
Attachment- and Relationship-Based Interventions during NICU Hospitalization for Families with Preterm/Low-Birth Weight Infants: A Systematic Review of RCT Data


Abstract
:1. Introduction
2. Methods
2.1. Core Questions
2.2. Search Strategy and Study Selection
2.3. Quality Assessment of the Selected Studies
2.4. Data Analysis
3. Results
3.1. Description of Studies
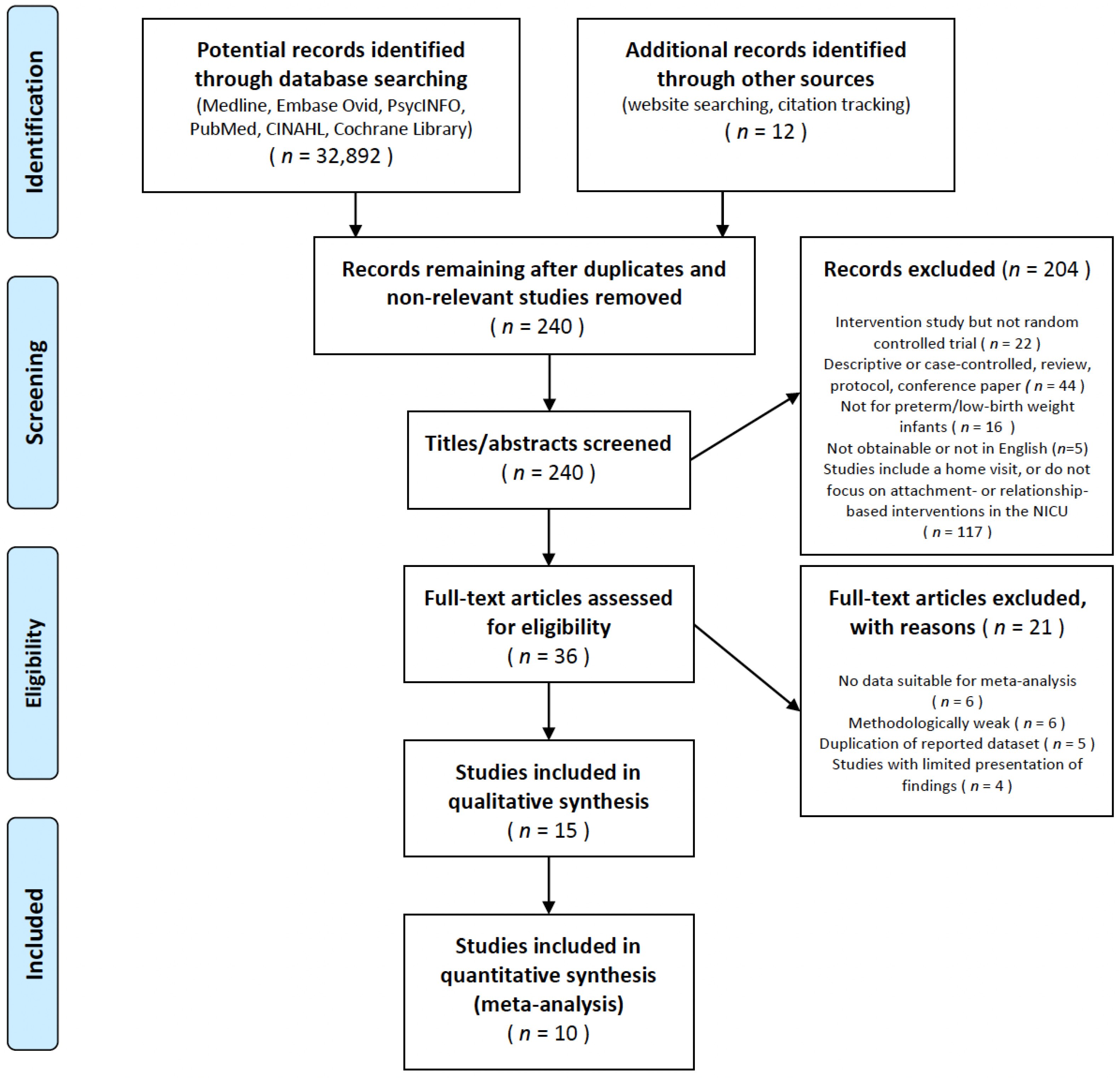
3.1.1. Search Results
3.1.2. Study Characteristics
3.1.3. Intervention Participants
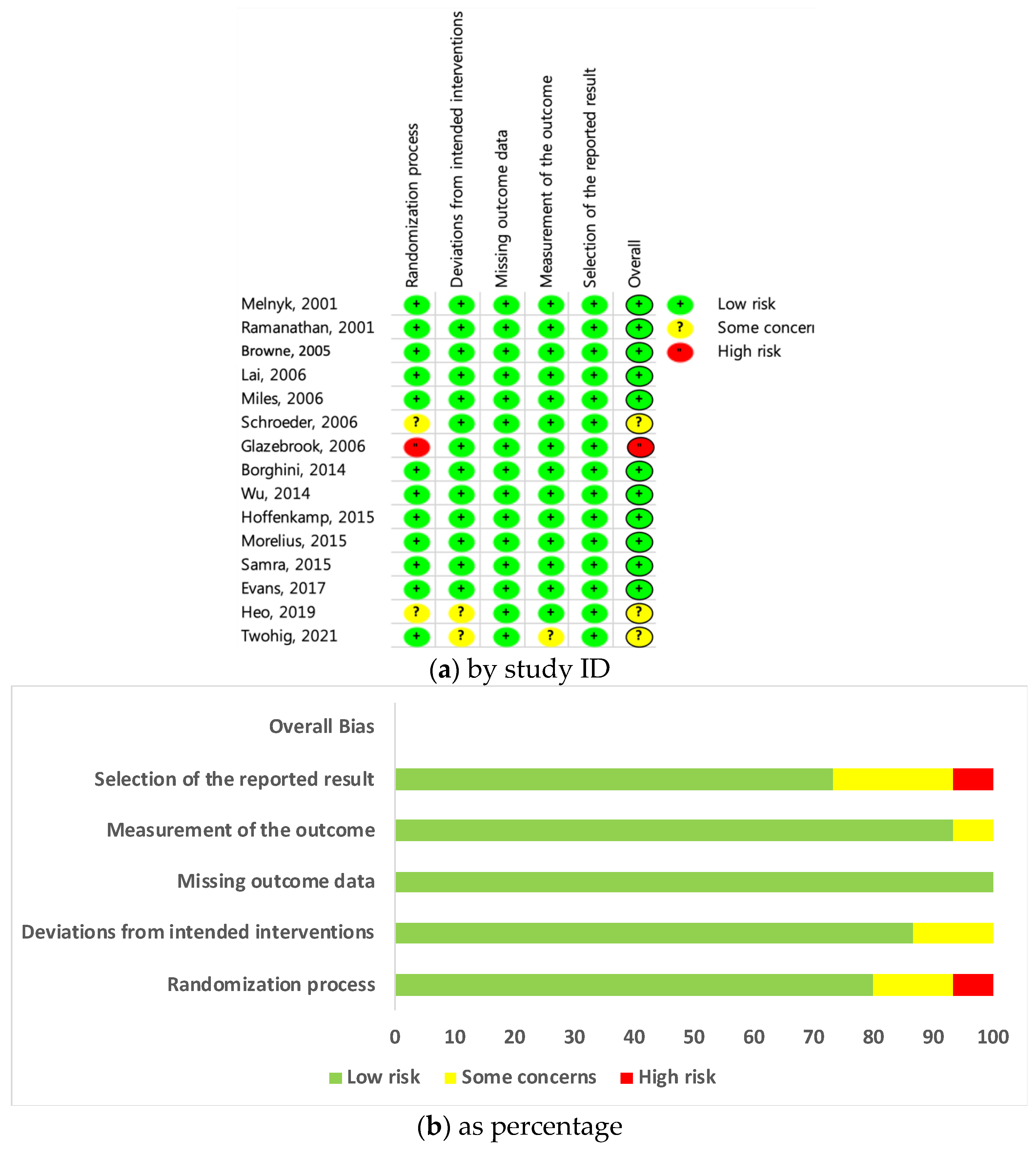
3.1.4. Quality Assessment of the Evidence
3.1.5. Intervention Components
3.2. Synthesis of Results
3.2.1. Effects of Interventions on Attachment/Bonding
3.2.2. Effects of Interventions on Mother–Infant Interactions
3.2.3. Effects of Interventions on Anxiety
3.2.4. Effects of Interventions on Parental Environmental Stress
3.2.5. Effects of Interventions on Maternal Traumatic Stress
3.2.6. Effects of Interventions on Maternal Depression
3.2.7. Effects of Interventions on Infants’ Weight Growth
3.2.8. Effects of Interventions on Infants’ Development
3.3. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feldman, R. The neurobiology of human attachments. Trends Cogn. Sci. 2017, 21, 80–99. [Google Scholar] [CrossRef]
- Junewicz, A.; Billick, S.B. Nature, nurture, and attachment: Implications in light of expanding definitions of parenthood. Psychiat. Quart. 2018, 89, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Ettenberger, M.; Bieleninik, L.; Epstein, S.; Elefant, C. Defining attachment and bonding: Overlaps, differences and implications for music therapy clinical practice and research in the neonatal intensive care unit (NICU). Int. J. Environ. Res. Public Health 2021, 18, 1733. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.R.; Kim, S.Y.; Yun, J.E. Attachment and relationship-based interventions for families during neonatal intensive care hospitalization: A study protocol for a systematic review and meta-analysis. Syst. Rev. 2020, 9, 61. [Google Scholar] [CrossRef]
- López-Maestro, M.; Sierra-Garcia, P.; Diaz-Gonzalez, C.; Torres-Valdivieso, M.J.; Lora-Pablos, D.; Ares-Segura, S.; Pallás-Alonso, C.R. Quality of attachment in infants less than 1500 g or less than 32 weeks. Related factors. Early Hum. Dev. 2017, 104, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Pennestri, M.H.; Gaudreau, H.; Bouvette-Turcot, A.A.; Moss, E.; Lecompte, V.; Atkinson, L.; Lydon, J.; Steiner, M.; Meaney, M.J.; Mavan Research Team. Attachment disorganization among children in neonatal intensive care unit: Preliminary results. Early Hum. Dev. 2015, 91, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Givrad, S.; Hartzell, G.; Scala, M. Promoting infant mental health in the neonatal intensive care unit (NICU): A review of nurturing factors and interventions for NICU infant-parent relationships. Early Hum. Dev. 2020, 154, 105281. [Google Scholar] [CrossRef]
- Kim, A.R.; Tak, Y.R.; Shin, Y.S.; Yun, E.H.; Park, H.K.; Lee, H.J. Mothers’ perceptions of quality of family-centered care and environmental stressors in neonatal intensive care units: Predictors of and relationships with psycho-emotional outcomes and postpartum attachment. Matern. Child Health J. 2020, 24, 601–611. [Google Scholar] [CrossRef]
- Grunberg, V.A.; Geller, P.A.; Bonacquisti, A.; Patterson, C.A. NICU infant health severity and family outcomes: A systematic review of assessments and findings in psychosocial research. J. Perinatol. 2019, 39, 156–172. [Google Scholar] [CrossRef]
- Mountain, G.; Cahill, J.; Thorpe, H. Sensitivity and attachment interventions in early childhood: A systematic review and meta-analysis. Infant Behav. Dev. 2017, 46, 14–32. [Google Scholar] [CrossRef]
- Wright, B.; Edginton, E. Evidence-based parenting interventions to promote secure attachment: Findings from a systematic review and meta-analysis. Glob. Pediatr. Health 2016, 3, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Rayce, S.B.; Rasmussen, I.S.; Klest, S.K.; Patras, J.; Pontoppidan, M. Effects of parenting interventions for at-risk parents with infants: A systematic review and meta-analyses. BMJ Open 2017, 7, e015707. [Google Scholar] [CrossRef] [Green Version]
- Bialoskurski, M.; Cox, C.L.; Hayes, J.A. The nature of attachment in a neonatal intensive care unit. J. Perinat. Neonatal Nurs. 1999, 13, 66–77. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Wiley: Hoboken, NJ, USA, 2019. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [Green Version]
- Browne, J.V.; Talmi, A. Family-based intervention to enhance infant-parent relationships in the neonatal intensive care unit. J. Pediatr. Psychol. 2005, 30, 667–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.C.; Leng, C.H.; Hsieh, W.S.; Hsu, C.H.; Chen, W.J.; Gau, S.S.F.; Chiu, N.C.; Yang, M.C.; Fang, L.J.; Hsu, H.C.; et al. A randomized controlled trial of clinic-based and home-based interventions in comparison with usual care for preterm infants: Effects and mediators. Res. Dev. Disabil. 2014, 35, 2384–2393. [Google Scholar] [CrossRef] [PubMed]
- Melnyk, B.M.; Alpert-Gillis, L.; Feinstein, N.F.; Fairbanks, E.; Schultz-Czarniak, J.; Hust, D.; Sherman, L.; LeMoine, C.; Moldenhauer, Z.; Small, L.; et al. Improving cognitive development of low-birth-weight premature infants with the COPE program: A pilot study of the benefit of early NICU intervention with mothers. Res. Nurs. Health 2001, 24, 373–389. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, K.; Paul, V.K.; Deorari, A.K.; Taneja, U.; George, G. Kangaroo mother care in very low birth weight infants. Indian J. Pediatr. 2001, 68, 1019–1023. [Google Scholar] [CrossRef]
- Lai, H.L.; Chen, C.J.; Peng, T.C.; Chang, F.M.; Hsieh, M.L.; Huang, H.Y.; Chang, S.C. Randomized controlled trial of music during kangaroo care on maternal state anxiety and preterm infants’ responses. Int. J. Nurs. Stud. 2006, 43, 139–146. [Google Scholar] [CrossRef]
- Miles, R.; Cowan, F.; Glover, V.; Stevenson, J.; Modi, N. A controlled trial of skin-to-skin contact in extremely preterm infants. Early Hum. Dev. 2006, 82, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, M.; Pridham, K. Development of relationship competencies through guided participation for mothers of preterm infants. J. Obstet. Gynecol. Neonatal Nurs. 2006, 35, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Glazebrook, C.; Marlow, N.; Israel, C.; Croudace, T.; Johnson, S.; White, I.R.; Whitelaw, A. Randomised trial of a parenting intervention during neonatal intensive care. Arch. Dis. Child Fetal Neonatal Ed. 2007, 92, 438–443. [Google Scholar] [CrossRef]
- Borghini, A.; Habersaat, S.; Forcada-Guex, M.; Nessi, J.; Pierrehumbert, B.; Ansermet, F.; Müller-Nix, C. Effects of an early intervention on maternal post-traumatic stress symptoms and the quality of mother-infant interaction: The case of preterm birth. Infant Behav. Dev. 2014, 37, 624–631. [Google Scholar] [CrossRef]
- Hoffenkamp, H.N.; Tooten, A.; Hall, R.A.S.; Braeken, J.; Eliëns, M.P.J.; Vingerhoets, A.J.J.M.; van Bakel, H.J.A. Effectiveness of hospital-based video interaction guidance on parental interactive behavior, bonding, and stress after preterm birth: A randomized controlled trial. J. Consult. Clin. Psychol. 2015, 83, 416–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mörelius, E.; Örtenstrand, A.; Theodorsson, E.; Frostell, A. A randomised trial of continuous skin-to-skin contact after preterm birth and the effects on salivary cortisol, parental stress, depression, and breastfeeding. Early Hum. Dev. 2015, 91, 63–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samra, H.A.; Dutcher, J.; McGrath, J.M.; Foster, M.; Klein, L.; Djira, G.; Hansen, J.; Wallenburg, D. Effect of skin-to-skin holding on stress in mothers of late-preterm infants: A randomized controlled trial. Adv. Neonatal Care 2015, 15, 354–364. [Google Scholar] [CrossRef]
- Evans, T.; Boyd, R.N.; Colditz, P.; Sanders, M.; Whittingham, K. Mother-very preterm infant relationship quality: RCT of baby triple P. J. Child Fam. Stud. 2017, 26, 284–295. [Google Scholar] [CrossRef]
- Heo, Y.J.; Oh, W.O. The effectiveness of a parent participation improvement program for parents on partnership, attachment infant growth in a neonatal intensive care unit: A randomized controlled trial. Int. J. Nurs. Stud. 2019, 95, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Twohig, A.; Murphy, J.F.; McCarthy, A.; Segurado, R.; Underdown, A.; Smyke, A.; McNicholas, F.; Molloy, E.J. The preterm infant–parent programme for attachment—PIPPA Study: A randomised controlled trial. Pediatr. Res. 2021, 90, 617–624. [Google Scholar] [CrossRef]
- Benzies, K.M.; Magill-Evans, J.E.; Hayden, K.A.; Ballantyne, M. Key components of early intervention programs for preterm infants and their parents: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2013, 13, S10. [Google Scholar] [CrossRef] [Green Version]
- Lee, J. Meta-analysis. J. Korean Endocr. Soc. 2008, 23, 361–378. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavallée, A.; De Clifford-Faugère, G.; Ballard, A.; Aita, M. Parent–infant interventions to promote parental sensitivity during NICU hospitalization: Systematic review and meta-analysis. J. Early Interv. 2021, 1–22. [Google Scholar] [CrossRef]
- Crittenden, P.M. A dynamic-maturational model of attachment. Aust. N. Z. J. Fam. Ther. 2006, 27, 105–115. [Google Scholar] [CrossRef]
- Ding, X.; Zhu, L.; Zhang, R.; Wang, L.; Wang, T.T.; Latour, J.M. Effects of family-centred care interventions on preterm infants and parents in neonatal intensive care units: A systematic review and meta-analysis of randomised controlled trials. Aust. Crit. Care 2019, 32, 63–75. [Google Scholar] [CrossRef]
- Mendelson, T.; Cluxton-Keller, F.; Vullo, G.C.; Tandon, S.D.; Noazin, S. NICU-based interventions to reduce maternal depressive and anxiety symptoms: A meta-analysis. Pediatrics 2017, 139, e20161870. [Google Scholar] [CrossRef] [Green Version]
- Burke, S. Systematic review of developmental care interventions in the neonatal intensive care unit since 2006. J. Child Health Care 2018, 22, 269–286. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Kim, J.H. Proceed with caution when using real world data and real world evidence. J. Korean Med. Sci. 2019, 34, e28. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| First Author (Year) | Risk of Bias | Country of Study | No. of Centers (n) | Infants Enrolled (n) | Group Allocation | Mean Gestational Age (Weeks) | Mean Birth Weight (Grams) | Follow Up | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| I a/I b | C/R c | I a/I b | C/R c | I a/I b | C/R c | ||||||
| Melnyk et al. (2001) [19] | Low | United States | 1 | 42 | 20 | 22 | 31.4 | 31.6 | 1482.7 | 1731.0 | |
| Ramanathan Paul, Deorari, Taneja, and George (2001) [20] | Low | India | 1 | 24 | 14 | 14 | (median) 30.4 | (median) 30.9 | 1219.0 | 1270.9 | |
| Browne and Talmi (2005) [17] | Low | United States | 1 | 84 | 28 a/31 b | 25 | 32.0 a/31.2 b | 31 | 1617.4 a/ 1509.3 b | 1518.0 | |
| Lai et al. (2006) [21] | Low | Taiwan | 2 | 30 | 15 | 15 | 33.8 | 2248 | |||
| Miles, Cowan, Glover, Stevenson, and Modi (2006) [22] | Low | United Kingdom | 2 | 78 | 42 | 32 | 28 | 28 | 1086 | 1133 | |
| Schroeder and Pridham (2006) [23] | Some concerns | United States | 2 | 16 | 8 | 8 | 26.8 | 27.5 | 828 | 1049 | |
| Glazebrook et al. (2007) [24] | High | United Kingdom | 6 | 210 | 99 | 111 | 20 | 21 | (median) 1120 | (median) 1220 | |
| Borghini et al. (2014) [25] | Low | Switzerland | 1 | 83 | 30 | 30/23 c | 30 | 30/39 c | 1343 | 1435/3281 | 12 months CA |
| Wu et al. (2014) [18] | Low | Taiwan | 3 | 178 | 57 a/63 b | 58 | 30.0 a/29.9 b | 29.3 | 1179 a/1149 b | 1091 | 24 months |
| Hoffenkamp et al. (2015) [26] | Low | Netherlands | 7 | 150 | 75 | 75 | 32 | 32 | 1828 | 1770 | at 1, 3, and 6 months postpartum |
| Mörelius, Örtenstrand, Theodorsson, and Frostell (2015) [27] | Low | Sweden | 2 | 42 | 23 | 19 | 34 | 34 | 2468 | 2512 | at 1 and 4 months CA |
| Samra et al. (2015) [28] | Low | United States | 1 | 40 | 20 | 20 | 35 | 35.5 | 2493 | 2693.8 | at discharge |
| Evans, Boyd, Colditz, Sanders, and Whittingham (2017) [29] | Low | Australia | 2 | 145 | 75 | 70 | 28.51 | 28.55 | 1159.3 | 1107.8 | at 12 months CA |
| Heo and Oh (2019) [30] | Some concerns | South Korea | 1 | 66 | 33 | 33 | 28.42 | 29.75 | 1139.6 | 1228.1 | |
| Twohig et al. (2021) [31] | Some concerns | Ireland | 1 | 80 | 42 | 38 | 28.4 | 28.3 | 1179 | 1176 | at 6,9, and 12 months CA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-Y.; Kim, A.R. Attachment- and Relationship-Based Interventions during NICU Hospitalization for Families with Preterm/Low-Birth Weight Infants: A Systematic Review of RCT Data. Int. J. Environ. Res. Public Health 2022, 19, 1126. https://doi.org/10.3390/ijerph19031126
Kim S-Y, Kim AR. Attachment- and Relationship-Based Interventions during NICU Hospitalization for Families with Preterm/Low-Birth Weight Infants: A Systematic Review of RCT Data. International Journal of Environmental Research and Public Health. 2022; 19(3):1126. https://doi.org/10.3390/ijerph19031126
Chicago/Turabian StyleKim, Soo-Yeon, and Ah Rim Kim. 2022. "Attachment- and Relationship-Based Interventions during NICU Hospitalization for Families with Preterm/Low-Birth Weight Infants: A Systematic Review of RCT Data" International Journal of Environmental Research and Public Health 19, no. 3: 1126. https://doi.org/10.3390/ijerph19031126