
Fidelity and Adherence to a Liquefied Petroleum Gas Stove and Fuel Intervention during Gestation: The Multi-Country Household Air Pollution Intervention Network (HAPIN) Randomized Controlled Trial

 , , , , , , ,
, , , , , , ,  , , , ,
on behalf of HAPIN Investigators
, , , ,
on behalf of HAPIN Investigators
Abstract
:1. Introduction
2. Methods
2.1. Trial Setting
2.2. Intervention Design
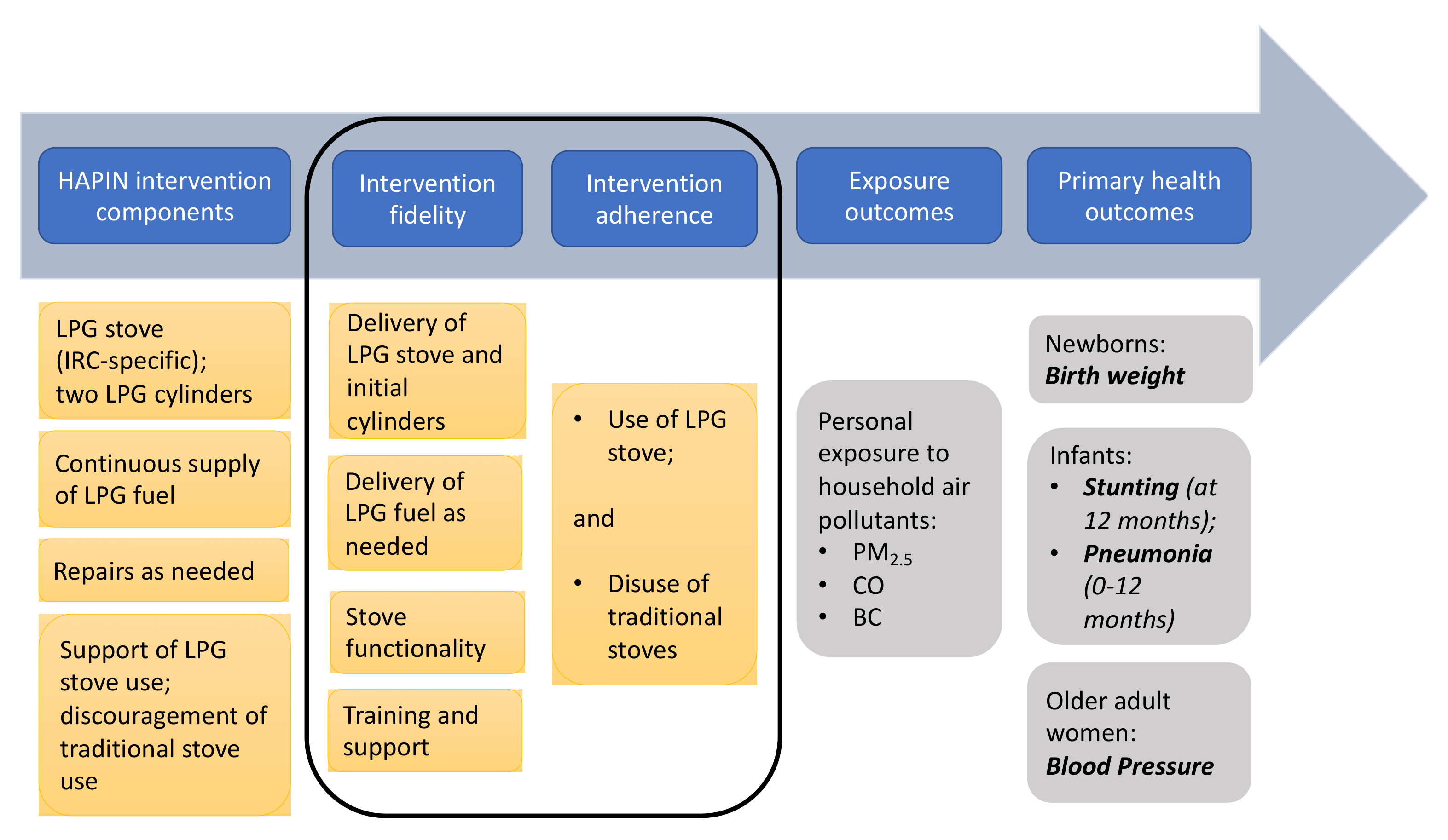
2.3. Measuring Intervention Fidelity
2.4. Measuring Intervention Adherence
2.5. Stove Use in Control Households
3. Results
3.1. Study Population and Procedures
3.2. Intervention Fidelity (Delivery of the Intervention as Intended)
3.2.1. Delivery of Intervention Stove
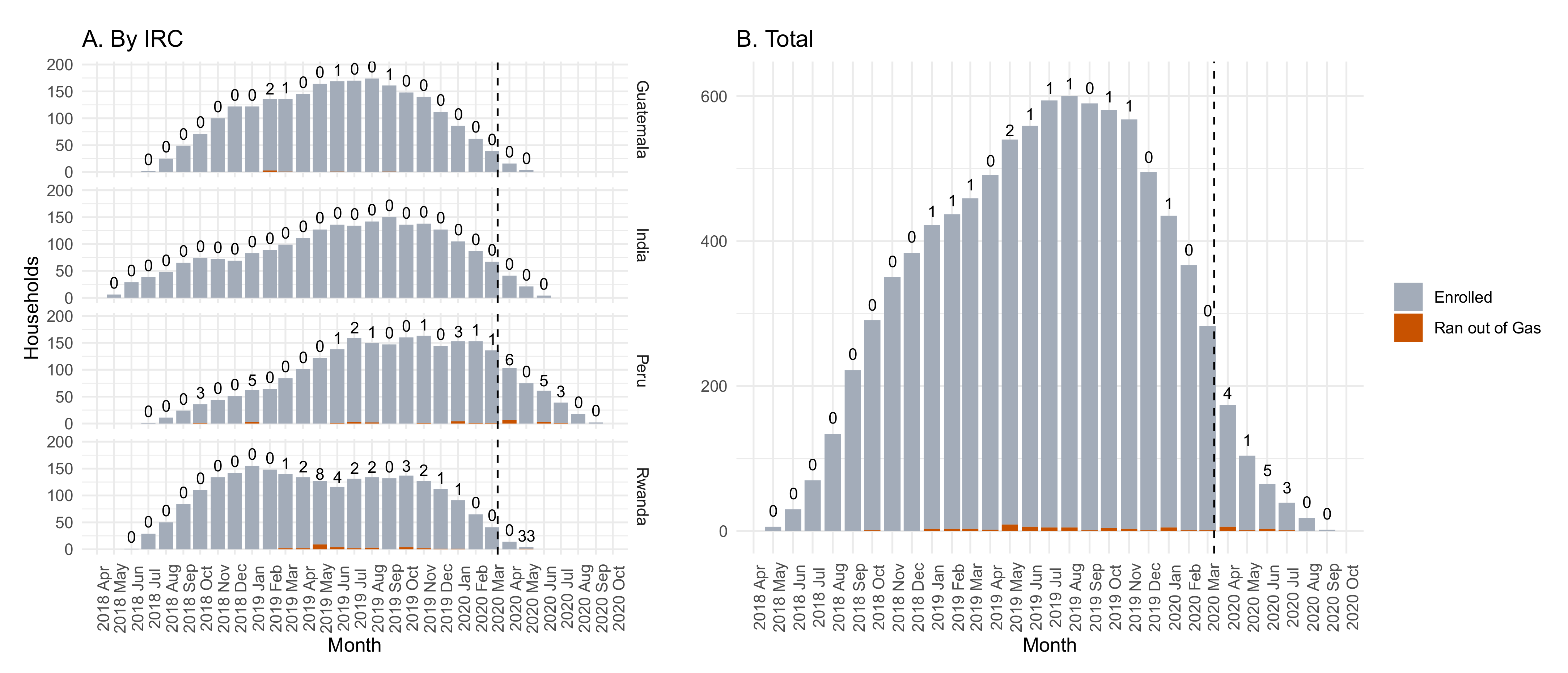
3.2.2. LPG Cylinder Refills
3.2.3. Repairs
3.2.4. Stove Use Reinforcement
3.3. Intervention Adherence (Stove Use)
3.4. Stove Use in Control Arm
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Mortimer, K.; Ndamala, C.B.; Naunje, A.W.; Malava, J.; Katundu, C.; Weston, W.; Havens, D.; Pope, D.; Bruce, N.G.; Nyirenda, M.; et al. A cleaner burning biomass-fuelled cookstove intervention to prevent pneumonia in children under 5 years old in rural Malawi (the Cooking and Pneumonia Study): A cluster randomised controlled trial. Lancet 2017, 389, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Jack, D.W.; Ae-Ngibise, K.A.; Gould, C.F.; Boamah-Kaali, E.; Lee, A.G.; Mujtaba, M.N.; Chillrud, S.; Kaali, S.; Quinn, A.K.; Gyaase, S.; et al. A cluster randomised trial of cookstove interventions to improve infant health in Ghana. BMJ Glob. Health 2021, 6, e005599. [Google Scholar] [CrossRef] [PubMed]
- Tielsch, J.M.; Katz, J.; Zeger, S.L.; Khatry, S.K.; Shrestha, L.; Breysse, P.; Checkley, W.; Mullany, L.C.; LeClerq, S.C. Designs of two randomized, community-based trials to assess the impact of alternative cookstove installation on respiratory illness among young children and reproductive outcomes in rural Nepal. BMC Public Health 2014, 14, 1271. [Google Scholar] [CrossRef] [Green Version]
- Alexander, D.A.; Northcross, A.; Karrison, T.; Morhasson-Bello, O.; Wilson, N.; Atalabi, O.M.; Dutta, A.; Adu, D.; Ibigbami, T.; Olamijulo, J.; et al. Pregnancy outcomes and ethanol cook stove intervention: A randomized-controlled trial in Ibadan, Nigeria. Environ. Int. 2018, 111, 152–163. [Google Scholar] [CrossRef]
- Checkley, W.; Williams, K.N.; Kephart, J.L.; Fandiño-Del-Rio, M.; Steenland, N.K.; Gonzales, G.F.; Naeher, L.P.; Harvey, S.A.; Moulton, L.H.; Davila-Roman, V.G.; et al. Effects of a Household Air Pollution Intervention with Liquefied Petroleum Gas on Cardiopulmonary Outcomes in Peru. A Randomized Controlled Trial. Am. J. Respir. Crit. Care Med. 2020, 203, 1386–1397. [Google Scholar] [CrossRef]
- Dickinson, K.L.; Piedrahita, R.; Coffey, E.R.; Kanyomse, E.; Alirigia, R.; Molnar, T.; Hagar, Y.; Hannigan, M.P.; Oduro, A.R.; Wiedinmyer, C. Adoption of improved biomass stoves and stove/fuel stacking in the REACCTING intervention study in Northern Ghana. Energy Policy 2019, 130, 361–374. [Google Scholar] [CrossRef]
- Chillrud, S.N.; Ae-Ngibise, K.A.; Gould, C.F.; Owusu-Agyei, S.; Mujtaba, M.; Manu, G.; Burkart, K.; Kinney, P.L.; Quinn, A.; Jack, D.W.; et al. The effect of clean cooking interventions on mother and child personal exposure to air pollution: Results from the Ghana Randomized Air Pollution and Health Study (GRAPHS). J. Expo. Sci. Environ. Epidemiol. 2021, 31, 683–698. [Google Scholar] [CrossRef] [PubMed]
- Carroll, C.; Patterson, M.; Wood, S.; Booth, A.; Rick, J.; Balain, S. A conceptual framework for implementation fidelity. Implement. Sci. 2007, 2, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for Implementation Research: Conceptual Distinctions, Measurement Challenges, and Research Agenda. Adm. Policy Ment. Health Serv. Res. 2011, 38, 65–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef] [Green Version]
- Clasen, T.F.; Checkley, W.; Peel, J.L.; Balakrishnan, K.; McCracken, J.P.; Rosa, G.; Thompson, L.M.; Barr, D.B.; Clark, M.L.; Johnson, M.A.; et al. Design and Rationale of the HAPIN Study: A Multicountry Randomized Controlled Trial to Assess the Effect of Liquefied Petroleum Gas Stove and Continuous Fuel Distribution. Environ. Health Perspect. 2020, 128, 047008. [Google Scholar] [CrossRef]
- Johnson, M.A.; Chiang, R.A. Quantitative Guidance for Stove Usage and Performance to Achieve Health and Environmental Targets. Environ. Health Perspect. 2015, 123, 820–826. [Google Scholar] [CrossRef] [Green Version]
- Williams, K.N.; Thompson, L.M.; Sakas, Z.; Hengstermann, M.; Quinn, A.; Díaz-Artiga, A.; Thangavel, G.; Puzzolo, E.; Rosa, G.; Balakrishnan, K.; et al. Designing a comprehensive behaviour change intervention to promote and monitor exclusive use of liquefied petroleum gas stoves for the Household Air Pollution Intervention Network (HAPIN) trial. BMJ Open 2020, 10, e037761. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.A.; Steenland, K.; Piedrahita, R.; Clark, M.L.; Pillarisetti, A.; Balakrishnan, K.; Peel, J.L.; Naeher, L.P.; Liao, J.; Wilson, D.; et al. Air Pollutant Exposure and Stove Use Assessment Methods for the Household Air Pollution Intervention Network (HAPIN) Trial. Environ. Health Perspect. 2020, 128, 047009. [Google Scholar] [CrossRef]
- Barr, D.B.; Puttaswamy, N.; Jaacks, L.M.; Steenland, K.; Rajkumar, S.; Gupton, S.; Ryan, P.B.; Balakrishnan, K.; Peel, J.L.; Checkley, W.; et al. Design and Rationale of the Biomarker Center of the Household Air Pollution Intervention Network (HAPIN) Trial. Environ. Health Perspect. 2020, 128, 047010. [Google Scholar] [CrossRef] [PubMed]
- Quinn, A.K.; Williams, K.; Thompson, L.M.; Rosa, G.; Díaz-Artiga, A.; Thangavel, G.; Balakrishnan, K.; Miranda, J.J.; Rosenthal, J.P.; Clasen, T.F.; et al. Compensating control participants when the intervention is of significant value: Experience in Guatemala, India, Peru and Rwanda. BMJ Glob. Health 2019, 4, e001567. [Google Scholar] [CrossRef] [Green Version]
- Hengstermann, M.; Díaz-Artiga, A.; Otzóy-Sucúc, R.; Ruiz-Aguilar, A.L.M.; Thompson, L.M.; Aravindalochanan, V.; Balakrishnan, K.; Barr, D.B.; Burrowes, V.; Campbell, D.; et al. Developing Visual Messages to Support Liquefied Petroleum Gas Use in Intervention Homes in the Household Air Pollution Intervention Network (HAPIN) Trial in Rural Guatemala. Health Educ. Behav. 2021, 48, 651–669. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.L.; Williams, K.N.; Pillarisetti, A. An Integrated Sensor Data Logging, Survey, and Analytics Platform for Field Research and Its Application in HAPIN, a Multi-Center Household Energy Intervention Trial. Sustainability 2020, 12, 1805. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Infor. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Simkovich, S.M.; Thompson, L.M.; Clark, M.L.; Balakrishnan, K.; Bussalleu, A.; Checkley, W.; Clasen, T.; Davila-Roman, V.G.; Diaz-Artiga, A.; Rosa, G.; et al. A risk assessment tool for resumption of research activities during the COVID-19 pandemic for field trials in low resource settings. BMC Med. Res. Methodol. 2021, 21, 68. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Riojas-Rodríguez, H.; Marrón-Mares, A.T.; Schilmann, A.; Perez-Padilla, R.; Masera, O. Improved biomass stove intervention in rural Mexico: Impact on the respiratory health of women. Am. J. Respir. Crit. Care Med. 2009, 180, 649–656. [Google Scholar] [CrossRef]
- Hanna, R.; Duflo, E.; Greenstone, M. Up in Smoke: The Influence of Household Behavior on the Long-Run Impact of Improved Cooking Stoves. Am. Econ. J. Econ. Policy 2016, 8, 80–114. [Google Scholar] [CrossRef]
- Kirby, M.A.; Nagel, C.L.; Rosa, G.; Zambrano, L.D.; Musafiri, S.; Ngirabega, J.D.D.; Thomas, E.A.; Clasen, T. Effects of a large-scale distribution of water filters and natural draft rocket-style cookstoves on diarrhea and acute respiratory infection: A cluster-randomized controlled trial in Western Province, Rwanda. PLoS Med. 2019, 16, e1002812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, J.; Tielsch, J.M.; Khatry, S.K.; Shrestha, L.; Breysse, P.; Zeger, S.L.; Kozuki, N.; Checkley, W.; LeClerq, S.C.; Mullany, L.C. Impact of Improved Biomass and Liquid Petroleum Gas Stoves on Birth Outcomes in Rural Nepal: Results of 2 Randomized Trials. Glob. Health Sci. Pr. 2020, 8, 372–382. [Google Scholar] [CrossRef]
- Pope, D.; Johnson, M.; Fleeman, N.; Jagoe, K.; Duarte, R.; Maden, M.; Ludolph, R.; Bruce, N.; Shupler, M.; Adair-Rohani, H.; et al. Are cleaner cooking solutions clean enough? A systematic review and meta-analysis of particulate and carbon monoxide concentrations and exposures. Environ. Res. Lett. 2021, 16, 083002. [Google Scholar] [CrossRef]
- Baquié, S.; Urpelainen, J. Access to modern fuels and satisfaction with cooking arrangements: Survey evidence from rural India. Energy Sustain. Dev. 2017, 38, 34–47. [Google Scholar] [CrossRef]
- Asante, K.P.; Afari-Asiedu, S.; Abdulai, M.A.; Dalaba, M.; Carrión, D.; Dickinson, K.L.; Abeka, A.N.; Sarpong, K.; Jack, D.W. Ghana’s rural liquefied petroleum gas program scale up: A case study. Energy Sustain. Dev. 2018, 46, 94–102. [Google Scholar] [CrossRef]
- Ozoh, O.B.; Okwor, T.J.; Adetona, O.; Akinkugbe, A.O.; Amadi, C.E.; Esezobor, C.; Adeyeye, O.O.; Ojo, O.; Nwude, V.N.; Mortimer, K. Cooking Fuels in Lagos, Nigeria: Factors Associated with Household Choice of Kerosene or Liquefied Petroleum Gas (LPG). Int. J. Environ. Res. Public Health 2018, 15, 641. [Google Scholar] [CrossRef] [Green Version]
- Thompson, L.M.; Hengstermann, M.; Weinstein, J.; Diaz-Artiga, A. Adoption of Liquefied Petroleum Gas Stoves in Guatemala: A Mixed-Methods Study. EcoHealth 2018, 15, 745–756. [Google Scholar] [CrossRef]
- Pye, A.; Ronzi, S.; Ngahane, B.H.M.; Puzzolo, E.; Ashu, A.H.; Pope, D. Drivers of the Adoption and Exclusive Use of Clean Fuel for Cooking in Sub-Saharan Africa: Learnings and Policy Considerations from Cameroon. Int. J. Environ. Res. Public Health 2020, 17, 5874. [Google Scholar] [CrossRef] [PubMed]
- Thoday, K.; Benjamin, P.; Gan, M.; Puzzolo, E. The Mega Conversion Program from kerosene to LPG in Indonesia: Lessons learned and recommendations for future clean cooking energy expansion. Energy Sustain. Dev. 2018, 46, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Gould, C.; Schlesinger, S.; Toasa, A.O.; Thurber, M.; Waters, W.F.; Graham, J.P.; Jack, D. Government policy, clean fuel access, and persistent fuel stacking in Ecuador. Energy Sustain. Dev. 2018, 46, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Astuti, S.P.; Day, R.; Emery, S.B. A successful fuel transition? Regulatory instruments, markets, and social acceptance in the adoption of modern LPG cooking devices in Indonesia. Energy Res. Soc. Sci. 2019, 58, 101248. [Google Scholar] [CrossRef]
- Shankar, A.V.; Quinn, A.K.; Dickinson, K.L.; Williams, K.N.; Masera, O.; Charron, D.; Jack, D.; Hyman, J.; Pillarisetti, A.; Bailis, R.; et al. Everybody stacks: Lessons from household energy case studies to inform design principles for clean energy transitions. Energy Policy 2020, 141, 111468. [Google Scholar] [CrossRef]
- Puzzolo, E.; Zerriffi, H.; Carter, E.; Clemens, H.; Stokes, H.; Jagger, P.; Rosenthal, J.; Petach, H. Supply Considerations for Scaling Up Clean Cooking Fuels for Household Energy in Low- and Middle-Income Countries. GeoHealth 2019, 3, 370–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steenland, K.; Pillarisetti, A.; Kirby, M.; Peel, J.; Clark, M.; Checkley, W.; Chang, H.H.; Clasen, T. Modeling the potential health benefits of lower household air pollution after a hypothetical liquified petroleum gas (LPG) cookstove intervention. Environ. Int. 2018, 111, 71–79. [Google Scholar] [CrossRef] [Green Version]
- Puzzolo, E.; Pope, D.; Stanistreet, D.; Rehfuess, E.A.; Bruce, N.G. Clean fuels for resource-poor settings: A systematic review of barriers and enablers to adoption and sustained use. Environ. Res. 2016, 146, 218–234. [Google Scholar] [CrossRef] [PubMed]
- Pollard, S.L.; Williams, K.N.; O’Brien, C.J.; Winiker, A.; Puzzolo, E.; Kephart, J.L.; Fandiño-Del-Rio, M.; Tarazona-Meza, C.; Grigsby, M.R.; Chiang, M.; et al. An evaluation of the Fondo de Inclusión Social Energético program to promote access to liquefied petroleum gas in Peru. Energy Sustain. Dev. 2018, 46, 82–93. [Google Scholar] [CrossRef]
- Pillarisetti, A.; Jamison, D.T.; Smith, K.R. Household Energy Interventions and Health and Finances in Haryana, India: An Extended Cost-Effectiveness Analysis. In Injury Prevention and Environmental Health, 3rd ed.; Mock, C.N., Nugent, R., Kobusingye, O., Smith, K.R., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2017; Chapter 12. Available online: https://pubmed.ncbi.nlm.nih.gov/30212113/ (accessed on 23 November 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Group | Control | Intervention | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| IRC | Guatemala | India | Peru | Rwanda | Guatemala | India | Peru | Rwanda | |
| Enrolled women (N) | 400 | 399 | 402 | 404 | 400 | 400 | 396 | 394 | 3195 |
| Exits before birth (N) | 14 | 13 | 44 | 10 | 16 | 12 | 11 | 15 | 135 |
| Live births (N) | 386 | 386 | 358 | 394 | 384 | 388 | 385 | 379 | 3060 |
| Days in study during pregnancy (randomization to the end of gestation): median (Q1, Q3) | 164.0 (144.8, 181.0) | 156.0 (136.5, 172.5) | 160.0 (136.0, 180.0) | 171.0 (154.0, 185.0) | 162.0 (143.0, 178.0) | 155.0 (136.0, 171.0) | 158.0 (138.0, 180.0) | 166.0 (152.0, 182.0) | 162.0 (142.0, 179.0) |
| Household size: median (Q1, Q3) | 4 (3, 6) | 3 (3, 5) | 4 (3, 6) | 3 (3, 4) | 5 (3, 7) | 3.5 (3, 5) | 4 (3, 5) | 3 (2, 4) | 4 (3, 5) |
| IRC | Guatemala | India | Peru | Rwanda | Total |
|---|---|---|---|---|---|
| Households receiving intervention 1 | 400 | 398 | 394 | 393 | 1585 |
| Stove and Initial LPG Cylinder Delivery | |||||
| Days between randomization and stove/cylinder delivery: median (Q1, Q3) | 9.0 (5.0, 15.0) | 14.0 (9.0, 20.0) | 5.0 (2.0 7.0) | 11.0 (7.0, 20.0) | 8.0 (5.0, 15.0) |
| Intervention delivery within 14 days of randomization: N (%) | 286 (71.5%) | 218 (54.8%) | 393 (99.7%) | 259 (65.9%) | 1156 (72.9%) |
| Gestational age at start of intervention (weeks): median (Q1, Q3) | 17.5 (15.4, 20.6) | 18.7 (16.4, 21.7) | 17.4 (14.6, 20.1) | 18.0 (15.7, 20.4) | 17.9 (15.4, 20.6) |
| Days under intervention during pregnancy (installation date to the end of gestation): median (Q1, Q3) | 150.0 (131.0, 167.0) | 139.0 (120.0, 157.0) | 153.5 (134.0, 176.0) | 153.0 (135.0, 170.0) | 149.0 (130.0, 168.0) |
| LPG Refill Delivery | |||||
| Time between request and delivery (days) 2: median (Q1, Q3) | 2.2 (1.9, 2.6) | 5.0 (3.0, 7.5) | 0.0 (0.0, 0.0) | 1.3 (0.5, 3.3) | 1.9 (0.0, 3.3) |
| Stove Use Reinforcement | |||||
| Participants who agreed to the stove use pledge: N (%) | 400 (100%) | 398 (100%) | 394 (100%) | 393 (100%) | 1585 (100%) |
| Participants who received LPG stove training: N (%) | 399 (99.8%) | 388 (97.5%) | 392 (99.5%) | 392 (99.8%) | 1571 (99.1%) |
| Participants with traditional stove use (TSU) who received a behavioral reinforcement visit: N (% of those with TSU) | 52 (57.1%) | 3 (7.7%) | 175 (79.9%) | 121 (71.6%) | 351 (67.8%) |
| IRC | Guatemala | India | Peru | Rwanda | Total |
|---|---|---|---|---|---|
| Households receiving intervention | 400 | 398 | 394 | 393 | 1585 |
| Households who Destroyed Traditional Stoves (no SUMs) | |||||
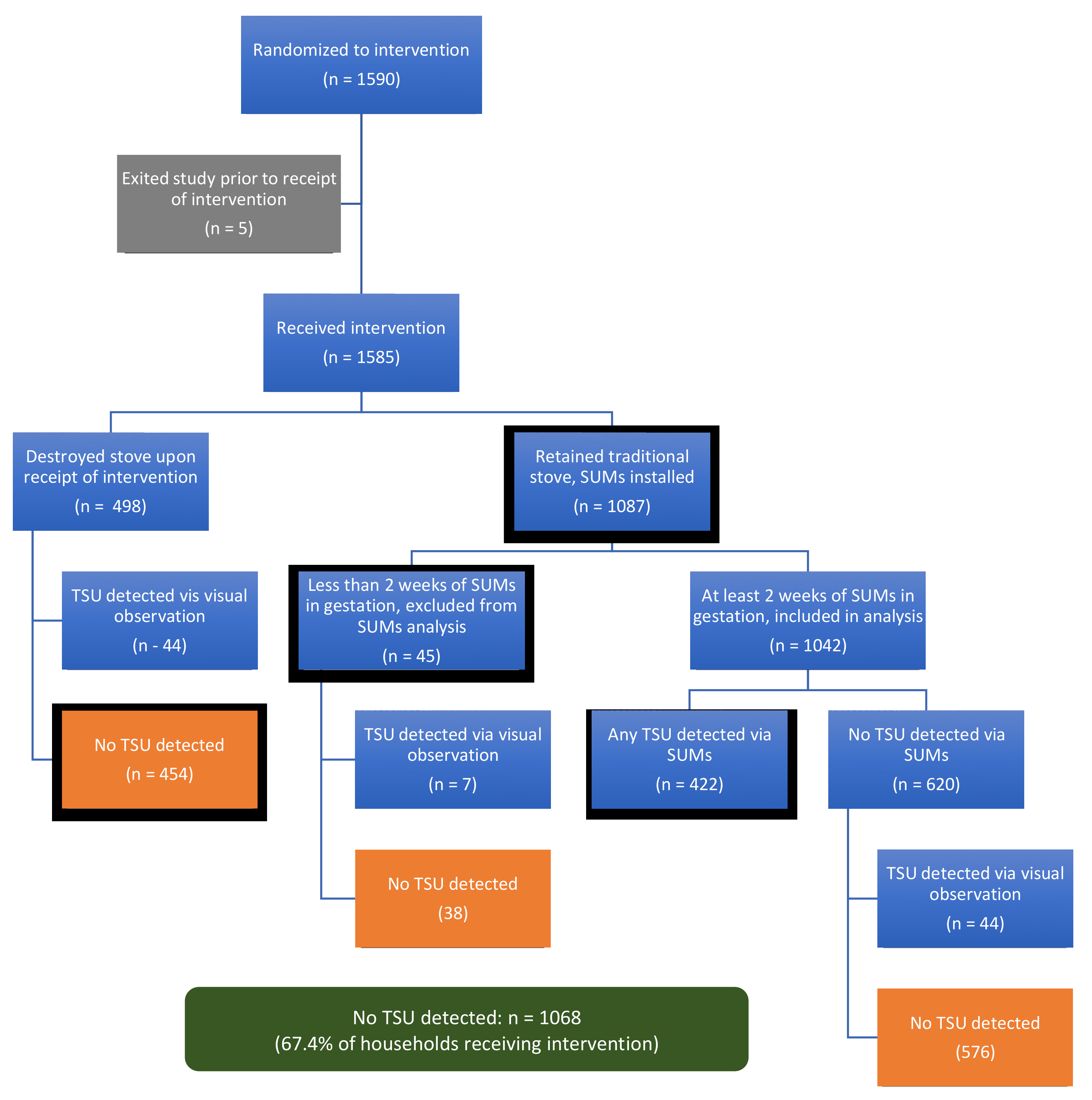
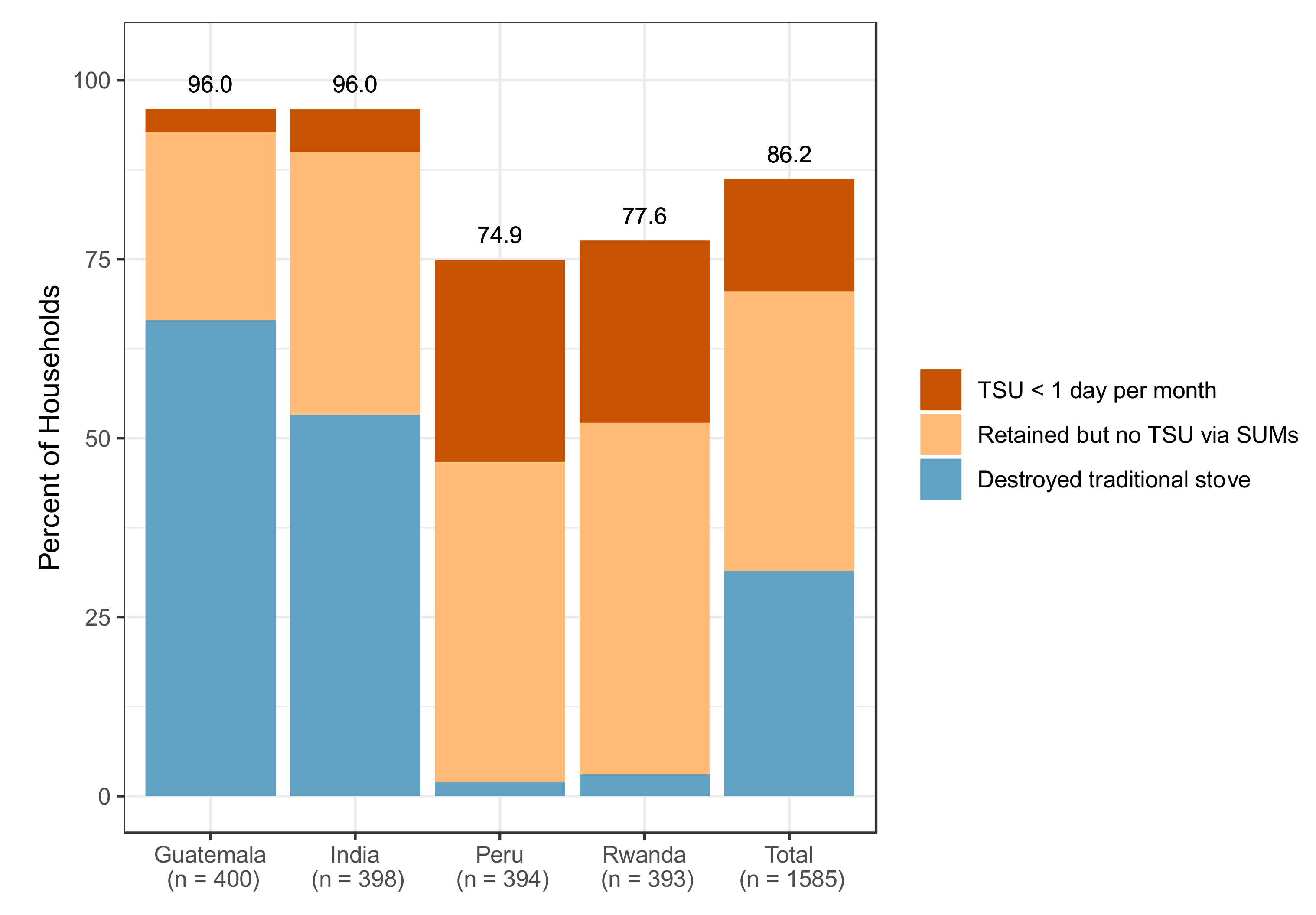
| Households who destroyed/stored traditional stove upon intervention: N (%) | 266 (66.5%) | 212 (53.3%) | 8 (2.0%) | 12 (3.1%) | 498 (31.4%) |
| Households with subsequent positive visual ID of TSU: N (% of those who destroyed) | 43 (16.2%) | 0 (0.0%) | 1 (12.5%) | 0 (0.0%) | 44 (8.8%) |
| Households who Retained Traditional Stoves (SUMs Installed) | |||||
| Households retaining a traditional stove: N (%) | 134 (33.5%) | 186 (46.7%) | 386 (98.0%) | 381 (96.9%) | 1087 (68.6%) |
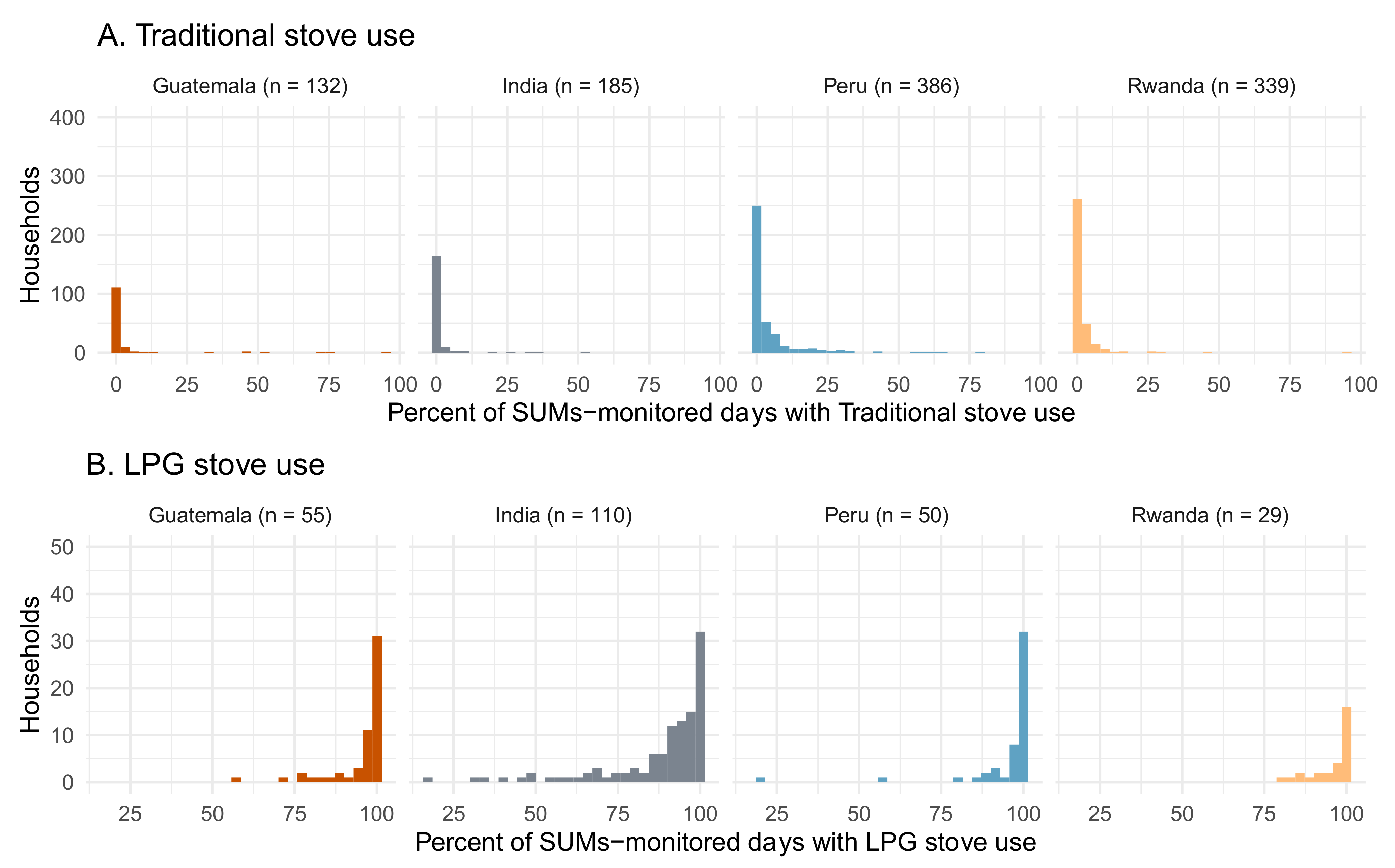
| Households with valid SUM data (≥ 2 weeks during gestation): N (% of those retaining a traditional stove) | 132 (99.2%) | 185 (100.0%) | 386 (100.0%) | 339 (97.7%) | 1042 (99.1%) |
| Days of stove-use-monitoring per household: median (Q1, Q3) | 99.0 (29.8, 146.0) | 127.0 (92.0, 148.0) | 144.5 (121.2, 170.0) | 133.0 (92.5, 160.0) | 134.0 (97.0, 160.0) |
| Proportion of gestational follow-up time monitored by SUMs: Median (Q1, Q3) | 69.3 (21.6, 100.0) | 100.0 (81.5, 100.0) | 100.0 (97.9, 100.0) | 100.0 (67.6, 100.0) | 100.0 (73.3, 100.0) |
| Percent of stove-use-monitored days with TSU detected: Median (Q1, Q3) | 0.0 (0.0, 0.0) | 0.0 (0.0, 0.0) | 0.6 (0.0, 3.6) | 0.0 (0.0, 1.4) | 0.0 (0.0, 1.6) |
| Households with no SUM-detected TSU during pregnancy: N (%) 1 | 105 (79.5%) | 146 (78.9%) | 176 (45.6%) | 193 (56.9%) | 620 (59.5%) |
| Households with < 1 day with TSU per 30 days of monitoring: N (%) 1 | 118 (89.4%) | 170 (91.9%) | 287 (74.4%) | 293 (86.4%) | 868 (83.3%) |
| Traditional stove cooking minutes per day, among those with ≥ 1 day of TSU in gestation: median (Q1, Q3) (N hh) | 138.0 (41.2, 385.3) (n = 27) | 85.0 (48.9, 121.5) (n = 39) | 95.0 (54.4, 131.7) (n = 210) | 81.7 (43.8, 151.7) (n = 146) | 91.0 (47.5, 142.4) (n = 422) |
| Overall TSU | |||||
| No TSU detected by SUMs or visual observation: N (%) | 309 (77.2%) | 359 (90.2%) | 175 (44.4%) | 224 (57.0%) | 1068 (67.4%) |
| Any TSU detected by SUMs or visual observation: N (%) | 91 (22.8%) | 39 (9.8%) | 219 (55.6%) | 168 (42.7%) | 517 (32.6%) |
| IRC | Top Three Ranked Reasons for Traditional Stove Use (N Reporting; Percent of the Intervention Households) |
|---|---|
| Guatemala |
|
| India |
|
| Peru |
|
| Rwanda |
|
| IRC | Guatemala | India | Peru | Rwanda | Total |
|---|---|---|---|---|---|
| Households receiving intervention | 400 | 398 | 394 | 393 | 1585 |
| Households with SUMs on LPG stove ≥ 2 wks during gestation: N (%) | 55 (13.8%) | 110 (27.6%) | 50 (12.7%) | 29 (7.4%) | 244 (15.4%) |
| Days of monitoring: median (Q1, Q3) | 128.0 (119.0, 142.0) | 127.0 (101.2, 148.8) | 116.0 (48.2, 134.0) | 112.0 (76.0, 130.0) | 123.0 (97.8, 142.0) |
| Percent of stove-use-monitored days with LPG stove use detected: median (Q1, Q3) | 99.0 (96.1, 100.0) | 93.8 (84.9, 99.4) | 99.3 (97.2, 100.0) | 99.3 (94.7, 100.0) | 98.3 (90.5, 100.0) |
| LPG stove cooking minutes per day of LPG stove use, among those with ≥ 1 day of LPG stove use in gestation: median (Q1, Q3) (N hh) | 299.3 (223.4, 439.8) (n = 55) | 197.0 (159.7, 248.8) (n = 110) | 285.4 (226.4, 341.0) (n = 50) | 231.2 (187.7, 292.3) (n = 29) | 232.5 (181.3, 301.6) (n = 244) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quinn, A.K.; Williams, K.N.; Thompson, L.M.; Harvey, S.A.; Piedrahita, R.; Wang, J.; Quinn, C.; Pillarisetti, A.; McCracken, J.P.; Rosenthal, J.P.; et al. Fidelity and Adherence to a Liquefied Petroleum Gas Stove and Fuel Intervention during Gestation: The Multi-Country Household Air Pollution Intervention Network (HAPIN) Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 12592. https://doi.org/10.3390/ijerph182312592
Quinn AK, Williams KN, Thompson LM, Harvey SA, Piedrahita R, Wang J, Quinn C, Pillarisetti A, McCracken JP, Rosenthal JP, et al. Fidelity and Adherence to a Liquefied Petroleum Gas Stove and Fuel Intervention during Gestation: The Multi-Country Household Air Pollution Intervention Network (HAPIN) Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(23):12592. https://doi.org/10.3390/ijerph182312592
Chicago/Turabian StyleQuinn, Ashlinn K., Kendra N. Williams, Lisa M. Thompson, Steven A. Harvey, Ricardo Piedrahita, Jiantong Wang, Casey Quinn, Ajay Pillarisetti, John P. McCracken, Joshua P. Rosenthal, and et al. 2021. "Fidelity and Adherence to a Liquefied Petroleum Gas Stove and Fuel Intervention during Gestation: The Multi-Country Household Air Pollution Intervention Network (HAPIN) Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 23: 12592. https://doi.org/10.3390/ijerph182312592