
The Influence of Acute Sprint Interval Training on Cognitive Performance of Healthy Younger Adults

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
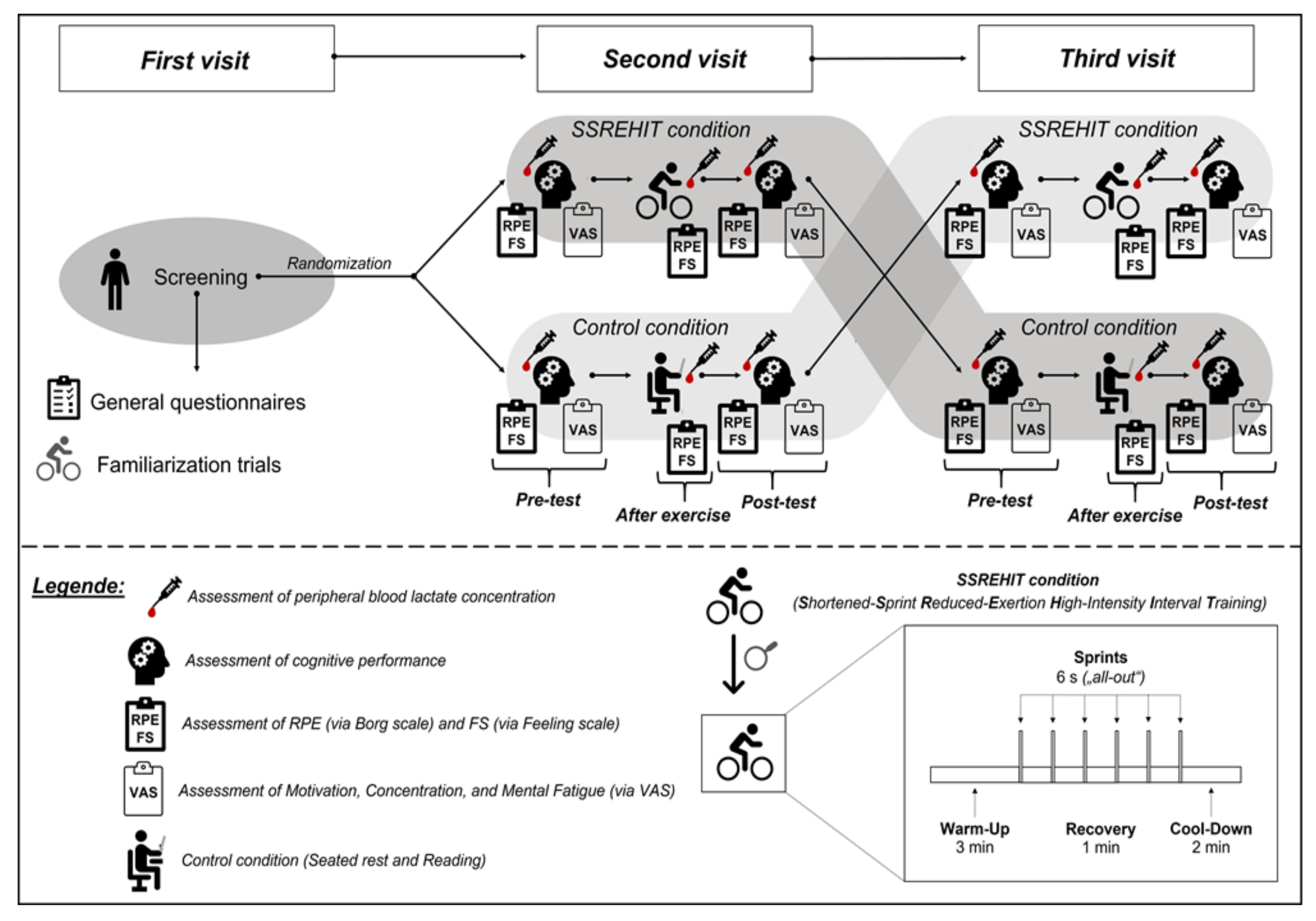
2.2. Study Design
2.3. Study Conditions
2.4. Outcomes
2.4.1. Primary Outcomes—Measures of Cognitive Performance
2.4.2. Secondary Outcomes—Psychological Parameters
2.4.3. Secondary Outcomes—Physiological Parameters
2.5. Statistical Analysis
3. Results
3.1. Cognitive Performance
3.2. Psychological and Physiological Parameters
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chang, Y.K.; Labban, J.D.; Gapin, J.I.; Etnier, J.L. The effects of acute exercise on cognitive performance: A meta-analysis. Brain Res. 2012, 1453, 87–101. [Google Scholar] [CrossRef] [Green Version]
- Pontifex, M.B.; McGowan, A.L.; Chandler, M.C.; Gwizdala, K.L.; Parks, A.C.; Fenn, K.; Kamijo, K. A primer on investigating the after effects of acute bouts of physical activity on cognition. Psychol. Sport. Exerc. 2019, 40, 1–22. [Google Scholar] [CrossRef]
- Ludyga, S.; Gerber, M.; Brand, S.; Holsboer-Trachsler, E.; Pühse, U. Acute effects of moderate aerobic exercise on specific aspects of executive function in different age and fitness groups: A meta-analysis. Psychophysiology 2016, 53, 1611–1626. [Google Scholar] [CrossRef]
- Allison, K.R.; Dwyer, J.J.; Makin, S. Perceived barriers to physical activity among high school students. Prev. Med. 1999, 28, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Arzu, D.; Tuzun, E.H.; Eker, L. Perceived barriers to physical activity in university students. J. Sports Sci. Med. 2006, 5, 615–620. [Google Scholar]
- Gjestvang, C.; Abrahamsen, F.; Stensrud, T.; Haakstad, L.A.H. Motives and barriers to initiation and sustained exercise adherence in a fitness club setting-A one-year follow-up study. Scand. J. Med. Sci. Sports 2020, 30, 1796–1805. [Google Scholar] [CrossRef]
- Herazo-Beltrán, Y.; Pinillos, Y.; Vidarte, J.; Crissien, E.; Suarez, D.; García, R. Predictors of perceived barriers to physical activity in the general adult population: A cross-sectional study. Braz. J. Phys. Ther. 2017, 21, 44–50. [Google Scholar] [CrossRef] [PubMed]
- El Masri, A.; Kolt, G.S.; George, E.S. The perceptions, barriers and enablers to physical activity and minimising sedentary behaviour among Arab-Australian adults aged 35-64 years. Health Promot. J. Austr. 2021, 32, 312–321. [Google Scholar] [CrossRef]
- Sørensen, M.; Gill, D.L. Perceived barriers to physical activity across Norwegian adult age groups, gender and stages of change. Scand. J. Med. Sci. Sports 2008, 18, 651–663. [Google Scholar] [CrossRef]
- Vollaard, N.B.J.; Metcalfe, R.S. Research into the health benefits of sprint interval training should focus on protocols with fewer and shorter sprints. Sports Med. 2017, 47, 2443–2451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle. Part II: Anaerobic energy, neuromuscular load and practical applications. Sports Med. 2013, 43, 927–954. [Google Scholar] [CrossRef] [PubMed]
- Sloth, M.; Sloth, D.; Overgaard, K.; Dalgas, U. Effects of sprint interval training on VO2max and aerobic exercise performance: A systematic review and meta-analysis. Scand. J. Med. Sci. Sports 2013, 23, e341–e352. [Google Scholar] [CrossRef]
- Viana, R.B.; Lira, C.A.B.; de Naves, J.P.A.; Coswig, V.S.; Del Vecchio, F.B.; Ramirez-Campillo, R.; Vieira, C.A.; Gentil, P. Can we draw general conclusions from interval training studies? Sports Med. 2018, 48, 2001–2009. [Google Scholar] [CrossRef] [PubMed]
- Burgomaster, K.A.; Howarth, K.R.; Phillips, S.M.; Rakobowchuk, M.; Macdonald, M.J.; McGee, S.L.; Gibala, M.J. Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. J. Physiol. 2008, 586, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Gillen, J.B.; Martin, B.J.; MacInnis, M.J.; Skelly, L.E.; Tarnopolsky, M.A.; Gibala, M.J. Twelve Weeks of Sprint Interval Training Improves Indices of Cardiometabolic Health Similar to Traditional Endurance Training despite a Five-Fold Lower Exercise Volume and Time Commitment. PLoS One 2016, 11, e0154075. [Google Scholar] [CrossRef]
- Cooper, S.B.; Bandelow, S.; Nute, M.L.; Dring, K.J.; Stannard, R.L.; Morris, J.G.; Nevill, M.E. Sprint-based exercise and cognitive function in adolescents. Prev. Med. Rep. 2016, 4, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Kujach, S.; Olek, R.A.; Byun, K.; Suwabe, K.; Sitek, E.J.; Ziemann, E.; Laskowski, R.; Soya, H. Acute sprint interval exercise increases both cognitive functions and peripheral neurotrophic factors in humans: The possible involvement of lactate. Front. Neurosci. 2020, 13, 539. [Google Scholar] [CrossRef]
- Vollaard, N.B.J.; Metcalfe, R.S.; Williams, S. Effect of number of sprints in an SIT session on change in V’O2max: A meta-analysis. Med. Sci. Sports Exerc. 2017, 49, 1147–1156. [Google Scholar] [CrossRef]
- Haines, M.; Broom, D.; Gillibrand, W.; Stephenson, J. Effects of three low-volume, high-intensity exercise conditions on affective valence. J. Sports Sci. 2020, 38, 121–129. [Google Scholar] [CrossRef]
- Townsend, L.K.; Islam, H.; Dunn, E.; Eys, M.; Robertson-Wilson, J.; Hazell, T.J. Modified sprint interval training protocols. Part II. Psychological responses. Appl. Physiol. Nutr. Metab. 2017, 42, 347–353. [Google Scholar] [CrossRef] [Green Version]
- Haines, M. Feasibility of procedures for a randomised pilot study of reduced exertion, high-intensity interval training (REHIT) with non-diabetic hyperglycaemia patients. Pilot Feasibility Stud. 2020, 6, 28. [Google Scholar] [CrossRef]
- Haines, M.; Broom, D.; Stephenson, J.; Gillibrand, W. Influence of sprint duration during minimal volume exercise on aerobic capacity and affect. Int. J. Sports Med. 2020, 42, 357–364. [Google Scholar] [CrossRef]
- Cuddy, T.F.; Ramos, J.S.; Dalleck, L.C. Reduced exertion high-intensity interval training is more effective at improving cardiorespiratory fitness and cardiometabolic health than traditional moderate-intensity continuous training. Int. J. Environ. Res. Public Health 2019, 16, 483. [Google Scholar] [CrossRef] [Green Version]
- Metcalfe, R.S.; Tardif, N.; Thompson, D.; Vollaard, N.B.J. Changes in aerobic capacity and glycaemic control in response to reduced-exertion high-intensity interval training (REHIT) are not different between sedentary men and women. Appl. Physiol. Nutr. Metab. 2016, 41, 1117–1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metcalfe, R.S.; Babraj, J.A.; Fawkner, S.G.; Vollaard, N.B.J. Towards the minimal amount of exercise for improving metabolic health: Beneficial effects of reduced-exertion high-intensity interval training. Eur. J. Appl. Physiol. 2012, 112, 2767–2775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamson, S.; Kavaliauskas, M.; Lorimer, R.; Babraj, J. The impact of sprint interval training frequency on blood glucose control and physical function of older adults. Int. J. Environ. Res. Public Health 2020, 17, 454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamson, S.; Lorimer, R.; Cobley, J.N.; Lloyd, R.; Babraj, J. High intensity training improves health and physical function in middle aged adults. Biology 2014, 3, 333–344. [Google Scholar] [CrossRef] [Green Version]
- Adamson, S.B.; Lorimer, R.; Cobley, J.N.; Babraj, J.A. Extremely short-duration high-intensity training substantially improves the physical function and self-reported health status of elderly adults. J. Am. Geriatr. Soc. 2014, 62, 1380–1381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMorris, T. Developing the catecholamines hypothesis for the acute exercise-cognition interaction in humans: Lessons from animal studies. Physiol. Behav. 2016, 165, 291–299. [Google Scholar] [CrossRef] [Green Version]
- McMorris, T.; Turner, A.; Hale, B.J.; Sproule, J. Beyond the Catecholamines Hypothesis for an Acute Exercise–Cognition Interaction. Exercise-Cognition Interaction; Elsevier: Amsterdam, The Netherlands, 2016; pp. 65–103. ISBN 9780128007785. [Google Scholar]
- McMorris, T. The acute exercise-cognition interaction: From the catecholamines hypothesis to an interoception model. Int. J. Psychophysiol. 2021, 170, 75–88. [Google Scholar] [CrossRef]
- Hashimoto, T.; Tsukamoto, H.; Ando, S.; Ogoh, S. Effect of exercise on brain health: The potential role of lactate as a myokine. Metabolites 2021, 11, 813. [Google Scholar] [CrossRef]
- Tsukamoto, H.; Suga, T.; Takenaka, S.; Tanaka, D.; Takeuchi, T.; Hamaoka, T.; Isaka, T.; Ogoh, S.; Hashimoto, T. Repeated high-intensity interval exercise shortens the positive effect on executive function during post-exercise recovery in healthy young males. Physiol. Behav. 2016, 160, 26–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamson, S.; Kavaliauskas, M.; Yamagishi, T.; Phillips, S.; Lorimer, R.; Babraj, J. Extremely short duration sprint interval training improves vascular health in older adults. Sport. Sci. Health 2019, 15, 123–131. [Google Scholar] [CrossRef] [Green Version]
- Dragovic, M. Categorization and validation of handedness using latent class analysis. Acta Neuropsychiatr. 2004, 16, 212–218. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Balady, G.J.; Chaitman, B.; Driscoll, D.; Foster, C.; Froelicher, E.; Gordon, N.; Pate, R.; Rippe, J.; Bazzarre, T. Recommendations for cardiovascular screening, staffing, and emergency policies at health/fitness facilities. Circulation 1998, 97, 2283–2293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, R.; Klaperski, S.; Gerber, M.; Seelig, H. Messung der Bewegungs- und Sportaktivität mit dem BSA-Fragebogen: [Measurement of Physical Activity and Sport Activity with the BSA Questionnaire]. Z. Gesundh. 2015, 23, 60–76. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Li, L.; Yu, Q.; Zhao, W.; Herold, F.; Cheval, B.; Kong, Z.; Li, J.; Mueller, N.; Kramer, A.F.; Cui, J.; et al. Physical activity and inhibitory control: The mediating role of sleep quality and sleep efficiency. Brain Sci. 2021, 11, 664. [Google Scholar] [CrossRef]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test–retest reliability and validity of the pittsburgh sleep quality index in primary insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef]
- Herold, F.; Aye, N.; Lehmann, N.; Taubert, M.; Müller, N.G. The contribution of functional magnetic resonance imaging to the understanding of the effects of acute physical exercise on cognition. Brain Sci. 2020, 10, 175. [Google Scholar] [CrossRef] [Green Version]
- Harris, D.M.; Kendall, K.; Haff, G.G.; Latella, C. Absolute and relative strength, power and physiological characteristics of indian junior national-level judokas. Sports 2020, 8, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herbert, P.; Sculthorpe, N.; Grace, F. Validation of a 6 second cycle test for the determination of Peak Power Output (PPO) using wattbike cycle ergometer. Med. Sci. Sports Exerc. 2015, 47, 933. [Google Scholar] [CrossRef]
- Knowles, A.-M.; Herbert, P.; Easton, C.; Sculthorpe, N.; Grace, F.M. Impact of low-volume, high-intensity interval training on maximal aerobic capacity, health-related quality of life and motivation to exercise in ageing men. Age 2015, 37, 25. [Google Scholar] [CrossRef] [Green Version]
- Sculthorpe, N.F.; Herbert, P.; Grace, F. One session of high-intensity interval training (HIIT) every 5 days, improves muscle power but not static balance in lifelong sedentary ageing men: A randomized controlled trial. Medicine 2017, 96, e6040. [Google Scholar] [CrossRef] [PubMed]
- Yasar, Z.; Dewhurst, S.; Hayes, L.D. Peak power output is similarly recovered after three- and five-days’ rest following sprint interval training in young and older adults. Sports 2019, 7, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wainwright, B.; Cooke, C.B.; O’Hara, J.P. The validity and reliability of a sample of 10 Wattbike cycle ergometers. J. Sports Sci. 2017, 35, 1451–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brickenkamp, R.; Schmidt-Atzert, L.; Liepmann, D. Test d2-Revision: Aufmerksamkeits- und Konzentrationstest; Hogrefe: Göttingen, Germany, 2010. [Google Scholar]
- Budde, H.; Brunelli, A.; Machado, S.; Velasques, B.; Ribeiro, P.; Arias-Carrion, O.; Voelcker-Rehage, C. Intermittent maximal exercise improves attentional performance only in physically active students. Arch. Med. Res. 2012, 43, 125–131. [Google Scholar] [CrossRef]
- Budde, H.; Voelcker-Rehage, C.; Pietrabyk-Kendziorra, S.; Ribeiro, P.; Tidow, G. Acute coordinative exercise improves attentional performance in adolescents. Neuroscience Letters 2008, 441, 219–223. [Google Scholar] [CrossRef]
- Schega, L.; Peter, B.; Törpel, A.; Mutschler, H.; Isermann, B.; Hamacher, D. Effects of intermittent hypoxia on cognitive performance and quality of life in elderly adults: A pilot study. Gerontology 2013, 59, 316–323. [Google Scholar] [CrossRef]
- Cooper, S.B.; Dring, K.J.; Morris, J.G.; Sunderland, C.; Bandelow, S.; Nevill, M.E. High intensity intermittent games-based activity and adolescents’ cognition: Moderating effect of physical fitness. BMC Public Health 2018, 18, 603. [Google Scholar] [CrossRef]
- Alves, C.R.R.; Tessaro, V.H.; Teixeira, L.A.C.; Murakava, K.; Roschel, H.; Gualano, B.; Takito, M.Y. Influence of acute high-intensity aerobic interval exercise bout on selective attention and short-term memory tasks. Percept. Mot. Skills 2014, 118, 63–72. [Google Scholar] [CrossRef]
- Wilke, J.; Stricker, V.; Usedly, S. Free-weight resistance exercise is more effective in enhancing inhibitory control than machine-based training: A randomized, controlled trial. Brain Sci. 2020, 10, 702. [Google Scholar] [CrossRef]
- Wilke, J. Functional high-intensity exercise is more effective in acutely increasing working memory than aerobic walking: An exploratory randomized, controlled trial. Sci Rep 2020, 10, 12335. [Google Scholar] [CrossRef] [PubMed]
- Hardy, C.J.; Rejeski, W.J. Not what, but how one feels: The measurement of affect during exercise. J. Sport Exerc. Psychol. 1989, 11, 304–317. [Google Scholar] [CrossRef]
- Maibach, M.; Niedermeier, M.; Sudeck, G.; Kopp, M. Erfassung unmittelbarer affektiver Reaktionen auf körperliche Aktivität. Z. Sportpsychol. 2020, 27, 4–12. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Hashimoto, T.; Tsukamoto, H.; Takenaka, S.; Olesen, N.D.; Petersen, L.G.; Sørensen, H.; Nielsen, H.B.; Secher, N.H.; Ogoh, S. Maintained exercise-enhanced brain executive function related to cerebral lactate metabolism in men. FASEB J. 2018, 32, 1417–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, W. p < 0.05, < 0.01, < 0.001, < 0.0001, < 0.00001, < 0.000001, or < 0.0000001 …. J. Sport. Health Sci. 2016, 5, 77–79. [Google Scholar] [CrossRef] [Green Version]
- Zhu, W. Sadly, the earth is still round (p < 0.05). J. Sport Health Sci. 2012, 1, 9–11. [Google Scholar] [CrossRef] [Green Version]
- Holm, S. A simple sequentially rejective multiple test procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Fritz, N.E.; McCarthy, C.J.; Adamo, D.E. Handgrip strength as a means of monitoring progression of cognitive decline—A scoping review. Ageing Res. Rev. 2017, 35, 112–123. [Google Scholar] [CrossRef]
- Coolican, H. Research Methods and Statistics In Psychology, 5th ed.; Hodder Education: London, UK, 2009; ISBN 978-0340983447. [Google Scholar]
- Herold, F.; Hamacher, D.; Törpel, A.; Goldschmidt, L.; Müller, N.G.; Schega, L. Does squatting need attention?—A dual-task study on cognitive resources in resistance exercise. PLoS ONE 2020, 15, e0226431. [Google Scholar] [CrossRef] [PubMed]
- Cano-Corres, R.; Sánchez-Álvarez, J.; Fuentes-Arderiu, X. The effect size: Beyond statistical significance. EJIFCC 2012, 23, 19–23. [Google Scholar] [PubMed]
- Volker, M.A. Reporting effect size estimates in school psychology research. Psychol. Schs. 2006, 43, 653–672. [Google Scholar] [CrossRef]
- Bakdash, J.Z.; Marusich, L.R. Repeated measures correlation. Front. Psychol. 2017, 8, 456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, D.; Chou, E. The acute effect of high-intensity exercise on executive function: A meta-analysis. Perspect. Psychol. Sci. 2019, 14, 734–764. [Google Scholar] [CrossRef] [Green Version]
- Stillman, C.M.; Cohen, J.; Lehman, M.E.; Erickson, K.I. Mediators of physical activity on neurocognitive function: A review at multiple levels of analysis. Front. Hum. Neurosci. 2016, 10, 626. [Google Scholar] [CrossRef] [Green Version]
- Herold, F.; Müller, P.; Gronwald, T.; Müller, N.G. Dose-response matters!—A perspective on the exercise prescription in exercise-cognition research. Front. Psychol. 2019, 10, 2338. [Google Scholar] [CrossRef] [Green Version]
- Herold, F.; Wiegel, P.; Scholkmann, F.; Müller, N.G. Applications of functional near-infrared spectroscopy (fnirs) neuroimaging in exercise⁻cognition science: A systematic, methodology-focused review. J. Clin. Med. 2018, 7, 466. [Google Scholar] [CrossRef] [Green Version]
- Hwang, J.; Brothers, R.M.; Castelli, D.M.; Glowacki, E.M.; Chen, Y.T.; Salinas, M.M.; Kim, J.; Jung, Y.; Calvert, H. Acute high-intensity exercise-induced cognitive enhancement and brain-derived neurotrophic factor in young, healthy adults. Neurosci. Lett. 2016, 630, 247–253. [Google Scholar] [CrossRef]
- Törpel, A.; Herold, F.; Hamacher, D.; Müller, N.G.; Schega, L. Strengthening the brain—Is resistance training with blood flow restriction an effective strategy for cognitive improvement? J. Clin. Med. 2018, 7, 337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riske, L.; Thomas, R.K.; Baker, G.B.; Dursun, S.M. Lactate in the brain: An update on its relevance to brain energy, neurons, glia and panic disorder. Ther. Adv. Psychopharmacol. 2017, 7, 85–89. [Google Scholar] [CrossRef] [Green Version]
- Taher, M.; Leen, W.G.; Wevers, R.A.; Willemsen, M.A. Lactate and its many faces. Eur. J. Paediatr. Neurol. 2016, 20, 3–10. [Google Scholar] [CrossRef] [PubMed]
- van Hall, G.; Stromstad, M.; Rasmussen, P.; Jans, O.; Zaar, M.; Gam, C.; Quistorff, B.; Secher, N.H.; Nielsen, H.B. Blood lactate is an important energy source for the human brain. J. Cereb. Blood Flow Metab. 2009, 29, 1121–1129. [Google Scholar] [CrossRef]
- Brooks, G.A. The science and translation of lactate shuttle theory. Cell Metab. 2018, 27, 757–785. [Google Scholar] [CrossRef] [Green Version]
- Quistorff, B.; Secher, N.H.; van Lieshout, J.J. Lactate fuels the human brain during exercise. FASEB J. 2008, 22, 3443–3449. [Google Scholar] [CrossRef]
- Herold, F.; Törpel, A.; Schega, L.; Müller, N.G. Functional and/or structural brain changes in response to resistance exercises and resistance training lead to cognitive improvements—A systematic review. Eur. Rev. Aging Phys. Act. 2019, 16, 1676. [Google Scholar] [CrossRef]
- Brooks, G.A. Lactate as a fulcrum of metabolism. Redox Biol. 2020, 35, 101454. [Google Scholar] [CrossRef] [PubMed]
- Brooks, G.A. The tortuous path of lactate shuttle discovery: From cinders and boards to the lab and ICU. J. Sport. Health Sci. 2020, 9, 446–460. [Google Scholar] [CrossRef]
- Brooks, G.A.; Arevalo, J.A.; Osmond, A.D.; Leija, R.G.; Curl, C.C.; Tovar, A.P. Lactate in contemporary biology: A phoenix risen. J Physiol 2021, 1–23, in press. [Google Scholar] [CrossRef]
- Coco, M.; Di Corrado, D.; Calogero, R.A.; Perciavalle, V.; Maci, T.; Perciavalle, V. Attentional processes and blood lactate levels. Brain Res. 2009, 1302, 205–211. [Google Scholar] [CrossRef]
- Coco, M.; Buscemi, A.; Guerrera, C.S.; Di Corrado, D.; Cavallari, P.; Zappalà, A.; Di Nuovo, S.; Parenti, R.; Maci, T.; Razza, G.; et al. Effects of a bout of intense exercise on some executive functions. Int. J. Environ. Res. Public Health 2020, 17, 898. [Google Scholar] [CrossRef] [Green Version]
- Johnson, L.; Crawford, L.; Zou, L.; Loprinzi, P.D. Experimental effects of acute exercise in attenuating memory interference: Considerations by biological sex. Medicina 2019, 55, 331. [Google Scholar] [CrossRef] [Green Version]
- Loprinzi, P.D.; Frith, E. The role of sex in memory function: Considerations and recommendations in the context of exercise. J. Clin. Med. 2018, 7, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, C.-L.; Chen, F.-C.; Pan, C.-Y.; Wang, C.-H.; Huang, T.-H.; Chen, T.-C. Impact of acute aerobic exercise and cardiorespiratory fitness on visuospatial attention performance and serum BDNF levels. Psychoneuroendocrinology 2014, 41, 121–131. [Google Scholar] [CrossRef]
- Tsai, C.-L.; Pan, C.-Y.; Chen, F.-C.; Wang, C.-H.; Chou, F.-Y. Effects of acute aerobic exercise on a task-switching protocol and brain-derived neurotrophic factor concentrations in young adults with different levels of cardiorespiratory fitness. Exp. Physiol. 2016, 101, 836–850. [Google Scholar] [CrossRef] [Green Version]
- Tsai, C.-L.; Ukropec, J.; Ukropcová, B.; Pai, M.-C. An acute bout of aerobic or strength exercise specifically modifies circulating exerkine levels and neurocognitive functions in elderly individuals with mild cognitive impairment. Neuroimage Clin. 2018, 17, 272–284. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.-L.; Wang, C.-H.; Pan, C.-Y.; Chen, F.-C.; Huang, T.-H.; Chou, F.-Y. Executive function and endocrinological responses to acute resistance exercise. Front. Behav. Neurosci. 2014, 8, 262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, S.-S.; Huang, C.-J.; Wu, C.-T.; Chang, Y.-K.; Hung, T.-M. Acute exercise facilitates the N450 inhibition marker and P3 attention marker during stroop test in young and older adults. J. Clin. Med. 2018, 7, 391. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| General Characteristics of the Participants | Mean ± Standard Deviation | Exercise Characteristics | Mean ± Standard Deviation |
|---|---|---|---|
| Education level (in years) | 15.21 ± 1.69 | (1) Sprint RPP (in W/kg)/PC (rpm) | 12.90 ± 3.12/115.37 ± 14.37 |
| BDI-II (total score) | 3.63 ± 2.52 | (2) Sprint RPP (in W/kg)/PC (rpm) | 12.87 ± 2.91/115.11 ± 13.98 |
| EHI (score) | 89.21 ± 15.34 | (3) Sprint RPP (in W/kg)/PC (rpm) | 12.69 ± 2.63/114.37 ± 12.92 |
| BSA PA (in min per week) | 371.91 ± 218.18 | (4) Sprint RPP (in W/kg)/PC (rpm) | 12.34 ± 2.48/113.37 ± 12.41 |
| BSA PE (in min per week) | 292.30 ± 232.46 | (5) Sprint RPP (in W/kg)/PC (rpm) | 11.95 ± 2.34/112.37 ± 12.00 |
| PSQI (global score) | 5.11 ± 2.61 a | (6) Sprint RPP (in W/kg)/PC (rpm) | 11.88 ± 2.21/112.00 ± 11.14 |
| SSREHIT Condition | Control Condition | |||||
|---|---|---|---|---|---|---|
| Pretest | Posttest | Delta Score | Pretest | Posttest | Delta Score | |
| GZ (score) | 558.90 (91.46) | 608.63 (77.22) | 49.74 (31.70) | 563.58 (87.96) | 596.16 (75.03) | 32.58 (29.78) |
| SKL (score) | 234.90 (48.27) | 267.68 (41.55) | 32.79 (21.92) | 241.47 (48.62) | 260.16 (39.52) | 18.68 (16.60) |
| F% (score) | 2.29 (2.34) | 0.96 (1.05) | −1.33 (1.74) * | 1.21 (1.16) | 0.88 (0.99) | −0.33 (0.63) * |
| DSF (pts) | 10.37 (1.64) | 10.37 (1.89) | 0.00 (1.89) | 10.11 (1.66) | 10.90 (1.80) | 0.79 (1.36) |
| DSB (pts) | 7.47 (2.09) | 7.74 (2.02) | 0.26 (1.52) | 7.47 (2.17) | 7.84 (2.12) | 0.37 (1.46) |
| SSREHIT Condition | Control Condition | |||||
|---|---|---|---|---|---|---|
| Pretest | After Exercise | Posttest | Pretest | After Exercise | Posttest | |
| RPE (Borg scale) | 6.00 (0.00) | 16.00 (3.00) # | 11.00 (3.50) #,† | 6.0 (0.00) | 6.00 (0.00) * | 6.00 (0.00) * |
| Feeling scale | 3.00 (2.50) | 2.00 (1.00) | 2.00 (3.00) | 3.00 (2.00) | 4.00 (2.00) * | 3.00 (2.00) * |
| VAS (Motivation) (in mm) | 80.00 (17.50) | n.a. | 75.00 (17.00) | 80.00 (15.00) | n.a. | 80.00 (19.50) |
| VAS (Concentration) (in mm) | 75.00 (27.50) | n.a. | 75.00 (29.00) | 70.00 (18.50) | n.a. | 80.00 (15.00) |
| VAS (Mental fatigue) (in mm) | 30.00 (37.50) | n.a. | 30.00 (34.50) | 30.00 (35.00) | n.a. | 30.00 (30.50) |
| Peripheral blood lactate concentration (in mmol/L) | 0.97 (0.49) | 9.11 (6.03) # | 6.21 (6.19) #,† | 1.08 (0.61) | 0.63 (0.50) * | 0.57 (0.62) *,# |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herold, F.; Behrendt, T.; Meißner, C.; Müller, N.G.; Schega, L. The Influence of Acute Sprint Interval Training on Cognitive Performance of Healthy Younger Adults. Int. J. Environ. Res. Public Health 2022, 19, 613. https://doi.org/10.3390/ijerph19010613
Herold F, Behrendt T, Meißner C, Müller NG, Schega L. The Influence of Acute Sprint Interval Training on Cognitive Performance of Healthy Younger Adults. International Journal of Environmental Research and Public Health. 2022; 19(1):613. https://doi.org/10.3390/ijerph19010613
Chicago/Turabian StyleHerold, Fabian, Tom Behrendt, Caroline Meißner, Notger G. Müller, and Lutz Schega. 2022. "The Influence of Acute Sprint Interval Training on Cognitive Performance of Healthy Younger Adults" International Journal of Environmental Research and Public Health 19, no. 1: 613. https://doi.org/10.3390/ijerph19010613