
The Effect of Periodontal Treatment on Clinical and Biological Indicators, Quality of Life, and Oral Health in Rheumatoid Arthritis Patients: A Quasi-Experimental Study


Abstract
:1. Introduction
2. Materials and Methods
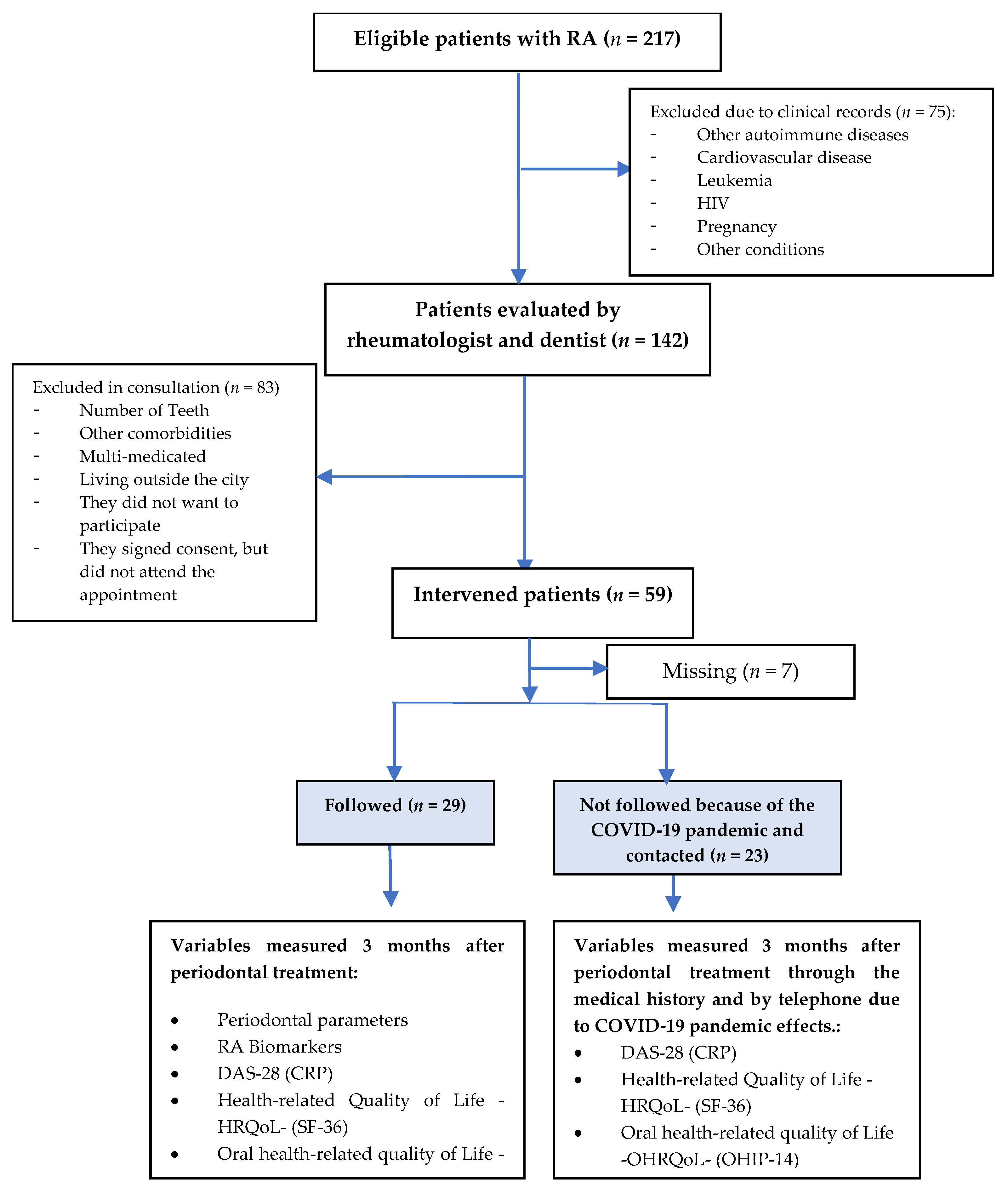
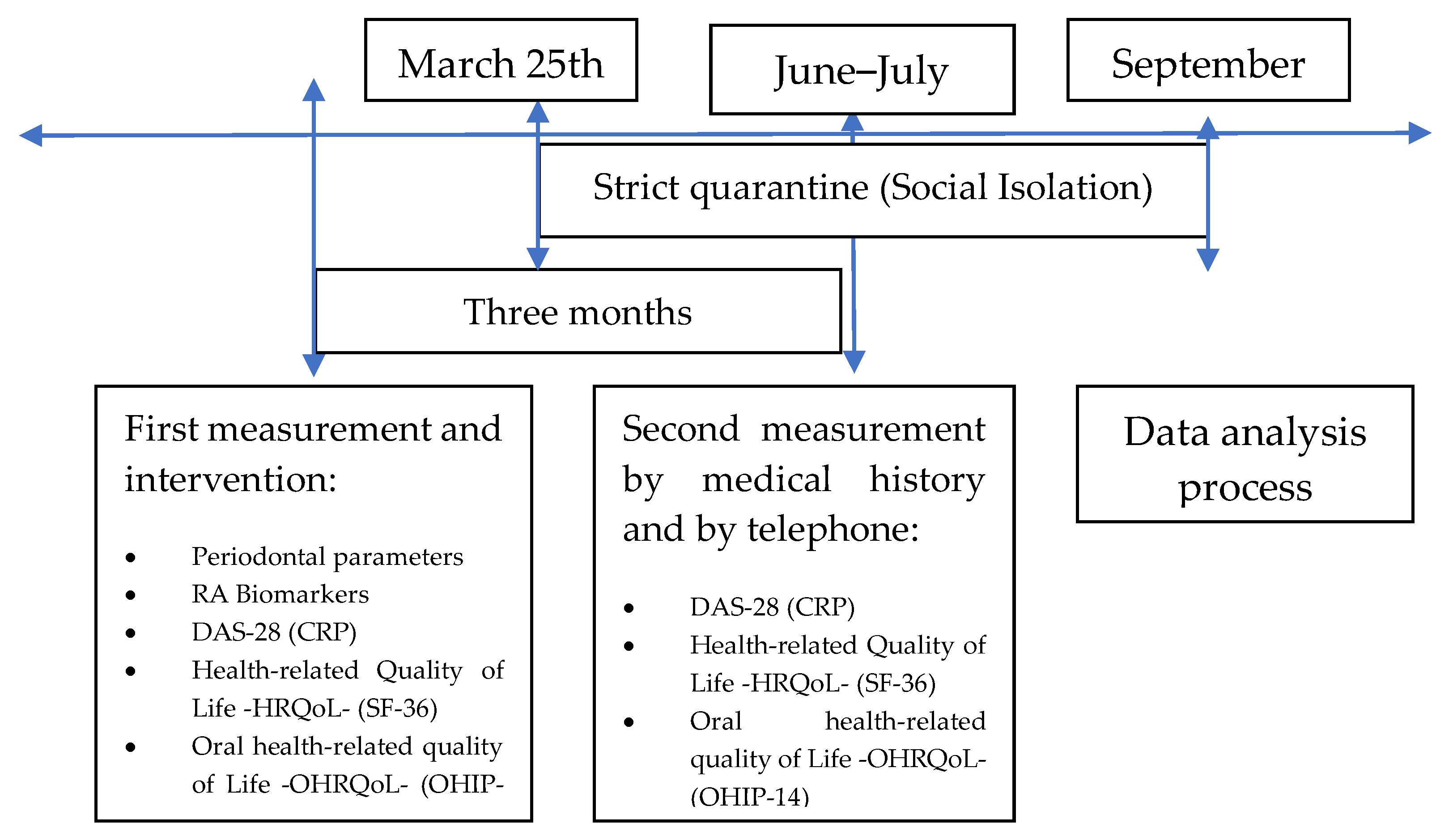
2.1. Design, Population, and Sample
2.2. Selection Criteria
2.3. Data Collection Techniques
2.3.1. Physical and Periodontal Examinations
2.3.2. Periodontal Procedures
2.4. Variables
2.5. Statistical Analysis
2.6. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Slots, J. Periodontitis: Facts, fallacies and the future. Periodontol. 2000 2017, 75, 7–23. [Google Scholar] [CrossRef]
- Dahlen, G.; Fejerskov, O.; Manji, F. Current concepts and an alternative perspective on periodontal disease. BMC Oral Health 2020, 20, 235. [Google Scholar] [CrossRef] [PubMed]
- Nazir, M.; Al-Ansari, A.; Al-Khalifa, K.; Alhareky, M.; Gaffar, B.; Almas, K. Global Prevalence of Periodontal Disease and Lack of Its Surveillance. Sci. World J. 2020, 2020, 2146160. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Salud y Protección Social (Colombia). IV Estudio Nacional de Salud Bucal. ENSAB IV: Para Saber Cómo Estamos y Saber qué Hacemos; Ministerio de Salud y Protección Social: Bogotá, Colombia, 2014.
- Kim, Y.; Oh, H.C.; Park, J.W.; Kim, I.S.; Kim, J.Y.; Kim, K.C.; Chae, D.S.; Jo, W.L.; Song, J.H. Diagnosis and Treatment of Inflammatory Joint Disease. Hip. Pelvis. 2017, 29, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Rojas, J.A.; Dávila-Ramírez, F.A.; Quintana-López, G.; Aristizábal-Gutiérrez, F.; Brown, P. Prevalencia de artritis reumatoide en Colombia: Una aproximación basada en la carga de la enfermedad durante el año 2005 [Rheumatoid arthritis prevalence in Colombia: An approach based on burden of disease study during 2005]. Rev. Colomb. Reumatol. 2016, 23, 11–16. [Google Scholar] [CrossRef]
- McInnes, I.B.; Schett, G. The pathogenesis of rheumatoid arthritis. N. Engl. J. Med. 2011, 365, 2205–2219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, S.B.; Botelho, J.; Machado, V.; Zehra, S.A.; Mendes, J.J.; Ciurtin, C.; Orlandi, M.; D’Aiuto, F. Is there a bidirectional association between rheumatoid arthritis and periodontitis? A systematic review and meta-analysis. Semin. Arthritis Rheum. 2020, 50, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Liu, Z.; Shu, D.; Xiong, Y.; He, M.; Xu, S.; Si, S.; Guo, B. Association of Periodontitis with Rheumatoid Arthritis and the Effect of Non-Surgical Periodontal Treatment on Disease Activity in Patients with Rheumatoid Arthritis. Med. Sci. Monit. 2018, 24, 5802–5810. [Google Scholar] [CrossRef]
- Del Rosa, C.D.R.D.; de Gomes, J.M.L.; de Moraes, S.L.D.; Lemos, C.A.A.; Minatel, L.; de Limirio, J.P.J.O.; Pellizzer, E.P. Does non-surgical periodontal treatment influence on rheumatoid arthritis? A systematic review and meta-analysis. Saudi Dent. J. 2021, 33, 795–804. [Google Scholar] [CrossRef]
- Qiao, Y.; Wang, Z.; Li, Y.; Han, Y.; Zhou, Y.; Cao, X. Rheumatoid arthritis risk in periodontitis patients: A systematic review and meta-analysis. Jt. Bone Spine 2020, 87, 556–564. [Google Scholar] [CrossRef]
- Samborska-Mazur, J.; Sikorska, D.; Wyganowska-Świątkowska, M. The relationship between periodontal status and rheumatoid arthritis—Systematic review. Reumatologia 2020, 58, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Mercado, F.B.; Marshall, R.I.; Klestov, A.C.; Bartold, P.M. Relationship between rheumatoid arthritis and periodontitis. J. Periodontol. 2001, 72, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Holmstrup, P.; Damgaard, C.; Olsen, I.; Klinge, B.; Flyvbjerg, A.; Nielsen, C.H.; Hansen, P.R. Comorbidity of periodontal disease: Two sides of the same coin? An introduction for the clinician. J. Oral Microbiol. 2017, 9, 1332710. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Choi, Y.Y. Rheumatoid arthritis and periodontitis in adults: Using the Korean National Health Insurance Service-National Sample Cohort. J. Periodontol. 2020, 91, 1186–1193. [Google Scholar] [CrossRef] [PubMed]
- Lew, P.H.; Rahman, M.T.; Safii, S.H.; Baharuddin, N.A.; Bartold, P.M.; Sockalingam, S.; Kassim, N.L.A.; Vaithilingam, R.D. Antibodies against citrullinated proteins in relation to periodontitis with or without rheumatoid arthritis: A cross-sectional study. BMC Oral Health 2021, 21, 360. [Google Scholar] [CrossRef]
- Tar, I.; Csősz, É.; Végh, E.; Lundberg, K.; Kharlamova, N.; Soós, B.; Szekanecz, Z.; Márton, I. Salivary citrullinated proteins in rheumatoid arthritis and associated periodontal disease. Sci. Rep. 2021, 11, 13525. [Google Scholar] [CrossRef]
- Nik-Azis, N.M.; Mohd, N.; Fadzilah, F.M.; Haflah, N.H.M.; Said, M.S.M.; Baharin, B. Rheumatoid arthritis serotype and synthetic disease-modifying anti-rheumatic drugs in patients with periodontitis: A case-control study. PLoS ONE 2021, 16, e0252859. [Google Scholar] [CrossRef]
- Roman-Torres, C.V.; Neto, J.S.; Souza, M.A.; Schwartz-Filho, H.O.; Brandt, W.C.; Diniz, R.E. An Evaluation of Non-Surgical Periodontal Therapy in Patients with Rheumatoid Arthritis. Open Dent. J. 2015, 9, 150–153. [Google Scholar] [CrossRef] [Green Version]
- Kaur, S.; Bright, R.; Proudman, S.M.; Bartold, P.M. Does periodontal treatment influence clinical and biochemical measures for rheumatoid arthritis? A systematic review and meta-analysis. Semin. Arthritis Rheum. 2014, 44, 113–122. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef]
- Romito, G.A.; Feres, M.; Gamonal, J.; Gomez, M.; Carvajal, P.; Pannuti, C.; Duque, A.D.; Romanelli, H.; Rösing, C.K.; Aranguiz Freyhofer, V.; et al. Periodontal disease and its impact on general health in Latin America: LAOHA Consensus Meeting Report. Braz. Oral Res. 2020, 34, e027. [Google Scholar] [CrossRef] [PubMed]
- Malm, K.; Bergman, S.; Andersson, M.L.; Bremander, A.; Larsson, I. Quality of life in patients with established rheumatoid arthritis: A phenomenographic study. SAGE Open Med. 2017, 5, 2050312117713647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woolf, A.D.; Pfleger, B. Burden of major musculoskeletal conditions. Bull. World Health Organ. 2003, 81, 646–656. [Google Scholar] [PubMed]
- Hsieh, P.H.; Wu, O.; Geue, C.; McIntosh, E.; McInnes, I.B.; Siebert, S. Economic burden of rheumatoid arthritis: A systematic review of literature in biologic era. Ann. Rheum. Dis. 2020, 79, 771–777. [Google Scholar] [CrossRef] [Green Version]
- Bloom, D.E.; Chen, S.; Kuhn, M.; McGovern, M.E.; Oxley, L.; Prettner, K. The economic burden of chronic diseases: Estimates and projections for China, Japan, and South Korea. J. Econ. Ageing 2020, 17, 100163. [Google Scholar] [CrossRef] [Green Version]
- Hijryana, M.; MacDougall, M.; Ariani, N.; Kusdhany, L.S.; Walls, A.W.G. Impact of Periodontal Disease on the Quality of Life of Older People in Indonesia: A Qualitative Study. JDR Clin. Trans. Res. 2021. [Google Scholar] [CrossRef]
- England, B.R.; Tiong, B.K.; Bergman, M.J.; Curtis, J.R.; Kazi, S.; Mikuls, T.R.; O’Dell, J.R.; Ranganath, V.K.; Limanni, A.; Suter, L.G.; et al. 2019 Update of the American College of Rheumatology Recommended Rheumatoid Arthritis Disease Activity Measures. Arthritis Care Res. 2019, 71, 1540–1555. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S173–S182. [Google Scholar] [CrossRef] [Green Version]
- Chapple, I.L.C.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S74–S84. [Google Scholar] [CrossRef]
- Lindy, O.; Suomalainen, K.; Mäkelä, M.; Lindy, S. Statin use is associated with fewer periodontal lesions: A retrospective study. BMC Oral Health 2008, 8, 16. [Google Scholar] [CrossRef] [Green Version]
- Prevoo, M.L.; van’t Hof, M.A.; Kuper, H.H.; van Leeuwen, M.A.; van de Putte, L.B.; van Riel, P.L. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995, 38, 44–48. [Google Scholar] [CrossRef] [Green Version]
- Lugo, L.E.; García, H.I.; Gómez, C. Confiabilidad del cuestionario de calidad de vida en salud SF-36 en Medellín, Colombia [Reliability of sf-36 quality of life in health questionnaire in Medellín, Colombia]. Rev. Fac. Nac. Salud Pública 2006, 24, 37–50. [Google Scholar]
- McHorney, C.A.; Ware, J.E., Jr.; Lu, J.F.; Sherbourne, C.D. The MOS 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med. Care 1994, 32, 40–66. [Google Scholar] [CrossRef] [PubMed]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Domingo-Salvany, A.; et al. The Spanish version of the Short Form 36 Health Survey: A decade of experience and new developments. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef] [Green Version]
- Slade, G.D. Derivation and validation of a short-form oral health impact profile. Community Dent. Oral Epidemiol. 1997, 25, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Locker, D.; Quiñonez, C. Functional and psychosocial impacts of oral disorders in Canadian adults: A national population survey. J. Can. Dent. Assoc. 2009, 75, 521. [Google Scholar] [PubMed]
- Agudelo-Suárez, A.A.; Vivares-Builes, A.M.; Muñoz-Pino, N.; Martínez-Martínez, J.M.; Reid, A.; Ronda-Pérez, E. Oral Health-Related Quality of Life in Native and Immigrant Populations in the PELFI Study in Spain. Int. J. Environ. Res. Public Health 2019, 16, 1796. [Google Scholar] [CrossRef] [Green Version]
- Suarez, A.A.A.; Hernández, A.V.; Villa, C.Z. Calidad de vida relacionada con la salud bucal en mujeres en situación de prostitución en Medellín (Colombia) y sus factores relacionados [Oral health-related quality of life of women in prostitution in Medellin (Colombia) and its associated factors]. CES Odontol. 2017, 30, 3–15. [Google Scholar] [CrossRef]
- Al-Katma, M.K.; Bissada, N.F.; Bordeaux, J.M.; Sue, J.; Askari, A.D. Control of periodontal infection reduces the severity of active rheumatoid arthritis. J. Clin. Rheumatol. 2007, 13, 134–137. [Google Scholar] [CrossRef]
- Grissom, R.J.; Kim, J.J. Effect Sizes for Research: A broad Practical Approach; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2005. [Google Scholar]
- Sánchez-Meca, J.; Marín-Martínez, F.; López-López, J.A. Meta-análisis e Intervención Psicosocial Basada en la Evidencia. Psychosoc. Interv. 2011, 20, 95–107. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Cross, M.; Smith, E.; Hoy, D.; Carmona, L.; Wolfe, F.; Vos, T.; Williams, B.; Gabriel, S.; Lassere, M.; Johns, N.; et al. The global burden of rheumatoid arthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1316–1322. [Google Scholar] [CrossRef] [PubMed]
- Camaño-Carballo, L.; Pimienta-Concepción, I.; Martínez-Martínez, R. Afectación bucal en pacientes con artritis reumatoide [Oral involvement in patients with rheumatoid arthritis]. Rev. Cuba. Reumatol. 2020, 22, e136. [Google Scholar]
- Monsarrat, P.; de Grado, G.F.; Constantin, A.; Willmann, C.; Nabet, C.; Sixou, M.; Cantagrel, A.; Barnetche, T.; Mehsen-Cetre, N.; Schaeverbeke, T.; et al. The effect of periodontal treatment on patients with rheumatoid arthritis: The ESPERA randomised controlled trial. Jt. Bone Spine 2019, 86, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Baeza, M.; Morales, A.; Cisterna, C.; Cavalla, F.; Jara, G.; Isamitt, Y.; Pino, P.; Gamonal, J. Effect of periodontal treatment in patients with periodontitis and diabetes: Systematic review and meta-analysis. J. Appl. Oral Sci. 2020, 28, e20190248. [Google Scholar] [CrossRef]
- Khan, S.; Khalid, T.; Bettiol, S.; Crocombe, L.A. Non-surgical periodontal therapy effectively improves patient-reported outcomes: A systematic review. Int. J. Dent. Hyg. 2021, 19, 18–28. [Google Scholar] [CrossRef]
- Tachibana, M.; Yonemoto, Y.; Okamura, K.; Suto, T.; Sakane, H.; Kaneko, T.; Dam, T.T.; Okura, C.; Tajika, T.; Tsushima, Y.; et al. Does periodontitis affect the treatment response of biologics in the treatment of rheumatoid arthritis? Arthritis Res. Ther. 2020, 22, 1–7. [Google Scholar] [CrossRef]
- Moura, M.F.; Cota, L.O.M.; Silva, T.A.; Cortelli, S.C.; Ferreira, G.A.; López, M.M.; Cortelli, J.R.; Costa, F.O. Clinical and microbiological effects of non-surgical periodontal treatment in individuals with rheumatoid arthritis: A controlled clinical trial. Odontology 2021, 109, 484–493. [Google Scholar] [CrossRef]
- Pinzón, E.M.R. Colombia: Impacto económico, social y político de la COVID-19 [Colombia: Economic, social and political impact of COVID-19]. Análisis Carol. 2020, 24, 1–14. [Google Scholar]
- Clemente-Suárez, V.J.; Martínez-González, M.B.; Benitez-Agudelo, J.C.; Navarro-Jiménez, E.; Beltran-Velasco, A.I.; Ruisoto, P.; Diaz Arroyo, E.; Laborde-Cárdenas, C.C.; Tornero-Aguilera, J.F. The Impact of the COVID-19 Pandemic on Mental Disorders. A Critical Review. Int. J. Environ. Res. Public Health 2021, 18, 41. [Google Scholar] [CrossRef]
- Bonfá, E.; Gossec, L.; Isenberg, D.A.; Li, Z.; Raychaudhuri, S. How COVID-19 is changing rheumatology clinical practice. Nat. Rev. Rheumatol. 2021, 17, 11–15. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Looking after Our Mental Health. Available online: https://bit.ly/3mLv20j (accessed on 4 November 2021).
- Cleaton, N.; Raizada, S.; Barkham, N.; Venkatachalam, S.; Sheeran, T.; Adizie, T.; Sapkota, H.; Singh, B.; Bateman, J. COVID-19 prevalence and the impact on quality of life from stringent social distancing in a single large UK rheumatology centre. Ann. Rheum. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ziadé, N.; El Kibbi, L.; Hmamouchi, I.; Abdulateef, N.; Halabi, H.; Hamdi, W.; Abutiban, F.; El Rakawi, M.; Eissa, M.; Masri, B. Impact of the COVID-19 pandemic on patients with chronic rheumatic diseases: A study in 15 Arab countries. Int. J. Rheum. Dis. 2020, 23, 1550–1557. [Google Scholar] [CrossRef] [PubMed]
- Tornero-Molina, J.; Sánchez-Alonso, F.; Fernández-Prada, M.; Bris-Ochaita, M.L.; Sifuentes-Giraldo, A.; Vidal-Fuentes, J. Tele-Rheumatology during the COVID-19 Pandemic. Reumatol. Clin. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mde, N.P.; Oliveira, R.D.; Novaes, A.B., Jr.; Voltarelli, J.C. Relationship between periodontitis and rheumatoid arthritis and the effect of non-surgical periodontal treatment. Braz. Dent. J. 2009, 20, 355–364. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, V.B.; Nguyen, T.T.; Huynh, N.C.; Nguyen, K.D.; Le, T.A.; Hoang, H.T. Effects of non-surgical periodontal treatment in rheumatoid arthritis patients: A randomized clinical trial. Dent. Med. Probl. 2021, 58, 97–105. [Google Scholar] [CrossRef]
- Okada, M.; Kobayashi, T.; Ito, S.; Yokoyama, T.; Abe, A.; Murasawa, A.; Yoshie, H. Periodontal treatment decreases levels of antibodies to Porphyromonas gingivalis and citrulline in patients with rheumatoid arthritis and periodontitis. J. Periodontol. 2013, 84, e74–e84. [Google Scholar] [CrossRef]
- Huang, Y.; Zhang, Z.; Zheng, Y.; Zhao, Z.; Zhong, Y.; Zhang, Q.; Xia, D.; Ma, N.; Zhang, L. Effects of non-surgical periodontal therapy on periodontal clinical data in periodontitis patients with rheumatoid arthritis: A meta-analysis. BMC Oral Health 2021, 21. [Google Scholar] [CrossRef]
- Escobar, M.L.; Grisales, R.H. Calidad de vida relacionada con la salud en pacientes con artritis reumatoide tratados en una IPS especializada, Medellín 2012 [Health-related quality of life among patients with rheumatoid arthritis treated by a specialized healthcare-providing institution, Medellín, 2012]. Rev. Fac. Nac. Salud Pública 2013, 31, 75–84. [Google Scholar]
- Schmalz, G.; Patschan, S.; Patschan, D.; Ziebolz, D. Oral-Health-Related Quality of Life in Adult Patients with Rheumatic Diseases-A Systematic Review. J. Clin. Med. 2020, 9, 1172. [Google Scholar] [CrossRef] [Green Version]
- Mühlberg, S.; Jäger, J.; Krohn-Grimberghe, B.; Patschan, S.; Mausberg, R.F.; Schmalz, G.; Haak, R.; Ziebolz, D. Oral health-related quality of life depending on oral health in patients with rheumatoid arthritis. Clin. Oral Investig. 2017, 21, 2661–2670. [Google Scholar] [CrossRef]
- Buset, S.L.; Walter, C.; Friedmann, A.; Weiger, R.; Borgnakke, W.S.; Zitzmann, N.U. Are periodontal diseases really silent? A systematic review of their effect on quality of life. J. Clin. Periodontol. 2016, 43, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Goel, K.; Baral, D. A Comparison of Impact of Chronic Periodontal Diseases and Nonsurgical Periodontal Therapy on Oral Health-Related Quality of Life. Int. J. Dent. 2017, 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanbhag, S.; Dahiya, M.; Croucher, R. The impact of periodontal therapy on oral health-related quality of life in adults: A systematic review. J. Clin. Periodontol. 2012, 39, 725–735. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | n | % |
|---|---|---|
| Sociodemographic | ||
| Sex | ||
| Male | 8 | 15.4 |
| Female | 44 | 84.6 |
| Age (years) | ||
| 27–59 | 35 | 67.3 |
| 60 and more | 17 | 32.7 |
| Years (X ± SD) | 55.2 | 9.2 |
| Education | ||
| ≤ Primary | 19 | 36.5 |
| Secondary | 28 | 53.8 |
| University | 5 | 9.6 |
| Socioeconomic status | ||
| Low | 8 | 15.4 |
| Medium | 40 | 76.9 |
| High | 4 | 7.7 |
| Labor situation | ||
| Employed | 14 | 26.1 |
| Unemployed | 38 | 73.1 |
| Habits. Medical history and medications | ||
| Smoking (Yes) | 2 | 3.8 |
| Practice exercise (Yes) | 21 | 40.4 |
| Diabetes (Yes) | 4 | 7.7 |
| Arterial hypertension (Yes) | 15 | 28.8 |
| Osteoporosis (Yes) | 11 | 21.2 |
| NSAIDs (Yes) | 14 | 26.9 |
| Corticosteroids | 36 | 69.2 |
| Biological DMARDs | 11 | 21.2 |
| Non- Biological DMARDs | 45 | 86.5 |
| RA clinical variables | ||
| ACPAs (Me-IQR) | 83.2 | 10.7–325.8 |
| RF (Me-IQR) | 77.7 | 25.0–187.7 |
| CPR (Me-IQR) | 2.3 | 0.6–7.9 |
| RA Duration in years (Me-IQR) | 8.2 | 4.1–15.0 |
| Type of RA | ||
| Polyarticular | 47 | 90.4 |
| Oligoarticular | 4 | 7.7 |
| Monoarticular | 1 | 1.9 |
| Remission (Yes) | 27 | 51.9 |
| Erosive RA (Yes) | 20 | 38.5 |
| Self-perception variables | ||
| Swelling (Yes) | 38 | 73.1 |
| Pain (Yes) | 39 | 75.0 |
| Morning stiffness (Yes) | 37 | 71.2 |
| Fatigue and depression (Yes) | 29 | 55.8 |
| Family support (Yes) | 52 | 100.0 |
| Periodontal variables | ||
| Number of teeth in mouth (Me-IQR) | 24.0 | 20.2–26.0 |
| Reduced periodontium (Yes) (n%) | 21 | 40.4 |
| Periodontitis (Yes) | 31 | 59.6 |
| Stage of periodontal disease | ||
| I | 0 | 0.0 |
| II | 1 | 3.2 |
| III | 18 | 58.1 |
| IV | 12 | 38.7 |
| Porphyromonas gingivalis (Yes) | 4 | 7.7 |
| PAL (Me-IQR) | 2.9 | 1.9–3.4 |
| PD (Me-IQR) | 2.5 | 2.1–3.4 |
| BoP (Me-IQR) | 15.6 | 10.8–26.2 |
| Variables | Before | After | Difference (95%CI) | p * | ||
|---|---|---|---|---|---|---|
| (X ± SD) | Me (IQR) | (X ± SD) | Me (IQR) | |||
| Periodontitis (n = 31) | ||||||
| RA | ||||||
| Disease activity score-28 (DAS-28) | 2.6 (1.7) | 2.3 (1.4;3.2) | 2.4 (1.5) | 2.2 (1.6;3.0) | 0.2 (−0.4;0.7) | 0.830 |
| Oral-health-related quality of life (OHRQoL) | ||||||
| OHIP-14 Score | 10.5 (12.0) | 8.0 (0.0;14.0) | 7.3 (8.5) | 5.0 (0.0;10.0) | 3.1 (0.1;6.1) | 0.054 |
| Extent | 1.9 (3.5) | 0.0 (0.0;2.0) | 0.9 (2.1) | 0.0 (0.0;0.0) | 0.9 (−0.1;1.9) | 0.065 |
| Functional limitation | 0.9 (2.1) | 0.0 (0.0;0.0) | 0.7 (1.2) | 0.0 (0.0;1.0) | 0.2 (−0.4;0.9) | 0.644 |
| Physical pain | 2.5 (2.7) | 2.0 (0.0;4.0) | 1.2 (1.6) | 0.0 (0.0;1.0) | 1.2 (0.5;1.9) | 0.004 |
| Psychological discomfort | 1.9 (2.5) | 1.0 (0.0;4.0) | 1.9 (2.1) | 2.0 (0.0;4.0) | 0.0 (−0.6;0.6) | 0.896 |
| Physical disability | 1.8 (2.2) | 0.0 (0.0:4.0) | 1.2 (1.9) | 0.0 (0.0;2.0) | 0.5 (−0.1;1.2) | 0.101 |
| Psychological disability | 1.9 (2.1) | 2.0 (0.0;3.0) | 1.0 (1.5) | 0.0 (0.0;2.0) | 0.8 (0.2;1.4) | 0.015 |
| Social disability | 0.5 (1.4) | 0.0 (0.0;0.0) | 0.3 (0.9) | 0.0 (0.0;0.0) | 0.2 (−0.3;0.7) | 0.593 |
| Handicap | 0.9 (1.6) | 0.0 (0.0;2.0) | 0.8 (1.4) | 0.0 (0.0;2.0) | 0.1 (−0.4;0.5) | 0.721 |
| Health-related quality of life (HRQoL) | ||||||
| General health perceptions | 55.3 (19.0) | 52.0 (40.0;70.0) | 62.3 (20.8) | 62.0 (50.0;77.0) | −6.9 (−13.9;0.0) | 0.037 |
| Physical functioning | 55.8 (27.3) | 60.0 (30.0;80.0) | 63.1 (22.6) | 65.0 (45.0;85.0) | −7.2 (−15.8;1.3) | 0.047 |
| Role limitations (physical) | 41.9 (45.4) | 25.0 (0.0;100.0) | 64.5 (43.2) | 100.0 (0.0;100.0) | −22.6 (−40.7;−4.5) | 0.020 |
| Role limitations (emotional) | 49.5 (50.1) | 33.3 (0.0;100.0) | 74.2 (42.7) | 100.0 (33.3;100.0) | −24.7 (−44.9;−0.5) | 0.014 |
| Social functioning | 66.9 (22.0) | 33.3 (0.0;100.0) | 70.2 (42.8) | 100.0 (33.3;100.0) | −3.2 (−11.3;4.9) | 0.459 |
| Bodily pain | 53.1 (12.4) | 54.0 (50.0;62.0) | 50.6 (13.8) | 50.0 (42.0;62.0) | 2.4 (−2.4;7.7) | 0.262 |
| Energy/vitality | 55.6 (19.4) | 55.0 (40.0;65.0) | 60.0 (21.3) | 55.0 (50.0;70.0) | −4.3 (−10.0;1.3) | 0.089 |
| Mental Health | 63.5 (19.6) | 56.0 (48.0;76.0) | 75.6 (18.8) | 76.0 (60.0;92.0) | −12.1 (−18.7;−5.5) | 0.001 |
| Health change | 27.4 (29.1) | 56.0 (48.0;76.0) | 26.6 (28.1) | 25.0 (0.0;50.0) | 0.8 (−12.2;−5.5) | 0.744 |
| Variables | Before | After | Difference (95%CI) | p * | ||
| (X ± SD) | Me (IQR) | (X ± SD) | Me (IQR) | |||
| Reduced Periodontium (n = 21) | ||||||
| RA | ||||||
| Disease activity score-28 (DAS-28) | 3.9 (1.7) | 3.7 (2.2;5.3) | 3.2 (2.0) | 2.6 (2.0;4.9) | 0.6 (−0.2;1.4) | 0.167 |
| Oral-health-related quality of life (OHRQoL) | ||||||
| OHIP-14 Score | 9.7 10.4) | 4.0 (1.5;20.5) | 13.0 (11.2) | 10.0 (3.5;17.5) | −3.2 (−8.1;1.6) | 0.196 |
| Extent | 1.6 (2.7) | 0.0 (0.0;4.5) | 1.9 (3.5) | 0.0 (0.0;2.0) | −0.3 (−1.8;1.1) | 0.623 |
| Functional limitation | 0.9 (1.4) | 0.0 (0.0;2.0) | 1.5 (1.5) | 0.0 (0.0;2.0) | −0.1 (−0.7;0.5) | 0.589 |
| Physical pain | 1.9 (2.1) | 1.1 (0.0;4.0) | 3.0 (1.9) | 3.0 (2.0;4.0) | −1.1 (−2.0;−0.2) | 0.013 |
| Psychological discomfort | 2.5 (2.2) | 2.0 (0.5;4.0) | 2.9 (2.4) | 2.0 (1.0;4.0) | −0.3 (−1.4;0.8) | 0.782 |
| Physical disability | 1.6 (2.5) | 0.0 (0.0;3.0) | 2.2 (2.6) | 2.0 (0.0;4.0) | −0.6 (−1.9;0.6) | 0.365 |
| Psychological disability | 1.4 (1.9) | 0.0 (0.0;3.0) | 1.9 (2.0) | 2.0 (0.0;3.0) | −0.5 (−1.4;0.4) | 0.235 |
| Social disability | 0.4 (0.9) | 0.0 (0.0;0.5) | 0.6 (1.1) | 0.0 (0.0;1.0) | −0.2 (−0.6;0.2) | 0.414 |
| Handicap | 0.9 (1.7) | 0.0 (0.0;2.0) | 1.2 (2.0) | 0.0 (0.0;2.0) | −0.3 (−1.2;0.6) | 0.343 |
| Health-related quality of life (HRQoL) | ||||||
| General health perceptions | 53.0 (18.3) | 47.0 (36.0;72.0) | 46.4 (22.6) | 50.0 (30.0;59.5) | 6.6 (0.1;13.1) | 0.046 |
| Physical functioning | 53.1 (22.5) | 55.0 (37.5;75.0) | 52.4 (28.3) | 55.0 (22.5;77.5) | 0.7 (−10.7;12.2) | 0.297 |
| Role limitations (physical) | 38.1 (45.1) | 0.0 (0.0;100.0) | 33.3 (44.9) | 0.0 (0.0;100.0) | 4.7 (−1.1;25.6) | 0.676 |
| Role limitations (emotional) | 52.4 (49.0) | 66.7 (0.0;100.0) | 57.1 (48.5) | 100.0 (0.0;100.0) | −4.8 (−16.1;25.6) | 0.518 |
| Social functioning | 71.4 (22.1) | 75.0 (50.0;87.5) | 61.3 (27.9) | 62.5 (43.7;87.5) | 10.2 (−1.1:21.3) | 0.067 |
| Bodily pain | 46.0 (14.7) | 52.0 (42.0;52.0) | 51.6 (12.0) | 52.0 (50.5;58.0) | 5.6 (−11.4;0.2) | 0.064 |
| Energy/vitality | 53.6 (13.8) | 50.0 (45.0;65.0) | 51.7 (18.5) | 50.0 (37.5;67.5) | 1.9 (4.5;8.2) | 0.518 |
| Mental Health | 66.1 (15.4) | 64.0 (54.0;78.0) | 65.3 (16.6) | 60.0 (56.0;76.0) | 0.8 (−5.3;6.8) | 0.759 |
| Health change | 27.4 (33.4) | 25.0 (0.0;50.0) | 39.3 (34.9) | 50.0 (0.0;75.0) | −11.9 (−26.6;2.7) | 0.128 |
| Variables | Followed Patients (n = 29) | Unfollowed Patients (n = 23) | Difference (95%CI) | p * | ||
|---|---|---|---|---|---|---|
| (X ± SD) | Me (IQR) | (X ± SD) | Me (IQR) | |||
| RA | ||||||
| DAS-28 | 2.6 (1.7) | 2.3 (1.7;3.1) | 3.0 (1.9) | 2.4 (1.7;4.2) | 0.4 (−0.6;1.4) | 0.562 |
| Oral-health-related quality of life (OHRQoL) | ||||||
| OHIP-14 Score | 12.2 (11.5) | 10.0 (3.0;17.0) | 6.6 (6.8) | 5.0 (0.0;10.5) | 5.6 (−11.3;0.0) | 0.065 |
| Extent | 2.1 (3.3) | 0.0 (0.0;2.5) | 0.3 (1.3) | 0.0 (0.0;0.0) | −1.8 (−3.3;0.2) | 0.004 |
| Functional limitation | 0.9 (1.6) | 0.0 (0.0;1.5) | 0.8 (1.0) | 0.0 (0.0;1.5) | −0.1 (−0.8;0.7) | 0.555 |
| Physical pain | 2.3 (1.9) | 2.0 (0.0;4.0) | 1.7 (1.8) | 2.0 (0.0;3.0) | −0.6 (−1.8;0.4) | 0.197 |
| Psychological discomfort | 2.9 (1.9) | 2.0 (0.0;4.0) | 1.6 (1.8) | 1.0 (0.0;2.5) | −1.3 (−2.3;0.1) | 0.043 |
| Physical disability | 2.3 (2.6) | 1.0 (0.0;5.0) | 0.9 (1.1) | 0.0 (0.0;2.0) | −1.4 (−2.6;0.2) | 0.117 |
| Psychological disability | 1.8 (2.0) | 1.0 (0.0;5.0) | 0.9 (1.1) | 0.0 (0.0;2.0) | −0.9 (−1.9;0.6) | 0.124 |
| Social disability | 0.6 (1.3) | 0.0 (0.0;0.5) | 0.3 (0.7) | 0.0(0.0;0.0) | −0.3 (−0.9;0.2) | 0.353 |
| Handicap | 1.3 (2.0) | 0.0 (0.0;2.0) | 0.5 (0.9) | 0.0 (0.0;1.0) | −0.8 (−0.9;0.2) | 0.175 |
| Health-related quality of life (HRQoL) | ||||||
| General health perceptions | 55.1 (26.3) | 55.0 (37.5;78.5) | 55.8 (17.5) | 57.0 (42.5;71.0) | 0.7 (−12.6;13.9) | 0.945 |
| Physical functioning | 56.2 (25.5) | 60.0 (35.0;75.0) | 59.3 (24.9) | 60.0 (37.5;80.0) | −3.1 (−11.5;17.6) | 0.629 |
| Role limitations (physical) | 42.2 (43.9) | 25.0 (0.0;100.0) | 60.7 (47.8) | 100.0 (0.0;100.0) | −18.5 (−7.7;44.7) | 0.132 |
| Role limitations (emotional) | 66.7 (45.4) | 100.0 (0.0;100.0) | 65.1 (47.7) | 100.0 (0.0;100.0) | −1.6(−28.3;25.1) | 0.891 |
| Social functioning | 68.1 (31.0) | 62.5 (37.5;100.0) | 61.9 (21.1) | 62.5 (50.0;75.0) | −6.2 (−22.0;9.6) | 0.287 |
| Bodily pain | 53.0 (11.3) | 51.0 (43.0;58.0) | 49.3 (14.9) | 51.0 (42.0;62.0) | −3.7 (−11.1;3.7) | 0.539 |
| Energy/vitality | 58.9 (23.4) | 55.0 (42.5;80.0) | 51.0 (12.6) | 50.0 (42.5;57.5) | −8.0 (−19.3;3.2) | 0.240 |
| Mental Health | 74.5 (20.2) | 76.0 (60.0;96.0) | 65.3 (14.3) | 64.0 (54.0;76.0) | −9.1 (−19.5;1.2) | 0.088 |
| Health change | 35.3 (31.0) | 25.0 (0.0;50.0) | 29.8 (32.2) | 25.0 (0.0;50.0) | 5.1 (−23.7;12.6) | 0.457 |
| Variables | Before | After | Difference (95%CI) | p * | ||
|---|---|---|---|---|---|---|
| (X ± SD) | Me (IQR) | (X ± SD) | Me (IQR) | |||
| RA | ||||||
| DAS-28 (n = 52) | 3.1 (1.8) | 2.3 (1.9;4.7) | 2.7 (1.8) | 2.2 (1.4;3.4) | 0.3 (−0.1;0.8) | 0.176 |
| DAS-28 (n = 29) | 3.1 (1.7) | 2.7 (2.0;4.3) | 2.6 (1.7) | 2.2 (1.7;3.1) | 0.5 (−0.2;1.1) | 0.106 |
| Variables | Before | After | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Components | KMO and Bartlett’s Test | p | Explained Variance (%) | Components | KMO and Bartlett’s Test | p | Explained Variance (%) | |||
| 1 | 2 | 1 | 2 | |||||||
| Oral-health-related quality of life (OHRQoL) | ||||||||||
| Functional limitation | 0.843 | 0.285 | 0.870 | 0.000 | 79.2 | 0.452 | 0.615 | 0.872 | 0.000 | 77.7 |
| Psychological discomfort | 0.588 | 0.643 | 0.694 | 0.499 | ||||||
| Physical disability | 0.401 | 0.821 | 0.609 | 0.586 | ||||||
| Psychological disability | 0.752 | 0.535 | 0.628 | 0.630 | ||||||
| Social disability | 0.804 | 0.204 | 0.866 | 0.307 | ||||||
| Handicap | 0.894 | 0.246 | 0.918 | 0.183 | ||||||
| Health-related quality of life (HRQoL) | ||||||||||
| General health perceptions | 0.578 | 0.446 | 0.827 | 0.000 | 73.4 | 0.404 | 0.792 | 0.880 | 0.000 | 76.2 |
| Role limitations (emotional) | 0.525 | 0.593 | 0.883 | 0.156 | ||||||
| Social functioning | 0.844 | 0.186 | 0.763 | 0.417 | ||||||
| Energy/vitality | 0.831 | 0.351 | 0.640 | 0.562 | ||||||
| Mental Health | 0.839 | 0.293 | 0.845 | 0.383 | ||||||
| Variables | Before | After | Difference (95%CI)) | p * | ||
|---|---|---|---|---|---|---|
| (X ± SD) | Me (IQR) | (X ± SD) | Me (IQR) | |||
| Oral-health-related quality of life (OHRQoL) | ||||||
| OHIP-14 Score | 12.4 (11.5) | 4.0 (0.5–17.5) | 12.2 (11.5) | 10.0 (3.0–17.0) | −1.9 (−5.9;2.0) | 0.230 |
| Extent | 1.9 (3.6) | 0.0 (0.0–3.0) | 2.1 (3.4) | 0.0 (0.0–2.5) | −0.2 (−1.4;1.0) | 0.511 |
| Functional limitation | 1.2 (2.1) | 0.0 (0.0–2.0) | 0.9 (1.6) | 0.0 (0.0–1.5) | 0.3 (−0.3;0.9) | 0.359 |
| Physical pain | 2.1 (2.4) | 1.0 (0.0–4.0) | 2.3 (1.9) | 2.0 (0.0–4.0) | −0.3 (−1.3;0.7) | 0.440 |
| Psychological discomfort | 2.1 (2.4) | 2.0 (0.0–4.0) | 3.0 (2.4) | 2.0 (0.5–5.5) | −0.9 (−1.7;−0.1) | 0.037 |
| Physical disability | 1.8 (2.5) | 0.0 (0.0–3.5) | 2.3 (2.6) | 1.0 (0.0–5.0) | −0.5 (−1.5;0.4) | 0.330 |
| Psychological disability | 1.7 (2.2) | 1.0 (0.0–3.0) | 1.8 (2.0) | 1.0 (0.0–3.0) | −0.1 (−0.9;0.8) | 0.867 |
| Social disability | 0.6 (1.5) | 0.0 (0.0–0.5) | 0.6 (1.2) | 0.0 (0.0–0.5) | 0.0 (−0.6;0.1) | 0.786 |
| Handicap | 0.8 (1.6) | 0.0 (0.0–1.0) | 1.3 (2.0) | 0.0 (0.0–2.0) | −0.5 (−1.1;1.1) | 0.151 |
| Health-related quality of life (HRQoL) | ||||||
| General health perceptions | 51.9 (18.3) | 47.0 (36.0–69.5) | 55.1 (26.3) | 55.0 (37.5–78.5) | −3.1 (−10.7;4.4) | 0.301 |
| Physical functioning | 51.7 (24.5) | 60.0 (35.0–75.0) | 56.2 (25.5) | 60.0 (35.0–75.0) | −4.4 (−14.4;5.4) | 0.607 |
| Role limitations (physical) | 37.9 (42.6) | 25.0 (0.0;87.5) | 42.2 (43.9) | 25.0 (0.0–100.0) | −28.7 (−47.1;−10.4) | 0.545 |
| Role limitations (emotional) | 50.6 (49.3) | 33.3 (0.0–100.0) | 66.7 (45.2) | 100.0 (0.0–100.0) | −16.1 (−34.8;2.7) | 0.046 |
| Social functioning | 69.8 (20.7) | 75.0 (50.0–87.5) | 68.1 (31.2) | 62.5 (37.5–100.0) | −1.7 (−9.2;12.7) | 0.644 |
| Bodily pain | 50.2 (13.2) | 52.0 (42.0–57.0) | 53.0 (11.3) | 51.0 (43.0–58.0) | −2.8 (−9.4;3.7) | 0.315 |
| Energy/vitality | 56.9 (17.2) | 55.0 (45.0–70.0) | 59.0 (23.4) | 55.0 (42.5–80.0) | −2.0 (−8.0;3.9) | 0.653 |
| Mental Health | 64.5 (18.9) | 56.0 (50.0–78.0) | 74.5 (20.1) | 76.0 (60.0–96.0) | −9.9 (−17.5;−2.4) | 0.019 |
| Health change | 31.0 (33.2) | 25.0 (0.0–50.0) | 35.3 (30.9) | 25.0 (0.0–50.0) | −4.3 (−17.5;8.9) | 0.530 |
| Variables with More Than Four Significant Correlations According to Spearman’s Rho (n = 29) | Variables in the Model | Before | After | ||
|---|---|---|---|---|---|
| Regression Coefficient | Determination Coefficient (%) | Regression Coefficient | Determination Coefficient (%) | ||
| Health-Related Quality of Life (HRQoL) | |||||
| General health perceptions | DAS-28 | 0.112 | 20.6 | −0.123 | 5.7 |
| Physical disability | −0.001 | −0.103 * | |||
| Psychological disability | −0.700 * | −0.107 | |||
| Physical pain | −0.595 * | −0.164 | |||
| PD Mean | −0.149 | −0.310 * | |||
| Role limitations (emotional) | DAS-28 | −0.015 | 8.7 | −0.305 | 12.2 |
| Physical disability | 0.121 | 0.19 | |||
| Psychological discomfort | −0.329 * | −0.358 * | |||
| Psychological disability | −0.326 * | −0.380 * | |||
| Physical pain | 0.104 | −0.262 * | |||
| PD Mean | 0.253 | 0.154 | |||
| Health change | DAS-28 | 0.076 | 18.2 | 0.348 * | 18.0 |
| Physical disability | −0.291 * | 0.349 ** | |||
| Psychological disability | 0.535 | −0.118 | |||
| Physical pain | 0.085 | 0.323 * | |||
| PD Mean | −0.264 | 0.001 | |||
| Number of teeth in mouth | 0.314 * | 0.327 * | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Posada-López, A.; Botero, J.E.; Pineda-Tamayo, R.A.; Agudelo-Suárez, A.A. The Effect of Periodontal Treatment on Clinical and Biological Indicators, Quality of Life, and Oral Health in Rheumatoid Arthritis Patients: A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2022, 19, 1789. https://doi.org/10.3390/ijerph19031789
Posada-López A, Botero JE, Pineda-Tamayo RA, Agudelo-Suárez AA. The Effect of Periodontal Treatment on Clinical and Biological Indicators, Quality of Life, and Oral Health in Rheumatoid Arthritis Patients: A Quasi-Experimental Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1789. https://doi.org/10.3390/ijerph19031789
Chicago/Turabian StylePosada-López, Adriana, Javier Enrique Botero, Ricardo Antonio Pineda-Tamayo, and Andrés A. Agudelo-Suárez. 2022. "The Effect of Periodontal Treatment on Clinical and Biological Indicators, Quality of Life, and Oral Health in Rheumatoid Arthritis Patients: A Quasi-Experimental Study" International Journal of Environmental Research and Public Health 19, no. 3: 1789. https://doi.org/10.3390/ijerph19031789