
A Digital Health Service for Elderly People with Balance Disorders and Risk of Falling: A Design Science Approach


Abstract
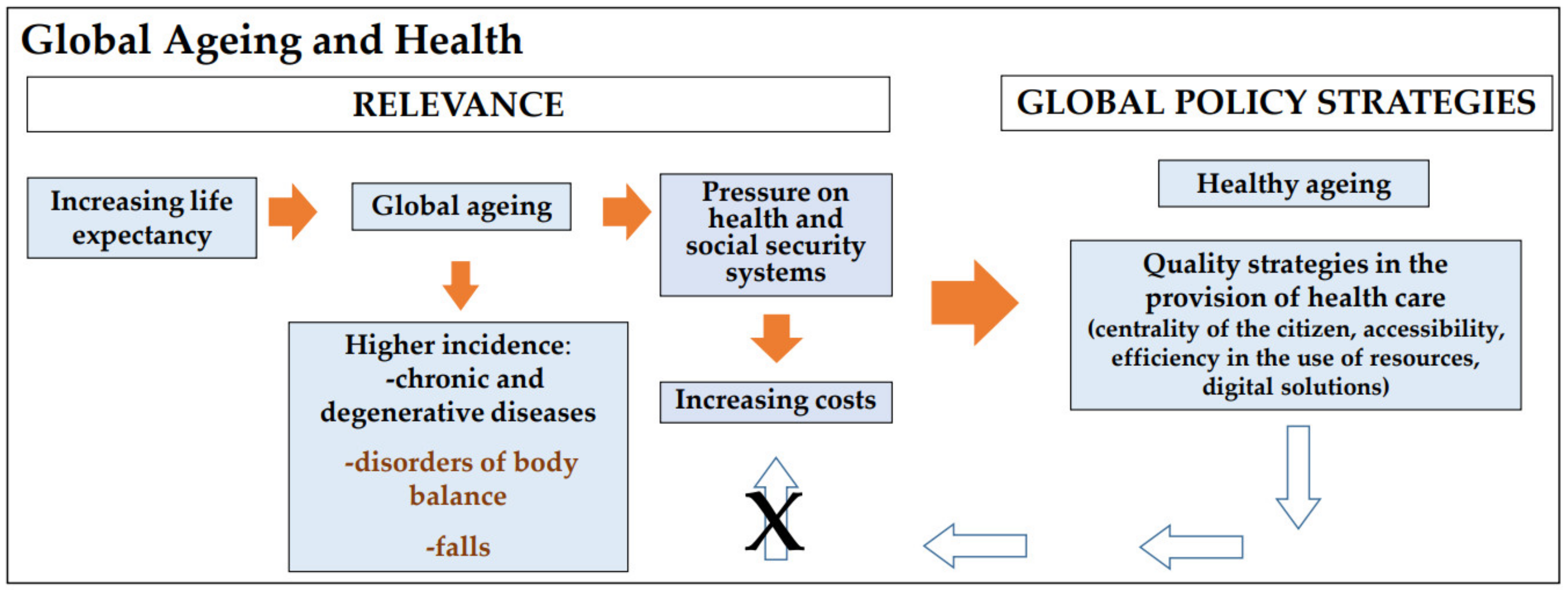
:1. Introduction
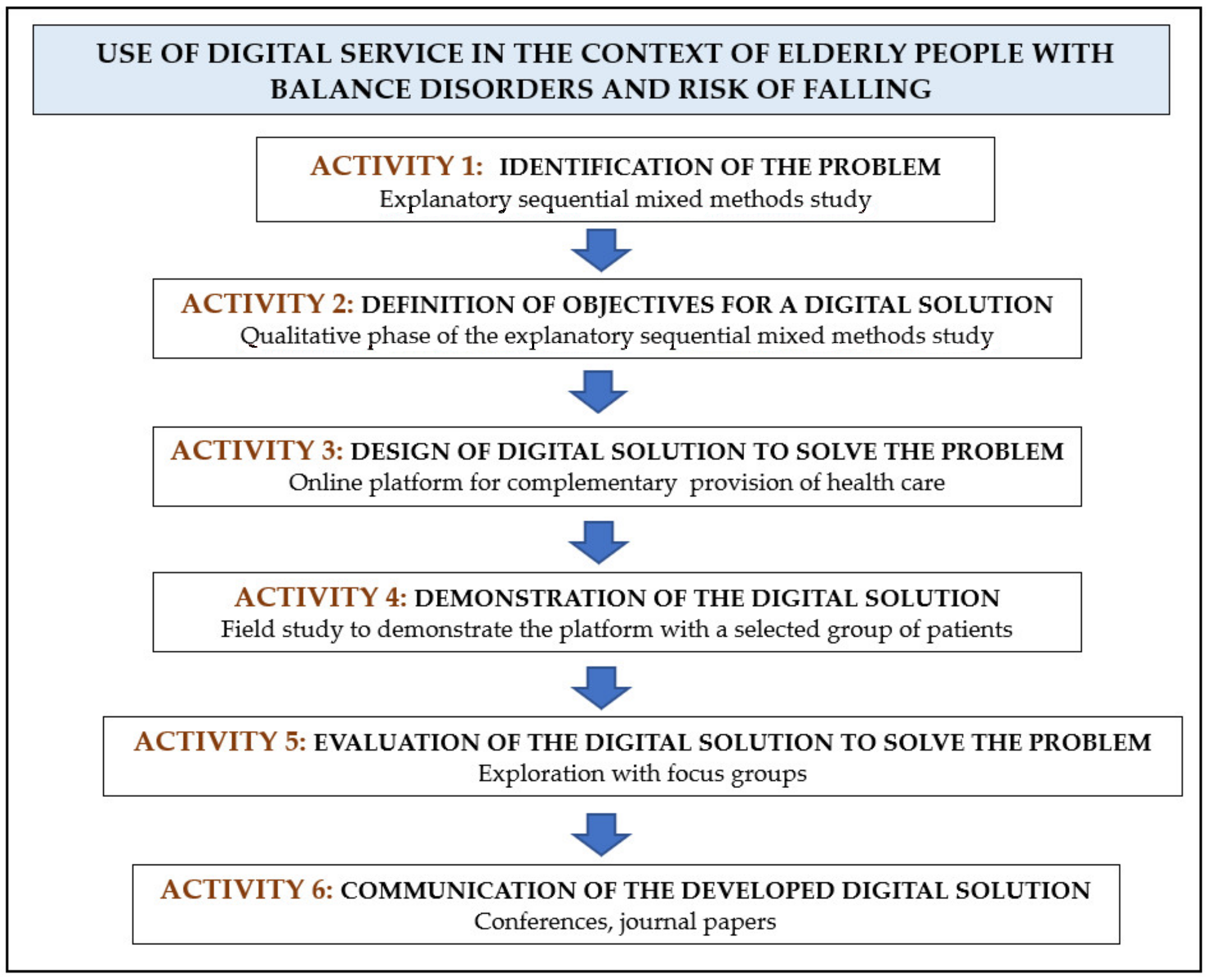
2. Materials and Methods
2.1. Study Design and Materials
2.2. Data Analysis
2.3. Ethical Considerations
3. Results
3.1. Design of a Digital Solution to Solve the Problem
- (a)
- Quick access to balance deterioration or recent fall data;
- (b)
- Provide tutorial videos with specific balance exercises (1. Walk; 2. Walk turning the head to the right and to the left; 3. Walk lifting your legs; 4. Walk lifting the legs and turning the head to the right and to the left; 5. Walk with legs progressively apart. Video A—Moving target with motionless head; Video B—Moving head with motionless target; Video C—Moving head and target);
- (c)
- Regular monitoring and adjustment of vestibular exercises.
3.1.1. Medical Profile
- (a)
- Balance monitoring (i.e., access to clinical data): the SOAP framework [32] was used, with a checklist and free-text, with the following: Subjective (complaints: vertigo, unsteadiness, difficulty walking at home or outside, need for crutches or canes to walk, falls, triggers, hearing loss or tinnitus); Objective clinical examination findings (gait, otoscopy, clinical and instrumental examination, Time Up and Go Test (TUGT), Berg Balance Scale (BBS), Tinetti Performance e-Oriented Mobility Assessment (POMA), cochleovestibular instrumental exams, imaging exams and blood tests); Assessment based on the information collected in the previous two sections, with the summary of the salient points; Plan (treatment: medication and balance rehabilitation);
- (b)
- Patient balance deterioration records: the physician could identify an eventual clinical deterioration and triggers, with a checklist and free-text structure data recorded by the patient from home;
- (c)
- Patient’s fall records: the physician could be alerted of an eventual episode of falling, triggers and consequences, with a checklist and free-text data recorded by the patient;
- (d)
- Dizziness Handicap Inventory (DHI) [25]: the physician could access the 25-item questionnaire and the final score, automatically summed;
- (e)
- Balance rehabilitation prescription: the physician could also provide additional information with free-text;
- (f)
- Patient record about exercises performed: the physician could monitor the daily frequency of the balance exercises performed and access a possible video link uploaded by the patient with exercises performed.
3.1.2. Patient Profile
- (a)
- Patient balance deterioration records: the patient or caregiver could record a recent deterioration of the balance. This information, either with checklist and free-text, can also be visible in the medical profile;
- (b)
- Patient’s fall records: the patient or caregiver can record the episodes of falling; this information, checklist and free-text, can be also visible in the medical profile;
- (c)
- DHI questionnaire [25]: to be completed before and after the balance rehabilitation program; the final score can be automatically summed and is visible in the medical profile;
- (d)
- Recorded tutorial videos with balance exercises: each one presents instructions on the exercise to be performed, allowing for viewing in slow motion and at normal speed of the exercise;
- (e)
- Patient record about exercises performed with checklist structure: the patient can upload a recorded video link of other exercises performed. This information can also be visible in the medical profile. At any time, both physician and participants can send or receive messages with questions or comments, enabling a more dynamic physician–patient interaction. All data are processed with security, respecting the General Data Protection Regulation rules.
3.2. Demonstration of the Digital Solution
3.2.1. Participants
3.2.2. Remote Monitoring
3.2.3. Participant and Caregiver Registration in the Digital Platform “BALANCE”
3.3. Evaluation of the Digital Solution to Solve the Problem
3.3.1. Focus Group Socio-Demographic Participant Data
3.3.2. Focus group-Content Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Thematic Categories | Questions |
|---|---|
| Benefits of “BALANCE” service | “In your opinion, was this digital service beneficial? Why?” |
| Constraints relatively the digital service | “Did you have difficulty using this digital service?” If yes, what were the difficulties“ |
| Satisfaction | “What is your level of satisfaction regarding the use of the “BALANCE” service?” |
| Strategies to improve the digital service | “What would you recommend to improve this service?” |
| Interest in maintaining the use | “Would you like to continue using the “BALANCE” service?” |
| Thematic Categories | Questions |
|---|---|
| Benefits of “BALANCE” service | “What do you think about the benefits of this digital service for the provision of complementary healthcare for elderly people with balance disorders and risk of falling?” |
| Constraints regarding the use of “BALANCE” service | “What is your opinion about the constrains/limitations regarding this service?” |
| Medical satisfaction with “BALANCE” service functionalities | “How satisfied are you with the potential of this digital service?” |
| Suggested strategies to adjust “BALANCE” service | “What strategies can be implemented to improve BALANCE service?” |
| Suggested strategies for clinical applicability | “How can “BALANCE” service be suitable for clinical applicability?” |
| Interest in the “BALANCE” service | “In your opinion, is there interest in this digital complementary health service?” |
References
- World Health Organization (WHO). Regional Office for Europe. Portugal-Country Case Study on the Integrated Delivery of Long-Term Care. 2020. Available online: https://www.euro.who.int/__data/assets/pdf_file/0004/426388/05_PORT-CountryRep_WEB.pdf (accessed on 10 August 2021).
- WHO Regional Office for Europe. Age-Friendly Environments in Europe. A Handbook of Domains for Policy Action. 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/334251/9789289052887-eng.pdf (accessed on 10 August 2021).
- World Health Organization (WHO). Decade of Healthy Ageing. Baseline Report. 2020. Available online: https://www.who.int/publications/i/item/9789240017900 (accessed on 11 October 2021).
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]
- OECD. Health at a Glance 2021: OECD Indicators; OECD Publishing: Paris, France, 2021. [Google Scholar] [CrossRef]
- Fernández, L.; Breinbauer, H.A.; Delano, P.H. Vertigo and Dizziness in the Elderly. Front. Neurol. 2015, 6, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, H.; Moreno-Agostino, D.; Chua, K.C.; Vitoratou, S.; Prina, A.M. Trajectories of healthy ageing among older adults with multimorbidity: A growth mixture model using harmonised data from eight ATHLOS cohorts. PLoS ONE 2021, 16, e0248844. [Google Scholar] [CrossRef] [PubMed]
- Casani, A.P.; Gufoni, M.; Capobianco, S. Current Insights into Treating Vertigo in Older Adults. Drugs Aging 2021, 38, 655–670. [Google Scholar] [CrossRef]
- Ha, V.A.T.; Nguyen, T.N.; Nguyen, T.X.; Nguyen, H.T.T.; Nguyen, T.T.H.; Nguyen, A.T.; Pham, T.; Thanh Vu, H.T. Prevalence and Factors Associated with Falls among Older Outpatients. Int. J. Environ. Res. Public Health 2021, 18, 4041. [Google Scholar] [CrossRef]
- Coto, J.; Alvarez, C.L.; Cejas, I.; Colbert, B.M.; Levin, B.E.; Huppert, J.; Rundek, T.; Balaban, C.; Blanton, S.H.; Lee, D.J.; et al. Peripheral vestibular system: Age-related vestibular loss and associated deficits. J. Otol. 2021, 16, 258–265. [Google Scholar] [CrossRef]
- Zhang, R.; Liu, B.; Bi, J.; Chen, Y. Relationship Between Chronic Conditions and Balance Disorders in Outpatients with Dizziness: A Hospital-Based Cross-Sectional Study. Med. Sci. Monit. 2021, 27, e928719 Feb 21. [Google Scholar] [CrossRef]
- Florence, C.S.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. Medical Costs of Fatal and Nonfatal Falls in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, E.; Wang, X.; Grill, E. Economic burden of vertigo: A systematic review. Health Econ. Rev. 2019, 9, 27. [Google Scholar] [CrossRef]
- Lapão, L.V.; Dussault, G. The contribution of eHealth and mHealth to improving the performance of the health workforce: A review. Public Health Panor. 2017, 3, 463–471. [Google Scholar]
- Uei, S.L.; Kuo, Y.M.; Tsai, C.H.; Kuo, Y.L. An Exploration of Intent to Use Telehealth at Home for Patients with Chronic Diseases. Int. J. Environ. Res. Public Health 2017, 14, 1544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsen, C.F.; Bergland, A.; Bye, A.; Debesay, J.; Langaas, A.G. Crossing knowledge boundaries: Health care providers’ perceptions and experiences of what is important to achieve more person-centered patient pathways for older people. BMC Health Serv. Res. 2021, 21, 310. [Google Scholar] [CrossRef] [PubMed]
- Wynn, R.; Gabarron, E.; Johnsen, J.K.; Traver, V. Special Issue on E-Health Services. Int. J. Environ. Res. Public Health 2020, 17, 2885. [Google Scholar] [CrossRef] [PubMed]
- Mucchi, L.; Jayousi, S.; Gant, A.; Paoletti, E.; Zoppi, P. Tele-Monitoring System for Chronic Diseases Management: Requirements and Architecture. Int. J. Environ. Res. Public Health 2021, 18, 7459. [Google Scholar] [CrossRef]
- Leirós-Rodríguez, R.; García-Soidán, J.L.; Romo-Pérez, V. Analyzing the Use of Accelerometers as a Method of Early Diagnosis of Alterations in Balance in Elderly People: A Systematic Review. Sensors 2019, 19, 3883. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.D.; Guo, L.; Kang, D.; Xiong, S. Exergame technology and interactive interventions for elderly fall prevention: A systematic literature review. Appl. Ergon. 2017, 65, 570–581. [Google Scholar] [CrossRef]
- Gaspar, A.G.M.; Lapão, L.V. eHealth for Addressing Balance Disorders in the Elderly: Systematic Review. J. Med. Internet Res. 2021, 23, e22215. [Google Scholar] [CrossRef]
- Peffers, K.; Tuunanen, T.; Rothenberger, M.A.; Chatterjee, S. A design science research methodology for information systems research. J. Manag. Inf. Syst. 2007, 24, 45–77. [Google Scholar] [CrossRef]
- Gaspar, A.G.M.; Escada, P.; Lapão, L.V. How Can We Develop an Efficient eHealth Service for Provision of Care for Elderly People with Balance Disorders and Risk of Falling? A Mixed Methods Study. Int. J. Environ. Res. Public Health 2021, 18, 7410. [Google Scholar] [CrossRef]
- Brandt, T.; Dieterich, M.; Strupp, M. Vertigo and Dizziness: Common Complaints, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2014; ISBN-10:085729590X. [Google Scholar]
- Jacobson, G.P.; Newman, C.W. The development of the Dizziness Handicap Inventory. Arch. Otolaryngol. Head Neck Surg. 1990, 116, 424–427. [Google Scholar] [CrossRef]
- Lapão, L.V.; Peyroteo, M.; Maia, M.; Seixas, J.; Gregório, J.; Mira da Silva, M.; Heleno, B.; Correia, J.C. Implementation of Digital Monitoring Services During the COVID-19 Pandemic for Patients with Chronic Diseases: Design Science Approach. J. Med. Internet Res. 2021, 26, e24181. [Google Scholar] [CrossRef]
- Blokdyk, G. Proof of Concept Poc. A Complete Guide-2020; Edition Paperback; 5STARCooks: Brendale, Australia, 2021; 304p, ISBN-10:0655930612, ISBN-13:978-0655930617. [Google Scholar]
- Morgado, J.; Rocha, C.S.; Maruta, C.; Guerreiro, M.; Martins, I.P. Novos valores normativos do Mini-Mental State Examination. Sinapse 2009, 9, 10–16. [Google Scholar]
- Creswell, J.W.; Creswell, J.D. Research design. In Qualitative, Quantitative, and Mixed Methods Approaches, 5th ed.; SAGE Publications Inc.: Los Angeles, CA, USA, 2018. [Google Scholar]
- Assembleia da República. Lei nº 58/2019 de 8 de Agosto de 2019. Diário da República n.º 151/2019, Série I de 2019-08-08. 3–40. Available online: https://data.dre.pt/eli/lei/58/2019/08/08/p/dre (accessed on 22 February 2021).
- General Data Protection Regulation. Art. 12 GDPR–Transparent Information, Communication and Modalities for the Exercise of the Rights of the Data Subject-General Data Protection Regulation (GDPR). Available online: Gdpr-info.eu (accessed on 22 February 2021).
- Pearce, P.F.; Ferguson, L.A.; George, G.S.; Langford, C.A. The essential SOAP note in an EHR age. Nurse Pract. 2016, 41, 29–36. [Google Scholar] [CrossRef]
- Goldsack, J.C.; Zanetti, C.A. Defining and Developing the Workforce Needed for Success in the Digital Era of Medicine. Digit. Biomark. 2020, 4, 136–142. [Google Scholar] [CrossRef]
- Tossaint-Schoenmakers, R.; Versluis, A.; Chavannes, N.; Talboom-Kamp, E.; Kasteleyn, M. The Challenge of Integrating eHealth Into Health Care: Systematic Literature Review of the Donabedian Model of Structure, Process, and Outcome. J. Med. Internet Res. 2021, 23, e27180. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Kwon, I.H.; Cha, W.C. Future and Development Direction of Digital Healthcare. Healthc. Inform. Res. 2021, 27, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Van Vugt, V.A.; van der Wouden, J.C.; Essery, R.; Yardley, L.; Twisk, J.W.; van der Horst, H.E.; Maarsingh, O.R. Internet based vestibular rehabilitation with and without physiotherapy support for adults aged 50 and older with a chronic vestibular syndrome in general practice: Three armed randomised controlled trial. BMJ 2019, 367, l5922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orton, M.; Agarwal, S.; Muhoza, P.; Vasudevan, L.; Vu, A. Strengthening Delivery of Health Services Using Digital Devices. Glob. Health Sci. Pract. 2018, 6, S61–S71. [Google Scholar] [CrossRef]
- Ricciardi, W.; Pita Barros, P.; Bourek, A.; Brouwer, W.; Kelsey, T.; Lehtonen, L. How to govern the digital transformation of health services. Eur. J. Public Health 2019, 29, 7–12. [Google Scholar] [CrossRef]
- Jun, W. A Study on the Current Status and Improvement of the Digital Divide among Older People in Korea. Int. J. Environ. Res. Public Health 2020, 17, 3917. [Google Scholar] [CrossRef]
- Heponiemi, T.; Jormanainen, V.; Leemann, L.; Manderbacka, K.; Aalto, A.M.; Hyppönen, H. Digital Divide in Perceived Benefits of Online Health Care and Social Welfare Services: National Cross-Sectional Survey Study. J. Med. Internet Res. 2020, 22, e17616. [Google Scholar] [CrossRef] [PubMed]
- Trenerry, B.; Chng, S.; Wang, Y.; Suhaila, Z.S.; Lim, S.S.; Lu, H.Y.; Oh, P.H. Preparing Workplaces for Digital Transformation: An Integrative Review and Framework of Multi-Level Factors. Front. Psychol. 2021, 12, 620766. [Google Scholar] [CrossRef] [PubMed]
- Raja, M.; Bjerkan, J.; Kymre, I.G.; Galvin, K.T.; Uhrenfeldt, L. Telehealth and digital developments in society that persons 75 years and older in European countries have been part of: A scoping review. BMC Health Serv. Res. 2021, 21, 1157. [Google Scholar] [CrossRef] [PubMed]
- Sowa, A.; Tobiasz-Adamczyk, B.; Topór-Mądry, R.; Poscia, A.; la Milia, D.I. Predictors of healthy ageing: Public health policy targets. BMC Health Serv. Res. 2016, 16, 289. [Google Scholar] [CrossRef] [PubMed]
- Bechtold, U.; Stauder, N.; Fieder, M. Let’s Walk It: Mobility and the Perceived Quality of Life in Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 11515. [Google Scholar] [CrossRef]
- Cohen, A.B.; Nahed, B.V. The Digital Neurologic Examination. Digit. Biomark. 2021, 5, 114–126. [Google Scholar] [CrossRef]
- Barreto, R.G.; Yacovino, D.A.; Cherchi, M.; Nader, S.N.; Teixeira, L.J.; Silva, D.A.D.; Verdecchia, D.H. The Role of the Smartphone in the Diagnosis of Vestibular Hypofunction: A Clinical Strategy for Teleconsultation during the COVID-19 Pandemic and Beyond. Int. Arch. Otorhinolaryngol. 2021, 25, e602–e609. [Google Scholar] [CrossRef]
- Da Fonseca, M.H.; Kovaleski, F.; Picinin, C.T.; Pedroso, B.; Rubbo, P. E-Health Practices and Technologies: A Systematic Review from 2014 to 2019. Healthcare 2021, 9, 1192. [Google Scholar] [CrossRef]
- Karpathakis, K.; Libow, G.; Potts, H.W.W.; Dixon, S.; Greaves, F.; Murray, E. An Evaluation Service for Digital Public Health Interventions: User-Centered Design Approach. J. Med. Internet Res. 2021, 8, e28356. [Google Scholar] [CrossRef]



| Patient | Patient Gender | Patient Age | Education Level (Years of Schooling) | MMSE * Score | Caregiver Gender | Caregiver Age | Caregiver Education Level (Years of Schooling) |
|---|---|---|---|---|---|---|---|
| 1 | F | 70 | 6 | 30 | F | 72 | 4 |
| 2 | F | 71 | +7 | 28 | - | - | - |
| 3 | F | 80 | 6 | 27 | F | 58 | +7 |
| 4 | F | 83 | 4 | 24 | F/F | 38/59 | +7/+7 |
| 5 | F | 83 | +7 | 30 | F | 53 | +7 |
| Patient | Complaints of Difficulty with Exercise Performance (Platform Message) | Complains of Clinical Deterioration (Telephone or Zoom) | Record of Clinical Deterioration on the Platform | Complains of Falls (Telephone or Zoom) | Record of Falls on the Platform | DHI Score Pre Rehabilitation | DHI Score Post Rehabilitation | Record of Balance Exercises Performed | Upload of Video with Exercises Performed |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Sometimes | Sometimes | Not filled | No | Not filled | Not filled | Not filled | Not filled | No |
| 2 | No | Once | Once | No | Not filled | 24 | 13 | Not filled | No |
| 3 | Several times | No | Not filled | No | Not filled | 68 | 56 | Incomplete 27 days | No |
| 4 | No | Once | Not filled | No | Not filled | 28 | 16 | Not filled | No |
| 5 | Several times | Once | Once | No | Not filled | 90 | Not filled | Incomplete 20 days | No |
| Physician | Gender | Age | Specialty | Regional Health Administration of Portugal |
|---|---|---|---|---|
| 1 | M | 49 | Family Medicine | LTV |
| 2 | F | 68 | Family Medicine | Center |
| 3 | M | 59 | Internal Medicine | LTV |
| 4 | F | 60 | Internal Medicine | LTV |
| 5 | M | 58 | Otorhinolaryngology | LTV |
| 6 | M | 59 | Otorhinolaryngology | North |
| 7 | M | 61 | Otorhinolaryngology | LTV |
| 8 | M | 68 | Otorhinolaryngology | Center |
| Thematic Categories | Focus Group: Patients and Caregivers | Focus Group: Physicians |
|---|---|---|
| 1. Benefits of “BALANCE” digital service | 1.1. Patient comfort 1.2. Closer physician-patient interaction anywhere 1.3. Availability of tutorial videos with balance exercises | 1.1. Patient comfort 1.2. Closer physician-patient interaction 1.3. Lower consumption of face-to-face resources 1.4. Patient motivation and adhesion |
| 2. Constraints regarding the use of “BALANCE” digital service | 2.1. Patient profile 2.2. Presentation screen on the mobile phone 2.3. Lack of time to record the exercises performed | 2.1. Patient profile 2.2. Resistance of healthcare professionals 2.3. Lack of working time by healthcare professionals |
| 3. Satisfaction with “BALANCE” digital service functionalities | 3.1. Satisfaction level | 3.1. Satisfaction level |
| 4. Suggested strategies to improve “BALANCE” digital service | 4.1. Presentation screen of “BALANCE” 4.2. Recorded videos with more identifiable exercises 4.3. Adjustment of interactive data relatively to performed balance exercises | 4.1. Inclusion of automatic tools—objective data of performed balance exercises |
| 5. Suggested strategies for new clinical applicability of “BALANCE” digital service | - | 5.1. Working hours organization 5.2. Involvement of other health professionals 5.3. Interoperability 5.4. Funding and continuity of the use of digital solution 5.5. Recognition of the hierarchy |
| 6. Interest in using “BALANCE”digital service | 6.1. Interest in maintaining the use | 6.1. Recognized interest in using “BALANCE” digital service |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaspar, A.G.M.; Lapão, L.V. A Digital Health Service for Elderly People with Balance Disorders and Risk of Falling: A Design Science Approach. Int. J. Environ. Res. Public Health 2022, 19, 1855. https://doi.org/10.3390/ijerph19031855
Gaspar AGM, Lapão LV. A Digital Health Service for Elderly People with Balance Disorders and Risk of Falling: A Design Science Approach. International Journal of Environmental Research and Public Health. 2022; 19(3):1855. https://doi.org/10.3390/ijerph19031855
Chicago/Turabian StyleGaspar, Andréa Gomes Martins, and Luís Velez Lapão. 2022. "A Digital Health Service for Elderly People with Balance Disorders and Risk of Falling: A Design Science Approach" International Journal of Environmental Research and Public Health 19, no. 3: 1855. https://doi.org/10.3390/ijerph19031855