
Prediction Model including Gastrocnemius Thickness for the Skeletal Muscle Mass Index in Japanese Older Adults

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
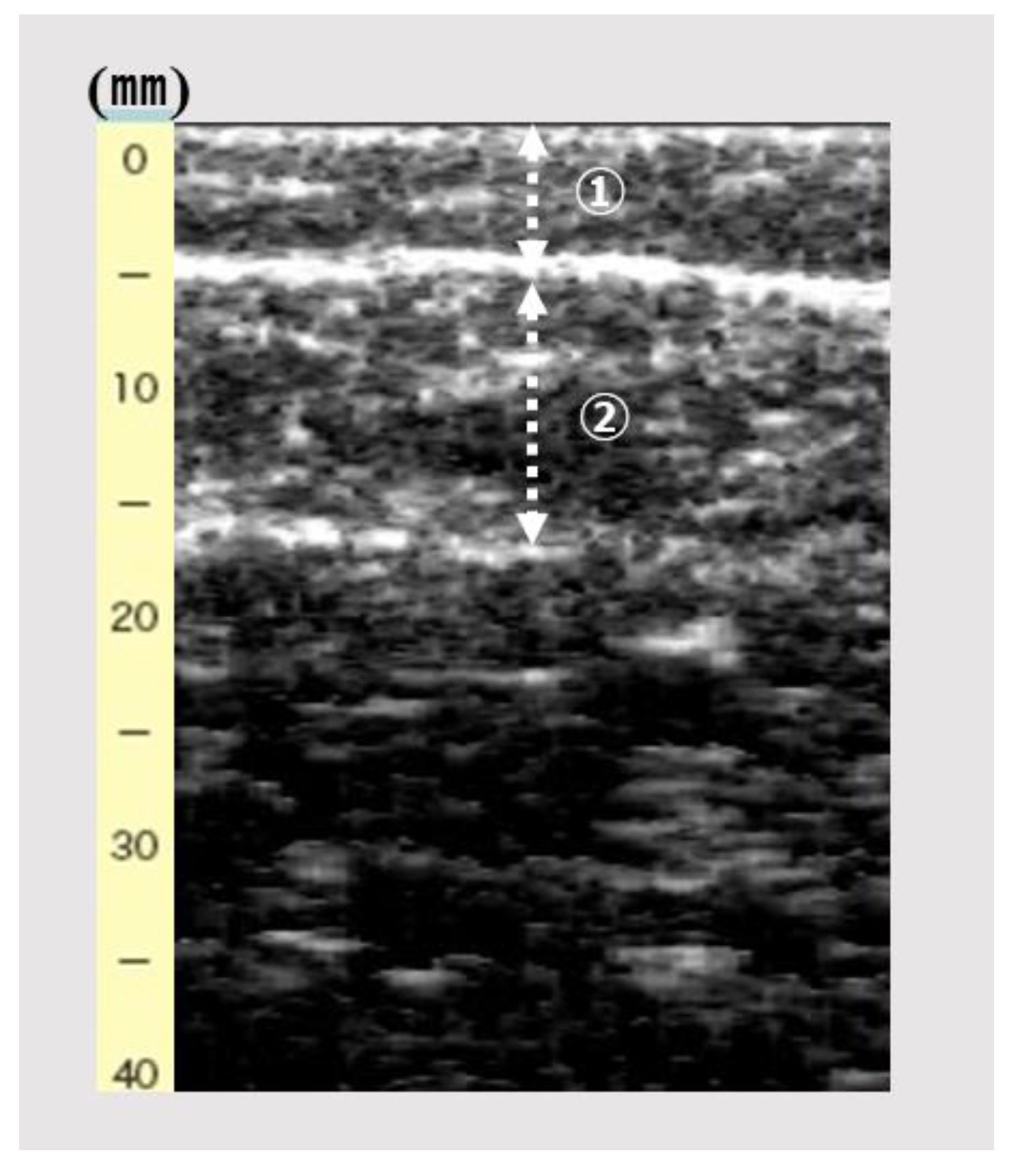
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beaudart, C.; Reginster, J.Y.; Petermans, J.; Gillain, S.; Quabron, A.; Locquet, M.; Slomian, J.; Buckinx, F.; Bruyère, O. Quality of life and physical components linked to sarcopenia: The SarcoPhAge study. Exp. Gerontol. 2015, 69, 103–110. [Google Scholar] [CrossRef]
- Spira, D.; Buchmann, N.; Nikolov, J.; Demuth, I.; Steinhagen-Thiessen, E.; Eckardt, R.; Norman, K. Association of Low Lean Mass with Frailty and Physical Performance: A Comparison Between Two Operational Definitions of Sarcopenia-Data from the Berlin Aging Study II (BASE-II). J. Gerontol. Ser. A 2015, 70, 779–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkins, J.L.; Whincup, P.H.; Morris, R.W.; Lennon, L.T.; Papacosta, O.; Wannamethee, S.G. Sarcopenic obesity and risk of cardiovascular disease and mortality: A population-based cohort study of older men. J. Am. Geriatr. Soc. 2014, 62, 253–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. JAMDA 2020, 21, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Kushner, R.F.; Gudivaka, R.; Schoeller, D.A. Clinical characteristics influencing bioelectrical impedance analysis measurements. Am. J. Clin. Nutr. 1996, 64, 423S–427S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fülster, S.; Tacke, M.; Sandek, A.; Ebner, N.; Tschöpe, C.; Doehner, W.; Anker, S.D.; von Haehling, S. Muscle wasting in patients with chronic heart failure: Results from the studies investigating co-morbidities aggravating heart failure (SICA-HF). Eur. Heart J. 2013, 34, 512–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narumi, T.; Watanabe, T.; Kadowaki, S.; Takahashi, T.; Yokoyama, M.; Kinoshita, D.; Honda, Y.; Funayama, A.; Nishiyama, S.; Takahashi, H.; et al. Sarcopenia evaluated by fat-free mass index is an important prognostic factor in patients with chronic heart failure. Eur. J. Intern. Med. 2015, 26, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Nishio, N.; Abe, Y.; Kakehi, T.; Fujimoto, J.; Tanaka, T.; Ohji, S.; Otobe, Y.; et al. Differential Characteristics of Skeletal Muscle in Community-Dwelling Older Adults. J. Am. Med. Dir. Assoc. 2017, 18, 807.e9–807.e16. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Hun, Y.; Tian, G. Ultrasound measurements of gastrocnemius muscle thickness in older people with sarcopenia. Clin. Interv. Aging 2018, 13, 2193–2199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuyumcu, M.E.; Halil, M.; Kara, O.; Çuni, B.; Çağlayan, G.; Güven, S.; Yeşil, Y.; Arık, G.; Yavuz, B.B.; Cankurtaran, M.; et al. Ultrasonographic evaluation of the calf muscle mass and architecture in elderly patients with and without sarcopenia. Arch. Gerontol. Geriatr. 2016, 65, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Sari, A.; Esme, M.; Aycicek, G.S.; Armagan, B.; Kilic, L.; Ertenli, A.I.; Halil, M.G.; Akdogan, A. Evaluating skeletal muscle mass with ultrasound in patients with systemic sclerosis. Nutrition 2021, 84, 110999. [Google Scholar] [CrossRef] [PubMed]
- Lera, L.; Albala, C.; Ángel, B.; Sánchez, H.; Picrin, Y.; Hormazabal, M.J.; Quiero, A. Anthropometric model for the prediction of appendicular skeletal muscle mass in Chilean older adults. Nutr. Hosp. 2014, 29, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Fujita, E.; Fukunaga, T.; Sawai, S. Quantitative evaluation of human muscle hardness using a newly developed ultrasonography. J. Jpn. Phys. Ther. Assoc. 2015, 42, 255–261. (In Japanese) [Google Scholar]
- Akima, H.; Yoshiko, A.; Tomita, A.; Ando, R.; Saito, A.; Ogawa, M.; Kondo, S.; Tanaka, N.I. Relationship between quadriceps echo intensity and functional and morphological characteristics in older men and women. Arch. Gerontol. Geriatr. 2017, 70, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Arts, I.M.P.; Pillen, S.; Schelhaas, H.J.; Overeem, S.; Zwarts, M.J. Normal values for quantitative muscle ultrasonography in adults. Muscle Nerve 2010, 41, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Burton, A.M.; Stock, M.S. Consistency of novel ultrasound equations for estimating percent intramuscular fat. Clin. Physiol. Funct. Imaging 2018, 38, 1062–1066. [Google Scholar] [CrossRef] [PubMed]
- Tey, S.L.; Chew, S.; How, C.H.; Yalawar, M.; Baggs, G.; Chow, W.L.; Cheong, M.; Ong, R.H.S.; Husain, F.S.; Kwan, S.C.; et al. Factors associated with muscle mass in community-dwelling older people in Singapore: Findings from the SHIELD study. PLoS ONE 2019, 14, e0223222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakanishi, N.; Tsutsumi, R.; Okayama, Y.; Takashima, T.; Ueno, Y.; Itagaki, T.; Tsutsumi, Y.; Sakaue, H.; Oto, J. Monitoring of muscle mass in critically ill patients: Comparison of ultrasound and two bioelectrical impedance analysis devices. J. Intensive Care 2019, 16, 61. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total n = 193 | Men n = 72 | Women n = 121 | p-Value (Men vs. Women) | |
|---|---|---|---|---|
| Age; years | 72.4 ± 4.3 | 73.2 ± 4.3 | 71.9 ± 4.2 | <0.05 |
| BMI; kg/m2 | 22.4 ± 2.9 | 23.2 ± 3.0 | 21.9 ± 2.8 | <0.01 |
| Grip strength; kg | 28.6 ± 7.9 | 36.6 ± 5.9 | 23.8 ± 4.2 | <0.001 |
| Low grip strength; n (%) | 11 (5.7) | 4 (5.5) | 7 (5.8) | 0.77 |
| Gait speed; m/s | 2.0 ± 0.4 | 1.9 ± 0.4 | 2.0 ± 0.4 | 0.24 |
| Low gait speed; n (%) | 9 (4.7) | 6 (8.3) | 3 (2.5) | 0.06 |
| SMI; kg/m2 | 7.0 ± 1.1 | 8.0 ± 1.0 | 6.4 ± 0.7 | <0.001 |
| Low muscle mass; n (%) | 31 (16.1) | 12 (16.7) | 19 (15.7) | 0.86 |
| Ultrasonography | ||||
| SFT; mm | 4.1 ± 2.2 | 2.6 ± 1.5 | 5.0 ± 2.1 | <0.001 |
| GT; mm | 13.0 ± 2.2 | 13.6 ± 2.6 | 12.7 ± 1.8 | <0.01 |
| Variable | r | p |
|---|---|---|
| Age | 0.15 | 0.49 |
| BMI | 0.67 | <0.001 |
| Grip strength | 0.62 | <0.001 |
| Gait speed | −0.06 | 0.41 |
| SFT | −0.09 | 0.22 |
| GT | 0.51 | <0.001 |
| Variable | Model 1 | Model 2 | Model 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | SE B | β | B | SE B | β | B | SE B | β | VIF | |
| Men | 1.57 | 0.12 | 0.69 * | 1.32 | 0.08 | 0.58 * | 1.27 | 0.08 | 0.56 * | 1.06 |
| BMI | 0.21 | 0.01 | 0.55 * | 0.18 | 0.01 | 0.47 * | 1.27 | |||
| GT | 0.09 | 0.02 | 0.19 * | 1.27 | ||||||
| α | 6.41 | 0.07 | 1.88 | 0.30 | 1.33 | 0.30 | ||||
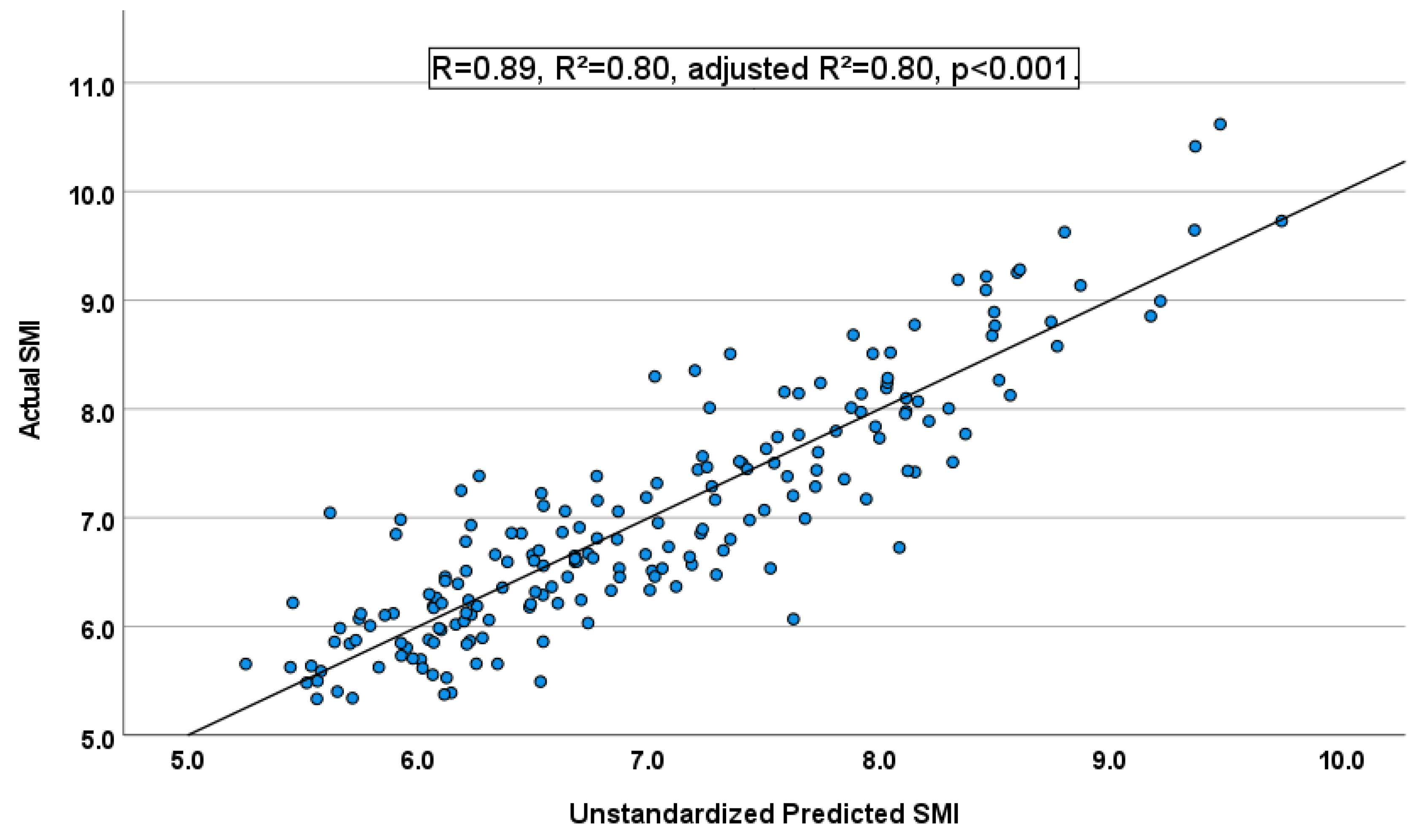
| R | 0.69 | 0.88 | 0.89 | |||||||
| R2 | 0.48 | 0.77 | 0.80 | |||||||
| Adjusted R2 | 0.48 | 0.77 | 0.80 | |||||||
| F | 175.2 * | 318.1 * | 247.6 * | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuguchi, S.; Asahi, R.; Kamo, T.; Azami, M.; Ogihara, H. Prediction Model including Gastrocnemius Thickness for the Skeletal Muscle Mass Index in Japanese Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 4042. https://doi.org/10.3390/ijerph19074042
Yuguchi S, Asahi R, Kamo T, Azami M, Ogihara H. Prediction Model including Gastrocnemius Thickness for the Skeletal Muscle Mass Index in Japanese Older Adults. International Journal of Environmental Research and Public Health. 2022; 19(7):4042. https://doi.org/10.3390/ijerph19074042
Chicago/Turabian StyleYuguchi, Satoshi, Ryoma Asahi, Tomohiko Kamo, Masato Azami, and Hirofumi Ogihara. 2022. "Prediction Model including Gastrocnemius Thickness for the Skeletal Muscle Mass Index in Japanese Older Adults" International Journal of Environmental Research and Public Health 19, no. 7: 4042. https://doi.org/10.3390/ijerph19074042