
Chronic Pain and Work Conditions of Hotel Housekeepers: A Descriptive Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Used Methods and Scales
2.2. Data Collection
2.3. Statistical Analysis
3. Results
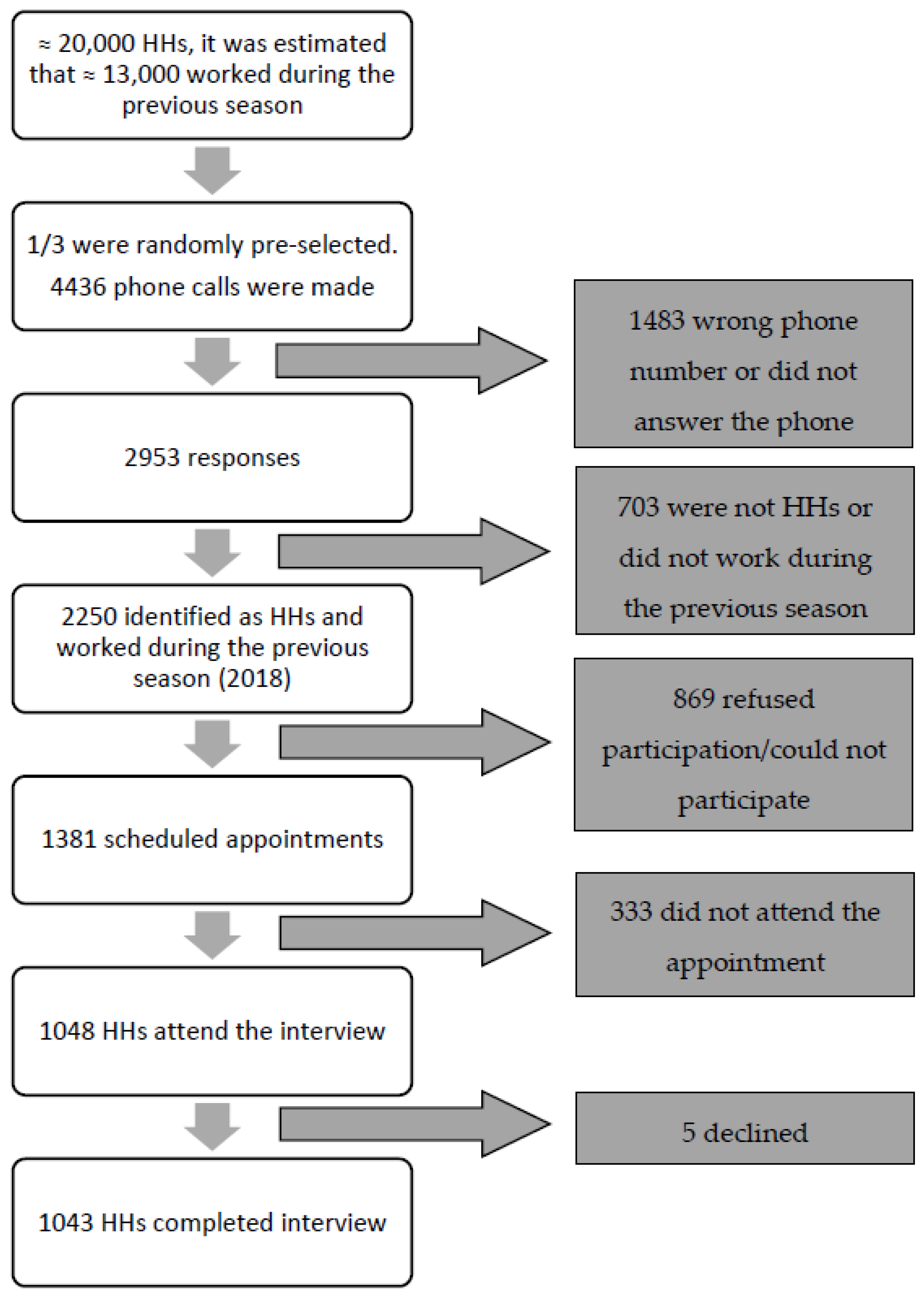
3.1. Participants
3.2. Personal and Workplace Characteristics
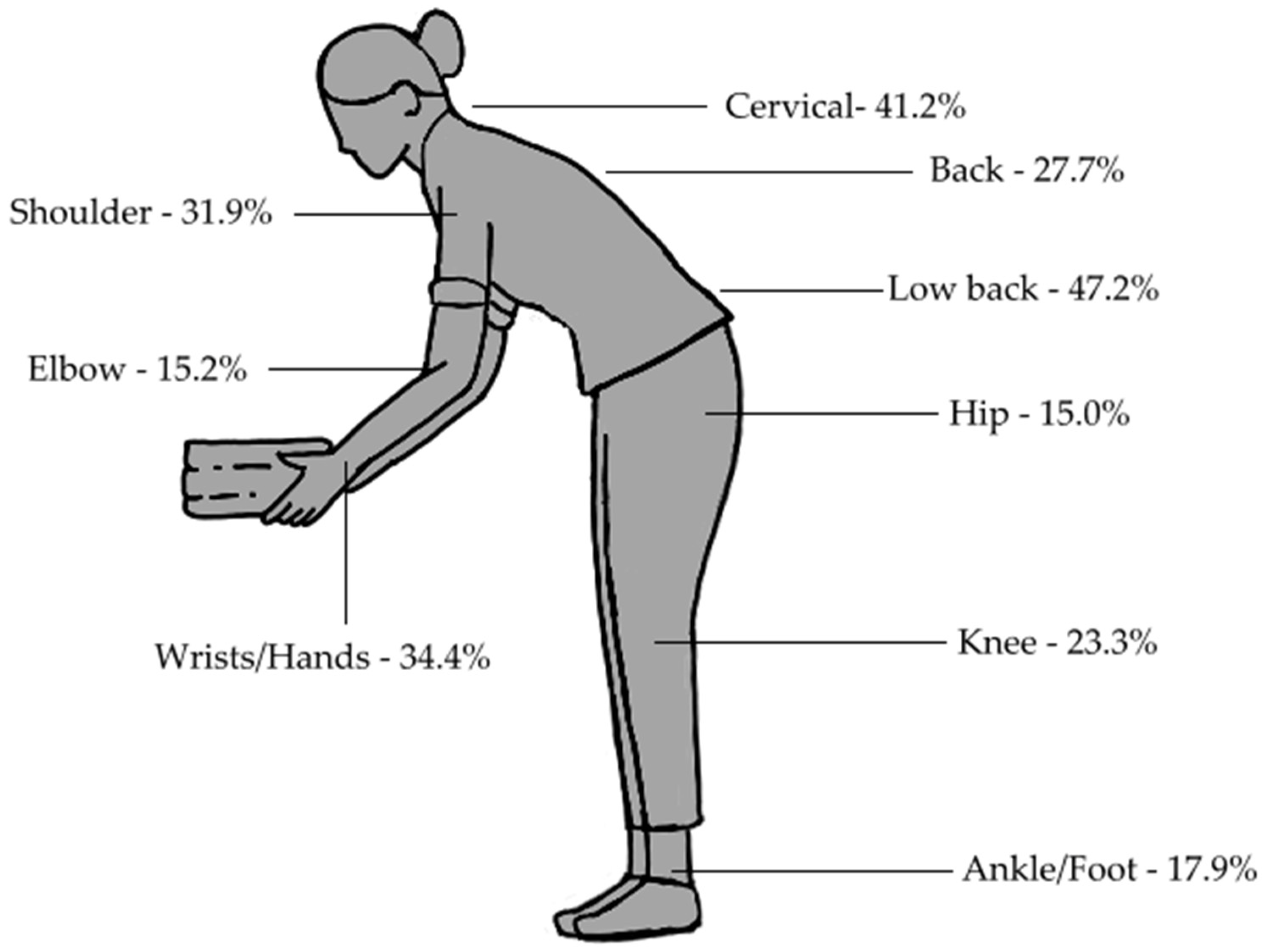
3.3. Musculoskeletal Pain
3.4. Use of Medicines
3.5. Occupational Risk Factors and Workload
3.6. Physical Activity, BMI and Perceived Health Status
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Age Subgroups | ||||||||||||||||
| <35 Years | 35–44 Years | 45–54 Years | ≥55 Years | Total | ||||||||||||
| n | % | 95% CI | n | % | 95% CI | n | % | 95% CI | n | % | 95% CI | n | % | 95% CI | ||
| Never | Neck | 47 | 22.6 | 17.1–28.1 | 61 | 17.5 | 13.7–21.9 | 61 | 21.1 | 16.5–26.3 | 38 | 22.1 | 16.1–29.0 | 207 | 20.4 | 17.9–22.9 |
| Back | 69 | 33.8 | 27.7–40.6 | 106 | 30.7 | 25.9–35.9 | 95 | 33.3 | 27.9–39.1 | 53 | 30.6 | 23.9–38.1 | 323 | 32.1 | 29.3–35.0 | |
| Low back | 28 | 13.4 | 9.0–18.7 | 32 | 9.2 | 6.3–12.7 | 39 | 13.6 | 9.8–18.1 | 21 | 12.1 | 7.7–17.9 | 120 | 11.8 | 9.9–13.9 | |
| Shoulders | 74 | 36.1 | 29.3–42.9 | 91 | 26.3 | 21.7–31.3 | 76 | 26.3 | 21.3–31.8 | 34 | 19.9 | 14.2–26.7 | 275 | 27.2 | 24.4–30.0 | |
| Elbows | 154 | 77.0 | 70.7–82.3 | 214 | 62.9 | 57.7–67.9 | 155 | 54.6 | 48.8–60.3 | 93 | 54.7 | 47.2–62.0 | 616 | 62.0 | 58.9–64.9 | |
| Wrists/Hands | 51 | 25.0 | 19.1–31.4 | 75 | 21.7 | 17.4–26.4 | 68 | 23.4 | 18.7–28.7 | 36 | 20.8 | 15–27.6 | 230 | 22.7 | 20.1–25.4 | |
| Hip | 132 | 65.0 | 58.2–71.2 | 205 | 60.3 | 55–65.3 | 178 | 62.7 | 56.9–68.1 | 104 | 61.2 | 53.7–68.2 | 619 | 62.1 | 59.0–65.0 | |
| Knees | 105 | 52.0 | 45.1–58.8 | 159 | 46.2 | 41.0–51.5 | 100 | 35.0 | 29.7–40.1 | 60 | 34.7 | 28–42.0 | 424 | 42.2 | 39.2–45.3 | |
| Ankle/Foot | 100 | 49.5 | 42.7–56.3 | 160 | 47.2 | 41.9–52.5 | 146 | 51.0 | 45.3–56.8 | 95 | 55.2 | 47.8–62.5 | 501 | 50.2 | 47.1–53.2 | |
| Occasionally | Neck | 61 | 29.3 | 23.6–35.8 | 94 | 27 | 22.4–32.0 | 64 | 22.1 | 17.5–27.4 | 29 | 16.9 | 11.6–23.3 | 248 | 24.4 | 21.9–27.1 |
| Back | 34 | 16.7 | 11.8–22.4 | 68 | 19.7 | 15.6–24.3 | 56 | 19.6 | 15.2–24.7 | 37 | 21.4 | 15.5–28.2 | 195 | 19.4 | 16.9–21.9 | |
| Low back | 41 | 19.6 | 14.4–25.5 | 74 | 21.2 | 17.0–25.9 | 54 | 18.8 | 14.5–23.8 | 35 | 20.2 | 14.5–27.0 | 204 | 20.0 | 17.6–22.6 | |
| Shoulders | 48 | 23.4 | 17.7–29.7 | 66 | 19.1 | 15.1–23.6 | 44 | 15.2 | 11.3–19.9 | 32 | 18.7 | 13.2–25.4 | 190 | 18.8 | 16.4–21.3 | |
| Elbows | 16 | 8.0 | 5.0–12.6 | 34 | 10 | 7.2–13.6 | 40 | 14.1 | 10.5–18.6 | 23 | 13.5 | 9.2–19.5 | 113 | 11.4 | 9.5–13.5 | |
| Wrists/Hands | 48 | 23.5 | 17.8–29.8 | 50 | 14.5 | 10.9–18.6 | 38 | 13.1 | 9.4–17.5 | 31 | 17.9 | 12.5–24.4 | 167 | 16.5 | 11.3–22.7 | |
| Hip | 36 | 17.7 | 13.1–23.6 | 56 | 16.5 | 12.9–20.8 | 32 | 11.3 | 8.1–15.5 | 25 | 14.7 | 10.2–20.8 | 149 | 14.9 | 12.9–17.3 | |
| Knees | 45 | 22.3 | 17.1–28.5 | 76 | 22.1 | 18.0–26.8 | 73 | 25.5 | 20.8–30.9 | 43 | 24.9 | 19–31.8 | 237 | 23.6 | 21.1–26.3 | |
| Ankle/Foot | 43 | 21.3 | 16.2–27.4 | 64 | 18.9 | 15.1–23.4 | 43 | 15.0 | 11.4–19.6 | 24 | 14.0 | 9.6–19.9 | 174 | 17.4 | 15.2–19.9 | |
| Percentages (%) are relative to age groups. | ||||||||||||||||
| Age Subgroups | ||||||||||||||||
| <35 years | 35–44 years | 45–54 years | ≥55 years | Total | ||||||||||||
| n | % | 95% CI | n | % | 95% CI | n | % | 95% CI | n | % | 95% CI | n | % | 95% CI | ||
| Often | Neck | 74 | 35.6 | 28.9–42.3 | 124 | 35.6 | 30.6–40.9 | 88 | 30.4 | 25.2–36.1 | 56 | 32.6 | 25.6–40.1 | 342 | 33.6 | 30.7–36.6 |
| Back | 71 | 34.8 | 28.1–41.6 | 111 | 32.2 | 27.3–37.3 | 84 | 29.5 | 24.2–35.1 | 44 | 25.4 | 19.1–32.6 | 310 | 30.8 | 27.9–33.7 | |
| Low back | 95 | 45.5 | 38.9–52.2 | 152 | 43.6 | 38.2–48.9 | 105 | 36.6 | 31.0–42.4 | 50 | 28.9 | 22.2–36.3 | 402 | 39.5 | 36.5–42.5 | |
| Shoulders | 55 | 26.8 | 21.2–33.3 | 132 | 38.2 | 33.0–43.5 | 104 | 36.0 | 30.4–41.8 | 54 | 31.6 | 24.7–39.1 | 345 | 34.1 | 31.3–37.1 | |
| Elbows | 24 | 12.0 | 8.2–17.2 | 64 | 18.8 | 15.0–23.3 | 50 | 17.6 | 13.6–22.5 | 32 | 18.8 | 13.7–25.4 | 170 | 17.1 | 14.9–19.6 | |
| Wrists/Hands | 75 | 36.8 | 30.5–43.6 | 139 | 40.2 | 34.9–45.5 | 109 | 37.6 | 32.0–43.4 | 53 | 30.6 | 23.9–38.1 | 376 | 37.1 | 34.2–40.1 | |
| Hip | 26 | 12.8 | 8.9–18.1 | 54 | 15.9 | 12.4–20.1 | 43 | 15.1 | 11.4–19.8 | 18 | 10.6 | 6.8–16.1 | 141 | 14.1 | 12.1–16.4 | |
| Knees | 42 | 20.8 | 15.8–26.9 | 71 | 20.6 | 16.7–25.2 | 70 | 24.5 | 19.9–29.8 | 33 | 19.1 | 13.9–25.6 | 216 | 21.5 | 19.1–24.1 | |
| Ankle/Foot | 43 | 21.3 | 16.2–27.4 | 80 | 23.6 | 19.4–28.4 | 65 | 22.7 | 18.3–27.9 | 29 | 16.9 | 12.0–23.2 | 217 | 21.7 | 19.3–24.4 | |
| Chronic | Neck | 26 | 12.5 | 8.3–17.7 | 69 | 19.8 | 15.8–24.4 | 76 | 26.3 | 21.3–31.8 | 49 | 28.5 | 21.9–35.9 | 220 | 21.6 | 19.1–24.3 |
| Back | 30 | 14.7 | 10.1–20.2 | 60 | 17.4 | 13.5–21.8 | 50 | 17.5 | 13.3–22.5 | 39 | 22.5 | 16.5–29.5 | 179 | 17.8 | 15.4–20.2 | |
| Low back | 45 | 21.5 | 16.1–27.6 | 91 | 26.1 | 21.5–31.0 | 89 | 31.0 | 25.7–36.7 | 67 | 38.7 | 31.4–46.4 | 292 | 28.7 | 25.9–31.5 | |
| Shoulders | 28 | 13.7 | 9.2–19 | 57 | 16.5 | 12.7–20.8 | 65 | 22.5 | 17.8–27.7 | 51 | 29.8 | 24.4–37.3 | 201 | 19.9 | 17.4–22.4 | |
| Elbows | 6 | 3.0 | 1.4–6.4 | 28 | 8.2 | 5.8–11.6 | 39 | 13.7 | 10.2–18.2 | 22 | 12.9 | 8.7–18.8 | 95 | 9.6 | 7.9–11.5 | |
| Wrists/Hands | 30 | 14.7 | 10.1–20.2 | 82 | 23.7 | 19.3–28.5 | 75 | 25.9 | 20.9–31.3 | 53 | 30.6 | 23.9–38.1 | 240 | 23.7 | 21.1–26.4 | |
| Hip | 9 | 4.4 | 2.3–8.2 | 25 | 7.4 | 5.0–10.6 | 31 | 10.9 | 7.8–15.1 | 23 | 13.5 | 9.2–19.5 | 88 | 8.8 | 7.2–10.7 | |
| Knees | 10 | 5.0 | 2.7–8.9 | 38 | 11 | 8.2–14.8 | 43 | 15.0 | 11.4–19.6 | 37 | 21.4 | 15.9–28.1 | 128 | 12.7 | 10.8–14.9 | |
| Ankle/Foot | 16 | 7.9 | 4.9–12.5 | 35 | 10.3 | 7.5–14.0 | 32 | 11.2 | 8.0–15.4 | 24 | 14.0 | 9.6–19.9 | 107 | 10.7 | 8.9–12.8 | |
| Percentages (%) are relative to age groups. | ||||||||||||||||
References
- Fingerhut, M.; Nelson, D.I.; Driscoll, T.; Concha-Barrientos, M.; Steenland, K.; Punnett, L.; Prüss-Ustün, A.; Leigh, J.; Corvalan, C.; Eijkemans, G.; et al. The contribution of occupational risks to the global burden of disease: Summary and next steps. Med. Lav. 2006, 97, 313–321. [Google Scholar] [PubMed]
- Buchanan, S.; Vossenas, P.; Krause, N.; Moriarty, J.; Frumin, E.; Shimek, J.A.M.; Mirer, F.; Orris, P.; Punnett, L. Occupational injury disparities in the US hotel industry. Am. J. Ind. Med. 2010, 53, 116–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdol Rahman, M.N.; Muhamad Jaffar, M.S.; Hassan, M.F.; Ngali, M.Z.; Pauline, O. Exposure level of ergonomic risk factors in hotel industries. IOP Conf Ser Mater Sci Eng. 2017, 226, 012018. [Google Scholar] [CrossRef]
- Abdol Rahman, M.N.; Muhamad Jaffar, M.S. Musculoskeletal Symptoms and Ergonomic Hazards Among Room Attendants in Hotel Industries. Malays. J. Hum. Factors Ergon. 2017, 1, 25–34. [Google Scholar]
- Krause, N.; Scherzer, T.; Rugulies, R. Physical workload, work intensification, and prevalence of pain in low wage workers: Results from a participatory research project with hotel room cleaners in Las Vegas. Am. J. Ind. Med. 2005, 48, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Lee, J.J.; Mun, H.J.; Lee, K.J. The Relationship between Musculoskeletal Symptoms and Work-related Risk Factors in Hotel Workers. Ann. Occup. Environ. Med. 2013, 25, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, I.; Cañada, E. Confronting job precarity in Spanish tourism: The rise of the hotel housekeepers. Glob. Labour. Column. 2017, 284, 1–3. [Google Scholar]
- Oxenbridge, S.; Moensted, M.L. The relationship between payment systems, work intensification and health and safety outcomes: A study of hotel room attendants. Policy Pract. Health Saf. 2011, 9, 7–26. [Google Scholar] [CrossRef]
- Hsieh, Y.C.; Apostolopoulos, Y.; Sönmez, S. The world at work: Hotel cleaners. Occup. Environ. Med. 2013, 70, 360–364. [Google Scholar] [CrossRef] [Green Version]
- Fontani, S.; Mercuri, I.; Salicco, R.; Silvia Veratti, L.S. Manual handling of loads in the hotel trade: The experience of the ASL (Local Health Unit) Milan. Med. Lav. 2010, 101, 437–445. [Google Scholar]
- European Agency for Safety and Health at Work (EU-OSHA). Protecting workers in hotels, restaurants and catering. Protecting workers in hotels, restaurants and catering. 2008. Available online: https://osha.europa.eu/en/publications/report-protecting-workers-hotels-restaurants-and-catering (accessed on 10 November 2021).
- Burdorf, A.; van der Beek, A.J. In musculoskeletal epidemiology are we asking the unanswerable in questionnaires on physical load? Scand. J. Work Environ. Health 1999, 25, 81–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EU-OSHA. European Agency for Safety and Health at Work. Musculoskeletal Disorders—Safety and Health at Work—EU-OSHA. Available online: https://osha.europa.eu/en/themes/musculoskeletal-disorders (accessed on 4 November 2021).
- Niño Lopez, M.A. Alteraciones musculo-esqueléticas de las camareras de piso. Mujeres Y Salud 2002, 9, 5–8. [Google Scholar]
- European Agency for Safety and Helath at Work. EU-OSHA. The Occupational Safety and Health of Cleaning Workers. European Risk Observatory. 2009. Available online: https://osha.europa.eu/en/publications/occupational-safety-and-health-cleaning-workers/view (accessed on 4 November 2021).
- Govern de les Illes Baleares. Estudio del impacto económico del Turismo sobre la economía y el empleo de las Islas Baleares. Impactur 2014. Impactur. 2015. Available online: http://www.exceltur.org/wp-content/uploads/2015/10/IMPACTUR-Baleares-2014-informe-completo.pdf (accessed on 10 November 2021).
- IBESTAT. Afiliaciones a la Seguridad Social del Sector Turístico [Internet]. [cited 2021 November 4]. Available online: https://ibestat.caib.es/ibestat/estadistiques/757266f3-2b85-473b-b83a-7eb0d0aa6729/3485c5b2-a2d8-4558-93e2-43f065e00c6a/es/I302039_TU01.px (accessed on 4 November 2021).
- Campbell, M.; Fitzpatrick, R.; Haines, A.; Kinmonth, A.L.; Sandercock, P.; Spiegelhalter, D.; Tyrer, P. Framework for design and evaluation of complex interventions to improve health. BMJ 2000, 321, 694–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Instituto Nacional de Seguridad e Higiene en el Trabajo. Manual para la Evaluación y Prevención de Riesgos Ergonómicos y Psicosociales en PYME. Madrid. 2003. Available online: https://www.insst.es/documentacion/catalogo-de-publicaciones/manual-para-la-evaluacion-y-prevencion-de-riesgos-ergonomicos-y-psicosociales-en-pyme (accessed on 4 November 2021).
- Martínez, M.M.; Alvarado Muñoz, R. Validación del Cuestionario Nórdico Estandarizado de Síntomas Musculoesqueléticos para la población trabajadora chilena, adicionando una escala de dolor. Rev. Salud Pública. 2017, 21, 43. [Google Scholar] [CrossRef] [Green Version]
- Puig-Ribera, A.; Martín-Cantera, C.; Puigdomenech, E.; Real, J.; Romaguera, M.; Magdalena-Belio, J.F.; Recio-Rodríguez, J.I.; Rodriguez-Martin, B.; Arietaleanizbeaskoa, M.S.; Repiso-Gento, I.; et al. Screening physical activity in family practice: Validity of the Spanish version of a brief physical activity questionnaire. PLoS ONE 2015, 10, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad C y, B.S. Encuesta Nacional de Salud de España 2017. 2018. Available online: https://www.sanidad.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2017.htm (accessed on 28 November 2020).
- Frumin, E.; Moriarty, J.; Vossenas, P.; Halpin, J.; Orris, P.; Krause, N.; Punnett, L. Workload-Related Musculoskeletal Disorders among Hotel Housekeepers: Employer Records Reveal a Growing National Problem. Public Health 2006. Available online: https://www.researchgate.net/publication/237722666_Workload-Related_Musculoskeletal_Disorders_among_Hotel_Housekeepers_Employer_Records_Reveal_a_Growing_National_Problem (accessed on 13 February 2022).
- Scherzer, T.; Rugulies, R.; Krause, N. Work-related pain and injury and barriers to workers’ compensation among Las Vegas hotel room cleaners. Am. J. Public Health 2005, 95, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Wami, S.D.; Abere, G.; Dessie, A.; Getachew, D. Work-related risk factors and the prevalence of low back pain among low wage workers: Results from a cross-sectional study. BMC Public Health 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wami, S.D.; Dessie, A.; Chercos, D.H. The impact of work-related risk factors on the development of neck and upper limb pain among low wage hotel housekeepers in Gondar town, Northwest Ethiopia: Institution-based cross-sectional study. Environ. Health Prev. Med. 2019, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Roquelaure, Y.; Ha, C.; Rouillon, C.; Fouquet, N.; Leclerc, A.; Descatha, A.; Touranchet, A.; Goldberg, M.; Imbernon, E. Risk factors for upper-extremity musculoskeletal disorders in the working population. Arthritis Care Res. 2009, 61, 1425–1434. [Google Scholar] [CrossRef] [Green Version]
- Rosemberg, M.A.S.; Li, Y.; McConnell, D.S.; McCullagh, M.C.; Seng, J.S. Stressors, allostatic load, and health outcomes among women hotel housekeepers: A pilot study. J. Occup. Environ. Hyg. 2019, 16, 206–217. [Google Scholar] [CrossRef] [PubMed]
- Parmar, S.; Dalal, P. A Study of Musculoskeletal Disorder Among Housekeeping Staff in Hotel Industry. Int. J. Home Sci. 2017, 3, 83–85. [Google Scholar]
- Harris-Adamson, C.; Lam, E.; Fathallah, F.; Tong, A.D.; Hill, S.; Smith, A. The ergonomic impact of a mattress lift tool and bottom sheet type on hotel room cleaners while making beds. Appl. Ergon. 2019, 81, 102880. [Google Scholar] [CrossRef] [PubMed]
- CCOHS-Canadian Centre for Occupational Health & Safety. Hotel Housekeeping. 2018. Available online: http://www.ccohs.ca/oshanswers/occup_workplace/hotel_housekeeping.html (accessed on 4 November 2021).
- Hsieh, Y.C.; Apostolopoulos, Y.; Sönmez, S. Work Conditions and Health and Well-Being of Latina Hotel Housekeepers. J. Immigr. Minor Health 2016, 18, 568–581. [Google Scholar] [CrossRef] [PubMed]
- Chela-Alvarez, X.; Bulilete, O.; García-Buades, M.E.; Ferrer-Perez, V.A.; Llobera-Canaves, J. Perceived Factors of Stress and Its Outcomes among Hotel Housekeepers in the Balearic Islands: A Qualitative Approach from a Gender Perspective. Int. J. Environ. Res. Public Health 2020, 18, 52. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.C.J.; Sönmez, S.; Apostolopoulos, Y.; Lemke, M.K. Perceived workplace mistreatment: Case of Latina hotel housekeepers. Work 2017, 56, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Korshøj, M.; Birk Jørgensen, M.; Lidegaard, M.; Mortensen, O.S.; Krustrup, P.; Holtermann, A.; Søgaard, K. Decrease in musculoskeletal pain after 4 and 12 months of an aerobic exercise intervention: A worksite RCT among cleaners. Scand. J. Public Health 2018, 46, 846–853. [Google Scholar] [CrossRef] [PubMed]


| Variables | Total Sample (n = 1043) | n | % | |
|---|---|---|---|---|
| Age in years (n = 1036) | Mean (SD) | 43.3 (10.1) | ||
| Groups | ≤35 | 217 | 20.9 | |
| 35 to 44 | 354 | 34.1 | ||
| 45 to 54 | 293 | 28.3 | ||
| ≥55 | 173 | 16.7 | ||
| Nationality (n = 1043) | Spanish | 563 | 54.0 | |
| Dual nationality | 182 | 17.4 | ||
| Foreign | 298 | 28.6 | ||
| Educational level (n = 1041) | Unfinished primary | 34 | 3.3 | |
| Primary education completed | 177 | 17.0 | ||
| Secondary education (first cycle) | 414 | 39.8 | ||
| Secondary education (second cycle) | 356 | 34.2 | ||
| University degree | 60 | 5.8 | ||
| Workplace characteristics | ||||
| Years worked as HH (n = 1019) | Mean (SD) | 10.7 (9.1) | ||
| Groups | <10 years | 562 | 55.2 | |
| 10–20 years | 325 | 31.9 | ||
| >20 years | 132 | 13.0 | ||
| Type of contract (n = 1035) | Permanent | 63 | 6.2 | |
| Recurring fixed-term | 551 | 54.2 | ||
| Temporary | 402 | 39.6 | ||
| Workplace (n = 1116) * | Hotel | 689 | 66.0 | |
| Apartment (tourist apartment, hotel apartment…) | 358 | 34.4 | ||
| Other (agritourism, bed and breakfast, rural accommodation…) | 66 | 6.3 | ||
| Star rating (stars/keys) (n = 1025) ** | None, 1, 2 or 3 stars/keys | 283/67 | 29.5/89.3 | |
| 4 stars/4 keys | 574/5 | 59.8/6.7 | ||
| 5 stars/4 keys superior | 103/3 | 10.7/4.0 | ||
| Hours of work/week (n = 1042) | Mean (SD) | 40.7 (5.6) | ||
| Groups | <40 h/week | 68 | 6.5 | |
| 40 h/week | 756 | 72.5 | ||
| 41–50 h/week | 196 | 18.8 | ||
| >50 h/week | 22 | 2.1 | ||
| Total | ||||
|---|---|---|---|---|
| Years Worked | Region of Chronic Pain | n | % | 95% CI |
| <10 years worked | Low back | 130 | 23.9 | 20.4–27.7 |
| Wrists/Hands | 98 | 18.1 | 1.9–21.6 | |
| Neck | 96 | 17.6 | 14.5–21.1 | |
| Shoulders | 86 | 15.9 | 12.9–19.4 | |
| Back | 85 | 18.9 | 12.9–19.2 | |
| 10–20 years worked | Low back | 96 | 29.9 | 24.9–35.2 |
| Wrists/Hands | 86 | 27 | 22.2–32.3 | |
| Neck | 76 | 23.7 | 19.1–28.7 | |
| Shoulders | 70 | 21.8 | 17.4–26.7 | |
| Back | 55 | 17.2 | 13.3–21.8 | |
| >20 years worked | Low back | 59 | 45 | 36.3–53.9 |
| Wrists/Hands | 50 | 38.2 | 29.8–47.1 | |
| Neck | 44 | 33.8 | 25.8–42.7 | |
| Shoulders | 40 | 30.8 | 22.9–39.5 | |
| Back | 36 | 27.5 | 20–35.9 | |
| Variables | Groups | Chronic Pain n (%) | p-Value |
|---|---|---|---|
| Age | <35 years | 77 (35.6) | 0.000 |
| 35–44 years | 175 (49.4) | ||
| 45–54 years | 157 (53.6) | ||
| ≥55 years | 119 (68.8) | ||
| Years worked as HH | 0–4 years | 117 (36.3) | 0.000 |
| 5–9 years | 130 (54.2) | ||
| 10–14 years | 87 (50.3) | ||
| 15–19 years | 66 (59.5) | ||
| ≥20 years | 120 (69.4) | ||
| Number of beds/day | 0–30 beds/day | 97 (36.9) | 0.000 |
| 31–44 beds/day | 137 (48.6) | ||
| 45–60 beds/day | 163 (56.6) | ||
| >61 beds/day | 135 (65.9) | ||
| Type of contract | Permanent | 26 (41.3) | 0.002 |
| Recurring fixed term | 308 (55.9) | ||
| Temporary | 184 (45.8) | ||
| Number of hours worked/week | <40 h/week | 25 (36.8) | 0.025 |
| 40 h/week | 403 (53.3) | ||
| 41–50 h/week | 91 (46.4) | ||
| >50 h/week | 13 (59.1) | ||
| Perception of health | Very good | 17 (27) | 0.000 |
| Good | 132 (36.2) | ||
| Fair | 248 (57.3) | ||
| Bad | 91 (74.6) | ||
| Very bad | 42 (72.4) | ||
| Physical activity | Insufficiently active | 307 (51.8) | 0.548 |
| Sufficiently active | 223 (49.9) | ||
| BMI | Underweight | 10 (47.6) | 0.074 |
| Normal weight | 245 (49.9) | ||
| Overweight | 182 (55.3) | ||
| Obese | 80 (49.38) |
| p-Value | OR | 95% CI | |
|---|---|---|---|
| Age | |||
| <35 years (ref.) | |||
| 35–44 years | 0.08 | 1.67 | 1.14–2.44 |
| 45–54 years | 0.00 | 2.51 | 1.45–3.20 |
| >55 years | 0.00 | 4.16 | 2.59–6.66 |
| Number of beds | |||
| <30 beds (ref.) | |||
| 31–44 beds | 0.66 | 1.09 | 0.74–1.59 |
| 45–60 beds | 0.07 | 1.68 | 1.15–2.46 |
| >60 beds | 0.00 | 2.44 | 1.60–3.74 |
| Scheduled breaks | |||
| Always (ref.) | |||
| Very often | 0.03 | 0.55 | 0.32–0.94 |
| Sometimes | 0.36 | 1.24 | 0.77–2.01 |
| Seldom | 0.11 | 1.50 | 0.90–2.49 |
| Never | 0.00 | 1.56 | 1.11–2.18 |
| Switches tasks with colleagues | |||
| Always (ref.) | |||
| Very often | 0.41 | 1.25 | 0.72–2.17 |
| Sometimes | 0.58 | 1.14 | 0.70–1.86 |
| Seldom | 0.20 | 1.43 | 0.81–2.50 |
| Never | 0.00 | 1.80 | 1.18–2.74 |
| Implements protocol of prevention of occupational risk when handling heavy loads | |||
| Always (ref.) | |||
| Very often | 0.15 | 1.56 | 0.84–2.86 |
| Sometimes | 0.14 | 1.54 | 0.86–2.75 |
| Seldom | 0.00 | 2.18 | 1.21–3.93 |
| Never | 0.00 | 2.36 | 1.44–3.84 |
| n | % | 95% CI | |||
|---|---|---|---|---|---|
| Physical activity (n = 1040) | Mean (SD) | 2.6 (2.3) | |||
| Groups | Insufficiently active | 593 | 57.0 | 54.0–60.0 | |
| Sufficiently active | 447 | 43.0 | 40.0–46.0 | ||
| BMI (n = 1003) | Mean (SD) | 25.7 (4.9) | |||
| Groups | Underweight (<18.5) | 21 | 2.1 | 1.4–3.2 | |
| Normal weight (18.5–24.9) | 491 | 49.0 | 45.9–52.0 | ||
| Overweight (25–29.9) | 329 | 32.8 | 30.0–35.8 | ||
| Obese (>30) | 162 | 16.2 | 14.0–15.6 | ||
| Perceived health status (n = 1041) | Mean (SD) | 72.4 (18.9) | |||
| Groups | Very good | 63 | 6.1 | 4.8–7.7 | |
| Good | 365 | 35.1 | 32.2–38.0 | ||
| Fair | 433 | 41.6 | 38.6–44.6 | ||
| Bad | 122 | 11.7 | 9.9–11.8 | ||
| Very bad | 58 | 5.6 | 4.3–7.1 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Rodríguez, C.; Bulilete, O.; Chela-Alvarez, X.; Velasco-Roldán, O.; Llobera-Canaves, J. Chronic Pain and Work Conditions of Hotel Housekeepers: A Descriptive Study. Int. J. Environ. Res. Public Health 2022, 19, 3383. https://doi.org/10.3390/ijerph19063383
Sánchez-Rodríguez C, Bulilete O, Chela-Alvarez X, Velasco-Roldán O, Llobera-Canaves J. Chronic Pain and Work Conditions of Hotel Housekeepers: A Descriptive Study. International Journal of Environmental Research and Public Health. 2022; 19(6):3383. https://doi.org/10.3390/ijerph19063383
Chicago/Turabian StyleSánchez-Rodríguez, Cristian, Oana Bulilete, Xenia Chela-Alvarez, Olga Velasco-Roldán, and Joan Llobera-Canaves. 2022. "Chronic Pain and Work Conditions of Hotel Housekeepers: A Descriptive Study" International Journal of Environmental Research and Public Health 19, no. 6: 3383. https://doi.org/10.3390/ijerph19063383