
The Prevalence and Severity of Sick Leave due to Low Back Disorders among Workers in Slovenia: Analysis of National Data across Gender, Age and Classification of Economic Activities


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Classification of Economic Activities
2.3. Outcome Measures
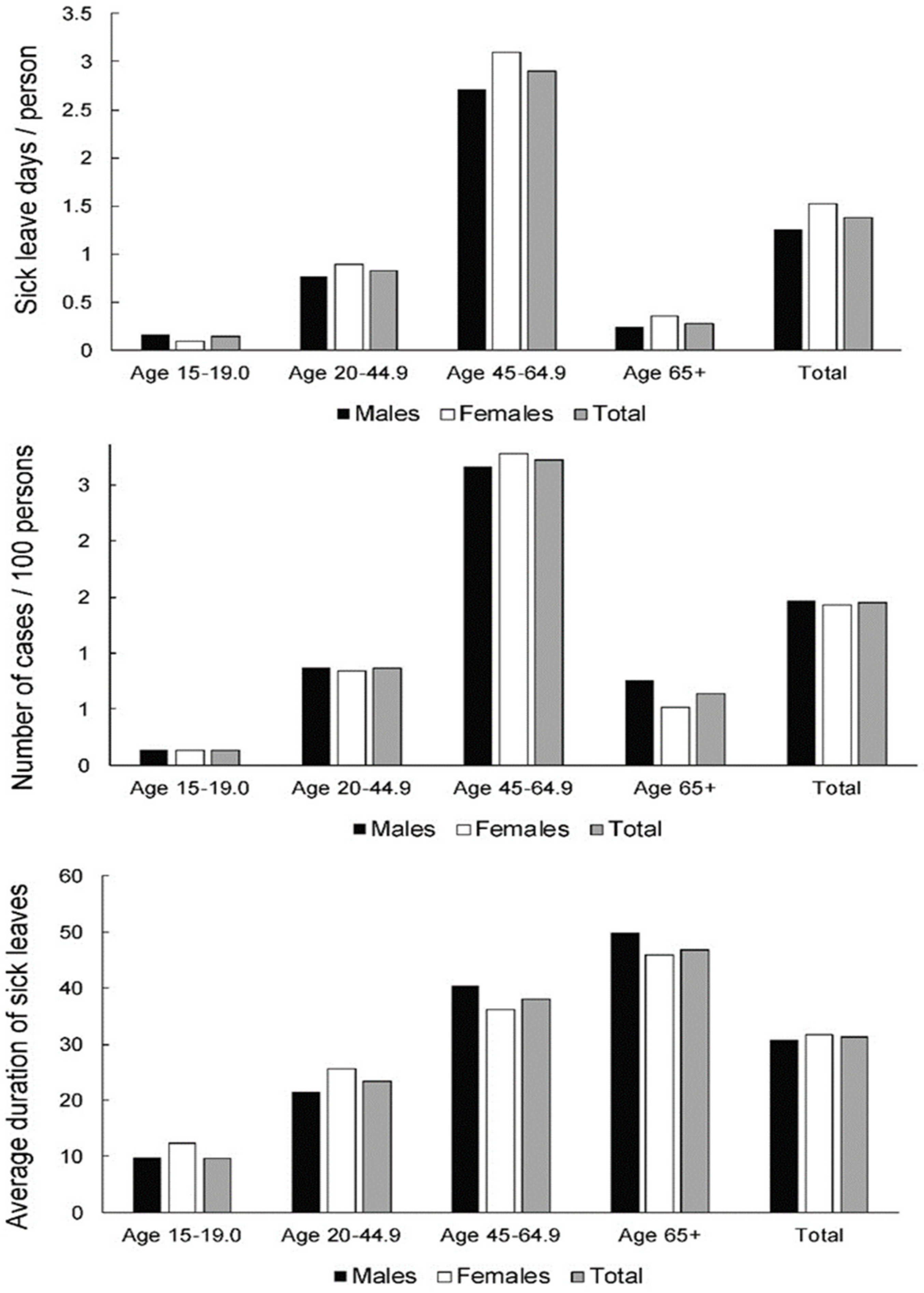
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Kok, J.; VroonHhof, P.; Snijders, J.; Roullis, G.; Clark, M.; Peerebom, K.; van Dorst, P.; Isusi, I. European Agency for Safety and Health at Work: Work-related musculoskeletal disorders: Prevalence, costs and demographics in the EU European Risk Observatory Report. Available online: https://osha.europa.eu/en/publications/summary-msds-facts-and-figures-overview-prevalence-costs-and-demographics-msds-europe/view (accessed on 10 November 2021).
- CDC Work-Related Musculoskeletal Disorders & Ergonomics. Available online: https://www.cdc.gov/workplacehealthpromotion/health-strategies/musculoskeletal-disorders/index.html (accessed on 8 November 2021).
- EU OSHA Discussion Paper: Return to Work after MSD-Related Sick Leave in the Context of Psychosocial Risk at Work. Available online: https://osha.europa.eu/en/publications/return-work-after-msd-related-sick-leave-context-psychosocial-risks-work/view (accessed on 2 November 2021).
- WHO Musculoskeletal Conditions. Available online: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions (accessed on 2 November 2021).
- Shannan, E.M. Work disabilities and musculoskeletal disease. Int. J. Rheum. Dis. 2019, 22, 965–966. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions on a EU Strategic Framework on Health and Safety at Work 2014–2020. Available online: https://eur-lex.europa.eu/legal-content/EN/ALL/?uri=CELEX:52014DC0332 (accessed on 2 November 2021).
- Prijon, T. Najpogostejša z Delom Povezana Kostno-Mišična Obolenja po Anatomskih Regijah. Primerjalna Analiza Zdravstvenega Absentizma v Letih 2015 in 2019. Available online: https://nijz.si/sites/www.nijz.si/files/uploaded/pkmo_najpogostejsa-kmo-po-anatomskih-regijah.pdf (accessed on 2 November 2021).
- Prijon, T. Zdravstveni Absentizem Zaradi z Delom Povezanih Kostno-Mišičnih Obolenj in Duševnih Stresnih Motenj v Sloveniji. Primerjalna Analiza Začasne Nezmožnosti za Delo v Letih 2015 in 2019 v Okviru Projekta “Promocija Aktivnosti za Preprečevanje Kostno-Mišičnih. Available online: https://nijz.si/sites/www.nijz.si/files/uploaded/pkmo_analiza_bs_zaradi_z_delom_povezanih_kmo_in_dusevnih-stresnih_motenj.pdf (accessed on 10 November 2021).
- Hartvigsen, J.; Hancock, M.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Thiese, M.S.; Hegmann, K.T.; Wood, E.M.; Garg, A.; Moore, J.S.; Kapellusch, J.; Foster, J.; Ott, U. Prevalence of low back pain by anatomic location and intensity in an occupational population. BMC Musculoskelet. Disord. 2014, 15, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Fatoye, F.; Gebrye, T.; Odeyemi, I. Real-world incidence and prevalence of low back pain using routinely collected data. Rheumatol. Int. 2019, 39, 619–626. [Google Scholar] [CrossRef] [Green Version]
- Da Costa, B.R.; Vieira, E.R. Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies. Am. J. Ind. Med. 2009, 53, 285–323. [Google Scholar] [CrossRef] [PubMed]
- Petersen, T.; Laslett, M.; Juhl, C.B. Clinical classification in low back pain: Best-evidence diagnostic rules based on systematic reviews. BMC Musculoskelet. Disord. 2017, 18, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Borczuk, P. An evidence-based approach to the evaluation and treatment of low back pain in the emergency department. Emerg. Med. Pr. 2013, 15, 1–23. [Google Scholar]
- Buchbinder, R.; van Tulder, M.; Öberg, B.; Costa, L.M.; Woolf, A.; Schoene, M.; Croft, P.; Lancet Low Back Pain Series Working Group. Low back pain: A call for action. Lancet 2018, 391, 2384–2388. [Google Scholar] [CrossRef]
- Clark, S.; Horton, R. Low back pain: A major global challenge. Lancet 2018, 391, 2302. [Google Scholar] [CrossRef]
- Foster, N.E.; Anema, J.R.; Cherkin, D.; Chou, R.; Cohen, S.P.; Gross, D.P.; Ferreira, P.H.; Fritz, J.M.; Koes, B.W.; Peul, W.; et al. Prevention and treatment of low back pain: Evidence, challenges, and promising directions. Lancet 2018, 391, 2368–2383. [Google Scholar] [CrossRef]
- Dueñas, M.; Ojeda, B.; Salazar, A.; Mico, J.A.; Failde, I. A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 2016, 9, 457–467. [Google Scholar] [CrossRef] [Green Version]
- Froud, R.; Patterson, S.; Eldridge, S.; Seale, C.; Pincus, T.; Rajendran, D.; Fossum, C.; Underwood, M. A systematic review and meta-synthesis of the impact of low back pain on people’s lives. BMC Musculoskelet. Disord. 2014, 15, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olafsson, G.; Jonsson, E.; Fritzell, P.; Hägg, O.; Borgström, F. Cost of low back pain: Results from a national register study in Sweden. Eur. Spine J. 2018, 27, 2875–2881. [Google Scholar] [CrossRef] [Green Version]
- Geurts, J.W.; Willems, P.C.; Kallewaard, J.W.; Van Kleef, M.; Dirksen, C. The Impact of Chronic Discogenic Low Back Pain: Costs and Patients’ Burden. Pain Res. Manag. 2018, 2018, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, B.F.; Muller, R.; Grant, W.D. Low back pain in Australian adults: The economic burden. Asia-Pac. J. Public Health 2003, 15, 79–87. [Google Scholar] [CrossRef]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef]
- Coulombe, B.J.; Games, K.E.; Neil, E.R.; Eberman, L.E. Core stability exercise versus general exercise for chronic low back pain. J. Athl. Train. 2017, 52, 71–72. [Google Scholar] [CrossRef]
- Gomes-Neto, M.; Lopes, J.M.; Conceição, C.S.; Araujo, A.; Brasileiro, A.; Sousa, C.; Carvalho, V.O.; Arcanjo, F.L. Stabilization exercise compared to general exercises or manual therapy for the management of low back pain: A systematic review and meta-analysis. Phys. Ther. Sport 2017, 23, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Owen, P.J.; Miller, C.T.; Mundell, N.L.; Verswijveren, S.J.J.M.; Tagliaferri, S.D.; Brisby, H.; Bowe, S.J.; Belavy, D.L. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br. J. Sports Med. 2020, 54, 1279–1287. [Google Scholar] [CrossRef]
- Sowah, D.; Boyko, R.; Antle, D.; Miller, L.; Zakhary, M.; Straube, S. Occupational interventions for the prevention of back pain: Overview of systematic reviews. J. Saf. Res. 2018, 66, 39–59. [Google Scholar] [CrossRef]
- European Communities NACE Rev. 2. Statistical Classification of Economic Activities in the European Community. EUROSTAT Methodologies and Working Papers. 2008. Available online: https://ec.europa.eu/eurostat/documents/3859598/5902521/KS-RA-07-015-EN.PDF (accessed on 3 December 2021).
- Pension and Disability Insurance Act (Official Gazette of the Republic of Slovenia; 2013; p. No. 96/12, 39/13, 99/13-ZSVarPre-C, 101/13-Z. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwjJusH8-vb0AhWvrlYBHR-ICZ8QFnoECAIQAQ&url=http%3A%2F%2Fpisrs.si%2FPis.web%2FnpbDocPdf%3FidPredpisa%3DZAKO8017%26idPredpisaChng%3DZAKO6280%26type%3Ddoc%26lang%3Den&usg=AOvVaw2lITH0Ub88LNqD552ChYmO (accessed on 3 December 2021).
- Employment Relationships; Official Gazette of the Republic of Slovenia. 2008. Available online: https://www.eui.eu/Projects/InternationalArtHeritageLaw/Documents/NationalLegislation/Slovenia/culturalheritageprotectionact.pdf (accessed on 3 December 2021).
- National Institute of Public Health Bolniški Stalež. Posredovanje Podatkov o Začasni Odsotnosti z Dela Zaradi Bolezenskih Razlogov. Available online: https://www.nijz.si/sites/www.nijz.si/files/uploaded/podatki/podatkovne_zbirke_raziskave/bs/mn_bs_2019.pdf (accessed on 3 December 2021).
- National Institute of Public Health Zdravstveni Statistični Letopis. Spremljanje Zdravstvenega Stanja Delavcev. Available online: https://www.nijz.si/sl/publikacije/zdravstveni-statisticni-letopis-2012 (accessed on 4 December 2021).
- Meucci, R.D.; Fassa, A.G.; Faria, N.M.X. Prevalence of chronic low back pain: Systematic review. Rev. Saude Publica 2015, 49, 1. [Google Scholar] [CrossRef] [PubMed]
- Public Administration and Defence; Compulsory Social Security statistics in Great Britain 2021. Available online: https://www.hse.gov.uk/statistics/industry/public-admin.pdf (accessed on 7 December 2021).
- Brinckmann, P.; Frobin, W.; Biggemann, M.; Tillotson, M.; Burton, K.; Burke, C.; Dickinson, C.; Krause, H.; Pangert, R.; Pfeifer, U.; et al. Quantification of overload injuries to thoracolumbar vertebrae and discs in persons exposed to heavy physical exertions or vibration at the workplace Part II Occurrence and magnitude of overload injury in exposed cohorts. Clin. Biomech. 1998, 13, S1–S36. [Google Scholar] [CrossRef]
- McPhee, B. Ergonomics in minning. Occup. Med. 2004, 54, 297–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hita-Gutiérrez, M.; Gómez-Galán, M.; Díaz-Pérez, M.; Callejón-Ferre, Á.-J. An overview of reba method applications in the world. Int. J. Environ. Res. Public Health 2020, 17, 2635. [Google Scholar] [CrossRef] [Green Version]
- Republic of Slovenia Statistical Office Persons in Employment By Activities (NACE Rev. 2), Slovenia, Monthly. Available online: https://pxweb.stat.si/SiStatData/pxweb/en/Data/-/0700921S.px/ (accessed on 5 December 2021).
- Reduce Occumational Musculoskeletal Disorders: Agriculture, Forestry and Fishing. Available online: https://www.cdc.gov/niosh/about/strategicplan/musag.html (accessed on 6 December 2021).
- Steenstra, I.; Verbeek, J.; Heymans, M.; Bongers, P. Prognostic factors for duration of sick leave in patients sick listed with acute low back pain: A systematic review of the literature. Occup. Environ. Med. 2005, 62, 851–860. [Google Scholar] [CrossRef] [Green Version]
- Discussion Paper: Musculoskeletal Disorders in the Healthcare Sector. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwiByLmm_fb0AhWksFYBHaZ5Cp8QFnoECAsQAQ&url=https%3A%2F%2Fhealthy-workplaces.eu%2Fsites%2Fdefault%2Ffiles%2Fpublications%2Fdocuments%2FDiscussion_paper_MSDs_in_health_care_sector.pdf&usg=AOvVaw3qvM3kQEj8NL9a8UKGhP3U (accessed on 8 December 2021).
- Reduce Occupational Musculoskeletal Disorders: Manufacturing. Available online: https://www.cdc.gov/niosh/about/strategicplan/muscmanuf.html (accessed on 9 December 2021).
- EU OSHA Work Related Musculoskeletal Disorders in the Service and Retail Sectors. Available online: https://osha.europa.eu/en/publications/e-fact-12-work-related-musculoskeletal-disorders-service-and-retail-sectors. (accessed on 7 December 2021).
- Yang, H.; Haldeman, S.; Lu, M.L.; Baker, D. Low Back Pain Prevalence and Related Workplace Psychosocial Risk Factors: A Study Using Data From the 2010 National Health Interview Survey. J. Manip. Physiol. Ther. 2016, 39, 459–472. [Google Scholar] [CrossRef] [Green Version]
- Wai, E.K.; Roffey, D.M.; Bishop, P.; Kwon, B.K.; Dagenais, S. Causal assessment of occupational bending or twisting and low back pain: Results of a systematic review. Spine J. 2010, 10, 76–88. [Google Scholar] [CrossRef]
- Wai, E.K.; Roffey, D.M.; Bishop, P.; Kwon, B.K.; Dagenais, S. Causal assessment of occupational lifting and low back pain: Results of a systematic review. Spine J. 2010, 10, 554–566. [Google Scholar] [CrossRef]
- Waters, T.R.; Dick, R.B.; Davis-Barkley, J.; Krieg, E.F. A cross-sectional study of risk factors for musculoskeletal symptoms in the workplace using data from the General Social Survey (GSS). J. Occup. Environ. Med. 2007, 49, 172–184. [Google Scholar] [CrossRef] [Green Version]
- Waters, T.R.; Dick, R.B.; Krieg, E.F. Trends in work-related musculoskeletal disorders: A comparison of risk factors for symptoms using quality of work life data from the 2002 and 2006 general social survey. J. Occup. Environ. Med. 2011, 53, 1013–1024. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | Female | All | |
|---|---|---|---|
| 2015 | 443,641 | 360,996 | 804,637 |
| 2016 | 446,863 | 370,346 | 817,209 |
| 2017 | 463,451 | 382,003 | 845,454 |
| 2018 | 478,148 | 394,624 | 872,772 |
| 2019 | 492,475 | 401,754 | 894,229 |
| Age gr. | 15–19.9 | 20–44.9 | 45–64.9 | 65+ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ec. Act. | M | F | TOTAL | M | F | TOTAL | M | F | TOTAL | M | F | TOTAL |
| A—agriculture, forestry and fishing | 43 | 2 | 45 | 4629 | 2054 | 6683 | 5759 | 3474 | 9233 | 35 | 8 | 43 |
| B—mining and quarrying | 12 | 0 | 12 | 1238 | 178 | 1416 | 800 | 164 | 965 | 6 | 1 | 7 |
| C—manufacturing | 755 | 90 | 845 | 79,124 | 32,639 | 111,763 | 55,898 | 30,735 | 86,633 | 399 | 58 | 457 |
| D—electricity, gas, steam, air cond. supply | 5 | 0 | 5 | 3017 | 814 | 3831 | 3128 | 791 | 3920 | 49 | 6 | 55 |
| E—water suppl; sewer., wst. manag., remed. act | 17 | 1 | 18 | 3562 | 1014 | 4576 | 3816 | 1025 | 4841 | 21 | 2 | 23 |
| F—construction | 371 | 12 | 383 | 33,094 | 3211 | 36,305 | 22,196 | 2085 | 24,281 | 191 | 6 | 197 |
| G—wholesale, retail; repair of mot. vehicles | 237 | 110 | 347 | 33,306 | 36,835 | 70,140 | 19,618 | 20,971 | 40,589 | 252 | 87 | 339 |
| H—transportation and storage | 73 | 6 | 79 | 24,050 | 4898 | 28,948 | 18,268 | 4401 | 2269 | 236 | 9 | 245 |
| I—accommodation and food ser. activities | 122 | 114 | 236 | 9819 | 13,389 | 23,157 | 4401 | 7881 | 12,283 | 73 | 56 | 129 |
| J—information and communication | 8 | 2 | 10 | 12,572 | 5810 | 18,383 | 5477 | 2796 | 8272 | 76 | 21 | 97 |
| K—financial and insurance activities | 10 | 0 | 1 | 4483 | 7140 | 11,622 | 3385 | 6430 | 9816 | 27 | 12 | 39 |
| L—real estate activities | 5 | 1 | 6 | 1558 | 1063 | 2620 | 2367 | 1087 | 3454 | 40 | 9 | 49 |
| M—professional, scientific, technical act | 31 | 10 | 41 | 17,762 | 16,527 | 34,289 | 11,552 | 9365 | 20,917 | 449 | 144 | 593 |
| N—administrative and support service act; | 192 | 67 | 259 | 12,806 | 10,487 | 23,293 | 7418 | 6702 | 14,120 | 58 | 22 | 80 |
| O—public admin, defense | 11 | 2 | 13 | 11,872 | 13,080 | 24,952 | 11,286 | 13,528 | 24,815 | 169 | 69 | 239 |
| P—education | 15 | 18 | 33 | 8604 | 30,541 | 39,145 | 8151 | 27,914 | 36,065 | 305 | 125 | 430 |
| Q—human health and social work; activities; | 65 | 140 | 204 | 7304 | 27,087 | 34,391 | 4543 | 23,215 | 27,757 | 333 | 233 | 566 |
| R—arts, entertainment and recreation | 67 | 5 | 72 | 4429 | 4653 | 9082 | 3376 | 3169 | 6544 | 92 | 28 | 120 |
| S—other service activities | 26 | 93 | 119 | 2715 | 6938 | 9625 | 2033 | 3735 | 5766 | 63 | 59 | 121 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zerbo Šporin, D.; Kozinc, Ž.; Prijon, T.; Šarabon, N. The Prevalence and Severity of Sick Leave due to Low Back Disorders among Workers in Slovenia: Analysis of National Data across Gender, Age and Classification of Economic Activities. Int. J. Environ. Res. Public Health 2022, 19, 131. https://doi.org/10.3390/ijerph19010131
Zerbo Šporin D, Kozinc Ž, Prijon T, Šarabon N. The Prevalence and Severity of Sick Leave due to Low Back Disorders among Workers in Slovenia: Analysis of National Data across Gender, Age and Classification of Economic Activities. International Journal of Environmental Research and Public Health. 2022; 19(1):131. https://doi.org/10.3390/ijerph19010131
Chicago/Turabian StyleZerbo Šporin, Dorjana, Žiga Kozinc, Ticijana Prijon, and Nejc Šarabon. 2022. "The Prevalence and Severity of Sick Leave due to Low Back Disorders among Workers in Slovenia: Analysis of National Data across Gender, Age and Classification of Economic Activities" International Journal of Environmental Research and Public Health 19, no. 1: 131. https://doi.org/10.3390/ijerph19010131