
Enteric Pathogens Risk Factors Associated with Household Drinking Water: A Case Study in Ugu District Kwa-Zulu Natal Province, South Africa


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Clearance Approval
2.2. Study Area and Sample Collection
2.3. Assessment of the Household Drinking Water Quality
2.3.1. Assessment of Sanitary Quality of Drinking Water in the Target Areas
2.3.2. Detection of the Presence of Presumptive Pathogenic Bacteria
2.3.3. Molecular Identification of Bacteria E. coli, Salmonella typhimurium, Shigella dysenteriae, and Vibrio cholerae
2.4. Recovery and Molecular Detection of Rotaviruses
2.5. Quantitative Microbial Risk Assessment (QMRA)
3. Results
3.1. Assessment of Sanitary Quality of Drinking Water in the Study Areas
3.2. Prevalence of Target Potential Pathogenic Bacteria Based on Culture Methods
3.3. Prevalence of the Target Bacterial Species According to Molecular Characteristics and Identification
3.4. Detection and Characterisation of Rotavirus from the Treated Drinking Water
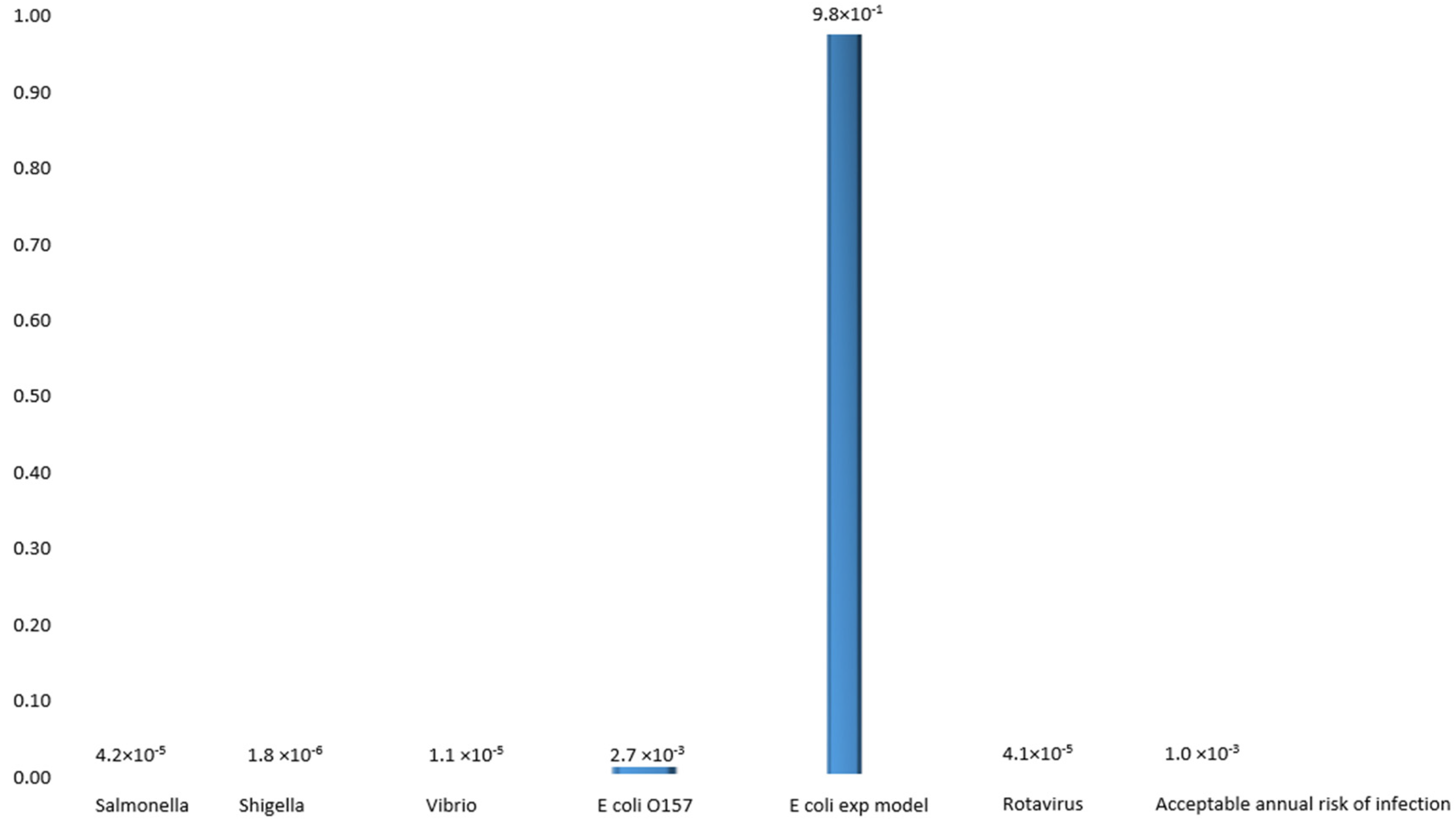
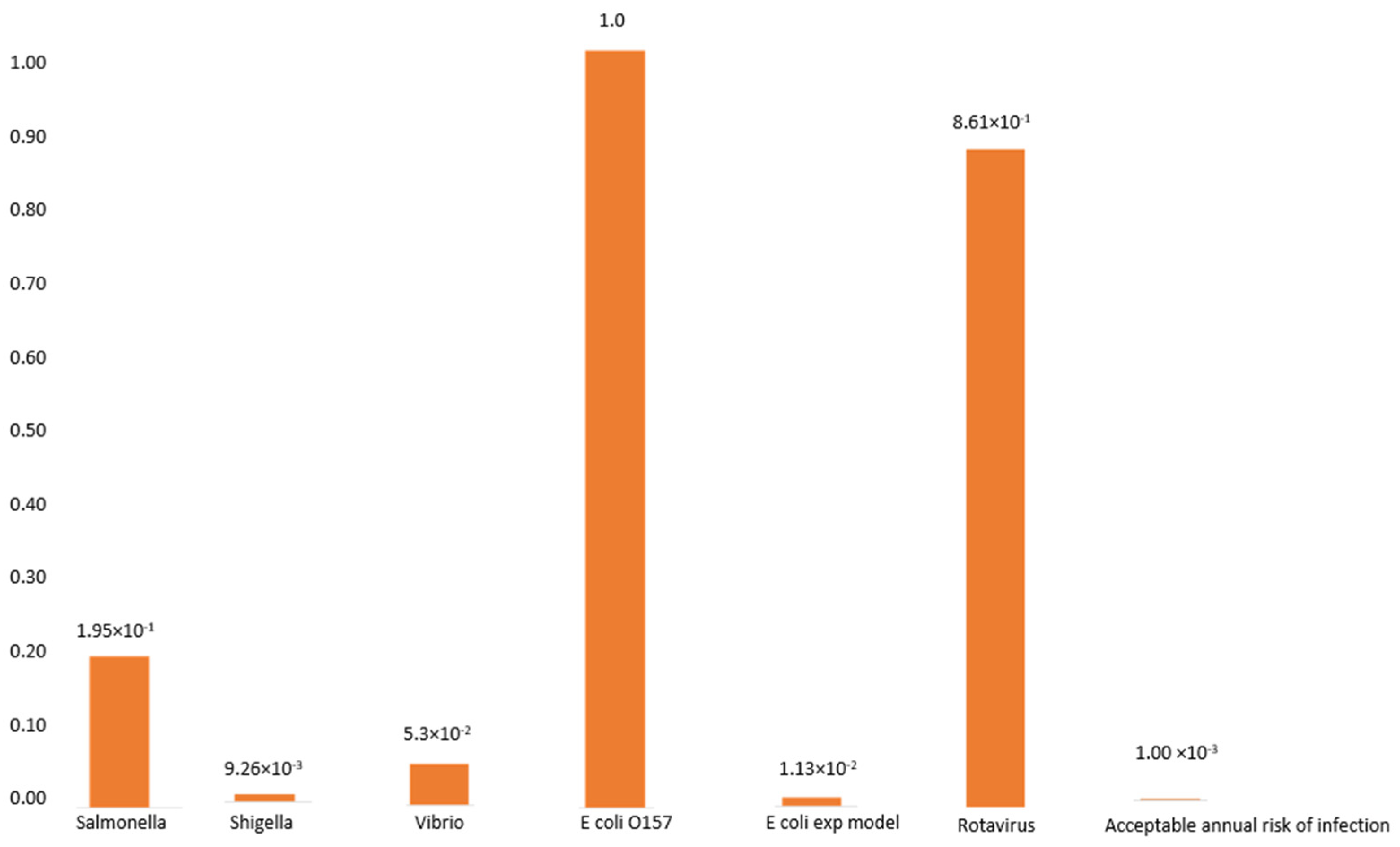
3.5. The Probability of Infection with S. typhimurium, S. dysenteriae, V. cholerae, E. coli, and Rotavirus
3.6. The Probability of Infection with Diarrheagenic E. coli
The Probability of Infection with Rotavirus in Water
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Gerba, C.P.; Rose, J.B.; Haas, C.N.; Crabtree, K.D. Waterborne rotavirus: A risk assessment. Water Res. 1996, 30, 2929–2940. [Google Scholar] [CrossRef]
- Johnson, J.R. American Society for Microbiology Virulence Factors in Escherichia coli Urinary Tract Infection. Clin. Microbiolol. Rev. 1991, 4, 80–128. [Google Scholar] [CrossRef]
- Dorner, S.M.; Anderson, W.B.; Gaulin, T.; Candon, H.L.; Slawson, R.M.; Payment, P.; Huck, P.M. Pathogen and indicator variability in a heavily impacted watershed. J. Water Health 2007, 5, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Barman, M.; Unold, D.; Shifley, K.; Amir, E.; Hung, K.; Bos, N.; Salzman, N. Enteric Salmonellosis Disrupts the Microbial Ecology of the Murine Gastrointestinal Tract. Infect. Immun. 2008, 76, 907–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nkwonta, O.I.; Ochieng, G.M. Water pollution in Soshanguve environs of South Africa. World Acad. Sci. Eng. Technol. 2009, 32, 499–503. [Google Scholar]
- Jamwal, P.; Mittal, A.K.; Mouchel, J.M. Point and non-point microbial source pollution: A case study of Delhi. Phys. Chem. Earth 2011, 36, 490–499. [Google Scholar] [CrossRef]
- Wilson, D.J. Insights from genomics into bacterial pathogen populations. PLoS Pathog. 2012, 8, e1002874. [Google Scholar] [CrossRef]
- Ashbolt, N.J. Microbial contamination of drinking water and disease outcomes in developing regions. Toxicology 2004, 198, 229–238. [Google Scholar] [CrossRef]
- Ternhag, A.; Törner, A.; Svensson, Å.; Ekdahl, K.; Giesecke, J. Short- and Long-term Effects of Bacterial Gastrointestinal Infections Emerging Infectious Diseases. Emerg. Infect. Dis. 2008, 14, 143. [Google Scholar] [CrossRef]
- Muoki, M.A.; Tumuti, D.S.; Rombo, G.O. Nutrition and public hygiene among children under five years of age in Mukuru slums of Makadara Division, Nairobi. East Afr. Med. J. 2018, 85, 386–397. [Google Scholar] [CrossRef] [Green Version]
- Alirol, E.; Getaz, L.; Stoll, B.; Chappuis, F.; Loutan, L. Urbanisation and infectious diseases in a globalized world. Lancet Infect. Dis. 2010, 10, 131–141. [Google Scholar]
- Murray, L.; Ian, B.; Wilkinson, A.B.; Wallin, E. Oxford Hanford of Clinical Medicine, 9th ed.; Oxford University Press: Sussex, UK, 2014; pp. 408–415. [Google Scholar]
- Ponnuvel, K.M.; Rajkumar, R.; Menon, T.; Sankaranarayanan, V.S. Role of Candida in indirect pathogenesis of antibiotic-associated diarrhea in infants. Mycopathologia 1996, 135, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, M.P.; Wein, L.M. Quantifying the routes of transmission for pandemic influenza. Bull. Math. Biol. 2008, 70, 820–867. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Principles and Guidelines for the Conduct of Microbiological Risk Assessment; CAC/GL-30; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Sewell, D.L. Laboratory-associated infections and biosafety. Clin. Microbiol. Rev. 1995, 8, 389–405. [Google Scholar] [CrossRef]
- Schmid-Hempel, P.; Frank, S.A. Pathogenesis, virulence, and infective dose. PLoS Pathog. 2007, 3, 1372–1373. [Google Scholar] [CrossRef] [Green Version]
- Pujol, J.M.; Eisenberg, J.E.; Haas, C.N.; Koopman, J.S. The effect of ongoing exposure dynamics in dose-response relationships. PLoS Comput. Biol. 2009, 5, e1000399. [Google Scholar] [CrossRef] [Green Version]
- Hutzler, A.J.; Boyle, W.C. Risk assessment in water reuse. In Water Reuse; Middlebrooks, E.J., Ed.; Ann Arbour Science Publishers Inc.; The Butterworth Group: Ann Arbor, MI, USA, 1982; pp. 293–324. [Google Scholar]
- Haas, C.N.; Rose, J.B.; Gerba, C.P. Quantitative Microbial Risk Assessment; John Wiley and Sons Inc.: Ontario, CA, USA; New York, NY, USA, 1999. [Google Scholar]
- Haas, C.H.; Thayyar-Madabusi, A.; Rose, J.B.; Gerba, C.P. Development of a dose-response relationship for Escherichia coli O157: H7. Int. J. Food Microbiol. 2000, 1748, 153–159. [Google Scholar] [CrossRef]
- Nauta, M.J.; Evers, E.G.; Takumi, K.; Havelaar, A.H. Risk Assessment of Shiga Toxin Producing Escherichia coli O157 in Steak Tartare in The Netherlands. RIVM Rapport 257851003. 2001. Available online: http://www.rivm.nl/ (accessed on 19 May 2010).
- Dowd, S.E.; Gerba, C.P.; Pepper, I.L.; Pillai, S.D. Bioaerosol transport modeling and risk assessment in relation to biosolid placement. J. Environ. Qual. 2000, 29, 343–348. [Google Scholar] [CrossRef]
- Ferguson, C.; de Roda Husman, A.M.; Altavilla, N.; Deere, D.; Ashbolt, N. Fate and Transport of Surface Water Pathogens in Watersheds. Crit. Rev. Environ. Sci. Technol. 2003, 33, 299–361. [Google Scholar] [CrossRef]
- Pedley, S.; Yates, M.; Schijven, J.F.; West, J.; Howard, G.; Barrett, M. Pathogens: Health relevance, transport, and attenuation. In Protecting Groundwater for Health: Managing the Quality of Drinking-Water Sources; Schmoll, O., Howard, G., Chilton, J., Chorus, I., Eds.; IWA Publishing: London, UK, 2006; pp. 49–79. [Google Scholar]
- Ashöon, P.; Ramasha, V. Water and HIV/AIDS: Some strategic considerations in Southern Africa. In Hydropolitics in the Developing World: A Southern African Perspective; Turton, A.R., Henwood, R., Eds.; African Water Issues Research Unit: Pretoria, South Africa, 2002; pp. 217–235. [Google Scholar]
- Muniesa, M.; Simon, M.; Prats, G.; Ferrer, D.; Panella, H.; Jofre, J. Shiga toxin 2-converting bacteriophages associated with clonal variability in Escherichia coli O157: H7 strains of human origin isolated from a single outbreak. Infect. Immun. 2003, 71, 4554–4562. [Google Scholar] [CrossRef] [Green Version]
- Mead, P.; Slutsker, L.; Dietz, V.; McCaig, L.; Bresee, J.; Shapiro, C.; Griffin, P.; Tauxe, R. Food-related illness and death in the United States. Emerg. Infect. Dis. 1999, 5, 607–625. [Google Scholar] [CrossRef] [PubMed]
- Scallan, E.; Hoekstra, R.; Angulo, F.; Tauxe, R.; Widdowson, M.; Roy, S.; Jones, J.; Griffin, P. Foodborne illness acquired in the United States-major pathogens. Emerg. Infect. Dis. 2011, 17, 7–15. [Google Scholar] [CrossRef]
- Crum-Cianflone, N.F. Salmonellosis and the GI Tract: More than Just Peanut Butter. Curr. Gastroenterol. Rep. 2008, 10, 424–431. [Google Scholar] [CrossRef]
- Shigellosis (PDF). State of the Art of New Vaccine Research and Development. Immunization, Vaccines and Biologicals; World Health Organization: Geneva, Switzerland, 2006; pp. 10–12. [Google Scholar]
- Khalil, I.A.; Troeger, C.; Blacker, B.F.; Rao, P.C.; Brown, A.; Atherly, D.E.; Brewer, T.G.; Engmann, C.M.; Houpt, E.R.; Kang, G.; et al. Morbidity and mortality due to shigella and enterotoxigenic Escherichia coli diarrhoea: The Global Burden of Disease Study 1990–2016. Lancet Infect. Dis. 2018, 18, 1229–1240. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.T.; Lee, C.N.; Shao, P.L.; Chang, L.Y.; Lu, C.Y.; Lee, P.I. Clinical characteristics of nosocomial rotavirus infection in children in Taiwan. J. Formos. Med. Assoc 2008, 107, 791.e7. [Google Scholar] [CrossRef] [Green Version]
- American Public Health Association (APHA). Standard Methods for the Examination of Water and Wastewater, 21st ed.; American Public Health Association; American Water Works Association; Water Environment Federation: Washington, DC, USA, 2005. [Google Scholar]
- Tsai, Y.-L.; Sobsey, M.D.; Sangermano, L.R.; Palmer, C.J. Simple Method of Concentrating Enteroviruses and Hepatitis A Virus from Sewage and Ocean Water for Rapid Detection by Reverse Transcriptase-Polymerase Chain Reaction. Appl. Environ. Microbiol. 1993, 59, 3488–3491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, R.Y.C.; Lee, S.K.Y.; Law, T.W.F.; Law, S.H.W.; Wu, R.S.S. Rapid detection of six types of bacterial pathogens in marine waters by multiplex PCR. Water Res. 2002, 36, 2802–2812. [Google Scholar] [CrossRef]
- Thiem, V.D.; Sethabutr, O.; Seidlein, L.V.; Tung, T.V.; Canh, D.G.; Chien, B.T.; Tho, L.H.; Lee, H.; Houng, H.S.; Hale, T.L.; et al. Detection of Shigella by PCR assay targeting the ipaH gene suggests an increased prevalence of shigellosis in Nha Trang, Vietnam. J. Clin. Microbiol. 2004, 42, 2031–2035. [Google Scholar] [CrossRef] [Green Version]
- Page, N.; Mapuroma, F.; Seheri, M.; Kruger, T.; Peenze, I.; Walaza, S.; Cohen, C.; Groome, M.; Madhi, S. Rotavirus surveillance report, South Africa, 2013. Commun. Dis. Surveill. Bull. 2014, 12, 130–135. [Google Scholar]
- World Health Organization (WHO). Water Quality: Guidelines, Standards, and Health. Assessment of Risk and Risk Management for Water-Related Infectious Diseases; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Abongo, B.O.; Momba, M.N.B.; Rodda, N. Health risk of Escherichia coli 0157: H7 in drinking water and meat and meat products and vegetables to diarrhoeic confirmed and non-confirmed HIV/AIDS patients. J. Appl. Sci. 2008, 8, 1455–1461. [Google Scholar]
- Muhammad, S.; Shah, M.T.; Khan, S. Health risk assessment of heavy metals and their source apportionment in drinking water of Kohistan region, northern Pakistan. Microchem. J. 2011, 98, 334–343. [Google Scholar] [CrossRef]
- Grabow, W.O.K. Waterborne diseases: Update on water quality assessment and control. Water SA 1996, 22, 193–202. [Google Scholar]
- Verma, B.L.; Srivastava, R.N. Measurement of the personal cost of illness due to some major water-related diseases in an Indian rural population. Int. J. Epidemiol. 1990, 19, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okeke, I.N.; Ojo, O.; Lamikanra, A.; Kaper, J.B. Etiology of acute diarrhea in adults in Southwestern Nigeria. J. Clin. Microbiol. 2003, 41, 4525–4530. [Google Scholar] [CrossRef] [Green Version]
- CDC. Centers for Disease Control and Prevention: N.p Web 23 Feb. Pink Book’s Chapter on Rotavirus. 2013. Available online: http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/rota.pdf (accessed on 4 June 2009).
- Hayes, C.; Elliot, E.; Krales, E.; Goulda, D. Food and water safety for persons infected with human immunodeficiency virus. Clin. Infect. Dis. 2003, 36, S106–S109. [Google Scholar] [CrossRef]
- Edwards, B.H. Salmonella and Shigella species. Clin. Lab. Med. 1999, 19, 469–487. [Google Scholar] [CrossRef]
- Parashar, U.D.; Hummelman, E.G.; Bresee, J.S.; Miller, M.A.; Glass, R.I. Global Illness and Deaths Caused by Rotavirus Disease in Children. Emerg. Infect. Dis. 2003, 9, 565. [Google Scholar] [CrossRef]
- Steele, A.D.; Glass, R. Rotavirus in South Africa: From discovery to vaccine introduction. S. Afr. J. Epidemiol. Infect. 2011, 26, 184–190. [Google Scholar] [CrossRef]
- Hot, D.; Legeay, O.; Jacgues, J.; Gantzer, C.; Caudrelier, Y.; Guyard, K.; Lange, M.; Andréoletti, L. Detection of somatic phages, infectious enteroviruses and enterovirus genomes as indicators of human enteric viral pollution in surface water. Water Res. 2003, 37, 4703–4710. [Google Scholar] [CrossRef]
- Greening, G.E. Human and animal viruses in food (including a taxonomy of enteric viruses). In Viruses in Food; Goyal, S.M., Ed.; Springer Science and Business Media: New York, NY, USA, 2006; pp. 5–42. [Google Scholar]
- Denis-Mize, K.; Fout, G.S.; Dahling, D.R.; Francy, D.S. Detection of human enteric viruses in stream water with RT-PCR and cell culture. J. Water Health 2004, 2, 37–47. [Google Scholar] [CrossRef]
- Miagostovich, P.M.; Ferreira, F.F.M.; Guimarães, F.R.; Fumian, T.M.; Diniz-Mendes, L.; Luz, S.L.B.; Silva, L.A.; Leite, J.P.G. Molecular detection and characterization of gastroenteritis viruses occurring naturally in stream waters of Manaus, Central Amazônia, Brazil. Appl. Environ. Microbiol. 2008, 74, 375–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Pathogens | Gene Targeted | Sequences | Amplicon Size | Ref. |
|---|---|---|---|---|
| E. coli | uidA | F-AAAACGGCAAGAAAAAGCAG- R-ACGCGTGGTTAACAGTCTTGCG- | 147 | [35] |
| PCR Steps | Temperature (°C) | Duration | Number of cycles | |
| Initial denaturation | 94 | 2 min | 35 | |
| Denaturation | 94 | 1 min | ||
| Annealing | 58 | 1 min | ||
| Extension | 72 | 1 min | ||
| Final extension | 72 | 5 min | ||
| Salmonella | IpaB | F-GGACTTTTTAAAAGCGGCGG- R-GCCTCTCCCAGAGCCGTCTGG | 314 | [36] |
| PCR Steps | Temperature (°C) | Duration | Number of cycles | |
| Initial denaturation | 94 | 2 min | 25 | |
| Denaturation | 94 | 1 min | ||
| Annealing | 62 | 1 min | ||
| Extension | 72 | 2 min and 5 s | ||
| Final extension | 72 | 7 min | ||
| Shigella | IpaH-U1 IpaH-L1 | -CCTTTTCCGCGTTCCTTGA- -CGGAATCCGGAGGTATTG C- | 199 | [37] |
| PCR Steps | Temperature (°C) | Duration | Number of cycles | |
| Initial denaturation | 95 | 5 min | 40 | |
| Denaturation | 95 | 30 s | ||
| Annealing | 60 | 1 min | ||
| Extension | 72 | 1 min | ||
| Final extension | 72 | 7 min | ||
| Vibrio | EpsM | F-GAATTATTGGCTCCTGTGCAGG- R-ATCGCTTGGCGCATCACTGCCC- | 248 | [36] |
| PCR Steps | Temperature (°C) | Duration | Number of cycles | |
| Initial denaturation | 94 | 2 min | 35 | |
| Denaturation | 94 | 1 min | ||
| Annealing | 58 | 1 min | ||
| Extension | 72 | 2 min and 5 s | ||
| Final extension | 72 | 4 min |
| Study Area | Faecal Coliforms CFU/100 mL | Total Coliforms CFU/100 mL | |
|---|---|---|---|
| Rural | Boboyi | Min < 2 Max > 97 | Min < 11 Max > 347 |
| Bomela | Min < 2 Max > 88 | Min < 17 Max < 220 | |
| Gamalakhe | Min < 0 Max > 64 | Min < 10 Max < 219 | |
| Urban | Anneline | Min < 1 Max > 12 | Min < 5 Max < 104 |
| Hibberdene | Min < 1 Max > 66 | Min < 1 Max > 161 | |
| Margate | Min < 0 Max > 2 | Min < 1 Max > 214 | |
| Portshepstone | Min < 0 Max > 3 | Min < 0 Max >199 | |
| Species | Study Sites | ||||||
|---|---|---|---|---|---|---|---|
| Boboyi | Bomela | Gamalakhe | Margate | Hibberdene | Anneline | P/Shepstone | |
| Bacillus spp. | 7 (7.7%) | 3 (3.3%) | 0(0%) | 0(0%) | 0(0%) | 1 (1.02%) | 0 (0%) |
| Citrobacter spp. | 9 (9.9%) | 12 (13.2%) | 20 (22.0%) | 16 (17.6%) | 12 (13.2%) | 24 (26.4%) | 24 (26.4%) |
| Enterobacter spp. | 12 (13.2%) | 2 (2.2%) | 16 (17.6%) | 12 (13.2%) | 32 (35.2%) | 16 (17.6%) | 8 (8.8%) |
| E. coli | 25 (27.5%) | 38 (41.8%) | 34 (37.4%) | 16 (17.6%) | 18 (19.8%) | 12 (13.2%) | 24 (26.4%) |
| Klebsiella spp. | 4 (4.3%) | 12 (13.2%) | 0 (0%) | 0 (0%) | 2 (2.2%) | 0 (0%) | 0 (0%) |
| Salmonella spp. | 8 (8.8%) | 2 (2.2%) | 6 (6.6%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Shigella boydii | 12 (13.2%) | 9 (9.9%) | 4 (4.4%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Pseudomonas spp. | 10 (11.0%) | 13 (14.3%) | 11 (12.1%) | 8 (8.8%) | 12 (13.2%) | 12 (13.2%) | 16 (17.6%) |
| Proteus mirabilis | 4 (4.4%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Total n = 638 | 91/91 (100%) | 91/91 (100%) | 91/91 (100%) | 52/91 (57%) | 76/91 (84%) | 65/91 (71%) | 72/91 (79%) |
| Bacterium | Sampling Points | ||||||
|---|---|---|---|---|---|---|---|
| Rural (n = 20 Per Site) | Urban (n = 20 Per Site) | ||||||
| Boboyi | Bomela | Gamalakhe | Anneline | Hibberdene | Margate | P/Shepston | |
| E. coli | 12 (60%) | 9 (45%) | 6 (30%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Salmonella typhimurium | 13 (65%) | 8 (40%) | 8 (40%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Shigella dysenteriae | 6 (30%) | 8 (40%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Vibrio cholerae | 8 (40%) | 8 (40%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Source | Type of Sample | Genotype |
|---|---|---|
| Tap water (Anneline) | Final treated water sample | G1P (8) |
| Tap water (P/Shepstone) | Final treated water sample | G1P (6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khabo-Mmekoa, C.M.; Genthe, B.; Momba, M.N.B. Enteric Pathogens Risk Factors Associated with Household Drinking Water: A Case Study in Ugu District Kwa-Zulu Natal Province, South Africa. Int. J. Environ. Res. Public Health 2022, 19, 4431. https://doi.org/10.3390/ijerph19084431
Khabo-Mmekoa CM, Genthe B, Momba MNB. Enteric Pathogens Risk Factors Associated with Household Drinking Water: A Case Study in Ugu District Kwa-Zulu Natal Province, South Africa. International Journal of Environmental Research and Public Health. 2022; 19(8):4431. https://doi.org/10.3390/ijerph19084431
Chicago/Turabian StyleKhabo-Mmekoa, Colette Mmapenya, Bettina Genthe, and Maggy Ndombo Benteke Momba. 2022. "Enteric Pathogens Risk Factors Associated with Household Drinking Water: A Case Study in Ugu District Kwa-Zulu Natal Province, South Africa" International Journal of Environmental Research and Public Health 19, no. 8: 4431. https://doi.org/10.3390/ijerph19084431