0, 2.0) | 1.6 (1.1, 2.3) | 1.2 (0.9, 1.7) | <0.001 |
| LDL-C, mg/dL (median; IQR) 2 | 2.9 (2.4, 3.4) | 3.0 (2.4, 3.6) | 2.8 (2.3, 3.3) | <0.001 |
| HDL-C, mg/dL (median; IQR) 2 | 1.2 (1.0, 1.3) | 1.1 (1.0, 1.3) | 1.2 (1.0, 1.4) | <0.001 |
| Fasting glucose, mg/dL (median; IQR) 2 | 5.4 (5.1, 6.0) | 5.6 (5.2, 6.2) | 5.4 (5.0, 5.9) | <0.001 |
| HbA1C, % (median; IQR) 2 | 5.6 (5.2, 5.9) | 5.6 (5.2, 6.1) | 5.5 (5.1, 5.9) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, C.; Liu, W.; Zhang, G.; Wang, Y.; Jiang, J.; Yang, Z.; Wu, W. Conjunctional Relationship between Serum Uric Acid and Serum Nickel with Non-Alcoholic Fatty Liver Disease in Men: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 6424. https://doi.org/10.3390/ijerph19116424
Liu C, Liu W, Zhang G, Wang Y, Jiang J, Yang Z, Wu W. Conjunctional Relationship between Serum Uric Acid and Serum Nickel with Non-Alcoholic Fatty Liver Disease in Men: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(11):6424. https://doi.org/10.3390/ijerph19116424
Chicago/Turabian StyleLiu, Chili, Wannian Liu, Guofu Zhang, Yongbin Wang, Jing Jiang, Zhongzhi Yang, and Weidong Wu. 2022. "Conjunctional Relationship between Serum Uric Acid and Serum Nickel with Non-Alcoholic Fatty Liver Disease in Men: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 11: 6424. https://doi.org/10.3390/ijerph19116424