
The Association between Trajectories of Loneliness and Physical Frailty in Chinese Older Adults: Does Age Matter?


Abstract
:1. Introduction
1.1. The Relationship between Loneliness and Physical Frailty
1.2. Age Role in the Relationship between Loneliness and Physical Frailty
2. Materials and Methods
2.1. Date Source and Participants
2.2. Measures
2.2.1. Trajectory of Loneliness
2.2.2. Trajectory of Physical Frailty
2.2.3. Age and Covariates
2.3. Statistical Analysis
3. Results
3.1. Associations between Baseline Loneliness and PF Transitions as Well as Baseline PF and Loneliness Transitions in Older Adults
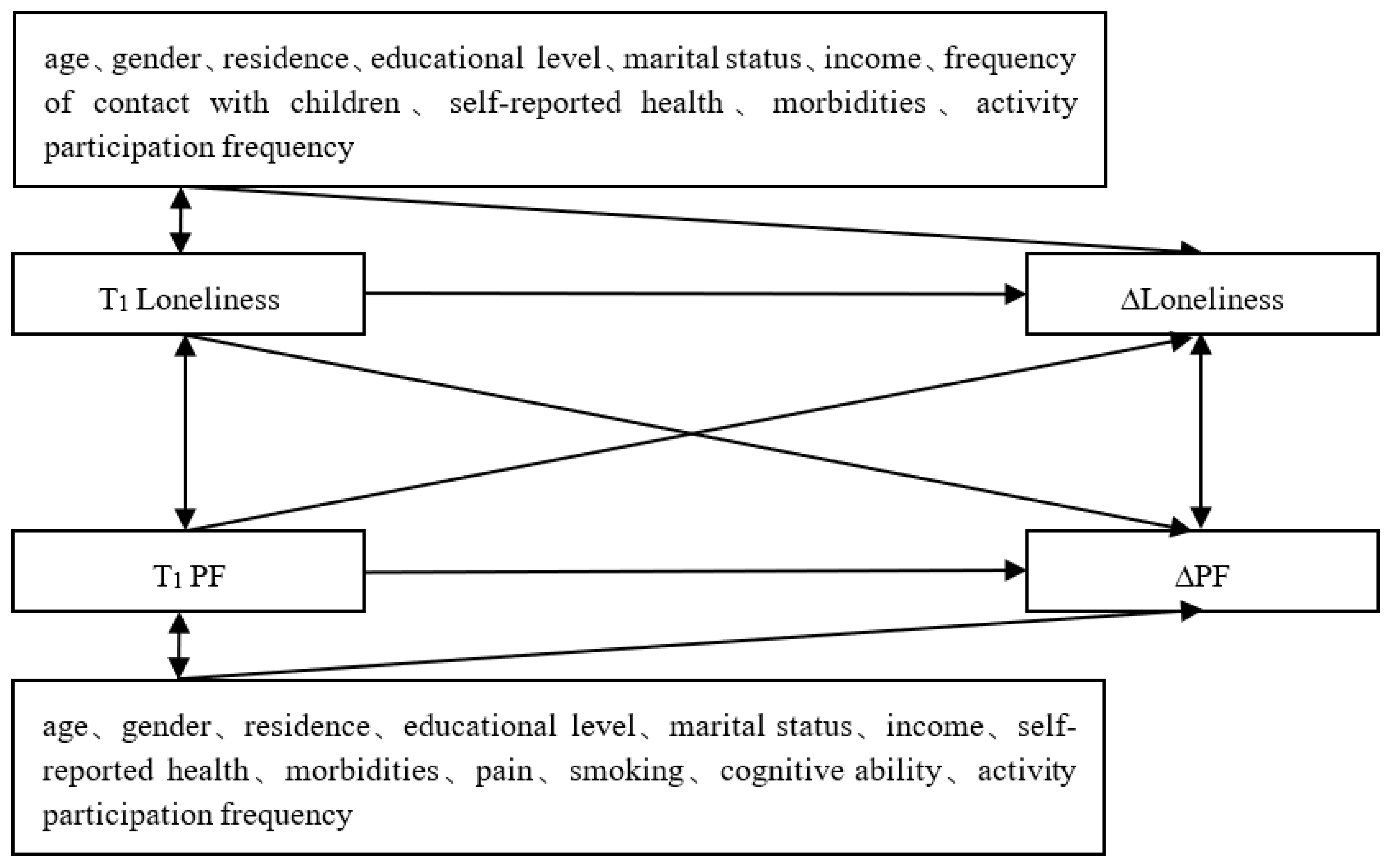
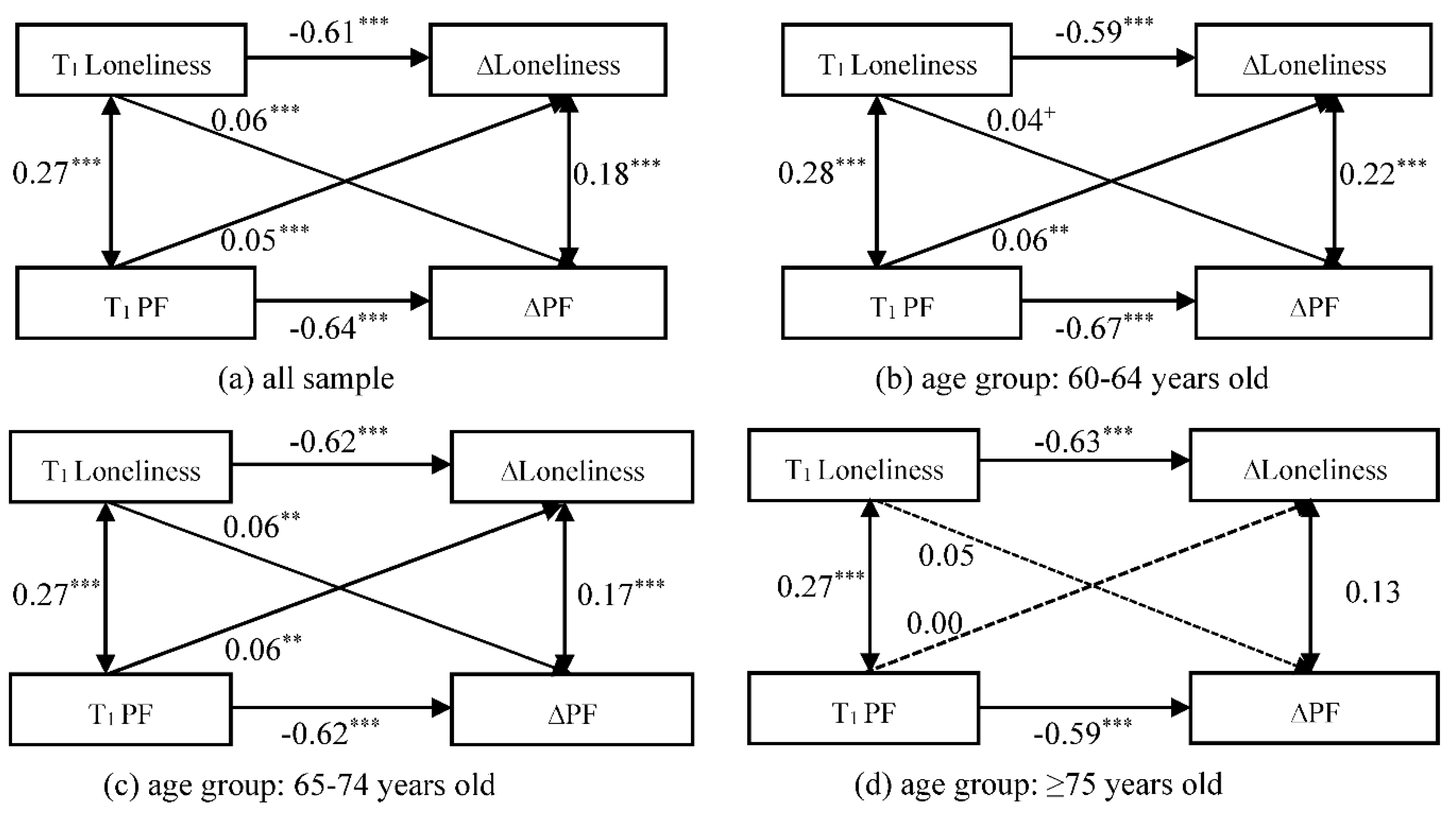
3.2. Stage II: Associations between Loneliness and PF Changes in Older Adults
3.3. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- 2019 Health and Health Development Statistics Bulletin. 2019. Availabe online: http://www.nhc.gov.cn/guihuaxxs/s10748/202006/ebfe31f24cc145b198dd730603ec4442.shtml (accessed on 4 April 2022).
- Guidance on the Establishment of a Comprehensive Health Service System for the Elderly. 2019. Availabe online: http://www.nhc.gov.cn/lljks/s7786/201911/4cbecd7450694416a268a181f9b37e92.shtml (accessed on 4 April 2022).
- Pinquart, M.; Sorensen, S. Influences on loneliness in older adults: A meta-analysis. Basic Appl. Soc. Psychol. 2001, 23, 245–266. [Google Scholar] [CrossRef]
- Seifert, A.; Hassler, B. Impact of the COVID-19 pandemic on older adults mental health services: A mixed methods study. Front. Sociol. 2020, 5, 590935. [Google Scholar] [CrossRef] [PubMed]
- McGinty, E.E.; Presskreischer, R.; Han, H.; Barry, C.L. Psychological distress and loneliness reported by US adults in 2018 and April 2020. JAMA 2020, 324, 93–94. [Google Scholar] [CrossRef]
- Hawkley, L.C.; Kocherginsky, M. Transitions in Loneliness Among Older Adults: A 5-Year Follow-Up in the National Social Life, Health, and Aging Project. Res. Aging 2018, 40, 365–387. [Google Scholar] [CrossRef]
- Luo, Y.; Hawkley, L.C.; Waite, L.J.; Cacioppo, J.T. Loneliness, health, and mortality in old age: A national longitudinal study. Soc. Sci. Med. 2012, 74, 907–914. [Google Scholar] [CrossRef] [Green Version]
- Zhong, B.-L.; Chen, S.-L.; Conwell, Y. Effects of transient versus chronic loneliness on cognitive function in older adults: Findings from the Chinese Longitudinal Healthy Longevity Survey. Am. J. Geriatr. Psychiatry 2016, 24, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Shankar, A.; McMunn, A.; Demakakos, P.; Hamer, M.; Steptoe, A. Social isolation and loneliness: Prospective associations with functional status in older adults. Health Psychol. 2017, 36, 179–187. [Google Scholar] [CrossRef] [Green Version]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Cesari, M.; Prince, M.; Thiyagarajan, J.A.; De Carvalho, I.A.; Bernabei, R.; Chan, P.; Gutierrez-Robledo, L.M.; Michel, J.P.; Morley, J.E.; Ong, P.; et al. Frailty: An Emerging Public Health Priority. J. Am. Med. Dir. Assoc. 2016, 17, 188–192. [Google Scholar] [CrossRef]
- Pranata, R.; Henrina, J.; Lim, M.A.; Lawrensia, S.; Yonas, E.; Vania, R.; Huang, I.; Lukito, A.A.; Suastika, K.; Kuswardhani, R.A.T.; et al. Clinical frailty scale and mortality in COVID-19: A systematic review and dose-response meta-analysis. Arch. Gerontol. Geriatr. 2021, 93, 104324. [Google Scholar] [CrossRef]
- She, Q.; Chen, B.; Liu, W.; Li, M.; Zhao, W.; Wu, J. Frailty pathogenesis, assessment, and management in older adults with COVID-19. Front. Med. 2021, 8, 694367. [Google Scholar] [CrossRef] [PubMed]
- Gill, T.M.; Gahbauer, E.A.; Allore, H.G.; Han, L. Transitions between frailty states among community-living older persons. Arch. Intern. Med. 2006, 166, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G.; Taniguchi, Y.; Iliffe, S.; Jivraj, S.; Walters, K. Transitions between frailty states among community-dwelling older people: A systematic review and meta-analysis. Ageing Res. Rev. 2019, 50, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Pollack, L.R.; Litwack-Harrison, S.; Cawthon, P.M.; Ensrud, K.; Lane, N.E.; Barrett-Connor, E.; Thuy-Tien, D. Patterns and Predictors of Frailty Transitions in Older Men: The Osteoporotic Fractures in Men Study. J. Am. Geriatr. Soc. 2017, 65, 2473–2479. [Google Scholar] [CrossRef]
- Gale, C.R.; Westbury, L.; Cooper, C. Social isolation and loneliness as risk factors for the progression of frailty: The English Longitudinal Study of Ageing. Age Ageing 2018, 47, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Ge, L.; Yap, C.W.; Heng, B.H. Associations of social isolation, social participation, and loneliness with frailty in older adults in Singapore: A panel data analysis. BMC Geriatr. 2022, 22, 26. [Google Scholar] [CrossRef]
- Mhaolain, A.M.N.; Fan, C.W.; Romero-Ortuno, R.; Cogan, L.; Cunningham, C.; Kenny, R.-A.; Lawlor, B. Frailty, depression, and anxiety in later life. Int. Psychogeriatr. 2012, 24, 1265–1274. [Google Scholar] [CrossRef] [Green Version]
- Veld, L.P.M.O.H.; van Rossum, E.; Kempen, G.I.J.M.; de Vet, H.C.W.; Hajema, K.; Beurskens, A.J.H.M. Fried phenotype of frailty: Cross-sectional comparison of three frailty stages on various health domains. BMC Geriatr. 2015, 15, 77. [Google Scholar] [CrossRef] [Green Version]
- Herrera-Badilla, A.; Paticia Navarrete-Reyes, A.; Amieva, H.; Alberto Avila-Funes, J. Loneliness is associated with frailty in community-dwelling elderly adults. J. Am. Geriatr. Soc. 2015, 63, 607–609. [Google Scholar] [CrossRef]
- Hoogendijk, E.O.; Suanet, B.; Dent, E.; Deeg, D.J.H.; Aartsen, M.J. Adverse effects of frailty on social functioning in older adults: Results from the Longitudinal Aging Study Amsterdam. Maturitas 2016, 83, 45–50. [Google Scholar] [CrossRef]
- Sha, S.; Xu, Y.; Chen, L. Loneliness as a risk factor for frailty transition among older Chinese people. BMC Geriatr. 2020, 20, 300. [Google Scholar] [CrossRef] [PubMed]
- Jarach, C.M.; Tettamanti, M.; Nobili, A.; D’Avanzo, B. Social isolation and loneliness as related to progression and reversion of frailty in the Survey of Health Aging Retirement in Europe (SHARE). Age Ageing 2020, 50, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Ozic, S.; Vasiljev, V.; Ivkovic, V.; Bilajac, L.; Rukavina, T. Interventions aimed at loneliness and fall prevention reduce frailty in elderly urban population. Medicine 2020, 99, e19145. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Zhang, J.; Wang, J. Correlates of loneliness in older adults in Shanghai, China: Does age matter? BMC Geriatr. 2018, 18, 300. [Google Scholar] [CrossRef] [Green Version]
- Ji, L.; Qiao, X.; Jin, Y.; Si, H.; Liu, X.; Wang, C. Age differences in the relationship between frailty and depression among community-dwelling older adults. Geriatr. Nurs. 2020, 41, 485–489. [Google Scholar] [CrossRef]
- Mroczek, D.K.; Kolarz, C.M. The effect of age on positive and negative affect: A developmental perspective on happiness. J. Personal. Soc. Psychol. 1998, 75, 1333–1349. [Google Scholar] [CrossRef]
- Brandtstadter, J.; Greve, W. The aging self—stabilizing and protective processes. Dev. Rev. 1994, 14, 52–80. [Google Scholar] [CrossRef]
- Zhao, Y.; Hu, Y.; Smith, J.P.; Strauss, J.; Yang, G. Cohort Profile: The China Health and Retirement Longitudinal Study (CHARLS). Int. J. Epidemiol. 2014, 43, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; Chen, Z.; Zhou, Y.; Shen, L.; Zhang, Z.; Wu, X. Melancholy or mahjong? Diversity, frequency, type, and rural-urban divide of social participation and depression in middle- and old-aged Chinese: A fixed-effects analysis. Soc. Sci. Med. 2019, 238, 112518. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Smith, J.; Strauss, J.; Wang, Y.; Zhao, Y. China Health and Retirement Longitudinal Study (CHARLS). In Encyclopedia of Geropsychology; Pachana, N.A., Ed.; Springer: Singapore, 2017; pp. 463–469. [Google Scholar] [CrossRef]
- Holmen, K.; Ericsson, K.; Andersson, L.; Winblad, B. Loneliness among elderly people living in stockholm: A population study. J. Adv. Nurs. 1992, 17, 43–51. [Google Scholar] [CrossRef]
- Luo, Y. Own health, spousal health and transitions in loneliness among middle-aged and older adults in China. Ageing Soc. 2021, 1–27. [Google Scholar] [CrossRef]
- Dahlberg, L.; Agahi, N.; Lennartsson, C. Lonelier than ever? Loneliness of older people over two decades. Arch. Gerontol. Geriatr. 2018, 75, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Li, Y.-X.; Hu, Y.; Wu, C. Association of Frailty with recovery from disability among community-dwelling Chinese older adults: China health and retirement longitudinal study. BMC Geriatr. 2020, 20, 119. [Google Scholar] [CrossRef] [Green Version]
- Xu, W.; Li, Y.-X.; Wu, C. Incidence of frailty among community-dwelling older adults: A nationally representative profile in China. BMC Geriatr. 2019, 19, 378. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Smit, E.; Xue, Q.L.; Odden, M.C. Prevalence and Correlates of Frailty Among Community-Dwelling Chinese Older Adults: The China Health and Retirement Longitudinal Study. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 73, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Xue, Q.-L.; Odden, M.C.; Chen, X.; Wu, C. Linking early life risk factors to frailty in old age: Evidence from the China Health and Retirement Longitudinal Study. Age Ageing 2020, 49, 208–217. [Google Scholar] [CrossRef]
- Lei, X.; Liu, H. Gender difference in the impact of retirement on cognitive abilities: Evidence from urban China. J. Comp. Econ. 2018, 46, 1425–1446. [Google Scholar] [CrossRef]
- Lei, X.; Hu, Y.; McArdle, J.J.; Smith, J.P.; Zhao, Y. Gender Differences in Cognition among Older Adults in China. J. Hum. Resour. 2012, 47, 951–971. [Google Scholar] [CrossRef] [Green Version]
- Kearney, M.W. Cross-Lagged Panel Analysis. In The SAGE Encyclopedia of Communication Research Methods; Allen, M.R., Ed.; Sage: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Carstensen, L.L.; Isaacowitz, D.M.; Charles, S.T. Taking time seriously—A theory of socioemotional selectivity. Am. Psychol. 1999, 54, 165–181. [Google Scholar] [CrossRef]
- Carstensen, L.L. Evidence for a life-span theory of socioemotional selectivity. Curr. Dir. Psychol. Sci. 1995, 4, 151–156. [Google Scholar] [CrossRef]
- Mather, M. The emotion paradox in the aging brain. In Year in Cognitive Neuroscience; Kingstone, A., Miller, M.B., Eds.; The New York Academy of Sciences: New York, NY, USA, 2012; Volume 1251, pp. 33–49. [Google Scholar]
- Yang, F.; Gu, D.; Mitnitski, A. Frailty and life satisfaction in Shanghai older adults: The roles of age and social vulnerability. Arch. Gerontol. Geriatr. 2016, 67, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Enkvist, A.; Ekstrom, H.; Elmstahl, S. What factors affect life satisfaction (LS) among the oldest-old? Arch. Gerontol. Geriatr. 2012, 54, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Gove, W.R.; Ortega, S.T.; Style, C.B. The maturational and role perspectives on aging and self through the adult years—An empirical-evaluation. Am. J. Sociol. 1989, 94, 1117–1145. [Google Scholar] [CrossRef]
- Mehta, M.; Whyte, E.; Lenze, E.; Hardy, S.; Roumani, Y.; Subashan, P.; Huang, W.; Studenski, S. Depressive symptoms in late life: Associations with apathy, resilience and disability vary between young-old and old-old. Int. J. Geriatr. Psychiatry 2008, 23, 238–243. [Google Scholar] [CrossRef]
- Jin, H.-Y.; Liu, X.; Xue, Q.-L.; Chen, S.; Wu, C. The Association between Frailty and Healthcare Expenditure among Chinese Older Adults. J. Am. Med. Dir. Assoc. 2020, 21, 780–785. [Google Scholar] [CrossRef]
- Shiovitz-Ezra, S.; Ayalon, L. Use of direct versus indirect approaches to measure loneliness in later life. Res. Aging 2012, 34, 572–591. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Model 1: PF Transition Types (OR (95% CI)) | Model 2: Loneliness Transition Types (OR (95% CI)) | ||||||
|---|---|---|---|---|---|---|---|
| Remain Robust | Worsen | Improve | Remain Unhealthy | Maintain | Worsen | Improve | |
| Baseline loneliness | |||||||
| total | 0.55 *** | 1.17 ** | 0.94 | 1.11 * | |||
| [0.49–0.63] | [1.05–1.30] | [0.85–1.04] | [1.02–1.21] | ||||
| 60–64 | 0.50 *** | 1.26 * | 0.93 | 1.14 | |||
| [0.41–0.61] | [1.05–1.52] | [0.79–1.10] | [0.98–1.32] | ||||
| 65–74 | 0.60 *** | 1.21 * | 0.92 | 1.08 | |||
| [0.49–0.72] | [1.03–1.42] | [0.79–1.07] | [0.95–1.24] | ||||
| ≥75 | 0.67 | 0.97 | 0.98 | 1.07 | |||
| [0.44–1.01] | [0.74–1.27] | [0.73–1.32] | [0.86–1.34] | ||||
| Baseline PF | |||||||
| total | |||||||
| prefrail | 0.91 | 1.41 ** | 0.65 * | ||||
| [0.75–1.11] | [1.11–1.78] | [0.47–0.91] | |||||
| frail | 0.76 | 1.56 | 0.83 | ||||
| [0.48–1.18] | [0.90–2.72] | [0.45–1.54] | |||||
| 60–64 | |||||||
| prefrail | 1.01 | 1.25 | 0.59 | ||||
| [0.72–1.41] | [0.84–1.87] | [0.32–1.07] | |||||
| frail | 0.48 | 3.64 * | 0.45 | ||||
| [0.19–1.18] | [1.25–10.56] | [0.08–2.40] | |||||
| 65–74 | |||||||
| prefrail | 0.81 | 1.47 * | 0.78 | ||||
| [0.62–1.08] | [1.05–2.07] | [0.50–1.22] | |||||
| frail | 0.96 | 1.11 | 0.81 | ||||
| [0.49–1.85] | [0.49–2.54] | [0.34–1.89] | |||||
| ≥75 | |||||||
| prefrail | 1.07 | 1.39 | 0.45 | ||||
| [0.64–1.78] | [0.75–2.60] | [0.20–1.01] | |||||
| frail | 0.82 | 0.95 | 1.11 | ||||
| [0.33–2.05] | [0.22–4.19] | [0.32–3.90] | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sha, S.; Chan, S.H.W.; Chen, L.; Xu, Y.; Pan, Y. The Association between Trajectories of Loneliness and Physical Frailty in Chinese Older Adults: Does Age Matter? Int. J. Environ. Res. Public Health 2022, 19, 5105. https://doi.org/10.3390/ijerph19095105
Sha S, Chan SHW, Chen L, Xu Y, Pan Y. The Association between Trajectories of Loneliness and Physical Frailty in Chinese Older Adults: Does Age Matter? International Journal of Environmental Research and Public Health. 2022; 19(9):5105. https://doi.org/10.3390/ijerph19095105
Chicago/Turabian StyleSha, Sha, Sunny H. W. Chan, Lin Chen, Yuebin Xu, and Yao Pan. 2022. "The Association between Trajectories of Loneliness and Physical Frailty in Chinese Older Adults: Does Age Matter?" International Journal of Environmental Research and Public Health 19, no. 9: 5105. https://doi.org/10.3390/ijerph19095105