
Having a Say in Research Directions: The Role of Community Researchers in Participatory Research with Communities of Refugee and Migrant Background
 , , , , ,
, , , , , {kind=link}
Abstract
:1. Introduction
1.1. Research with Women, Families, and Communities of Refugee and Migrant Background
1.2. Inequities during the Perinatal Period
1.3. Thinking Differently about Research Practices
2. Materials and Methods
2.1. Methodology
2.2. Eligibility and Recruitment
2.3. Ethics and Consent
2.4. Data Collection
2.5. Saturation
2.6. Trustworthiness
2.7. Reflexivity
2.8. Data Analysis
2.9. Participant Demographics
3. Results
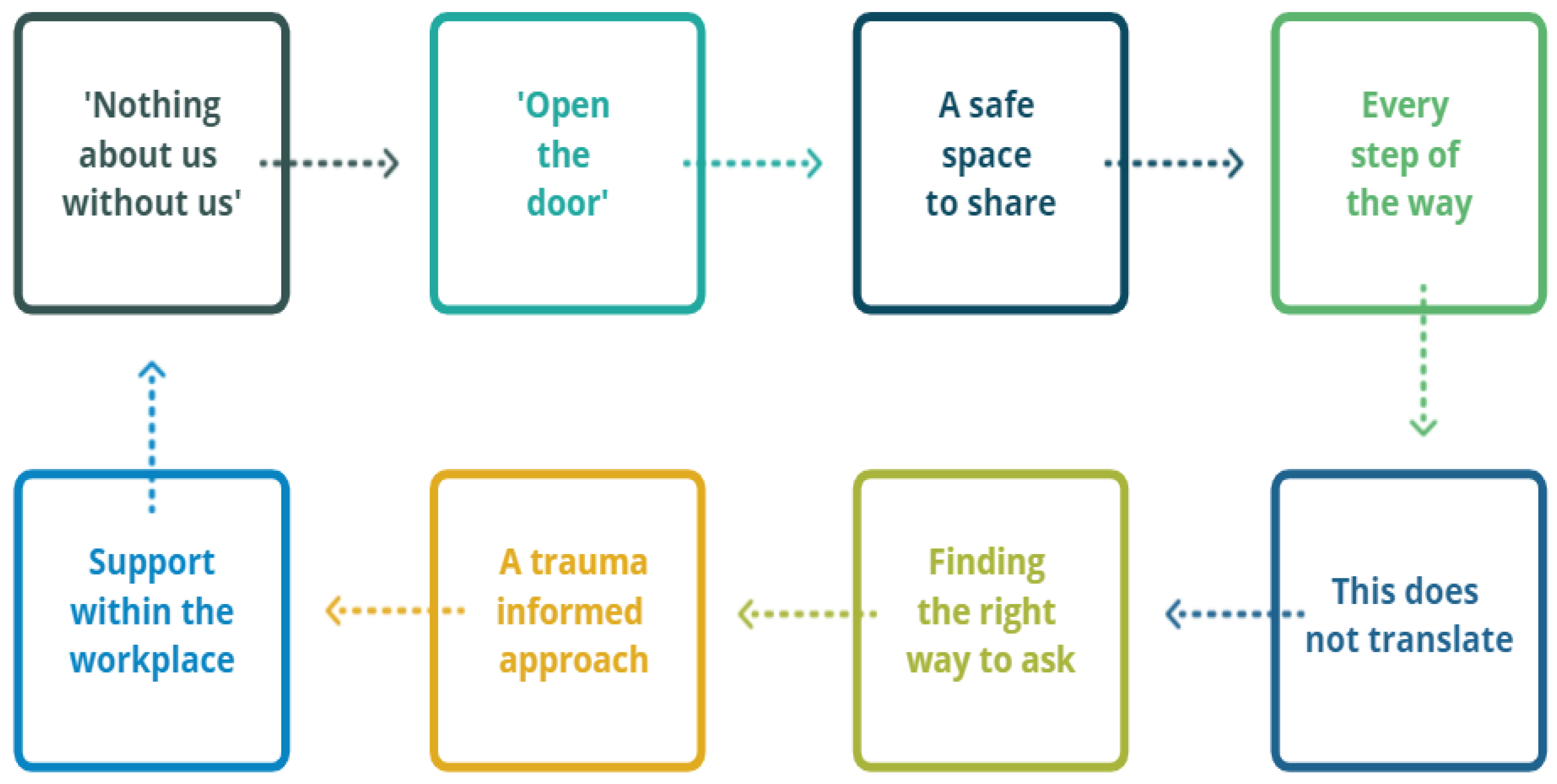
3.1. ‘Nothing about Us without Us’
3.2. ‘Open the Door’
3.3. A Safe Space to Share
3.4. Every Step of the Way
3.5. This Does Not Translate
3.6. Finding the Right Way to Ask
3.7. A Trauma-Informed Approach
3.8. Support within the Workplace
4. Discussion
4.1. Community Researcher Expertise
4.2. Integrating Community Researcher Expertise into Research Processes
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Government, Australian Institute of Health and Welfare. Australia’s Mothers and Babies: Demographics of Mothers and Babies. Australian Government, Australian Institute of Health and Welfare. 2021. Available online: https://www.aihw.gov.au/reports/mothers-babies/australias-mothers-babies/contents/demographics-of-mothers-and-babies (accessed on 21 February 2022).
- Australian Government, Australian Bureau of Statistics. Understanding Migrant Outcomes-Insights from the Australian Census and Migrants Integrated Dataset, Australia: Social and Economic Characteristics of Permanent Migrants Using Census Data for People that Migrated to Australia under Different Entry Conditions: Reference Period–2016. Australian Government, Australian Bureau of Statistics. 2018. Available online: https://www.abs.gov.au/statistics/people/people-and-communities/understanding-migrant-outcomes-insights-australian-census-and-migrants-integrated-dataset-australia/latest-release#data-download (accessed on 21 February 2022).
- Lee, S.K.; Sulaiman-Hill, C.R.; Thompson, S.C. Overcoming language barriers in community-based research with refugee and migrant populations: Options for using bilingual workers. BMC Int. Health Hum. Rights 2014, 14, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kokanovic, R.; Furler, J.; May, C.; Dowrick, C.; Herrman, H.; Evert, H.; Gunn, J. The Politics of Conducting Research on Depression in a Cross-Cultural Context. Qual. Health Res. 2009, 19, 708–717. [Google Scholar] [CrossRef] [PubMed]
- Furness, J.; Nikora, L.W.; Hodgetts, D.; Robertson, N. Beyond Ethics to Morality: Choices and Relationships in Bicultural Research Settings: Ethics in bicultural research. J. Community Appl. Soc. Psychol. 2016, 26, 75–88. [Google Scholar] [CrossRef]
- Woodland, L.; Blignault, I.; O’Callaghan, C.; Harris-Roxas, B. A framework for preferred practices in conducting culturally competent health research in a multicultural society. Health Res. Policy Syst. 2021, 19, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Liamputtong, P. Performing Qualitative Cross-Cultural Research; Cambridge University Press: New York, NY, USA, 2010. [Google Scholar]
- Wild, A.; Kunstler, B.; Goodwin, D.; Onyala, S.; Zhang, L.; Kufi, M.; Salim, W.; Musse, F.; Mohideen, M.; Asthana, M.; et al. Communicating COVID-19 health information to culturally and linguistically diverse communities: Insights from a participatory research collaboration. Public Health Res. Pract. 2021, 30, e3112105. [Google Scholar] [CrossRef]
- Rogers, H.J.; Hogan, L.; Coates, D.; Homer, C.S.E.; Henry, A. Responding to the health needs of women from migrant and refugee backgrounds—Models of maternity and postpartum care in high-income countries: A systematic scoping review. Health Soc. Care Community 2020, 28, 1343–1365. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Promoting the Health of Refugees and Migrants: Frameworks of Priorities and Guiding Principles to Promote the Health of Refugees and Migrants; World Health Organisation: Geneva, Switzerland, 2019; Available online: https://www.who.int/migrants/about/framework_refugees-migrants.pdf (accessed on 11 November 2021).
- Hoang, H.T.; Le, Q.; Kilpatrick, S. Having a baby in the new land: A qualitative exploration of the experiences of Asian migrants in rural Tasmania, Australia. Rural Remote Health 2009, 9, e1084. [Google Scholar] [CrossRef] [Green Version]
- Billett, H.; Vazquez Corona, M.; Bohren, M.A. Women from migrant and refugee backgrounds’ perceptions and experiences of the continuum of maternity care in Australia: A qualitative evidence synthesis. Women Birth, 2021; e1–e13, In Press. [Google Scholar] [CrossRef]
- Porter, M.; Haslam, N. Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons: A meta-analysis. JAMA J. Am. Med. Assoc. 2005, 294, 602–612. [Google Scholar] [CrossRef]
- Kaplan, I. Rebuilding Shattered Lives: Integrated Trauma Recovery for People of Refugee Background, 2nd ed.; The Victorian Foundation for Survivors of Torture Inc. (Foundation House): Melbourne, Australia, 2020. [Google Scholar]
- Wei, K.; Chopra, P.; Strehlow, S.; Stow, M.; Kaplan, I.; Szwarc, J.; Minas, H. The capacity-building role of community liaison workers with refugee communities in Victoria, Australia. Int. J. Ment. Health Syst. 2021, 15, 1–13. [Google Scholar] [CrossRef]
- Riggs, E.; Yelland, J.; Mensah, F.K.; Gold, L.; Szwarc, J.; Kaplan, I.; Small, R.; Middleton, P.; Krastev, A.; McDonald, E.; et al. Group Pregnancy Care for refugee background women: A codesigned, multimethod evaluation protocol applying a community engagement framework and an interrupted time series design. BMJ Open 2021, 11, e048271. [Google Scholar] [CrossRef]
- Riggs, E.; Yelland, J.; Szwarc, J.; Duell-Piening, P.; Wahidi, S.; Fouladi, F.; Casey, S.; Chesters, D.; Brown, S. Afghan families and health professionals’ access to health information during and after pregnancy. Women Birth 2020, 33, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, M.L.; Riley, M.A.; Caffrey, M.P.; Wallbank, G.A.; Milne, C.M.; Harris, M.F.; Lloyd, J. Supporting newly arrived migrant mothers: A pilot health literacy intervention. Health Lit. Res. Pract. 2021, 5, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Yelland, J.; Riggs, E.; Szwarc, J.; Casey, S.; Duell-Piening, P.; Chesters, D.; Wahidi, S.; Fouladi, F.; Brown, S. Compromised communication: A qualitative study exploring Afghan families and health professionals’ experience of interpreting support in Australian maternity care. BMJ Qual. Saf. 2016, 25, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Riggs, E.; Yelland, J.; Szwarc, J.; Casey, S.; Chesters, D.; Duell-Piening, P.; Wahidi, S.; Fouladi, F.; Brown, S. Promoting the inclusion of Afghan women and men in research: Reflections from research and community partners involved in implementing a “proof of concept” project. Int. J. Equity Health 2015, 14, e1–e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gartland, D.; Riggs, E.; Giallo, R.; Glover, K.; Casey, S.; Muyeen, S.; Weetra, D.; White, S.; Koolmatrie, T.; Brown, S.J. Using participatory methods to engage diverse families in research about resilience in middle childhood. J. Health Care Poor Underserved 2021, 32, 1844–1871. [Google Scholar] [CrossRef]
- Yelland, J.; Riggs, E.; Szwarc, J.; Casey, S.; Dawson, W.; Vanpraag, D.; East, C.; Wallace, E.; Teale, G.; Harrison, B.; et al. Bridging the Gap: Using an interrupted time series design to evaluate systems reform addressing refugee maternal and child health inequalities. Implement. Sci. 2015, 10, e62. [Google Scholar] [CrossRef] [Green Version]
- Yelland, J.; Biro, M.A.; Dawson, W.; Riggs, E.; Vanpraag, D.; Wigg, K.; Antonopoulos, J.; Morgans, J.; Szwarc, J.; East, C.; et al. Bridging the language gap: A co-designed quality improvement project to engage professional interpreters for women during labour. Aust. Health Rev. 2017, 41, 499–504. [Google Scholar] [CrossRef]
- Yelland, J.; Mensah, F.; Riggs, E.; McDonald, E.; Szwarc, J.; Dawson, W.; Vanpraag, D.; Casey, S.; East, C.; Biro, M.A.; et al. Evaluation of systems reform in public hospitals, Victoria, Australia, to improve access to antenatal care for women of refugee background: An interrupted time series design. PLoS Med. 2020, 17, e1003089. [Google Scholar] [CrossRef]
- Riggs, E.; Muyeen, S.; Brown, S.; Dawson, W.; Petschel, P.; Tardiff, W.; Norman, F.; Vanpraag, D.; Szwarc, J.; Yelland, J. Cultural safety and belonging for refugee background women attending group pregnancy care: An Australian qualitative study. Birth 2017, 44, 145–152. [Google Scholar] [CrossRef]
- Smith, L.T. Decolonizing Methodologies: Research and Indigenous Peoples, 3rd ed.; Zed Books: London, UK, 2021. [Google Scholar]
- Varcoe, C.; Bottorff, J.L.; Carey, J.; Sullivan, D.; Williams, W. Wisdom and Influence of Elders: Possibilities for Health Promotion and Decreasing Tobacco Exposure in First Nations Communities. Can. J. Public Health 2010, 101, 154–158. [Google Scholar] [CrossRef]
- Thambinathan, V.; Kinsella, E.A. Decolonizing Methodologies in Qualitative Research: Creating spaces for transformative praxis. Int. J. Qual. Methods 2021, 20, e160940692110147. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, e103208. [Google Scholar] [CrossRef] [PubMed]
- Liamputtong, P. Qualitative Research Methods, 5th ed.; Oxford University Press: London, UK, 2020. [Google Scholar]
- Sipes, J.B.A.; Roberts, L.D.; Mullan, B. Voice-only Skype for use in researching sensitive topics: A research note. Qual. Res. Psychol. 2019, 19, e1–e17. [Google Scholar] [CrossRef]
- Vasileiou, K.; Barnett, J.; Thorpe, S.; Young, T. Characterising and justifying sample size sufficiency in interview-based studies: Systematic analysis of qualitative health research over a 15-year period. BMC Med. Res. Methodol. 2018, 18, e1–e18. [Google Scholar] [CrossRef] [Green Version]
- Morse, J.M. Determining Sample Size. Qual. Health Res. 2000, 10, e3–e5. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qual. Res. Sport Exerc. Health 2021, 13, 201–216. [Google Scholar] [CrossRef]
- Lincoln, Y.; Lynham, S.; Guba, E. Paradigmatic controversies, contradictions, and emerging confluences, revisited. In The Sage Handbook of Qualitative Research, 5th ed.; Denzin, N.K., Lincoln, Y., Eds.; Sage: Thousand Oaks, CA, USA, 2018; pp. 108–150. [Google Scholar]
- Lincoln, Y.; Guba, E. Naturalistic Inquiry; Sage: Beverly Hills, CA, USA, 1985. [Google Scholar]
- Wathen, C.N.; Schmitt, B.; MacGregor, J.C.D. Measuring trauma- (and violence-) informed care: A scoping Review. Trauma Violence Abus. 2021; e1–e17, In Press. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Clarke, V.; Braun, V. Thematic analysis. J. Posit. Psychol. 2017, 12, 297–298. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Couns. Psychother. Res. 2021, 21, 37–47. [Google Scholar] [CrossRef]
- Green, J.; Willis, K.; Hughes, E.; Small, R.; Welch, N.; Gibbs, L.; Daly, J. Generating best evidence from qualitative research: The role of data analysis. Aust. N. Z. J. Public Health 2007, 31, 545–550. [Google Scholar] [CrossRef]
- NVivo (Version 12). QSR International Pty Ltd. 2022. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 10 December 2021).
- Braun, V.; Clarke, V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual. Res. Psychol. 2020, 18, 328–352. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qualitative Research in Sport. Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Darder, A. Decolonizing interpretive research: A critical bicultural methodology for social change. Int. Educ. J. 2015, 14, 63–77. [Google Scholar]
- Rugkåsa, J.; Canvin, K. Researching Mental Health in Minority Ethnic Communities: Reflections on Recruitment. Qual. Health Res. 2011, 21, 132–143. [Google Scholar] [CrossRef]
- Prinjha, S.; Miah, N.; Ali, E.; Farmer, A. Including “seldom heard” views in research: Opportunities, challenges and recommendations from focus groups with British South Asian people with type 2 diabetes. BMC Med. Res. Methodol. 2020, 20, 157. [Google Scholar] [CrossRef]
- Caretta, M.A. Situated knowledge in cross-cultural, cross-language research: A collaborative reflexive analysis of researcher, assistant and participant subjectivities. Qual. Res. 2015, 15, 489–505. [Google Scholar] [CrossRef] [Green Version]
- Stapleton, H.M.; Murphy, R.; Kildea, S. Insiders as outsiders: Bicultural research assistants describe their participation in the evaluation of an antenatal clinic for women from refugee backgrounds. Qual. Soc. Work 2015, 14, 275–292. [Google Scholar] [CrossRef]
- Ragavan, M.I.; Cowden, J.D. Bilingual and Bicultural Research Teams: Unpacking the Complexities. Health Equity 2020, 4, 243–246. [Google Scholar] [CrossRef]
- Schinke, R.J.; Peltier, D.; Hanrahan, S.J.; Eys, M.A.; Recollet-Saikonnen, D.; Yungblut, H.; Ritchie, S.; Pickard, P.; Michel, G. The progressive integration of Canadian Indigenous culture within a sport psychology bicultural research team. Int. J. Sport Exerc. Psychol. 2009, 7, 309–322. [Google Scholar] [CrossRef]
- Laird, L.D.; de Marrais, J.; Barnes, L.L. Portraying Islam and Muslims in MEDLINE: A content analysis. Soc. Sci. Med. 2007, 65, 2425–2439. [Google Scholar] [CrossRef]
- Racine, L.; Petrucka, P. Enhancing decolonization and knowledge transfer in nursing research with non-western populations: Examining the congruence between primary healthcare and postcolonial feminist approaches. Nurs. Inq. 2011, 18, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Salma, J.; Ogilvie, L.; Keating, N.; Hunter, K.F. A Bicultural researcher’s reflections on ethical research practices with Muslim immigrant women: Merging boundaries and challenging binaries. Adv. Nurs. Sci. 2017, 40, 109–121. [Google Scholar] [CrossRef] [PubMed]
- O’Rourke, K.; Abdulghani, N.; Yelland, J.; Newton, M.; Shafiei, T. Cross-cultural realist interviews: An integration of the realist interview and cross-cultural qualitative research methods. Eval. J. Australas. 2021, 22, e1035719. [Google Scholar] [CrossRef]
- Ganga, D.; Scott, S. Cultural “insiders” and the issue of positionality in qualitative migration research: Moving “across” and moving “along” researcher-participant divides. Qual. Soc. Res. 2006, 7, e1–e12. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hearn, F.; Biggs, L.; Brown, S.; Tran, L.; Shwe, S.; Noe, T.M.P.; Toke, S.; Alqas Alias, M.; Essa, M.; Hydari, S.; et al. Having a Say in Research Directions: The Role of Community Researchers in Participatory Research with Communities of Refugee and Migrant Background. Int. J. Environ. Res. Public Health 2022, 19, 4844. https://doi.org/10.3390/ijerph19084844
Hearn F, Biggs L, Brown S, Tran L, Shwe S, Noe TMP, Toke S, Alqas Alias M, Essa M, Hydari S, et al. Having a Say in Research Directions: The Role of Community Researchers in Participatory Research with Communities of Refugee and Migrant Background. International Journal of Environmental Research and Public Health. 2022; 19(8):4844. https://doi.org/10.3390/ijerph19084844
Chicago/Turabian StyleHearn, Fran, Laura Biggs, Stephanie Brown, Lien Tran, Sherinald Shwe, Ta Mwe Paw Noe, Shadow Toke, May Alqas Alias, Maryaan Essa, Shogoufa Hydari, and et al. 2022. "Having a Say in Research Directions: The Role of Community Researchers in Participatory Research with Communities of Refugee and Migrant Background" International Journal of Environmental Research and Public Health 19, no. 8: 4844. https://doi.org/10.3390/ijerph19084844