
Deficiency of Daily Calcium and Vitamin D in Primary School Children in Lviv, Ukraine

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
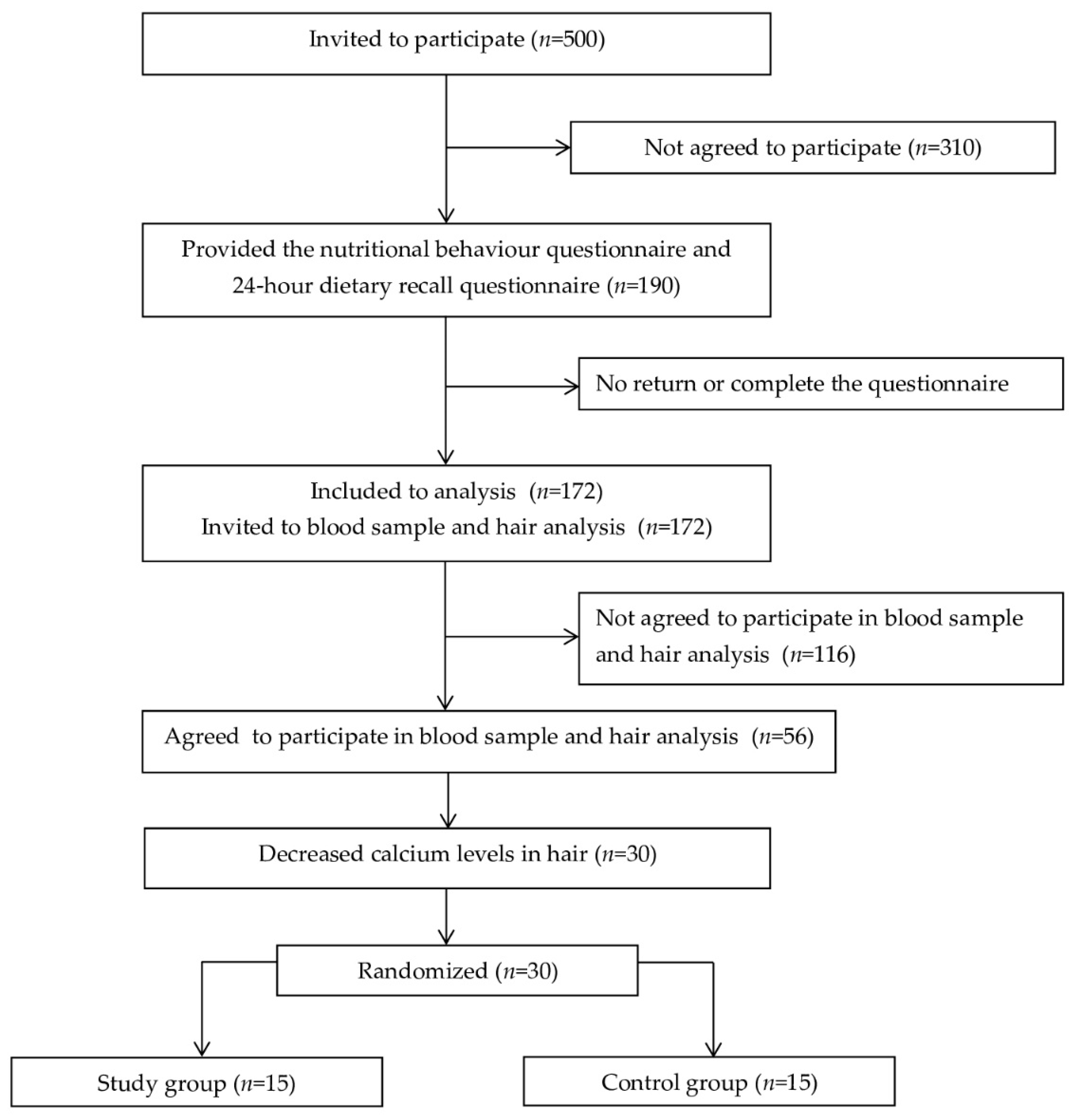
2.1. Participants
2.2. Measurements
2.2.1. Nutritional Behavior
2.2.2. Determination of the Level of Calcium and Vitamin D
2.3. Intervention
2.4. Statistical Analysis
2.5. Ethics
3. Results
4. Discussion
The Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tutelian, V.A.; Baturin, A.K. The influence of nutrition on human health and active longevity: A modern view. In The Future of the Food System in Russia (Assessment of the Expert Community); Lishenko, V.F., Ed.; Economics: Moscow, Russia, 2014; 309p. (In Russian) [Google Scholar]
- Pogozheva, A.V. Healthy eating for the prevention of noncommunicable diseases. Handb. Paramed. Midwife 2014, 2, 8–13. [Google Scholar]
- Available online: https://www.nuzest.com/blog/the-role-of-nutrition-in-childhood-growth-and-development/ (accessed on 12 November 2021).
- Available online: https://www.unicef.org/media/60806/file/SOWC-2019.pdf (accessed on 12 November 2021).
- Stennikova, O.V.; Levchuk, L.V.; Sannikova, N.E. Prevention of deficient conditions in vitamins and minerals in children. Quest. Mod. Pediatr. 2012, 1, 56–60. [Google Scholar]
- Ross, A.C.; Taylor, C.L.; Yaktine, A.L.; Del Valle, H.B. Committee to Review Dietary Reference Intakes for Vitamin D and Calcium; Institute of Medicine (US); National Academy Press: Washington, DC, USA, 2011. [Google Scholar]
- Cerezo de Ríos, S.; Ríos-Castillo, I.; Brito, A.; López de Romaña, D. Nutritional counseling increases consumption of calcium-rich foods, but mean intake remains below the daily requirement. Rev. Chil. Nutr. 2014, 41, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Muños, M.; Salas, J.; Bonanda, A.; Trallero, R. Dietadurante la infancia y la adolescencia. In Nutricion y Dietética Clínica; Elsevier: Amsterdam, The Netherlands, 2008; Volume 8, p. 83. [Google Scholar]
- Ortega-Anta, R.M.; Jiménez-Ortega, A.I.; López-Sobaler, A.M. El calcio y la salud. Nutr. Hosp. 2015, 31, 10–17. [Google Scholar]
- Grupo de Trabajo de la Guía de Práctica Clínica Sobre Osteoporosis y Prevención de Fracturas por Fragilidad. Guía de Práctica Clínica Sobre Osteoporosis y Prevención de Fracturas por Fragilidad. Plan de Calidad Para el Sistema Nacional de Salud del Ministerio de Sanidad, Política Social e Igualdad. Agència d’Informació, Avaluació I Qualitat en Salut (AIAQS) de Cataluña. 2010. Available online: http://aquas.gencat.cat/web/.content/minisite/aquas/publicacions/2010/pdf/gpc_osteoporosis_aiaqs2010_pcsns_vcompl_es.pdf (accessed on 12 November 2021).
- Pettifor, J.M.; Prentice, A. The role of Vitamin D in paediatric bone health. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 573–584. [Google Scholar] [CrossRef]
- Bae, Y.J.; Kratzsch, J. Vitamin D and calcium in the human breast milk. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 39–45. [Google Scholar] [CrossRef]
- Sarma, D.; Saikia, U.K.; Baro, A. Vitamin D Status of School Children in and around Guwahati. Indian J. Endocrinol. Metab. 2019, 23, 81–85. [Google Scholar] [CrossRef]
- Pulungan, A.; Soesanti, F.; Tridjaja, B.; Batubara, J. Vitamin D insufficiency and its contributing factors in primary school-aged children in Indonesia, a sun-rich country. Ann. Pediatr. Endocrinol. Metab. 2021, 26, 92–98. [Google Scholar] [CrossRef]
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.D.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Mäkitie, O.; et al. Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. J. Clin. Endocrinol. Metab. 2016, 101, 394–415. [Google Scholar] [CrossRef]
- Neyestani, T.R.; Hajifaraji, M.; Omidvar, N.; Eshraghian, M.R.; Shariatzadeh, N.; Kalayi, A.; Gharavi, A.; Khalaji, N.; Haidari, H.; Zowghi, T.; et al. High prevalence of vitamin D deficiency in school-age children in Tehran, 2008: A red alert. Public Health Nutr. 2012, 15, 324–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vatanparast, H.; Islam, N.; Patil, R.P.; Shafiee, M.; Whiting, S.J. Calcium intake from food and supplemental sources decreased in the Canadian population from 2004 to 2015. J. Nutr. 2020, 150, 833–841. [Google Scholar] [CrossRef] [PubMed]
- Haddad, L.; Achadi, E.; Bendech, M.A.; Ahuja, A.; Bhatia, K.; Bhutta, Z.; Blössner, M.; Borghi, E.; Colecraft, E.; De Onis, M.; et al. The Global Nutrition Report 2014: Actions and accountability to accelerate the world’s progress on nutrition. J. Nutr. 2015, 145, 663–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kvashnina, L.V. Alimentary calcium deficiency in children and approaches to its correction. Modern Pediatr. 2016, 7, 26–32. [Google Scholar] [CrossRef]
- Cosenza, L.; Pezzella, V.; Nocerino, R.; Di Costanzo, M.; Coruzzo, A.; Passariello, A.; Leone, L.; Savoia, M.; Del Puente, A.; Esposito, A.; et al. Calcium and vitamin D intakes in children: A randomized controlled trial. BMC Pediatr. 2013, 13, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bacchetta, J.; Edouard, T.; Laverny, G.; Bernardor, J.; Bertholet-Thomas, A.; Castanet, M.; Garnier, C.; Gennero, I.; Harambat, J.; Lapillonne, A. Vitamin D and calcium intakes in general pediatric populations: A French expert consensus paper. Arch. Pediatr. 2022, in press. [Google Scholar] [CrossRef]
- Foster, E.; Bradley, J. Methodological considerations and future insights for 24-h dietary recall assessment in children. Nutr. Res. 2018, 51, 1–11. [Google Scholar] [CrossRef]
- Kim, O.Y.; Baek, S.H.; Lee, Y.J.; Lee, K.H. Association of Increased Hair Calcium Levels and Enhanced Augmentation Index (AIx): A Marker of Arterial Stiffness. Biol. Trace Elem. Res. 2010, 138, 90–98. [Google Scholar] [CrossRef]
- Ukrainian Standard—MB 77-02010793:2019; Measurement of the Mass Concentration of Calcium in the Hair by Atomic Absorption Spectrophotometry. Ukrainian Standard: Kyiv, Ukraine, 2019. (In Ukrainian)
- Global Nutrition Report: Shining a Light to Spur Action on Nutrition. 2018. Available online: https://www.who.int/nutrition/globalnutritionreport/2018_Global_Nutrition_Report.pdf?ua=1 (accessed on 12 November 2021).
- Kanter, R.; Vanderlee, L.; Vandevijvere, S. Front-of-package nutrition labelling policy: Global progress and future directions. Public Health Nutr. 2018, 21, 1399–1408. [Google Scholar] [CrossRef] [Green Version]
- Macias, A.I.; Gordillo, L.G.; Camacho, E.J. Eating habits in school-age children and the health education paper. Rev. Chil. Nutr. 2012, 39, 40–43. [Google Scholar]
- World Health Organization. Estrategia Mundial Sobre Régimen Alimentario, Actividad Física y Salud: Sobrepeso y Obesidad Infantil. Available online: http://www.who.int/dietphysicalactivity/childhood/es/ (accessed on 12 November 2021).
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium Food and Nutrition Board. Dietary Reference Intakes for Calcium and Vitamin D; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Bouziani, A.; Saeid, N.; Benkirane, H.; Qandoussi, L.; Taboz, Y.; El Hamdouchi, A.; El Kari, K.; El Mzibri, M.; Aguenaou, H. Dietary Calcium Intake in Sample of School Age Children in City of Rabat, Morocco. J. Nutr. Metab. 2018, 2, 8084623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zitterman, A. Vitamin D in preventive medicine: Are we ignoring the violence? Br. J. Nutr. 2003, 89, 552–572. [Google Scholar] [CrossRef]
- Christakos, S.; DeLuca, H.F. Minireview: Vitamin D: Is there a role in extraskeletal health? Endocrinology 2011, 152, 2930–2936. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D. Pediatrics 2012, 130, e1424. [Google Scholar] [CrossRef] [Green Version]
- Guerrant, R.L.; Lima, A.A.; Davidson, F. Micronutrients and infection: Interactions and implications with enteric and other infections and future priorities. J. Infect. Dis. 2000, 182, 134–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adair, L.S.; Fall, C.H.; Osmond, C.; Stein, A.D.; Martorell, R.; Ramirez-Zea, M.; Sachdev, H.S.; Dahly, D.L.; Bas, I.; Norris, S.A.; et al. Associations of linear growth and relative weight gain during early life with adult health and human capital in countries of low and middle income: Findings from five birth cohort studies. Lancet 2013, 382, 525–534. [Google Scholar] [CrossRef] [Green Version]
- Kvashnina, L.V.; Apukhovska, L.I.; Nikiforova, T.M.; Antonenko, L.V.; Rachkovskaya, V.V. Modern approaches to complex prevention and correction of hypocalcemic conditions in children. Perinatol. Pediatr. 2007, 3, 107. [Google Scholar]
- Golden, N.H.; Abrams, S.A.; Committee on Nutrition. Optimizing bone health in children and adolescents. Pediatrics 2014, 134, 1229–1243. [Google Scholar] [CrossRef] [Green Version]
- Pilz, S.; Trummer, C.; Pandis, M.; Schwetz, V.; Aberer, F.; Gruebler, M.; Verheyen, N.; Tomaschitz, A.; Maerz, W. Vitamin D: Current Guidelines and Future Outlook. Anticancer Res. 2018, 38, 1145–1151. [Google Scholar]
- Rubio-López, N.; Llopis-González, A.; Morales-Suárez-Varela, M. Calcium Intake and Nutritional Adequacy in Spanish Children: The ANIVA Study. Nutrients 2017, 9, 170. [Google Scholar] [CrossRef] [Green Version]
- Fiorentino, M.; Landais, E.; Bastard, G.; Carriquiry, A.; Wieringa, F.T.; Berger, J. Nutrient intake is insufficient among senegalese urban school children and adolescents: Results from two 24 h recalls in state primary schools in Dakar. Nutrients 2016, 8, 650. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhai, R.; Liu, J.; Guang, H.; Li, B.; Zhang, S. Seasonal Variation of Blood Calcium Levels in Children Aged 1-10. J. Clin. Lab. Anal. 2016, 30, 741–744. [Google Scholar] [CrossRef] [PubMed]
- Ozmen, H.; Akarsu, S.; Polat, F.; Cukurovali, A. The levels of calcium and magnesium, and of selected trace elements, in whole blood and scalp hair of children with growth retardation. Iran. J. Pediatr. 2013, 23, 125–130. [Google Scholar] [PubMed]
- Hendrie, G.A.; Brindal, E.; Baird, D.; Gardner, C. Improving children’s dairy food and calcium intake: Can intervention work? A systematic review of the literature. Public Health Nutr. 2013, 16, 365–376. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.T.; Leung, S.S.; Wang, S.H.; Xu, Y.C.; Zeng, W.P.; Lau, J.; Oppenheimer, S.J.; Cheng, J.C. Double-blind, controlled calcium supplementation and bone mineral accretion in children accustomed to a low-calcium diet. Am. J. Clin. Nutr. 1994, 60, 744–750. [Google Scholar] [CrossRef]
- Lee, W.T.; Leung, S.S.; Leung, D.M.; Cheng, J.C. A follow-up study on the effects of calcium supplement withdrawal and puberty on bone acquisition of children. Am. J. Clin. Nutr. 1996, 64, 71–77. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Nutrient | Level of Consumption | Age (Years) | p | ||||
|---|---|---|---|---|---|---|---|
| 7 n (%; CI) | 8 n (%; CI) | 9 n (%; CI) | 10 n (%; CI) | 11 n (%; CI) | |||
| Calcium | Reduced | 29 (76.32%; 62.80–89.83) | 26 (70.27%; 55.54–85.00) | 11 (35.48%; 18.64–52.33) | 27 (61.36%; 46.98–75.75) | 14 (63.64%; 43.54–83.74) | <0.01 |
| Normal | 4 (10.53%; 0.77–20.28) | 5 (13.51%; 2.50–24.53) | 13 (41.94%; 24.56–59.31) | 7 (15.91%; 5.10–26.72) | 0 (0.00%; 0.00–0.00) | ||
| Increased | 5 (13.16%; 2.41–23.91) | 6 (16.22%; 4.34–28.09) | 7 (22.58%; 7.86–37.30) | 10 (22.73%; 10.34–35.11) | 8 (36.36%; 16.26–56.46) | ||
| Indicator | Level | Boys n (%; CI) | Girls n (%; CI) | p |
|---|---|---|---|---|
| Vitamin D intake | Reduced | 62 (84.93%; 76.73–93.14) | 96 (96.97%; 93.59–100.00) | 0.01 |
| Normal | 6 (8.22%; 1.92–14.52) | 1 (1.01%; 0.00–2.98) | ||
| Increased | 5 (6.85%; 1.05–12.64) | 2 (2.02%; 0.00–4.79) | ||
| Total blood calcium | Reduced | 2 (7.69%; 0.00–17.93) | 13 (43.33%; 25.60–61.07) | <0.01 |
| Normal | 23 (88.46%; 76.18–100.00) | 17 (56.67%; 38.93–74.40) | ||
| Increased | 1 (3.85%; 0.00–11.24) | 0 (0.00%; 0.00–0.00) | ||
| Ionized blood calcium | Reduced | 1 (3.85%; 0.00–11.24) | 8 (26.67%; 10.84–42.49) | <0.01 |
| Normal | 14 (53.85%; 34.68–73.01) | 19 (63.33%; 46.09–80.58) | ||
| Increased | 11 (42.31%; 23.32–61.30) | 3 (10.00%; 0.00–20.74) | ||
| Vitamin D in blood | Reduced | 8 (30.77%; 13.03–48.51) | 19 (63.33%; 46.09–80.58) | 0.02 |
| Normal | 18 (69.23%; 51.49–86.97) | 11 (36.67%; 19.42–53.91) | ||
| Calcium in hair | Reduced | 8 (30.80%; 13.03–48.51) | 22 (73.30%; 57.51–89.16) | 0.01 |
| Normal | 17 (65.40%; 47.09–83.67) | 8 (26.70%; 10.84–42.50) | ||
| Increased | 1 (3.80%; 0–11.23) | 0 (0.00%) |
| Group | At the Start | After 3 Months | Difference | p |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| Control | 164.43 ± 80.88 | 185.14 ± 82.38 | 20.71 | 0.07 |
| Study | 181.55 ± 86.95 | 293.60 ± 80.66 | 112.05 | <0.01 |
| Difference | 17.12 | 108.46 | ||
| p | 0.58 | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tytusa, A.; Wyszyńska, J.; Yatsula, M.; Nyankovskyy, S.; Mazur, A.; Dereń, K. Deficiency of Daily Calcium and Vitamin D in Primary School Children in Lviv, Ukraine. Int. J. Environ. Res. Public Health 2022, 19, 5429. https://doi.org/10.3390/ijerph19095429
Tytusa A, Wyszyńska J, Yatsula M, Nyankovskyy S, Mazur A, Dereń K. Deficiency of Daily Calcium and Vitamin D in Primary School Children in Lviv, Ukraine. International Journal of Environmental Research and Public Health. 2022; 19(9):5429. https://doi.org/10.3390/ijerph19095429
Chicago/Turabian StyleTytusa, Andrii, Jutyna Wyszyńska, Marta Yatsula, Serhiy Nyankovskyy, Artur Mazur, and Katarzyna Dereń. 2022. "Deficiency of Daily Calcium and Vitamin D in Primary School Children in Lviv, Ukraine" International Journal of Environmental Research and Public Health 19, no. 9: 5429. https://doi.org/10.3390/ijerph19095429