
The Impact of the COVID-19 Pandemic on Dentistry and Dental Education: A Narrative Review


Abstract
:1. Introduction
2. COVID-19 and the New Approach to Dental Healthcare
3. Dental Public Health Issues during the COVID-19 Pandemic
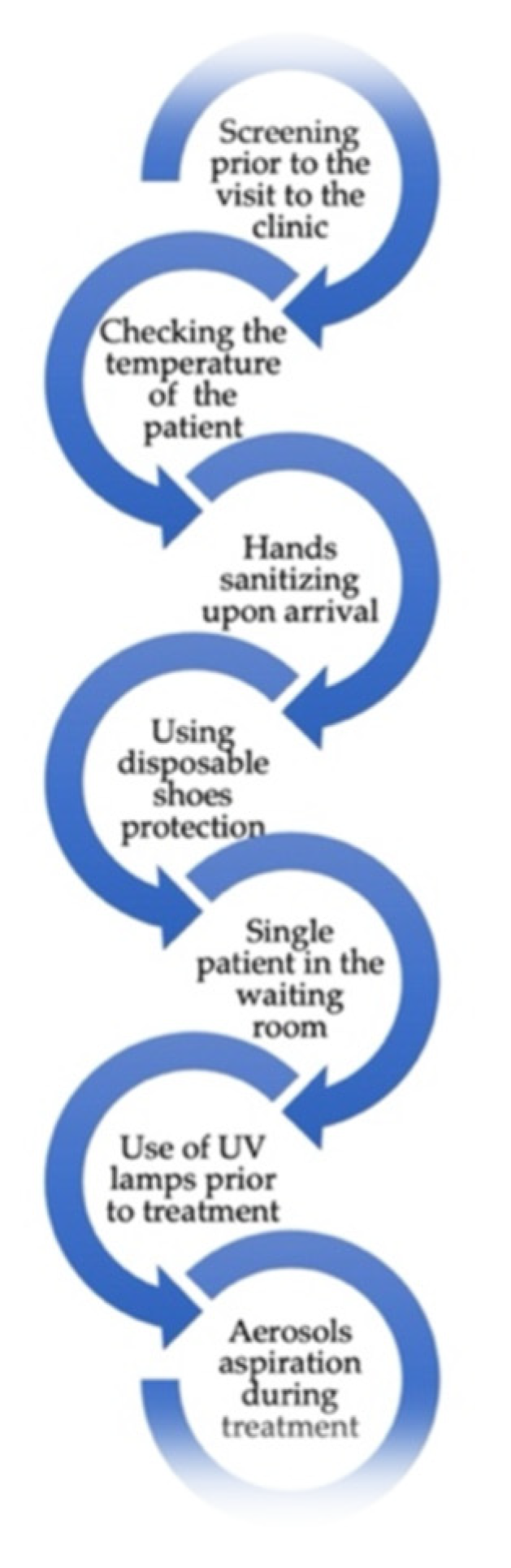
4. Pre-, during and Post-Pandemic Particular Aspects of Dental Treatments
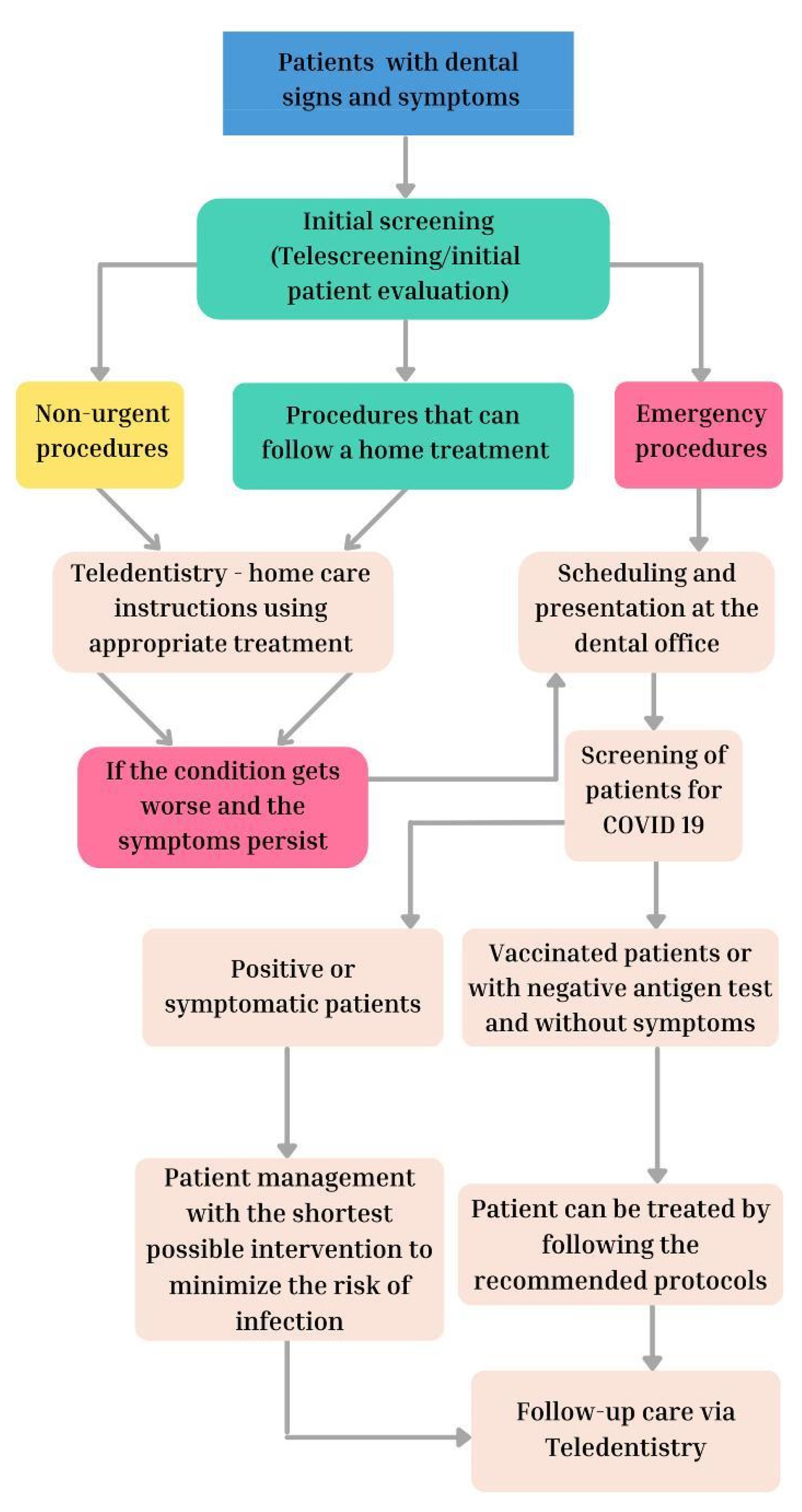
5. Teledentistry and COVID-19
6. The Impact of COVID-19 on Dental Staff
7. The Impact of COVID-19 on Dental Academic Environments
7.1. Emotional and Psychological Effects
7.2. Quality of Dental Education
7.3. Dental Research
8. Perspectives and Limitations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Devlin, H.; Soltani, P. COVID-19 and Dentistry. Encyclopedia 2021, 1, 496–504. [Google Scholar] [CrossRef]
- Darvish, S.; Salman, B.N. General Considerations for the Practice of Pediatric Dentistry in the Period of COVID-19 pandemic: A Review. J. Biosci. Med. 2021, 9, 29–42. [Google Scholar] [CrossRef]
- Senpuku, H.; Fukumoto, M.; Uchiyama, T.; Taguchi, C.; Suzuki, I.; Arikawa, K. Effects of Extraoral Suction on Droplets and Aerosols for Infection Control Practices. Dent. J. 2021, 9, 80. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Li, Y.; Gan, F.; Du, Y.; Yao, Y. Salivary Glands: Potential Reservoirs for COVID-19 Asymptomatic Infection. J. Dent. Res. 2020, 99, 989. [Google Scholar] [CrossRef] [Green Version]
- Giraudeau, N. Teledentistry and COVID-19: Be Mindful of Bogus “Good” Ideas! Inquiry 2021, 58, 00469580211015050. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Natoli, V.; Bruni, A.; Coscione, C.; Magliano, G.; Giacobbo, G.; Morelli, A.; Moressa, S.; Scribante, A. Bio-Inspired Systems in Nonsurgical Periodontal Therapy to Reduce Contaminated Aerosol during COVID-19: A Comprehensive and Bibliometric Review. J. Clin. Med. 2020, 9, 3914. [Google Scholar] [CrossRef]
- Kwok, Y.L.A.; Gralton, J.; McLaws, M.L. Face Touching: A Frequent Habit that Has Implications for Hand Hygiene. Am. J. Infect. Control 2020, 43, 112–114. [Google Scholar] [CrossRef]
- Salgarello, S.; Salvadori, M.; Mazzoleni, F.; Francinelli, J.; Bertoletti, P.; Audino, E.; Garo, M.L. The New Normalcy in Dentistry after the COVID-19 Pandemic: An Italian Cross-Sectional Survey. Dent. J. 2021, 9, 86. [Google Scholar] [CrossRef]
- Vergara-Buenaventura, A.; Castro-Ruiz, C. Use of mouthwashes against COVID-19 in dentistry. Br. J. Oral Maxillofac. Surg. 2020, 58, 924–927. [Google Scholar] [CrossRef]
- Kappenberg-Nitescu, D.C.; Luchian, I.; Martu, I.; Solomon, S.; Martu, S.; Pasarin, L.; Martu, A.; Sioustis, I.A.; Goriuc, A.; Tatarciuc, M. Periodontal effects of two innovative oral rinsing substances in oncologic patients. Exp. Ther. Med. 2021, 21, 1. [Google Scholar] [CrossRef]
- Scarano, A.; Inchingolo, F.; Lorusso, F. Environmental Disinfection of a Dental Clinic during the COVID-19 Pandemic: A Narrative Insight. BioMed Res. Int. 2020, 1, 15. [Google Scholar] [CrossRef] [PubMed]
- Meethil, A.P.; Saraswat, S.; Chaudhary, P.P.; Dabdoub, S.M.; Kumar, P.S. Sources of SARS-CoV-2 and Other Microorganisms in Dental Aerosols. J. Dent. Res. 2021, 100, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Nijakowski, K.; Cieślik, K.; Łaganowski, K.; Gruszczyński, D.; Surdacka, A. The Impact of the COVID-19 Pandemic on the Spectrum of Performed Dental Procedures. Int. J. Environ. Res. Public Health 2021, 18, 3421. [Google Scholar] [CrossRef] [PubMed]
- Benzian, H.; Beltrán-Aguilar, E.; Niederman, R. Systemic Management of Pandemic Risks in Dental Practice: A Consolidated Framework for COVID-19 Control in Dentistry. Front. Med. 2021, 8, 196. [Google Scholar] [CrossRef]
- Expósito-Delgado, A.J.; Ausina-Márquez, V.; Mateos-Moreno, M.V.; Martínez-Sanz, E.; del Carmen Trullols-Casas, M.; Llamas-Ortuño, M.E.; Blanco-González, J.M.; Almerich-Torres, T.; Bravo, M.; Martínez-Beneyto, Y. Delivery of Health Care by Spanish Dental Hygienists in Private and Public Dental Services during the COVID-19 De-Escalation Phase (June 2020): A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 8298. [Google Scholar] [CrossRef]
- Ghai, S. Teledentistry during COVID-19 pandemic. Diabetes Metab. Syndr. 2020, 14, 933–935. [Google Scholar] [CrossRef]
- Giudice, A.; Barone, S.; Muraca, D.; Averta, F.; Diodati, F.; Antonelli, A.; Fortunato, L. Can Teledentistry Improve the Monitoring of Patients during the COVID-19 Dissemination? A Descriptive Pilot Study. Int. J. Environ. Res. Public Health. 2020, 17, 3399. [Google Scholar] [CrossRef]
- Dusseja, S.H.; Dinesh, R.; Panwar, S.; Safna, A. Patients’ Views Regarding Dental Concerns and Tele dentistry during COVID-19 Pandemic. Int. J. Environ. Res. Public Health. 2020, 5, 423–429. [Google Scholar]
- Machado, R.A.; Souza, N.L.; Oliveira, R.M.; Martelli Junior, H.; Bonan, P.R.F. Social media and telemedicine for oral diagnosis and counselling in the COVID-19 era. Oral Oncol. 2020, 105, 104685. [Google Scholar] [CrossRef]
- Estai, M.; Kruger, E.; Tennant, M.; Bunt, S.; Kanagasingam, Y. Challenges in the uptake of telemedicine in dentistry. Rural Remote Health 2016, 16, 3915. [Google Scholar] [CrossRef]
- Kappenberg-Niţescu, D.C.; Păsărin, L.; Mârţu, S.; Teodorescu, C.; Vasiliu, B.; Mârţu, I.; Luchian, I.; Solomon, S.M. Determining Chemotherapy Agents in Saliva through Spectrometry and Chromatography Methods Correlated with Periodontal Status in Oncology Patients. Appl. Sci. 2021, 11, 5984. [Google Scholar] [CrossRef]
- Madi, M.; Kumar, M.; Pentapati, K.C.; Vineetha, R. Smart-phone based telemedicine: Instant messaging application as a platform for radiographic interpretations of jaw pathologies. J. Oral Biol. Craniofac. Res. 2021, 11, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Torul, D.; Kahveci, K.; Kahveci, C. Is Tele-Dentistry an Effective Approach for Patient Follow-up in Maxillofacial Surgery. J. Maxillofac. Oral Surg. 2021, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wallace, C.K.; Schofield, C.E.; Burbridge, L.A.L.; O’Donnell, K.L. Role of teledentistry in paediatric dentistry. Br. Dent. J. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Mekhemar, M.; Attia, S.; Dörfer, C.; Conrad, J. Dental Nurses’ Mental Health in Germany: A Nationwide Survey during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 8108. [Google Scholar] [CrossRef]
- Schmidt, J.; Perina, V.; Treglerova, J.; Pilbauerova, N.; Suchanek, J.; Smucler, R. COVID-19 Prevalence among Czech Dentists. Int. J. Environ. Res. Public Health 2021, 18, 12488. [Google Scholar] [CrossRef] [PubMed]
- Koç, Y.; Akyüz, S.; Akşit-Bıçak, D. Clinical Experience, Knowledge, Attitudes and Practice of Turkish Pediatric Dentists during the COVID-19 Pandemic. Medicina 2021, 57, 1140. [Google Scholar] [CrossRef]
- Morgado, M.; Mendes, J.J.; Proença, L. COVID-19 Risk Perception and Confidence among Clinical Dental Students: Impact on Patient Management. Med. Sci. Forum 2021, 5, 26. [Google Scholar] [CrossRef]
- Balkaran, R.; Bhat, M.; Smith, W.; Marchan, S. COVID-19 Stressors among Dental Academics at UWI—A Caribbean Perspective. Oral 2021, 1, 5. [Google Scholar] [CrossRef]
- Mekhemar, M.; Attia, S.; Dörfer, C.; Conrad, J. Dental Students in Germany throughout the COVID-19 Pandemic: A Psychological Assessment and Cross-Sectional Survey. Biology 2021, 10, 611. [Google Scholar] [CrossRef]
- Zarzecka, J.; Zarzecka-Francica, E.; Gala, A.; Gębczyński, K.; Pihut, M. Dental environmental stress during the COVID-19 pandemic at the Jagiellonian University Medical College, Kraków, Poland. Int. J. Occup. Med. Environ. Health 2021, 34, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.G.; Amer, H. Dental Education in the Time of COVID-19 Pandemic: Challenges and Recommendations. Front. Med. 2021, 8, 648899. [Google Scholar] [CrossRef] [PubMed]
- Talapko, J.; Perić, I.; Vulić, P.; Pustijanac, E.; Jukić, M.; Bekić, S.; Meštrović, T.; Škrlec, I. Mental Health and Physical Activity in Health-Related University Students during the COVID-19 Pandemic. Healthcare 2021, 9, 801. [Google Scholar] [CrossRef] [PubMed]
- Teodorescu, A.C.; Martu, I.; Teslaru, S.; Kappenberg-Nitescu, D.C.; Goriuc, A.; Luchian, I.; Martu, M.A.; Solomon, S.M.; Martu, S. Assessment of Salivary Levels of RANKL and OPG in Aggressive versus Chronic Periodontitis. J. Immunol. Res. 2019, 2019, 6195258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luchian, I.; Moscalu, M.; Goriuc, A.; Nucci, L.; Tatarciuc, M.; Martu, I.; Covasa, M. Using Salivary MMP-9 to Successfully Quantify Periodontal Inflammation during Orthodontic Treatment. J. Clin. Med. 2021, 10, 379. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.K.; Chen, S.Y.; Liu, I.J.; Chen, Y.C.; Chen, H.L.; Yang, C.F.; Chen, P.J.; Yeh, S.H.; Kao, C.L.; Huang, L.M.; et al. Detection of SARS-Associated Coronavirus in Throat Wash and Saliva in Early Diagnosis. Emerg. Infect. Dis. 2004, 10, 1213–1219. [Google Scholar] [CrossRef] [PubMed]
- Sabino-Silva, R.; Jardim, A.C.G.; Siqueira, W.L. Coronavirus COVID-19 Impacts to Dentistry and Potential Salivary Diagnosis. Clin. Oral Investig. 2020, 24, 1619–1621. [Google Scholar] [CrossRef] [Green Version]
- Luchian, I.; Vata, I.; Martu, I.; Stirbu, C.; Tatarciuc, M.; Martu, S. The periodontal effects of an optimal intrusive force on a maxillary central incisor. A FEM evaluation. Rom. J. Oral Rehab. 2016, 8, 51–55. [Google Scholar]
- Luchian, I.; Martu, M.-A.; Tatarciuc, M.; Scutariu, M.M.; Ioanid, N.; Pasarin, L.; Kappenberg-Nitescu, D.C.; Sioustis, I.-A.; Solomon, S.M. Using FEM to Assess the Effect of Orthodontic Forces on Affected Periodontium. Appl. Sci. 2021, 11, 7183. [Google Scholar] [CrossRef]
- Tatarciuc, M.; Maftei, G.A.; Vitalariu, A.; Luchian, I.; Martu, I.; Diaconu-Popa, D. Inlay-Retained Dental Bridges—A Finite Element Analysis. Appl. Sci. 2021, 11, 3770. [Google Scholar] [CrossRef]
- Sioustis, I.-A.; Axinte, M.; Prelipceanu, M.; Martu, A.; Kappenberg-Nitescu, D.-C.; Teslaru, S.; Luchian, I.; Solomon, S.M.; Cimpoesu, N.; Martu, S. Finite Element Analysis of Mandibular Anterior Teeth with Healthy, but Reduced Periodontium. Appl. Sci. 2021, 11, 3824. [Google Scholar] [CrossRef]
- Devlin, A. Post-pandemic dentistry—Restart or reform? Br. Dent. J. 2021, 230, 306. [Google Scholar] [CrossRef] [PubMed]
- Martu, M.A.; Maftei, G.A.; Sufaru, I.G.; Jelihovschi, I.; Luchian, I.; Hurjui, L.; Martu, I.; Pasarin, L. COVID-19 and Periodontal Disease-Ethiopathogenic and Clinical Implications. Rom. J. Oral Rehab. 2020, 12, 116–124. [Google Scholar]



{kind=link}
{kind=link}
| SARS-CoV-2 | Percentage |
|---|---|
| United States | 18.19% |
| India | 15.22% |
| Brazil | 9.65% |
| Russia | 3.17% |
| France | 3.11% |
| United Kingdom | 3.06% |
| Spain | 2.25% |
| Romania | 6.87% |
| Average | 7.69% |
| Country | Cases Confirmed | Deaths | Case Fatality (%) |
|---|---|---|---|
| Peru | 2,358,685 | 203,019 | 8.6% |
| Brazil | 22,529,183 | 620,251 | 2.8% |
| Belgium | 2,231,686 | 28,459 | 1.3% |
| Italy | 7,436,939 | 139,038 | 1.9% |
| Mexico | 4,125,388 | 300,334 | 7.3% |
| United States | 60,074,429 | 837,594 | 1.4% |
| United Kingdom | 14,563,769 | 150,634 | 1.0% |
| Ecuador | 559,950 | 33,699 | 6.0% |
| Romania | 1,844,537 | 59,011 | 3.2% |
| Spain | 7,164,906 | 89,934 | 1.3% |
| Portugal | 1,499,976 | 19,029 | 1.3% |
| France | 12,218,022 | 126,427 | 1.0% |
| South Africa | 3,526,054 | 92,453 | 2.6% |
| Iran | 6,206,405 | 131,878 | 2.1% |
| Russia | 10,470,006 | 309,787 | 3.0% |
| Greece | 1,507,616 | 21,394 | 1,4% |
| Austria | 1,339,421 | 13,848 | 1.0% |
| Germany | 7,553,743 | 114,033 | 1.5% |
| Average | 970,464,876 | 163,519,323 | 2.70% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goriuc, A.; Sandu, D.; Tatarciuc, M.; Luchian, I. The Impact of the COVID-19 Pandemic on Dentistry and Dental Education: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 2537. https://doi.org/10.3390/ijerph19052537
Goriuc A, Sandu D, Tatarciuc M, Luchian I. The Impact of the COVID-19 Pandemic on Dentistry and Dental Education: A Narrative Review. International Journal of Environmental Research and Public Health. 2022; 19(5):2537. https://doi.org/10.3390/ijerph19052537
Chicago/Turabian StyleGoriuc, Ancuta, Darius Sandu, Monica Tatarciuc, and Ionut Luchian. 2022. "The Impact of the COVID-19 Pandemic on Dentistry and Dental Education: A Narrative Review" International Journal of Environmental Research and Public Health 19, no. 5: 2537. https://doi.org/10.3390/ijerph19052537