
Comparison of Physical Fitness Profiles Obtained before and during COVID-19 Pandemic in Two Independent Large Samples of Children and Adolescents: DAFIS Project

 ,
,  ,
,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
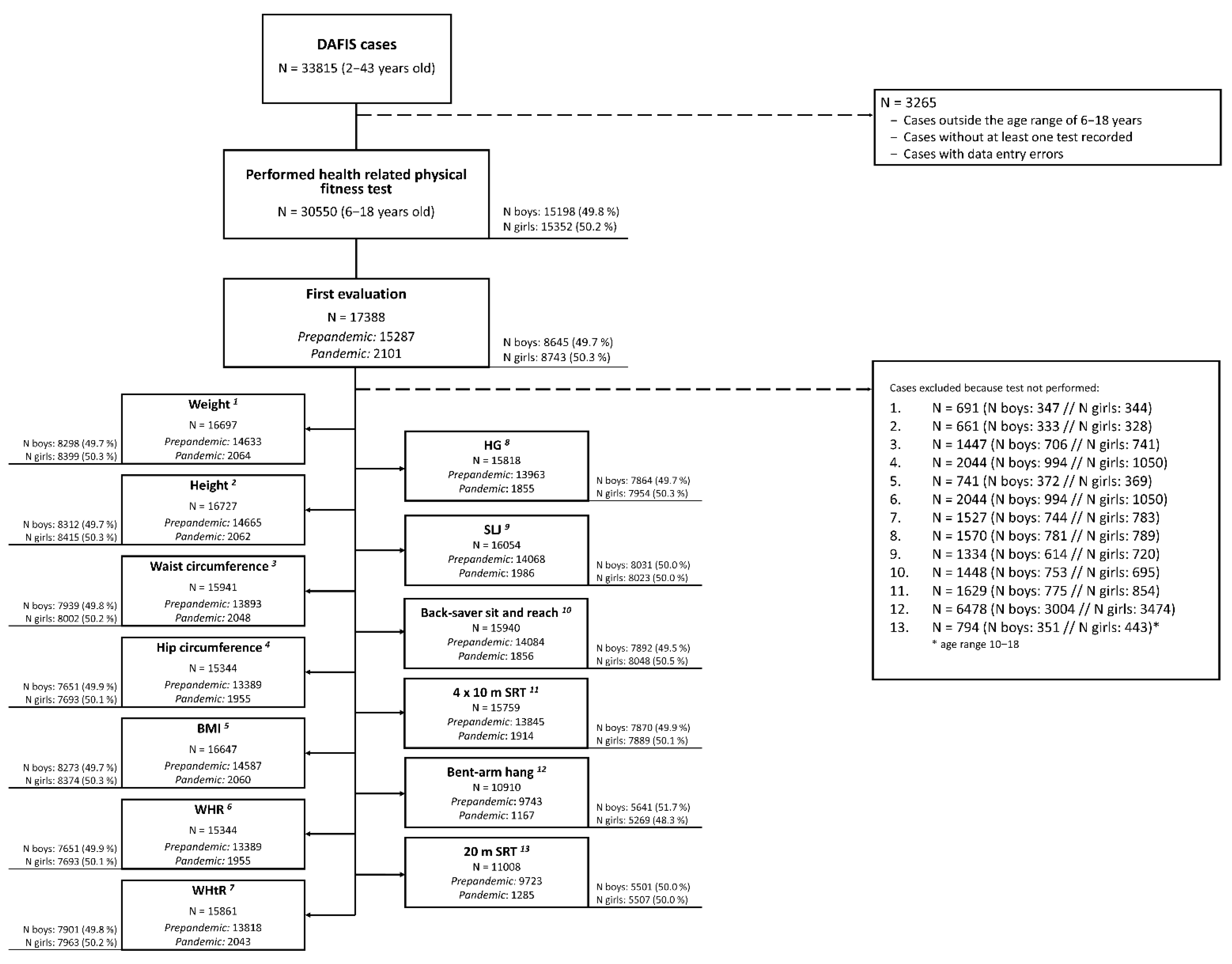
2.1. Participants
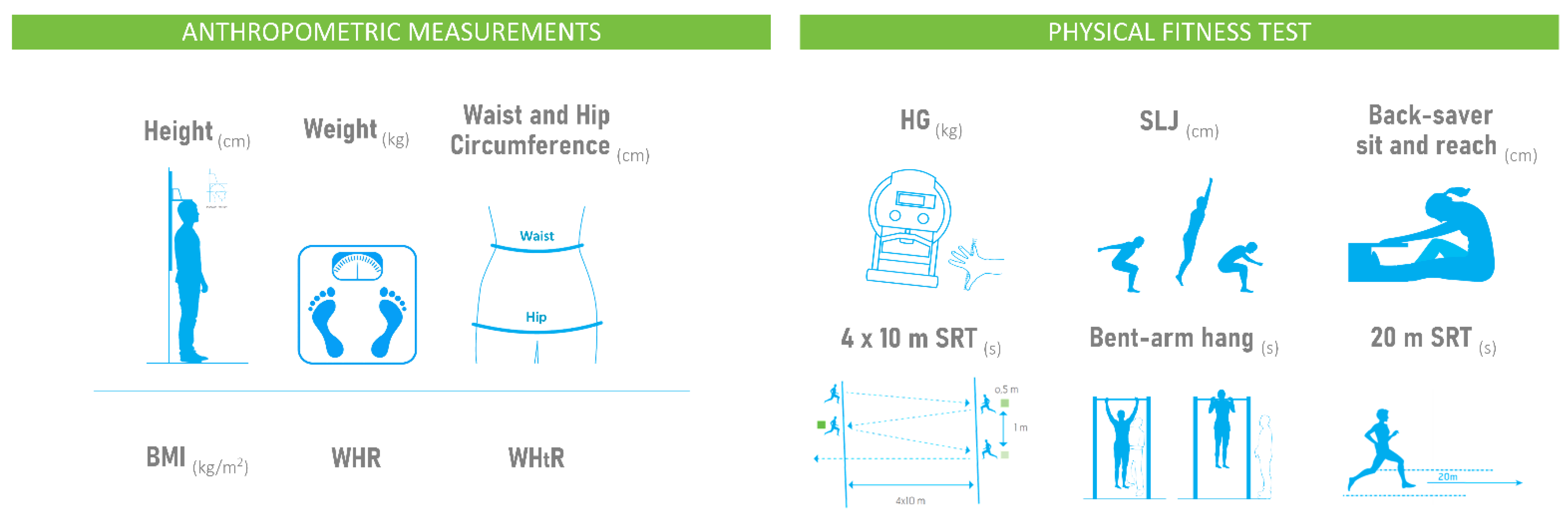
2.2. Anthropometric and Physical Fitness Evaluation: DAFIS Battery
2.3. Statistical Analysis
3. Results
3.1. Sex and Age Characteristics of the Samples
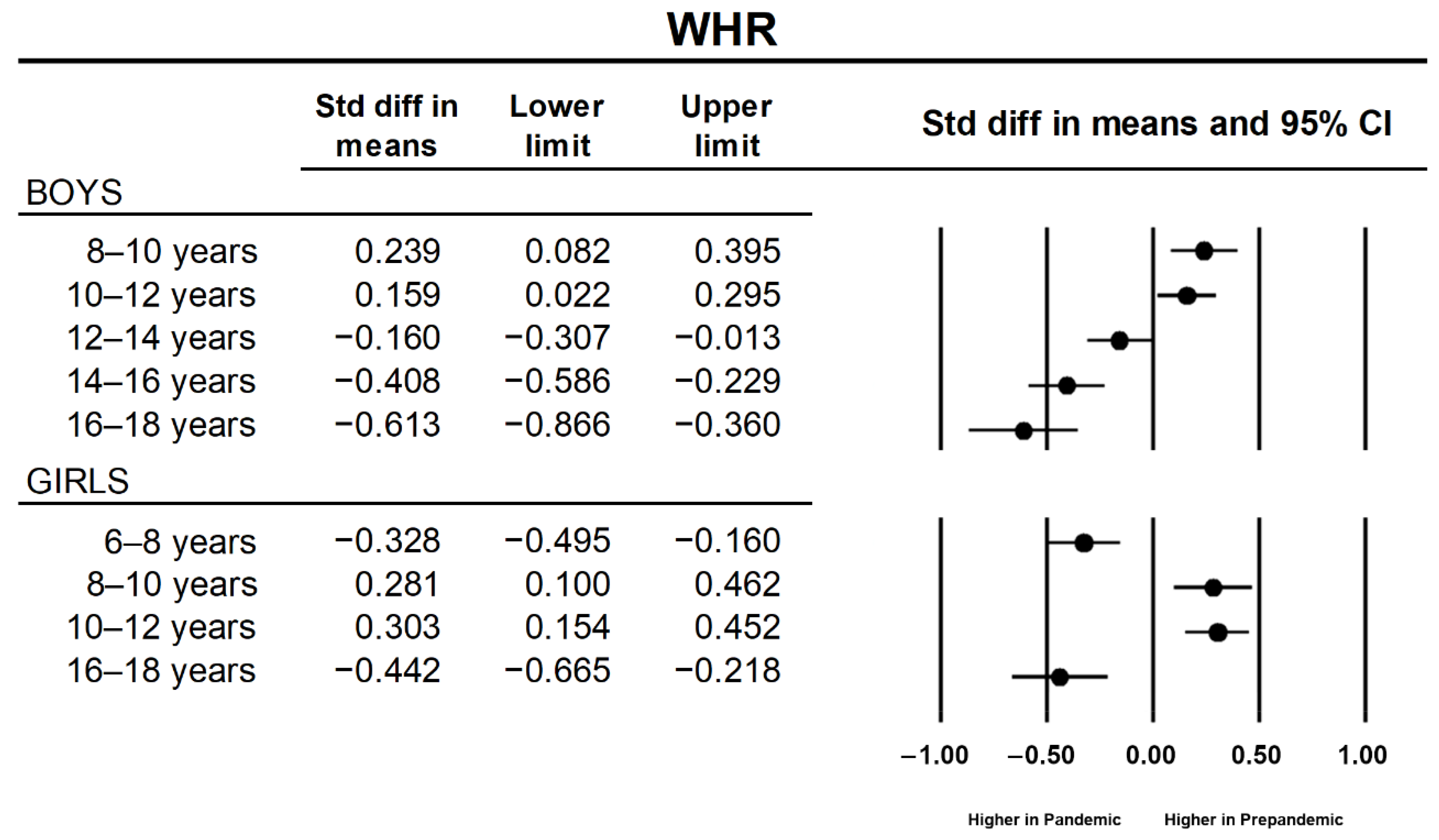
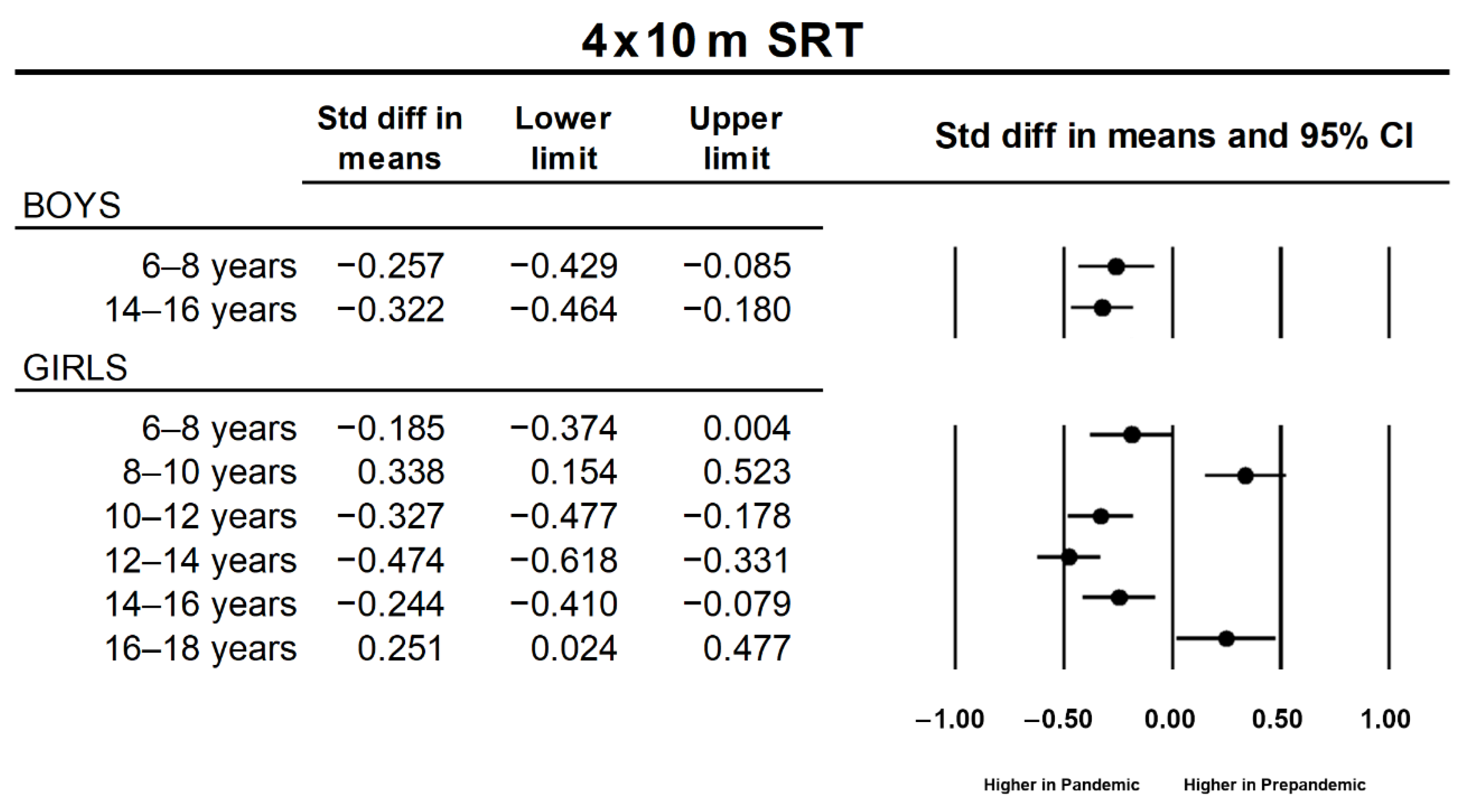
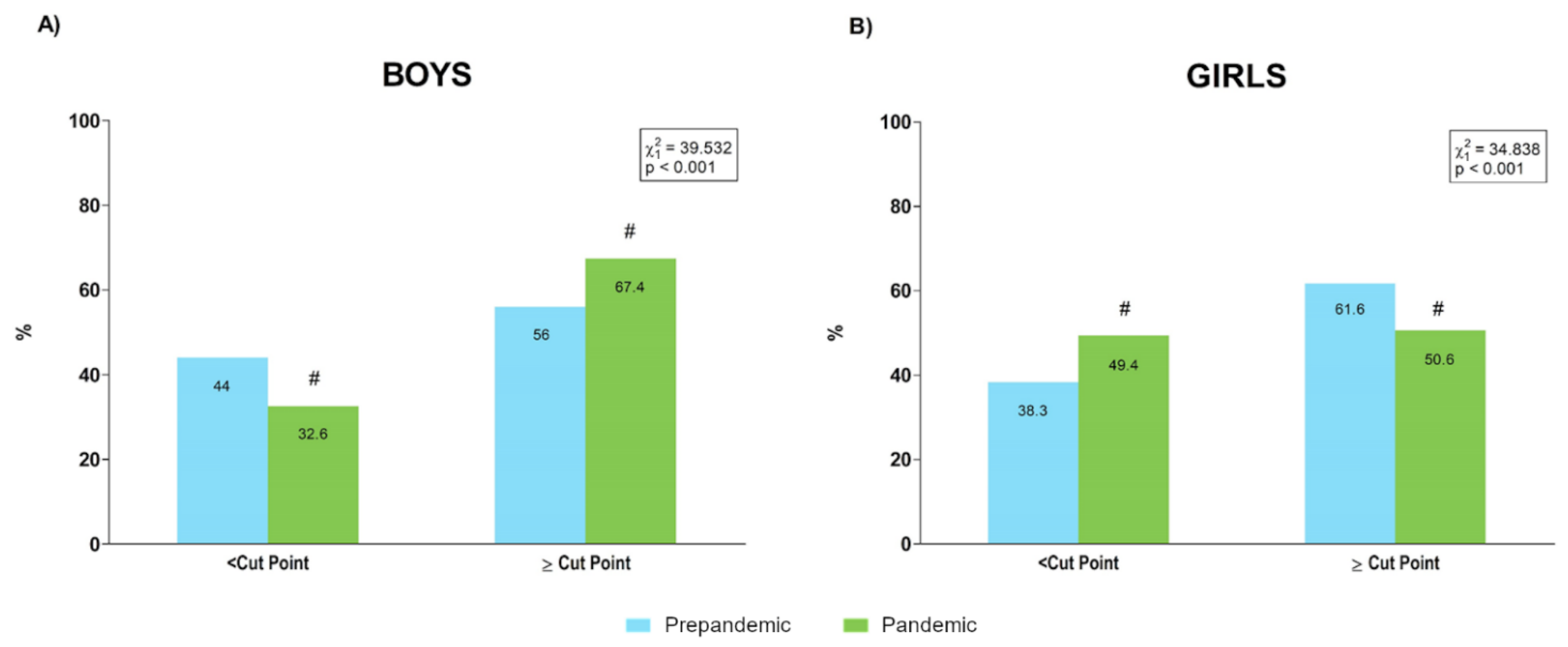
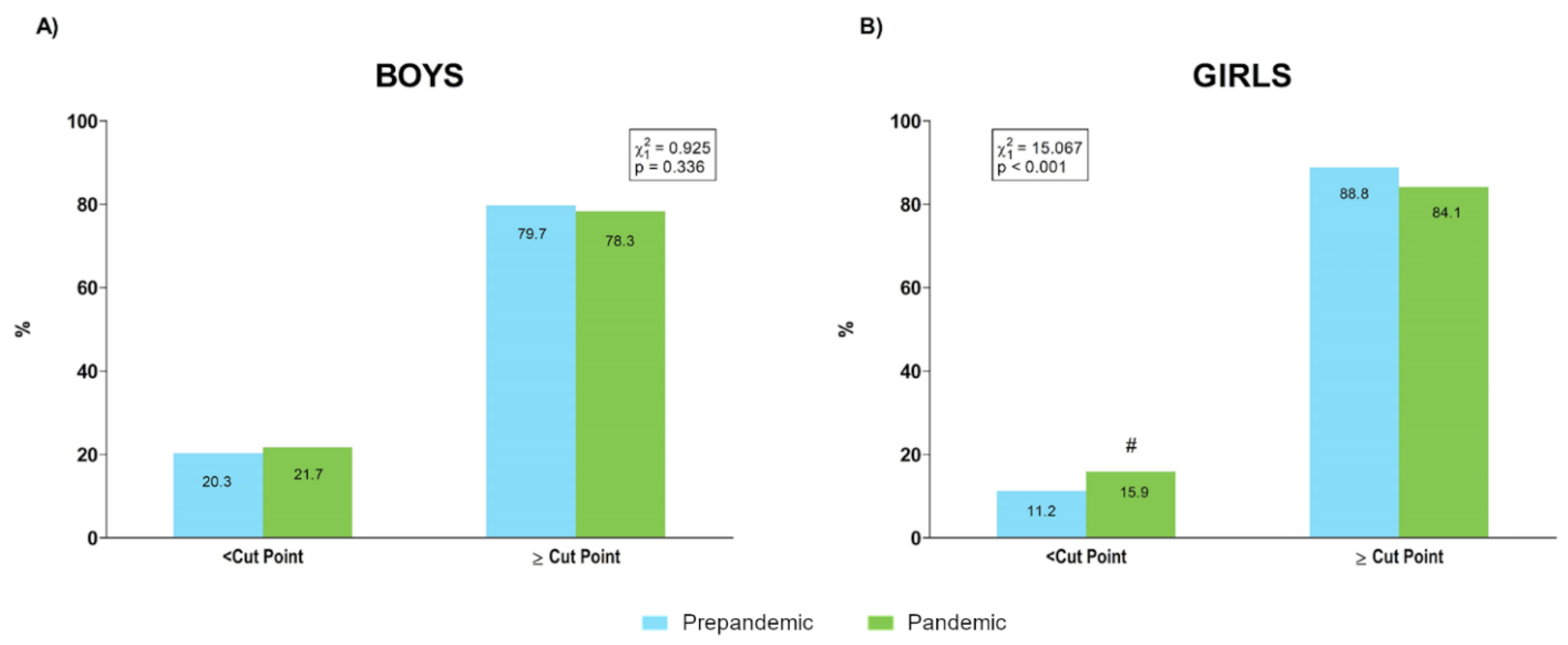
3.2. Health-Related Tests Results
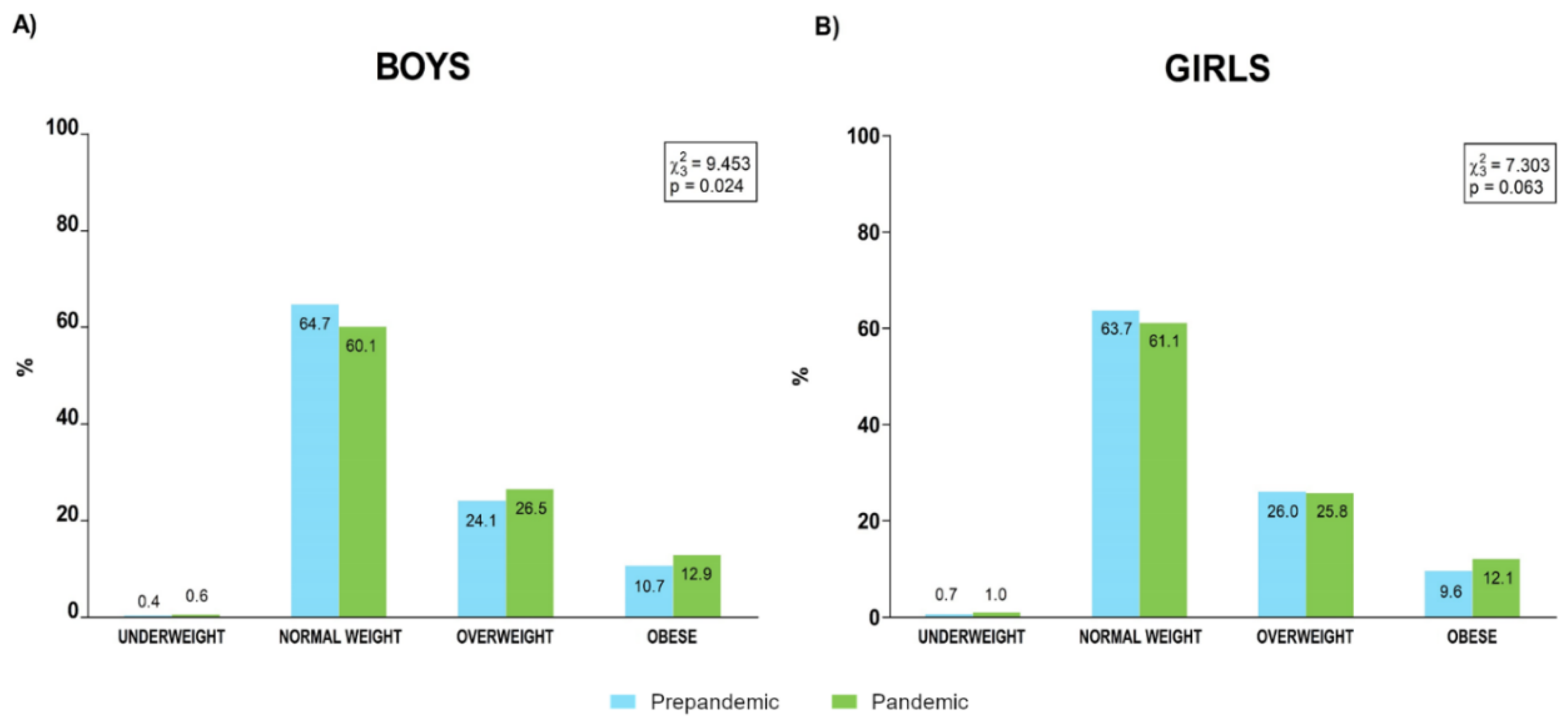
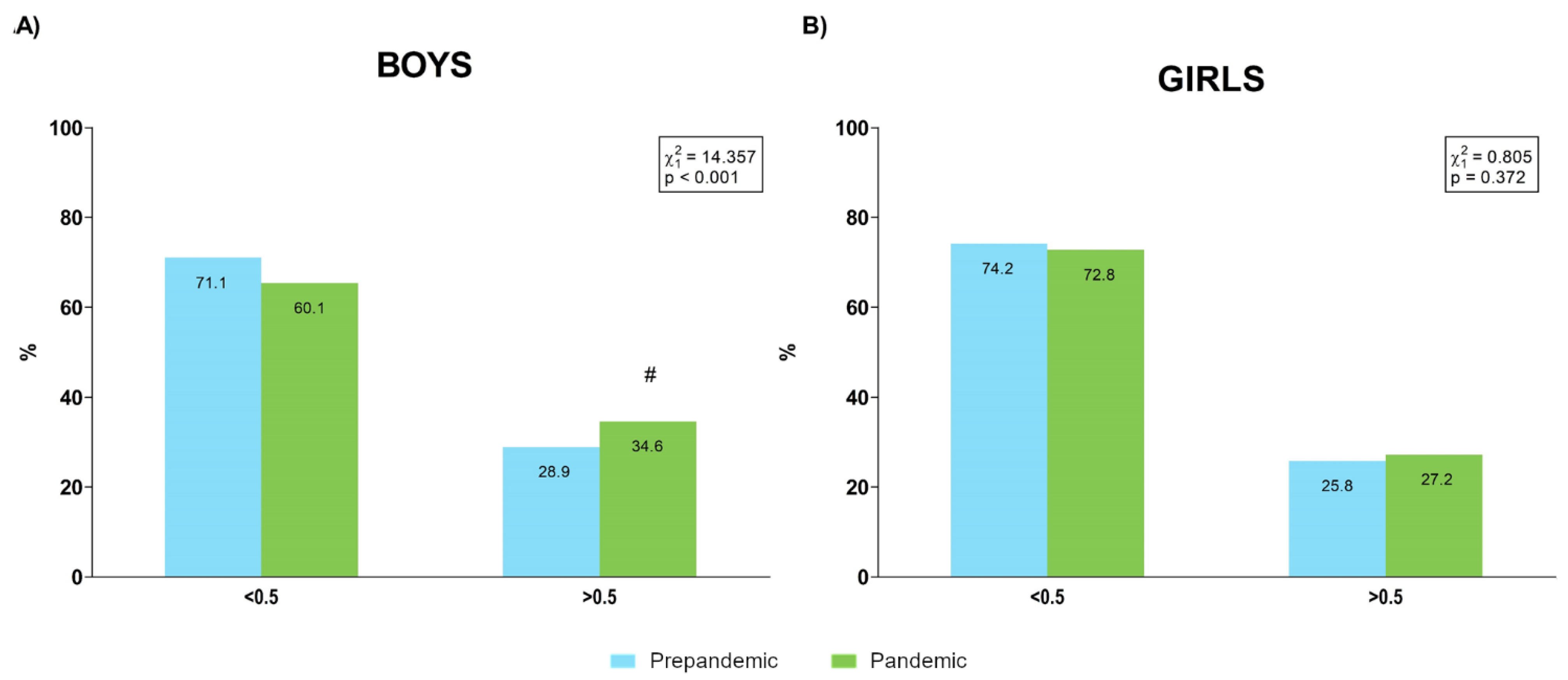
3.3. Prevalence of Body Composition and Fitness Categories
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Martinez, A.; Zhou, B.; Sophiea, M.K.; Bentham, J.; Paciorek, C.J.; Iurilli, M.L.; Carrillo-Larco, R.M.; Bennett, J.E.; Di Cesare, M.; Taddei, C.; et al. Height and body-mass index trajectories of school-aged children and adolescents from 1985 to 2019 in 200 countries and territories: A pooled analysis of 2181 population-based studies with 65 million participants. Lancet 2020, 396, 1511–1524. [Google Scholar] [CrossRef]
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S. Temporal trends in the cardiorespiratory fitness of children and adolescents representing 19 high-income and upper middle-income countries between 1981 and 2014. Br. J. Sports Med. 2019, 53, 478–486. [Google Scholar] [CrossRef] [Green Version]
- Laddu, D.R.; Parimi, N.; Stone, K.L.; Lapidus, J.; Hoffman, A.R.; Stefanick, M.L.; Langsetmo, L. Physical Activity Trajectories and Associated Changes in Physical Performance in Older Men: The MrOS Study. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1967–1973. [Google Scholar] [CrossRef]
- Sialino, L.D.; Schaap, L.A.; Van Oostrom, S.H.; Nooyens, A.C.J.; Picavet, H.S.J.; Twisk, J.W.R.; Verschuren, W.M.M.; Visser, M.; Wijnhoven, H.A.H. Sex differences in physical performance by age, educational level, ethnic groups and birth cohort: The Longitudinal Aging Study Amsterdam. PLoS ONE 2019, 14, e0226342. [Google Scholar] [CrossRef] [Green Version]
- Hoekstra, T.; Rojer, A.G.M.; van Schoor, N.M.; Maier, A.B.; Pijnappels, M. Distinct Trajectories of Individual Physical Performance Measures Across 9 Years in 60- to 70-Year-Old Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1951–1959. [Google Scholar] [CrossRef] [PubMed]
- Lamoureux, N.R.; Fitzgerald, J.S.; Norton, K.I.; Sabato, T.; Tremblay, M.S.; Tomkinson, G.R. Temporal Trends in the Cardiorespiratory Fitness of 2,525,827 Adults Between 1967 and 2016: A Systematic Review. Sports Med. 2019, 49, 41–55. [Google Scholar] [CrossRef]
- Dooley, F.L.; Kaster, T.; Fitzgerald, J.S.; Walch, T.J.; Annandale, M.; Ferrar, K.; Lang, J.J.; Smith, J.J.; Tomkinson, G.R. A Systematic Analysis of Temporal Trends in the Handgrip Strength of 2,216,320 Children and Adolescents Between 1967 and 2017. Sports Med. 2020, 50, 1129–1144. [Google Scholar] [CrossRef] [PubMed]
- Dufner, T.J.; Fitzgerald, J.S.; Lang, J.J.; Tomkinson, G.R. Temporal Trends in the Handgrip Strength of 2,592,714 Adults from 14 Countries Between 1960 and 2017: A Systematic Analysis. Sports Med. 2020, 50, 2175–2191. [Google Scholar] [CrossRef]
- Tomkinson, G.R.; Kaster, T.; Dooley, F.L.; Fitzgerald, J.S.; Annandale, M.; Ferrar, K.; Lang, J.J.; Smith, J.J. Temporal Trends in the Standing Broad Jump Performance of 10,940,801 Children and Adolescents Between 1960 and 2017. Sports Med. 2021, 51, 531–548. [Google Scholar] [CrossRef]
- Eberhardt, T.; Bös, K.; Niessner, C. The Fitness Barometer: A Best Practice Example for Monitoring Motor Performance With Pooled Data Collected From Practitioners. Front. Public Health 2021, 9, 720589. [Google Scholar] [CrossRef] [PubMed]
- Iglesias-Soler, E.; Rúa-Alonso, M.; Rial-Vázquez, J.; Lete-Lasa, J.R.; Clavel, I.; Giráldez-García, M.A.; Rico-Díaz, J.; Corral, M.R.-D.; Carballeira-Fernández, E.; Dopico-Calvo, X. Percentiles and Principal Component Analysis of Physical Fitness From a Big Sample of Children and Adolescents Aged 6–18 Years: The DAFIS Project. Front. Psychol. 2021, 12, 17. [Google Scholar] [CrossRef]
- Catucci, A.; Scognamiglio, U.; Rossi, L. Lifestyle Changes Related to Eating Habits, Physical Activity, and Weight Status During COVID-19 Quarantine in Italy and Some European Countries. Front. Nutr. 2021, 8, 718877. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Sánchez, E.; Ramírez-Vargas, G.; Avellaneda-López, Y.; Orellana-Pecino, J.I.; García-Marín, E.; Díaz-Jimenez, J. Eating Habits and Physical Activity of the Spanish Population during the COVID-19 Pandemic Period. Nutrients 2020, 12, 2826. [Google Scholar] [CrossRef] [PubMed]
- Carriedo, A.; Cecchini, J.A.; Fernandez-Rio, J.; Méndez-Giménez, A. COVID-19, Psychological Well-being and Physical Activity Levels in Older Adults During the Nationwide Lockdown in Spain. Am. J. Geriatr. Psychiatry 2020, 28, 1146–1155. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Coca, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef]
- García-Tascón, M.; Sahelices-Pinto, C.; Mendaña-Cuervo, C.; Magaz-González, A.M. The impact of the COVID-19 confinement on the habits of pa practice according to gender (Male/female): Spanish case. Int. J. Environ. Res. Public Health 2020, 17, 6961. [Google Scholar] [CrossRef]
- Martínez-de-Quel, Ó.; Suárez-Iglesias, D.; López-Flores, M.; Pérez, C.A. Physical activity, dietary habits and sleep quality before and during COVID-19 lockdown: A longitudinal study. Appetite 2021, 158, 105019. [Google Scholar] [CrossRef]
- Chen, L.; Li, J.; Xia, T.; Matthews, T.A.; Tseng, T.S.; Shi, L.; Zhang, D.; Chen, Z.; Han, X.; Li, Y.; et al. Changes of exercise, screen time, fast food consumption, alcohol, and cigarette smoking during the COVID-19 pandemic among adults in the United States. Nutrients 2021, 13, 3359. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; López-Núñez, M.I.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Choo, F.; Ho, R.; Ho, C.; Aparicio García, M.E. The Impact of the COVID-19 Pandemic on Physical and Mental Health in China and Spain: Cross-sectional Study. JMIR Form. Res. 2021, 5, e27818. [Google Scholar] [CrossRef]
- Tang, S.; Xiang, M.; Cheung, T.; Xiang, Y.-T. Mental health and its correlates among children and adolescents during COVID-19 school closure: The importance of parent-child discussion. J. Affect. Disord. 2021, 279, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, E.W.; Beyl, R.A.; Fearnbach, S.N.; Altazan, A.D.; Martin, C.K.; Redman, L.M. The Impact of COVID-19 Stay-At-Home Orders on Health Behaviors in Adults. Obesity 2021, 29, 438–445. [Google Scholar] [CrossRef]
- López-Bueno, R.; Calatayud, J.; Andersen, L.L.; Casaña, J.; Ezzatvar, Y.; Casajús, J.A.; López-Sánchez, G.F.; Smith, L. Cardiorespiratory fitness in adolescents before and after the COVID-19 confinement: A prospective cohort study. Eur. J. Pediatr. 2021, 180, 2287–2293. [Google Scholar] [CrossRef]
- Nobari, H.; Fashi, M.; Eskandari, A.; Villafaina, S.; Murillo-Garcia, Á.; Pérez-Gómez, J. Effect of COVID-19 on health-related quality of life in adolescents and children: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 4563. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.H.; Chen, Y.C.; Chen, W.Y.; Chen, C.Y.; Hsu, W.Y.; Chou, Y.; Chang, Y.H. Weight gain associated with COVID-19 lockdown in children and adolescents: A systematic review and meta-analysis. Nutrients 2021, 13, 3668. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child. Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.C.; Ramage, K.; Moore, S.A.; Riazi, N.; Tremblay, M.S.; Faulkner, G. Exploring the impact of COVID-19 on the movement behaviors of children and youth: A scoping review of evidence after the first year. J. Sport Health Sci. 2021, 10, 675–689. [Google Scholar] [CrossRef]
- Gao, Z.; Chen, S.; Huang, C.C.; Stodden, D.F.; Xiang, P. Investigating elementary school children’s daily physical activity and sedentary behaviours during weekdays. J. Sports Sci. 2017, 35, 99–104. [Google Scholar] [CrossRef]
- Saar, M.; Jürimäe, T. Sports participation outside school in total physical activity of children. Percept. Mot. Ski. 2007, 105, 559–562. [Google Scholar] [CrossRef] [PubMed]
- Rolland, B.; Haesebaert, F.; Zante, E.; Benyamina, A.; Haesebaert, J.; Franck, N. Global Changes and Factors of Increase in Caloric/Salty Food Intake, Screen Use, and Substance Use During the Early COVID-19 Containment Phase in the General Population in France: Survey Study. JMIR Public Health Surveill. 2020, 6, e19630. [Google Scholar] [CrossRef]
- Cole, T.J. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240. [Google Scholar] [CrossRef] [Green Version]
- Nevill, A.M.; Duncan, M.J.; Lahart, I.M.; Sandercock, G.R. Scaling waist girth for differences in body size reveals a new improved index associated with cardiometabolic risk. Scand. J. Med. Sci. Sports 2017, 27, 1470–1476. [Google Scholar] [CrossRef] [PubMed]
- Castro-Piñero, J.; Perez-Bey, A.; Cuenca-Garcia, M.; Cabanas-Sanchez, V.; Gómez-Martínez, S.; Veiga, O.L.; Marcos, A.; Ruiz, J.R.; Marcos, A.; Gomez-Martinez, S.; et al. Muscle Fitness Cut Points for Early Assessment of Cardiovascular Risk in Children and Adolescents. J. Pediatr. 2019, 206, 134–141.e3. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Cavero-Redondo, I.; Ortega, F.B.; Welk, G.J.; Andersen, L.B.; Martinez-Vizcaino, V. Cardiorespiratory fitness cut points to avoid cardiovascular disease risk in children and adolescents; what level of fitness should raise a red flag? A systematic review and meta-analysis. Br. J. Sports Med. 2016, 50, 1451–1458. [Google Scholar] [CrossRef] [PubMed]
- Karatzi, K.; Poulia, K.-A.; Papakonstantinou, E.; Zampelas, A. The Impact of Nutritional and Lifestyle Changes on Body Weight, Body Composition and Cardiometabolic Risk Factors in Children and Adolescents during the Pandemic of COVID-19: A Systematic Review. Children 2021, 8, 1130. [Google Scholar] [CrossRef]
- Chaffee, B.W.; Cheng, J.; Couch, E.T.; Hoeft, K.S.; Halpern-Felsher, B. Adolescents’ Substance Use and Physical Activity Before and During the COVID-19 Pandemic. JAMA Pediatr. 2021, 175, 715. [Google Scholar] [CrossRef] [PubMed]
- Hurter, L.; McNarry, M.; Stratton, G.; Mackintosh, K. Back to school after lockdown: The effect of COVID-19 restrictions on children’s device-based physical activity metrics. J. Sport Health Sci. 2022, 1–7. [Google Scholar] [CrossRef]
- Vogel, M.; Geserick, M.; Gausche, R.; Beger, C.; Poulain, T.; Meigen, C.; Körner, A.; Keller, E.; Kiess, W.; Pfäffle, R. Age- and weight group-specific weight gain patterns in children and adolescents during the 15 years before and during the COVID-19 pandemic. Int. J. Obes. 2022, 46, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Castro-Piñero, J.; Laurson, K.R.; Artero, E.G.; Ortega, F.B.; Labayen, I.; Ruperez, A.I.; Zaqout, M.; Manios, Y.; Vanhelst, J.; Marcos, A.; et al. Muscle strength field-based tests to identify European adolescents at risk of metabolic syndrome: The HELENA study. J. Sci. Med. Sport 2019, 22, 929–934. [Google Scholar] [CrossRef]
- Faigenbaum, A.D.; Rebullido, T.R.; MacDonald, J.P. Pediatric Inactivity Triad. Curr. Sports Med. Rep. 2018, 17, 45–47. [Google Scholar] [CrossRef]
- Poon, E.T.-C.; Zheng, C.; Wong, S.H.-S. Effect of Wearing Surgical Face Masks During Exercise: Does Intensity Matter? Front. Physiol. 2021, 12, 2151. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | ANOVA p-Value (η2) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Test | Sex | Sample | 6–8 Years | 8–10 Years | 10–12 Years | 12–14 Years | 14–16 Years | 16–18 Years | S | A | Sample | S × A | S × Sample | A × Sample | S × A × Sample |
| Waist Circumference (cm) | Boys | Pre | 59.77 ± 6.76 | 64.68 ± 8.99 | 69.04 ± 10.04 | 73.48 ± 11.51 | 76.66 ± 10.74 | 78.62 ± 10.51 | <0.001 (0.012) | <0.001 (0.129) | <0.001 (0.002) | <0.001 (0.006) | 0.012 (0.000398) | 0.128 (0.000537) | 0.092 (0.000594) |
| Post | 60.56 ± 7.57 | 66.21 ± 8.90 | 70.71 ± 10.23 | 75.01 ± 12.32 | 80.95 ± 11.34 | 81.14 ± 13.47 | |||||||||
| Girls | Pre | 59.10 ± 6.58 | 64.25 ± 8.58 | 67.48 ± 9.49 | 70.72 ± 10.18 | 71.85 ± 9.72 | 72.47 ± 9.61 | ||||||||
| Post | 60.52 ± 7.53 | 64.9 ± 10.06 | 67.00 ± 9.08 | 72.6 ± 10.67 | 72.91 ± 10.01 | 72.97 ± 8.83 | |||||||||
| Hip Circumference (cm) | Boys | Pre | 68.51 ± 6.11 | 74.86 ± 8.19 | 80.53 ± 8.76 | 86.28 ± 9.82 | 92.06 ± 9.69 | 95.60 ± 9.30 | 0.102 (0.000174) | <0.001 (0.288) | <0.001 (0.001) | <0.001 (0.002) | 0.223 (0.000097) | <0.001 (0.002) | 0.115 (0.00057) |
| Post | 68.63 ± 6.81 | 77.38 ± 8.20 | 84.29 ± 8.74 | 86.98 ± 11.44 | 94.97 ± 10.61 | 92.49 ± 10.92 | |||||||||
| Girls | Pre | 68.71 ± 6.28 | 75.21 ± 7.95 | 81.38 ± 9.59 | 88.04 ± 9.99 | 93.34 ± 9.38 | 95.12 ± 9.67 | ||||||||
| Post | 68.11 ± 7.22 | 77.74 ± 9.53 | 83.47 ± 10.07 | 90.72 ± 10.62 | 92.69 ± 10.56 | 92.80 ± 12.12 | |||||||||
| BMI (kg/m2) | Boys | Pre | 17.33 ± 2.74 | 18.85 ± 3.38 | 19.81 ± 3.61 | 21.15 ± 4.09 | 21.99 ± 4.11 | 22.93 ± 3.96 | 0.014 (0.000363) | <0.001 (0.095) | 0.002 (0.001) | 0.001 (0.001) | 0.440 (0.000036) | 0.651 (0.000200) | 0.117 (0.001) |
| Post | 17.63 ± 2.71 | 19.42 ± 3.64 | 20.18 ± 3.93 | 21.05 ± 4.42 | 22.58 ± 4.19 | 22.51 ± 4.36 | |||||||||
| Girls | Pre | 17.32 ± 2.60 | 18.77 ± 3.19 | 19.82 ± 3.79 | 21.42 ± 4.03 | 22.67 ± 4.07 | 22.99 ± 4.33 | ||||||||
| Post | 17.73 ± 2.96 | 19.08 ± 3.71 | 19.62 ± 3.66 | 22.05 ± 4.30 | 23.12 ± 4.42 | 23.56 ± 4.18 | |||||||||
| WHR | Boys | Pre | 0.88 ± 0.05 | 0.87 ± 0.06 | 0.86 ± 0.07 | 0.85 ± 0.07 | 0.83 ± 0.07 | 0.82 ± 0.07 | <0.001 (0.031) | <0.001 (0.049) | <0.001 (0.001) | <0.001 (0.014) | 0.057 (0.000237) | <0.001 (0.006) | 0.018 (0.001) |
| Post | 0.88 ± 0.07 | 0.85 ± 0.06 | 0.85 ± 0.07 | 0.86 ± 0.10 | 0.86 ± 0.08 | 0.86 ± 0.08 | |||||||||
| Girls | Pre | 0.87 ± 0.06 | 0.86 ± 0.06 | 0.83 ± 0.07 | 0.80 ± 0.07 | 0.77 ± 0.07 | 0.76 ± 0.06 | ||||||||
| Post | 0.89 ± 0.08 | 0.84 ± 0.08 | 0.81 ± 0.08 | 0.81 ± 0.10 | 0.78 ± 0.07 | 0.79 ± 0.07 | |||||||||
| WHtR | Boys | Pre | 0.48 ± 0.05 | 0.48 ± 0.06 | 0.47 ± 0.06 | 0.47 ± 0.07 | 0.45 ± 0.06 | 0.45 ± 0.06 | <0.001 (0.003) | <0.001 (0.015) | <0.001 (0.002) | <0.001 (0.002) | 0.008 (0.000449) | 0.322 (0.000369) | 0.194 (<0.001) |
| Post | 0.49 ± 0.05 | 0.49 ± 0.06 | 0.49 ± 0.06 | 0.48 ± 0.07 | 0.47 ± 0.06 | 0.47 ± 0.08 | |||||||||
| Girls | Pre | 0.48 ± 0.05 | 0.48 ± 0.06 | 0.46 ± 0.06 | 0.45 ± 0.06 | 0.45 ± 0.06 | 0.45 ± 0.06 | ||||||||
| Post | 0.49 ± 0.05 | 0.48 ± 0.07 | 0.46 ± 0.06 | 0.46 ± 0.06 | 0.45 ± 0.06 | 0.45 ± 0.05 | |||||||||
| Age Group | ANOVA p-Value (η2) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Test | Sex | Sample | 6–8 Years | 8–10 Years | 10–12 Years | 12–14 Years | 14–16 Years | 16–18 Years | S | A | Sample | S × A | S × Sample | A × Sample | S × A × Sample |
| Handgrip (kg) | Boys | Pre | 19.87 ± 4.48 | 26.65 ± 5.95 | 34.11 ± 7.86 | 45.99 ± 12.30 | 64.21 ± 15.20 | 74.16 ± 15.01 | <0.001 (0.060) | <0.001 (0.472) | <0.001 (0.002) | <0.00 (0.068) | 0.157 (0.0001) | 0.033 (0.001) | 0.200 (0.0001) |
| Post | 22.47 ± 4.14 | 28.33 ± 6.48 | 34.89 ± 7.44 | 45.05 ± 11.47 | 66.44 ± 17.78 | 74.12 ± 15.73 | |||||||||
| Girls | Pre | 18.43 ± 4.27 | 25.26 ± 5.61 | 33.39 ± 7.97 | 42.34 ± 9.01 | 47.95 ± 8.79 | 49.32 ± 9.06 | ||||||||
| Post | 20.53 ± 4.33 | 27.65 ± 5.87 | 33.88 ± 8.44 | 43.84 ± 9.02 | 49.69 ± 10.22 | 51.54 ± 8.58 | |||||||||
| SLJ (cm) | Boys | Pre | 107.81 ± 19.41 | 123.88 ± 21.35 | 139.91 ± 23.37 | 157.23 ± 26.95 | 182.10 ± 29.29 | 197.10 ± 29.87 | <0.001 (0.060) | <0.001 (0.261) | 0.187 (0.0001) | <0.001 (0.031) | 0.801 (0.0001) | 0.007 (0.001) | 0.455 (0.0001) |
| Post | 108.68 ± 19.69 | 124.70 ± 21.21 | 138.39 ± 25.62 | 154.60 ± 28.93 | 182.39 ± 31.10 | 193.55 ± 28.15 | |||||||||
| Girls | Pre | 100.09 ± 17.70 | 117.06 ± 19.47 | 133.46 ± 22.40 | 142.93 ± 23.21 | 148.23 ± 24.82 | 148.61 ± 24.78 | ||||||||
| Post | 99.57 ± 19.01 | 120.50 ± 24.37 | 129.86 ± 20.56 | 137.23 ± 25.34 | 150.05 ± 27.32 | 149.30 ± 25.59 | |||||||||
| Back-saver sit and reach (cm) | Boys | Pre | 24.21 ± 5.68 | 22.53 ± 5.99 | 22.07 ± 6.16 | 21.39 ± 6.37 | 23.56 ± 7.60 | 25.50 ± 7.89 | <0.001 (0.052) | <0.001 (0.016) | <0.001 (0.001) | <0.001 (0.005) | 0.176 (0.0001) | 0.032 (0.001) | 0.837 (0.0001) |
| Post | 25.49 ± 5.43 | 22.68 ± 6.39 | 22.84 ± 6.74 | 21.79 ± 7.63 | 25.28 ± 9.17 | 24.89 ± 9.10 | |||||||||
| Girls | Pre | 27.21 ± 5.77 | 26.53 ± 6.45 | 26.42 ± 7.00 | 28.11 ± 7.39 | 30.51 ± 8.09 | 30.74 ± 7.73 | ||||||||
| Post | 28.19 ± 4.92 | 27.44 ± 6.87 | 27.97 ± 7.09 | 28.45 ± 7.68 | 32.65 ± 8.80 | 31.45 ± 8.43 | |||||||||
| 4 × 10 m SRT (s) | Boys | Pre | 15.60 ± 2.05 | 14.46 ± 1.83 | 13.51 ± 1.53 | 12.50 ± 1.43 | 11.68 ± 1.31 | 11.26 ± 1.84 | <0.001 (0.028) | <0.001 (0.206) | 0.023 (0.0001) | <0.001 (0.009) | 0.119 (0.0001) | <0.001 (0.005) | <0.001 (0.002) |
| Post | 16.18 ± 3.02 | 14.29 ± 2.08 | 13.39 ± 1.70 | 12.97 ± 1.73 | 11.44 ± 2.09 | 10.94 ± 1.63 | |||||||||
| Girls | Pre | 16.19 ± 1.85 | 14.89 ± 1.63 | 13.85 ± 1.54 | 13.14 ± 1.35 | 12.94 ± 1.38 | 12.91 ± 1.42 | ||||||||
| Post | 16.54 ± 2.19 | 14.34 ± 1.65 | 14.38 ± 1.99 | 13.78 ± 1.45 | 13.31 ± 2.10 | 12.53 ± 1.95 | |||||||||
| Bent-Arm Hang (s) | Boys | Pre | 6.06 ± 5.81 | 8.75 ± 8.65 | 11.09 ± 10.81 | 13.41 ± 13.41 | 23.44 ± 17.60 | 28.40 ± 19.05 | <0.001 (0.028) | <0.001 (0.065) | 0.868 (0.0001) | <0.001 (0.023) | 0.648 (0.0001) | 0.009 (0.0001) | 0.094 (0.001) |
| Post | 5.54 ± 5.42 | 8.80 ± 8.41 | 8.34 ± 10.03 | 13.50 ± 12.76 | 27.58 ± 25.18 | 29.99 ± 20.34 | |||||||||
| Girls | Pre | 5.26 ± 5.10 | 6.57 ± 7.06 | 7.40 ± 8.09 | 9.22 ± 10.20 | 10.29 ± 11.84 | 11.78 ± 13.25 | ||||||||
| Post | 3.81 ± 3.38 | 8.46 ± 7.94 | 7.25 ± 8.36 | 6.39 ± 6.53 | 10.78 ± 13.46 | 13.15 ± 15.47 | |||||||||
| 20 m SRT (stages) | Boys | Pre | 4.26 ± 2.34 | 5.28 ± 2.62 | 6.58 ± 2.89 | 7.21 ± 3.00 | <0.001 (0.061) | <0.001 (0.029) | 0.951 (0.0001) | <0.001 (0.010) | 0.960 (0.0001) | <0.001 (0.003) | 0.302 (0.0001) | ||
| Post | 4.84 ± 3.23 | 4.68 ± 2.51 | 6.73 ± 3.07 | 7.07 ± 3.20 | |||||||||||
| Girls | Pre | 3.35 ± 1.88 | 3.77 ± 1.90 | 3.88 ± 1.90 | 4.16 ± 1.98 | ||||||||||
| Post | 3.55 ± 2.44 | 3.28 ± 1.80 | 3.89 ± 2.10 | 4.42 ± 2.37 | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rúa-Alonso, M.; Rial-Vázquez, J.; Nine, I.; Lete-Lasa, J.R.; Clavel, I.; Giráldez-García, M.A.; Rodríguez-Corral, M.; Dopico-Calvo, X.; Iglesias-Soler, E. Comparison of Physical Fitness Profiles Obtained before and during COVID-19 Pandemic in Two Independent Large Samples of Children and Adolescents: DAFIS Project. Int. J. Environ. Res. Public Health 2022, 19, 3963. https://doi.org/10.3390/ijerph19073963
Rúa-Alonso M, Rial-Vázquez J, Nine I, Lete-Lasa JR, Clavel I, Giráldez-García MA, Rodríguez-Corral M, Dopico-Calvo X, Iglesias-Soler E. Comparison of Physical Fitness Profiles Obtained before and during COVID-19 Pandemic in Two Independent Large Samples of Children and Adolescents: DAFIS Project. International Journal of Environmental Research and Public Health. 2022; 19(7):3963. https://doi.org/10.3390/ijerph19073963
Chicago/Turabian StyleRúa-Alonso, María, Jessica Rial-Vázquez, Iván Nine, Jose Ramón Lete-Lasa, Iván Clavel, Manuel A. Giráldez-García, Miguel Rodríguez-Corral, Xurxo Dopico-Calvo, and Eliseo Iglesias-Soler. 2022. "Comparison of Physical Fitness Profiles Obtained before and during COVID-19 Pandemic in Two Independent Large Samples of Children and Adolescents: DAFIS Project" International Journal of Environmental Research and Public Health 19, no. 7: 3963. https://doi.org/10.3390/ijerph19073963