
Evaluation of BNT162b2 Vaccine Effectiveness in Galicia, Northwest Spain

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Exposure and Outcome Ascertainment
2.4. Statistical Analysis
3. Results
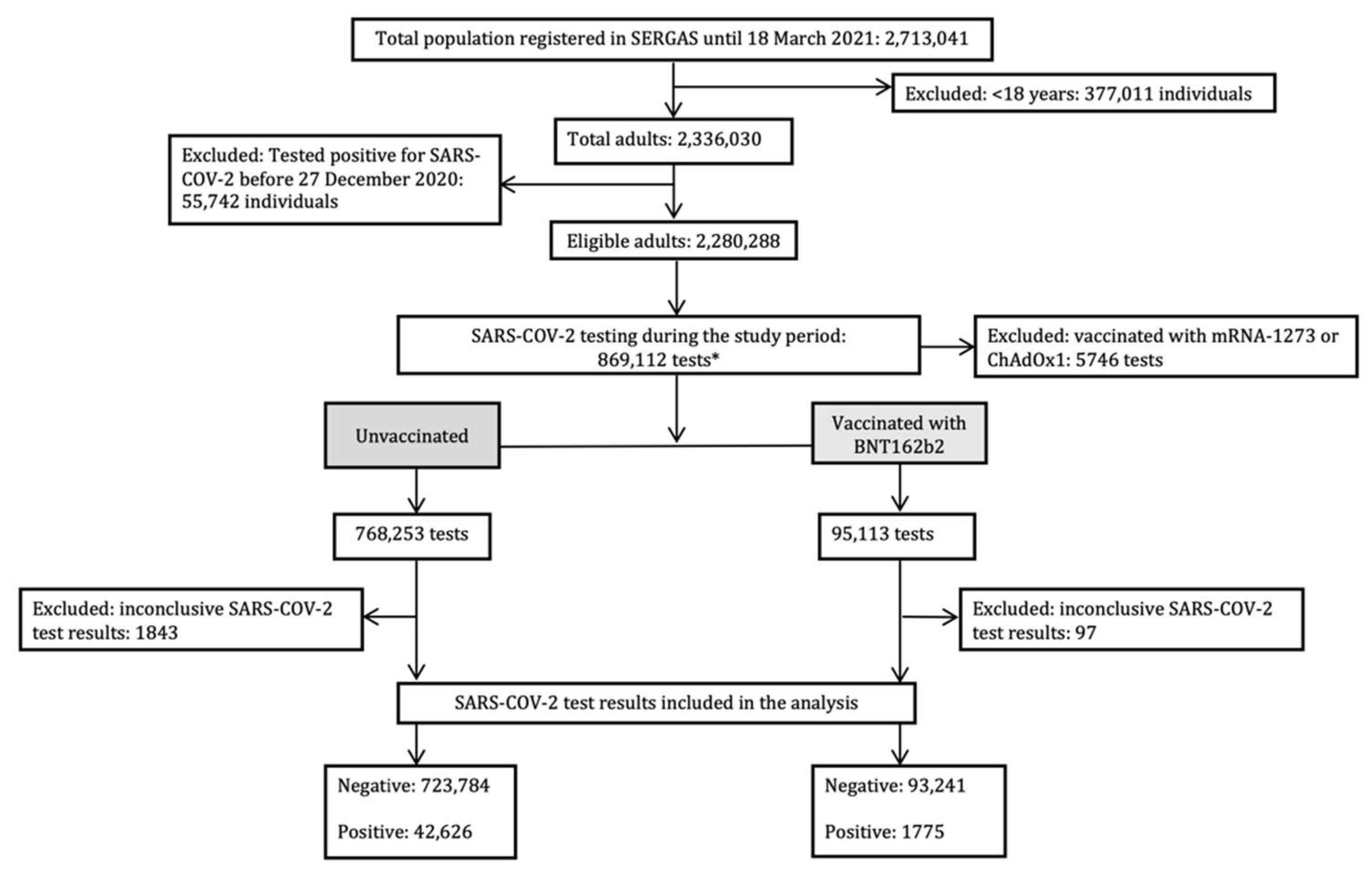
3.1. Study Population
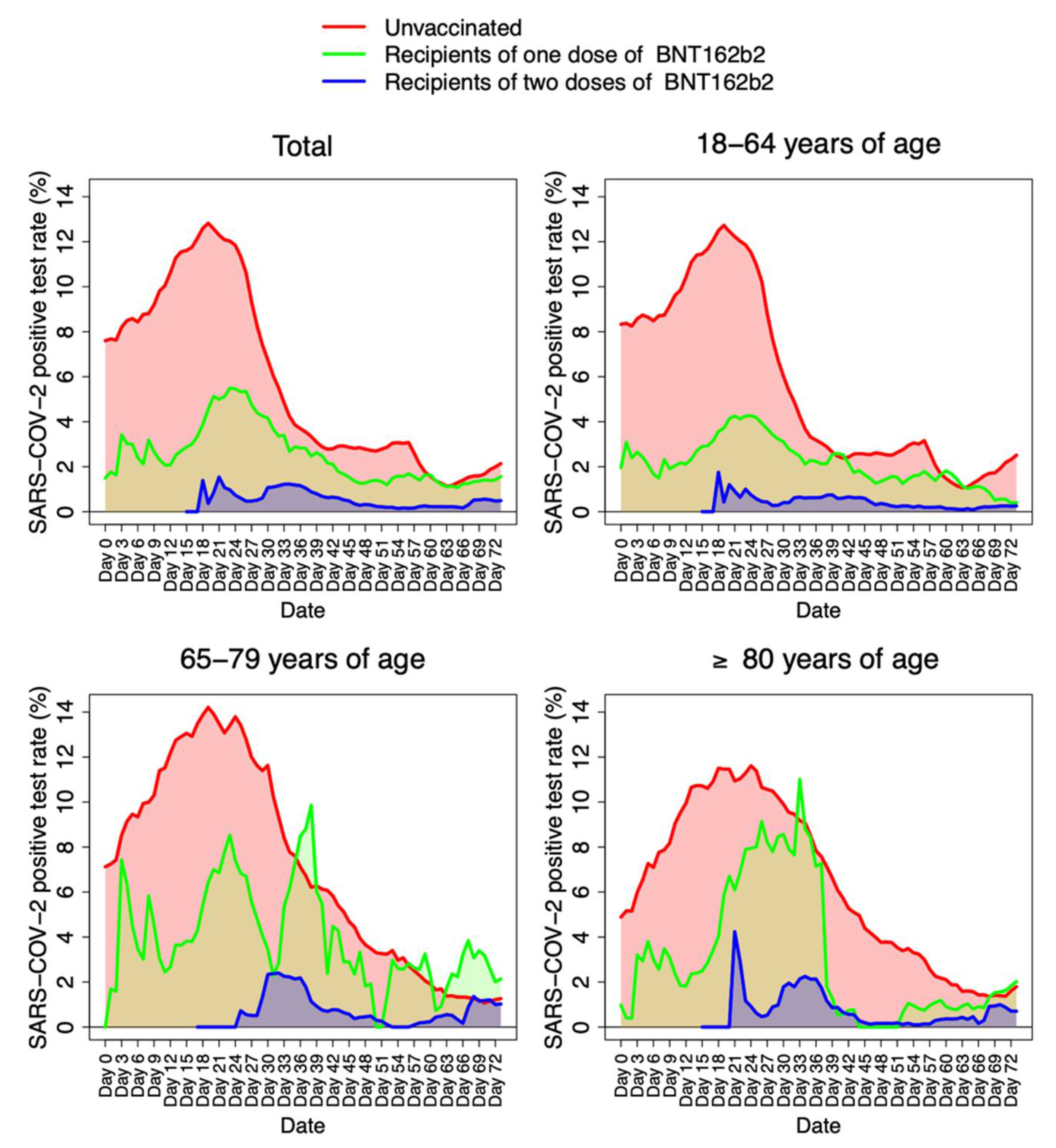
3.2. BNT162b2 Vaccine Effectiveness against SARS-CoV-2 Infection
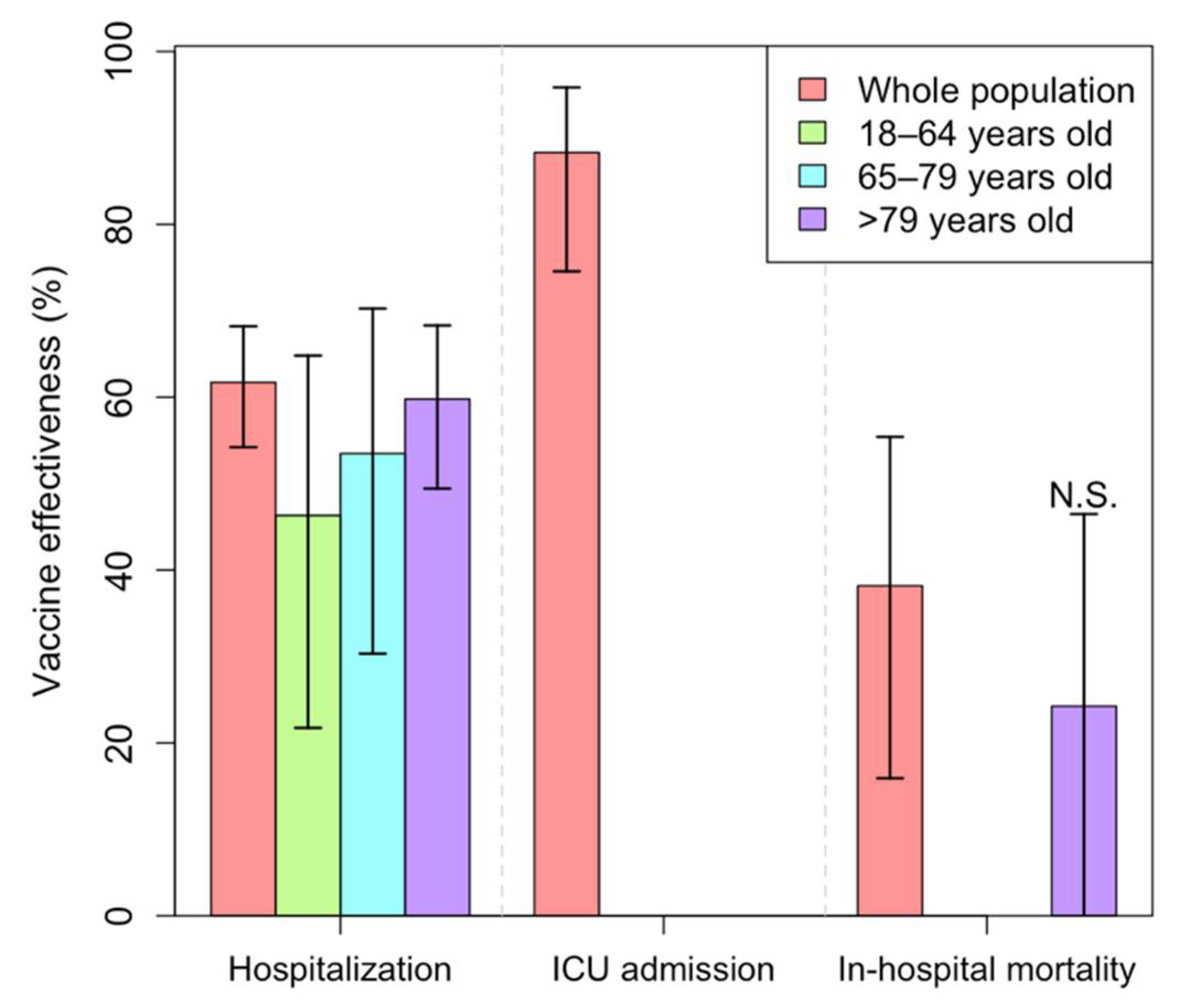
3.3. BNT162b2 Vaccine Effectiveness against COVID-19 Severity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Medicines Agency. COVID-19 Vaccines: Authorised; European Medicines Agency: Amsterdam, The Netherlands, 2020.
- Ministerio de Sanidad. Estrategia de Vacunación Frente al COVD-19 en España; Ministerio de Sanidad: Madrid, Spain, 2020.
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Poland, G.A.; Ovsyannikova, I.G.; Kennedy, R.B.; Haralambieva, I.H.; Jacobson, R.M. Vaccinomics and a new paradigm for the development of preventive vaccines against viral infections. OMICS 2011, 15, 625–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kow, C.S.; Hasan, S.S. Real-world effectiveness of BNT162b2 mRNA vaccine: A meta-analysis of large observational studies. Inflammopharmacology 2021, 29, 1075–1090. [Google Scholar] [CrossRef] [PubMed]
- Dean, N.E.; Hogan, J.W.; Schnitzer, M.E. COVID-19 Vaccine Effectiveness and the Test-Negative Design. N. Engl. J. Med. 2021, 385, 1431–1433. [Google Scholar] [CrossRef]
- Fukushima, W.; Hirota, Y. Basic principles of test-negative design in evaluating influenza vaccine effectiveness. Vaccine 2017, 35, 4796–4800. [Google Scholar] [CrossRef]
- Chua, H.; Feng, S.; Lewnard, J.A.; Sullivan, S.G.; Blyth, C.C.; Lipsitch, M.; Cowling, B.J. The Use of Test-negative Controls to Monitor Vaccine Effectiveness: A Systematic Review of Methodology. Epidemiology 2020, 31, 43–64. [Google Scholar] [CrossRef]
- SERGAS. Plan Galego de Vacinación Fronte Ao SARS-CoV-2; Sergas: Galicia, Spain, 2021; Available online: https://coronavirus.sergas.gal/Contidos/Plan-galego-vacinacion-COVID (accessed on 15 February 2022).
- R Core Team R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021.
- Vasileiou, E.; Simpson, C.R.; Shi, T.; Kerr, S.; Agrawal, U.; Akbari, A.; Bedston, S.; Beggs, J.; Bradley, D.; Chuter, A.; et al. Interim findings from first-dose mass COVID-19 vaccination roll-out and COVID-19 hospital admissions in Scotland: A national prospective cohort study. Lancet 2021, 397, 1646–1657. [Google Scholar] [CrossRef]
- Amit, S.; Regev-Yochay, G.; Afek, A.; Kreiss, Y.; Leshem, E. Early rate reductions of SARS-CoV-2 infection and COVID-19 in BNT162b2 vaccine recipients. Lancet 2021, 397, 875–877. [Google Scholar] [CrossRef]
- Pritchard, E.; Matthews, P.C.; Stoesser, N.; Eyre, D.W.; Gethings, O.; Vihta, K.D.; Jones, J.; House, T.; VanSteenHouse, H.; Bell, I.; et al. Impact of vaccination on new SARS-CoV-2 infections in the United Kingdom. Nat. Med. 2021, 27, 1370–1378. [Google Scholar] [CrossRef]
- Harel, T.; Hacohen, N.; Shaag, A.; Gomori, M.; Singer, A.; Elpeleg, O.; Meiner, V. Homozygous null variant in CRADD, encoding an adaptor protein that mediates apoptosis, is associated with lissencephaly. Am. J. Med. Genet. A 2017, 173, 2539–2544. [Google Scholar] [CrossRef]
- Shrotri, M.; Krutikov, M.; Palmer, T.; Giddings, R.; Azmi, B.; Subbarao, S.; Fuller, C.; Irwin-Singer, A.; Davies, D.; Tut, G.; et al. Vaccine effectiveness of the first dose of ChAdOx1 nCoV-19 and BNT162b2 against SARS-CoV-2 infection in residents of long-term care facilities in England (VIVALDI): A prospective cohort study. Lancet Infect. Dis. 2021, 21, 1529–1538. [Google Scholar] [CrossRef]
- Cabezas, C.; Coma, E.; Mora-Fernandez, N.; Li, X.; Martinez-Marcos, M.; Fina, F.; Fabregas, M.; Hermosilla, E.; Jover, A.; Contel, J.C.; et al. Associations of BNT162b2 vaccination with SARS-CoV-2 infection and hospital admission and death with COVID-19 in nursing homes and healthcare workers in Catalonia: Prospective cohort study. BMJ 2021, 374, n1868. [Google Scholar] [CrossRef] [PubMed]
- Monge, S.; Olmedo, C.; Alejos, B.; Lapeña, M.F.; Sierra, M.J.; Limia, A.; COVID-19 Registries Study Group. Direct and Indirect Effectiveness of mRNA Vaccination against Severe Acute Respiratory Syndrome Coronavirus 2 in Long-Term Care Facilities, Spain. Emerg. Infect. Dis 2021, 27, 2595–2603. [Google Scholar] [CrossRef] [PubMed]
- Mazagatos, C.; Monge, S.; Olmedo, C.; Vega, L.; Gallego, P.; Martín-Merino, E.; Sierra, M.J.; Limia, A.; Larrauri, A.; Working Group for the Surveillance and Control of COVID-19 in Spain. Effectiveness of mRNA COVID-19 vaccines in preventing SARS-CoV-2 infections and COVID-19 hospitalisations and deaths in elderly long-term care facility residents, Spain, weeks 53 2020 to 13 2021. Euro Surveill. 2021, 26, 2100452. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Baz, I.; Miqueleiz, A.; Casado, I.; Navascués, A.; Trobajo-Sanmartín, C.; Burgui, C.; Guevara, M.; Ezpeleta, C.; Castilla, J.; Working Group for the Study of COVID-19 in Navarra. Effectiveness of COVID-19 vaccines in preventing SARS-CoV-2 infection and hospitalisation, Navarre, Spain, January to April 2021. Euro Surveill. 2021, 26, 2100438. [Google Scholar] [CrossRef]
- Gómez-Carballa, A.; Pardo-Seco, J.; Bello, X.; Martinón-Torres, F.; Salas, A. Superspreading in the emergence of COVID-19 variants. Trends Genet. 2021, 37, 1069–1080. [Google Scholar] [CrossRef]
- Gómez-Carballa, A.; Bello, X.; Pardo-Seco, J.; Pérez Del Molino, M.L.; Martinón-Torres, F.; Salas, A. Phylogeography of SARS-CoV-2 pandemic in Spain: A story of multiple introductions, micro-geographic stratification, founder effects, and super-spreaders. Zool. Res. 2020, 41, 605–620. [Google Scholar] [CrossRef]
- Gómez-Carballa, A.; Bello, X.; Pardo-Seco, J.; Martinón-Torres, F.; Salas, A. Mapping genome variation of SARS-CoV-2 worldwide highlights the impact of COVID-19 super-spreaders. Genome Res. 2020, 30, 1434–1448. [Google Scholar] [CrossRef]
- Brunet-Ratnasingham, E.; Anand, S.P.; Gantner, P.; Dyachenko, A.; Moquin-Beaudry, G.; Brassard, N.; Beaudoin-Bussières, G.; Pagliuzza, A.; Gasser, R.; Benlarbi, M.; et al. Integrated immunovirological profiling validates plasma SARS-CoV-2 RNA as an early predictor of COVID-19 mortality. Sci. Adv. 2021, 7, eabj5629. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.V. Side effects of BNT162b2 mRNA COVID-19 vaccine: A randomized, cross-sectional study with detailed self-reported symptoms from healthcare workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. of Participants | Vaccination Status | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unvaccinated (n = 766,410) | Dose 1 (n = 42,999) | Dose 2 (n = 52,017) | Dose 2 (n = 52,017) | |||||||||||
| Negative Test | Positive Test | Negative Test | Positive Test | Negative Test | Positive Test | |||||||||
| n | % | n | % | n | % | n | % | n | % | % | n | % | ||
| Whole population | 861,426 | - | 723,784 | 94.4% | 42,626 | 5.6% | 41,497 | 96.5% | 1502 | 3.5% | 51,744 | 99.5% | 273 | 0.5% |
| Age category (Years) | ||||||||||||||
| 18–64 | 680,312 | 78.5% | 583,526 | 94.8% | 32,285 | 5.2% | 26,499 | 97.0% | 809 | 3.0% | 31,381 | 99.6% | 122 | 0.4% |
| 65–79 | 104,198 | 12.0% | 88,491 | 93.1% | 6598 | 6.9% | 3735 | 95.3% | 183 | 4.7% | 5108 | 99.2% | 41 | 0.8% |
| ≥80 | 82,650 | 9.5% | 51,767 | 93.3% | 3743 | 6.7% | 11,263 | 95.7% | 510 | 4.3% | 15,255 | 99.3% | 110 | 0.7% |
| Sex | ||||||||||||||
| Male | 366,578 | 42.3% | 322,178 | 94.7% | 20,116 | 5.3% | 10,220 | 96.5% | 366 | 3.5% | 12,356 | 99.5% | 82 | 0.5% |
| Female | 500,567 | 57.7% | 401,591 | 94.1% | 22,510 | 5.9% | 31,277 | 96.5% | 1502 | 3.5% | 39,388 | 99.3% | 191 | 0.7% |
| Missing | 15 | 0.0% | 15 | 100% | - | - | - | - | - | - | - | - | - | - |
| Whole Population | 18–64 Years | 65–79 Years | ≥80 Years | |||||
|---|---|---|---|---|---|---|---|---|
| Vaccination Status | OR | VE | OR | VE | OR | VE | OR | VE |
| (95% CI) 1 | (95% CI) | (95% CI) 1 | (95% CI) | (95% CI) 2 | (95% CI) | (95% CI) 2 | (95% CI) | |
| Unvaccinated | 1 | - | 1 | - | 1 | - | 1 | - |
| 1–6 days dose 1 | 0.3 | 70.50% | 0.37 | 63.10% | 0.2 | 80.50% | 0.19 | 81.30% |
| (0.26–0.33) | (66.5–74.1) | (0.32–0.42) | (57.5–68.1) | (0.12–0.31) | (69–88.6) | (0.13–0.26) | (74.3–86.8) | |
| 7–13 days dose 1 | 0.36 | 64.30% | 0.36 | 63.80% | 0.38 | 62.90% | 0.43 | 57.90% |
| (0.33–0.39) | (61.2–67.2) | (0.32–0.40) | (59.7–67.7) | (0.29–0.47) | (53.2–71.2) | (0.36–0.50) | (50.8–64.1) | |
| 14–20 days dose 1 | 0.32 | 67.70% | 0.25 | 74.70% | 0.43 | 57.40% | 0.5 | 51.40% |
| (0.29–0.35) | (64.6–70.6) | (0.22–0.29) | (71.0–78.0) | (0.34–0.55) | (46.1–66.9) | (0.42–0.58) | (43.5–58.4) | |
| 1–6 days dose 2 | 0.18 | 81.60% | 0.17 | 83.40% | 0.22 | 78.70% | 0.16 | 84.70% |
| (0.15–0.22) | (77.7–85.0) | (0.12–0.22) | (78.3–87.6) | (0.12–0.36) | (65.1–88.1) | (0.11–0.22) | (78.9–89.3) | |
| 7–13 days dose 2 | 0.25 | 75.40% | 0.21 | 79.00% | 0.17 | 83% | 0.22 | 78.80% |
| (0.20–0.30) | (70.1–80.1) | (0.15–0.28) | (71.7–84.9) | (0.09–0.29) | (71.2–90.9) | (0.16–0.29) | (71.7–84.6) | |
| ≥14 days dose 2 | 0.09 | 90.80% | 0.07 | 92.90% | 0.15 | 85.80% | 0.09 | 91.40% |
| (0.07–0.11) | (88.6–92.7) | (0.05–0.10) | (90.2–95.1) | (0.08–0.23) | (77.3–91.9) | (0.06–0.12) | (87.9–94.1) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pardo-Seco, J.; Mallah, N.; López-Pérez, L.R.; González-Pérez, J.M.; Rosón, B.; Otero-Barrós, M.T.; Durán-Parrondo, C.; Rodríguez-Tenreiro, C.; Rivero-Calle, I.; Gómez-Carballa, A.; et al. Evaluation of BNT162b2 Vaccine Effectiveness in Galicia, Northwest Spain. Int. J. Environ. Res. Public Health 2022, 19, 4039. https://doi.org/10.3390/ijerph19074039
Pardo-Seco J, Mallah N, López-Pérez LR, González-Pérez JM, Rosón B, Otero-Barrós MT, Durán-Parrondo C, Rodríguez-Tenreiro C, Rivero-Calle I, Gómez-Carballa A, et al. Evaluation of BNT162b2 Vaccine Effectiveness in Galicia, Northwest Spain. International Journal of Environmental Research and Public Health. 2022; 19(7):4039. https://doi.org/10.3390/ijerph19074039
Chicago/Turabian StylePardo-Seco, Jacobo, Narmeen Mallah, Luis Ricardo López-Pérez, Juan Manuel González-Pérez, Benigno Rosón, María Teresa Otero-Barrós, Carmen Durán-Parrondo, Carmen Rodríguez-Tenreiro, Irene Rivero-Calle, Alberto Gómez-Carballa, and et al. 2022. "Evaluation of BNT162b2 Vaccine Effectiveness in Galicia, Northwest Spain" International Journal of Environmental Research and Public Health 19, no. 7: 4039. https://doi.org/10.3390/ijerph19074039