
Does Childcare Work Promote Cardiorespiratory Fitness and Health? A Cross-Sectional Study of Danish Childcare Workers Based on Accelerometry and Heart Rate Measurements

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Protection and Ethical Approval
2.2. Recruitment of Childcare Institutions
2.3. Workers within Participating Centers
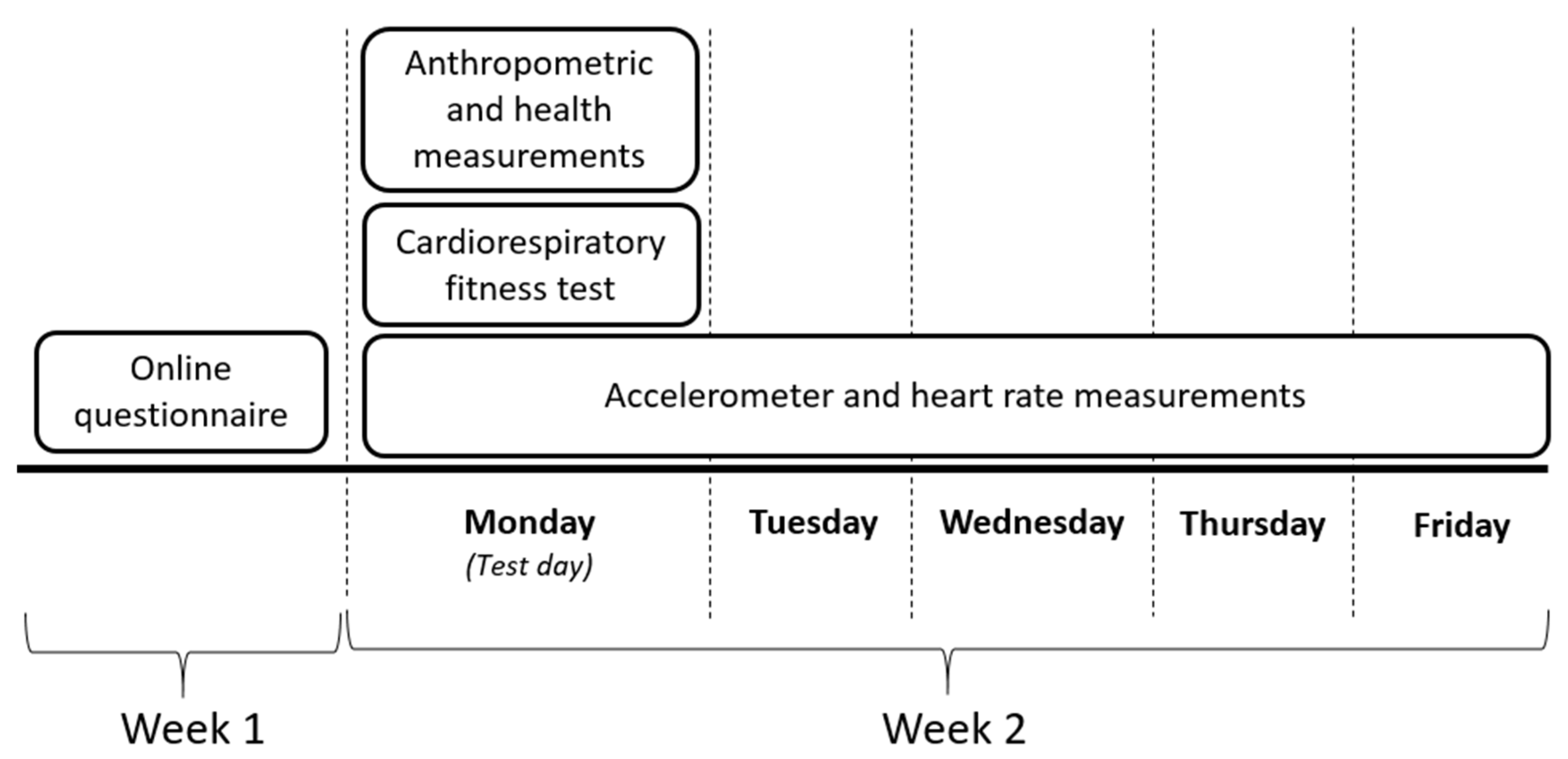
2.4. Data Collection
2.4.1. Online Questionnaires
2.4.2. Physical Assessment
2.4.3. Wearable Sensor Measurements of Physical Behaviors
2.5. Statistical Analyses
3. Results
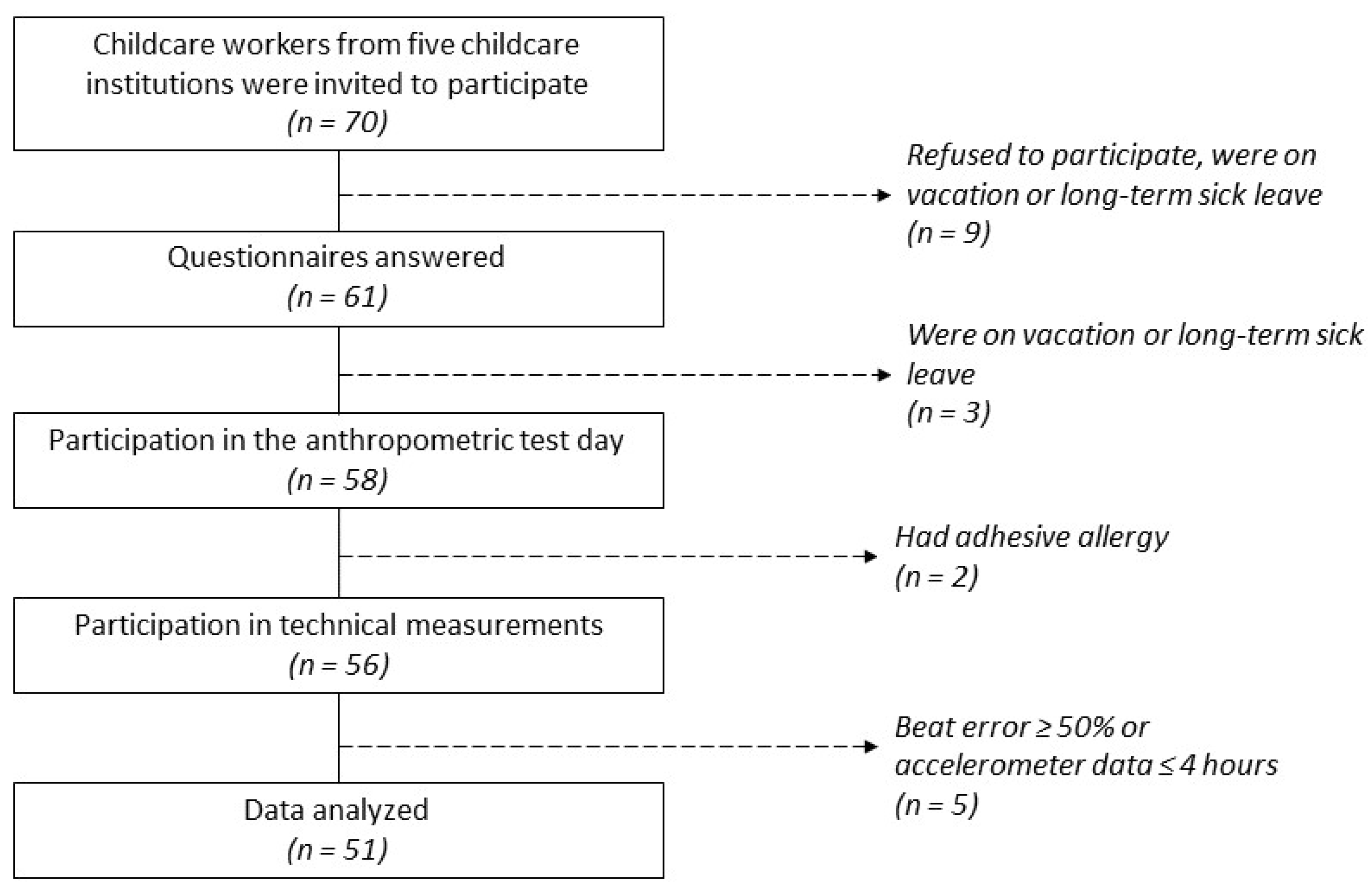
3.1. Participants Flow
3.2. Demographics and Cardiorespiratory Fitness
3.3. Composition of Physical Behaviors
3.4. Intensity of Physical Behaviors Based on Heart Rate Data
3.5. Alternation of Physical Behaviors at Work
4. Discussion
4.1. Practical Implications
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Sedentary Work Time | Standing Work Time | Active Work Time | |
|---|---|---|---|
| Sedentary Leisure Time | −0.02 | 0.10 | 0.06 |
| Standing Leisure Time | 0.16 | −0.08 | −0.22 |
| Active Leisure Time | 0.09 | −0.03 | 0.05 |
Appendix B
| ≤25% HRR Work Time | >25–<60% HRR Work Time | ≥60% HRR Work Time | |
|---|---|---|---|
| ≤25% HRR Leisure Time | 0.72 | −0.49 | −0.30 |
| >25–<60% HRR Leisure Time | −0.57 | 0.57 | 0.07 |
| ≥60% HRR Leisure Time | −0.18 | 0.13 | 0.44 |
Appendix C
| Sedentary < 5 min Work Time | Sedentary 5–30 min Work Time | Sedentary > 30 min Work Time | Standing < 5 min Work Time | Standing 5–30 min Work Time | Standing > 30 min Work Time | Active < 5 min Work Time | Active 5–30 min Work Time | Active > 30 min Work Time | |
|---|---|---|---|---|---|---|---|---|---|
| Sedentary <5 min Leisure Time | 0.20 | 0.14 | 0.04 | −0.31 | −0.25 | −0.09 | −0.23 | −0.03 | NA |
| Sedentary 5–30 min Leisure Time | 0.20 | 0.14 | 0.04 | −0.31 | −0.25 | −0.09 | −0.23 | −0.41 | NA |
| Sedentary > 30 min Leisure Time | −0.18 | −0.11 | 0.16 | 0.06 | 0.17 | 0.19 | 0.05 | 0.09 | NA |
| Standing < 5 min Leisure Time | 0.11 | 0.15 | 0.07 | −0.14 | −0.07 | −0.17 | −0.11 | −0.13 | NA |
| Standing 5–30 min Leisure Time | −0.05 | 0.24 | −0.08 | 0.05 | 0.03 | 0.01 | −0.28 | 0.11 | NA |
| Standing > 30 min Leisure Time | −0.11 | 0.07 | −0.14 | 0.05 | −0.03 | −0.03 | −0.05 | −0.06 | NA |
| Active < 5 min Leisure Time | 0.14 | 0.20 | 0.06 | −0.03 | −0.17 | −0.21 | 0.06 | −0.13 | NA |
| Active 5–30 min Leisure Time | 0.04 | 0.00 | −0.14 | 0.09 | −0.14 | −0.03 | 0.01 | 0.20 | NA |
| Active > 30 min Leisure Time | −0.11 | −0.18 | 0.19 | 0.01 | −0.19 | −0.03 | 0.02 | 0.00 | NA |
References
- Cumming, T. Early Childhood Educators’ Well-Being: An Updated Review of the Literature. J. Fam. Econ. Issues 2017, 45, 583–593. [Google Scholar] [CrossRef]
- Linnan, L.; Arandia, G.; Bateman, L.A.; Vaughn, A.; Smith, N.; Ward, D. The Health and Working Conditions of Women Employed in Child Care. Int. J. Environ. Res. Public Health 2017, 14, 283. [Google Scholar] [CrossRef]
- Otten, J.J.; Bradford, V.A.; Stover, B.; Hill, H.D.; Osborne, C.; Getts, K.; Seixas, N. The Culture Of Health In Early Care And Education: Workers’ Wages, Health, And Job Characteristics. Health Aff. (Millwood) 2019, 38, 709–720. [Google Scholar] [CrossRef] [Green Version]
- Arbejdstilsynet. Arbejdsmiljø og helbred 2012–2018. 2020. Available online: https://at.dk/arbejdsmiljoe-i-tal/arbejdsmiljoe-og-helbred-2012-2018/ (accessed on 26 November 2021).
- Holtermann, A.; Mortensen, O.S.; Burr, H.; Søgaard, K.; Gyntelberg, F.; Suadicani, P. Physical demands at work, physical fitness, and 30-year ischaemic heart disease and all-cause mortality in the Copenhagen Male Study. Scand. J. Work. Environ. Health 2010, 36, 357–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Written, K.; Pearce, J. Geographies of Obesity: Environmental Understandings of the Obesity Epidemic; Routledge: London, UK, 2010; p. 356. [Google Scholar]
- Buchbinder, R.; van Tulder, M.; Öberg, B.; Costa, L.M.; Woolf, A.; Schoene, M.; Croft, P.; Lancet Low Back Pain Series Working Group. Low back pain: A call for action. Lancet 2018, 9, 2384–2388. [Google Scholar] [CrossRef]
- Linnan, L.A.; Vaughn, A.E.; Smith, F.T.; Westgate, P.; Hales, D.; Arandia, G.; Neshteruk, C.; Willis, E.; Ward, D.S. Results of caring and reaching for health (CARE): A cluster-randomized controlled trial assessing a worksite wellness intervention for child care staff. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 64. [Google Scholar] [CrossRef]
- Gosliner, W.A.; James, P.; Yancey, A.K.; Ritchie, L.; Studer, N.; Crawford, P.B. Impact of a Worksite Wellness Program on the Nutrition and Physical Activity Environment of Child Care Centers. Am. J. Health Promot. 2010, 24, 186–189. [Google Scholar] [CrossRef] [PubMed]
- Holtermann, A.; Straker, L.; Lee, I.-M.; Stamatakis, E.; van der Beek, A.J. Workplace physical activity promotion: Why so many failures and few successes? The need for new thinking. Br. J. Sports Med. 2020, 55, 650–651. [Google Scholar] [CrossRef] [PubMed]
- Holtermann, A.; Mathiassen, S.E.; Straker, L. Promoting health and physical capacity during productive work: The Goldilocks Principle. Scand. J. Work. Environ. Health 2019, 45, 90–97. [Google Scholar] [CrossRef]
- Straker, L.; Mathiassen, S.E.; Holtermann, A. The ‘Goldilocks Principle’: Designing physical activity at work to be ‘just right’ for promoting health. Br. J. Sports Med. 2018, 52, 818–819. [Google Scholar] [CrossRef] [Green Version]
- Holtermann, A.; Hendriksen, P.F.; Schmidt, K.G.; Svendsen, M.J.; Rasmussen, C.D.N. Physical Work Demands of Childcare Workers in Denmark: Device-Based Measurements and Workplace Observations Among 199 Childcare Workers from 16 Day Nurseries. Ann. Work. Expo. Health 2020, 64, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Horng, Y.S.; Hsieh, S.F.; Wu, H.C.; Feng, C.T.; Lin, M.C. Work-related musculoskeletal disorders of the workers in a Child Care institution. Tw I Phys. Med. Rehabil. 2008, 36, 15–21. [Google Scholar]
- Prince, S.A.; Adamo, K.B.; Hamel, M.; Hardt, J.; Gorber, S.C.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, D.S.; Vaughn, A.E.; Hales, D.; Viera, A.J.; Gizlice, Z.; Bateman, L.A.; Grummon, A.H.; Arandia, G.; Linnan, L.A. Workplace health and safety intervention for child care staff: Rationale, design, and baseline results from the CARE cluster randomized control trial. Contemp. Clin. Trials 2018, 68, 116–126. [Google Scholar] [CrossRef] [Green Version]
- Lidegaard, M.; Lerche, A.; Munch, P.K.; Schmidt, K.G.; Rasmussen, C.L.; Mathiassen, S.E.; Straker, L.; Holtermann, A.; Rasmussen, C.D.N. Can childcare work be designed to promote moderate and vigorous physical activity, cardiorespiratory fitness and health? Study protocol for the Goldilocks-childcare randomised controlled trial. BMC Public Health 2020, 20, 237. [Google Scholar] [CrossRef] [PubMed]
- Lerche, A.F.; Vilhelmsen, M.; Schmidt, K.G.; Kildedal, R.; Launbo, N.; Munch, P.K.; Lidegaard, M.; Jacobsen, S.S.; Rasmussen, C.L.; Mathiassen, S.E.; et al. Can Childcare Work Be Designed to Promote High Intensity Physical Activity for Improved Fitness and Health? A Proof of Concept Study of the Goldilocks Principle. Int. J. Environ. Res. Public Health 2020, 17, 7419. [Google Scholar] [CrossRef] [PubMed]
- Bosaeus, M.; Andersson-Hall, U.; Andersson, L.; Karlsson, T.; Ellegård, L.; Holmäng, A. Body Composition During Pregnancy: Longitudinal Changes and Method Comparisons. Reprod. Sci. 2020, 27, 1477–1489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danquah, I.H.; Petersen, C.B.; Skov, S.S.; Tolstrup, J.S. Validation of the NPAQ-short—A brief questionnaire to monitor physical activity and compliance with the WHO recommendations. BMC Public Health 2018, 18, 601. [Google Scholar] [CrossRef]
- Björkman, F.; Ekblom-Bak, E.; Ekblom, Ö.; Ekblom, B. Validity of the revised Ekblom Bak cycle ergometer test in adults. Graefe’s Arch. Clin. Exp. Ophthalmol. 2016, 116, 1627–1638. [Google Scholar] [CrossRef] [Green Version]
- Ekblom-Bak, E.; Bjorkman, F.; Hellenius, M.; Ekblom, B. A new submaximal cycle ergometer test for prediction of VO2max. Scand. J. Med. Sci. Sports 2014, 24, 319–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skotte, J.; Korshøj, M.; Kristiansen, J.; Hanisch, C.; Holtermann, A. Detection of Physical Activity Types Using Triaxial Accelerometers. J. Phys. Act. Health 2014, 11, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, M.B.; Gupta, N.; Korshøj, M.; Lagersted-Olsen, J.; Villumsen, M.; Mortensen, O.S.; Skotte, J.; Søgaard, K.; Madeleine, P.; Samani, A.; et al. The DPhacto cohort: An overview of technically measured physical activity at work and leisure in blue-collar sectors for practitioners and researchers. Appl. Ergon. 2019, 77, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Holliday, K.M.; Howard, A.G.; Emch, M.; Rodríguez, D.A.; Evenson, K.R. Are buffers around home representative of physical activity spaces among adults? Health Place 2017, 45, 181–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef] [Green Version]
- Kristiansen, J.; Korshøj, M.; Skotte, J.H.; Jespersen, T.; Søgaard, K.; Mortensen, O.S.; Holtermann, A. Comparison of two systems for long-term heart rate variability monitoring in free-living conditions—A pilot study. Biomed. Eng. Online 2011, 10, 27. [Google Scholar] [CrossRef] [Green Version]
- Hallman, D.M.; Mathiassen, S.E.; Gupta, N.; Korshøj, M.; Holtermann, A. Differences between work and leisure in temporal patterns of objectively measured physical activity among blue-collar workers. BMC Public Health 2015, 15, 976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loef, B.; Van Der Beek, A.J.; Holtermann, A.; Hulsegge, G.; Van Baarle, D.; Proper, K. Objectively measured physical activity of hospital shift workers. Scand. J. Work. Environ. Health 2018, 44, 265–273. [Google Scholar] [CrossRef] [Green Version]
- Peereboom, K.; Langen, N.; Bortkiewicz, A. Prolonged static sitting at work. European Agency for Safety and Health at Work. 2021. Available online: Prolonged_static_sitting_at_work.pdf (accessed on 26 November 2021).
- Gormley, S.E.; Swain, D.P.; High, R.; Spina, R.J.; Dowling, E.A.; Kotipalli, U.S.; Gandrakota, R. Effect of intensity of aerobic training on VO2max. Med. Sci. Sports Exerc. 2008, 40, 1336–1343. [Google Scholar] [CrossRef] [PubMed]
- Bacon, A.P.; Carter, R.E.; Ogle, E.A.; Joyner, M.J. VO2max Trainability and High Intensity Interval Training in Humans: A Meta-Analysis. PLoS ONE 2013, 8, e73182. [Google Scholar] [CrossRef]
- Waters, T.R.; Dick, R.B. Evidence of Health Risks Associated with Prolonged Standing at Work and Intervention Effectiveness. Rehabil. Nurs. 2014, 40, 148–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Cerin, E.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Breaks in Sedentary Time: Beneficial associations with metabolic risk. Diabetes Care 2008, 31, 661–666. [Google Scholar] [CrossRef] [Green Version]
- Larsen, R.; Kingwell, B.; Sethi, P.; Cerin, E.; Owen, N.; Dunstan, D. Breaking up prolonged sitting reduces resting blood pressure in overweight/obese adults. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 976–982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coenen, P.; Parry, S.; Willenberg, L.; Shi, J.W.; Romero, L.; Blackwood, D.M.; Healy, G.N.; Dunstan, D.W.; Straker, L.M. Associations of prolonged standing with musculoskeletal symptoms—A systematic review of laboratory studies. Gait Posture 2017, 58, 310–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, D.R.; Hivert, M.-F.; Alhassan, S.; Camhi, S.M.; Ferguson, J.F.; Katzmarzyk, P.; Lewis, C.E.; Owen, N.; Perry, C.; Siddique, J.; et al. Sedentary Behavior and Cardiovascular Morbidity and Mortality: A Science Advisory From the American Heart Association. Circulation 2016, 134, e262–e279. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Bredin, S.S.D. Reflections on Physical Activity and Health: What Should We Recommend? Can. J. Cardiol. 2016, 32, 495–504. [Google Scholar] [CrossRef] [Green Version]
- Holtermann, A.; Krause, N.; Van Der Beek, A.J.; Straker, L. The physical activity paradox: Six reasons why occupational physical activity (OPA) does not confer the cardiovascular health benefits that leisure time physical activity does. Br. J. Sports Med. 2018, 52, 149–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekelund, U.; Tarp, J.; Fagerland, M.W.; Johannessen, J.S.; Hansen, B.H.; Jefferis, B.J.; Whincup, P.H.; Diaz, K.M.; Hooker, S.; Howard, V.J.; et al. Joint associations of accelero-meter measured physical activity and sedentary time with all-cause mortality: A harmonised meta-analysis in more than 44,000 middle-aged and older individuals. Br. J. Sports Med. 2020, 54, 1499–1506. [Google Scholar] [CrossRef] [PubMed]
- Imboden, M.T.; Harber, M.P.; Whaley, M.H.; Finch, W.H.; Bishop, D.L.; Kaminsky, L.A. Cardiorespiratory Fitness and Mortality in Healthy Men and Women. J. Am. Coll. Cardiol. 2018, 72, 2283–2292. [Google Scholar] [CrossRef] [PubMed]
- Parak, J.; Jorhonen, I. Accuracy of Firstbeat Bodyguard 2 Beat-To-Beat Heart Rate Monitor. Available online: https://assets.firstbeat.com/firstbeat/uploads/2015/10/white_paper_bodyguard2_final.pdf (accessed on 26 November 2021).


| Variables | N (%) | Mean (SD) |
|---|---|---|
| Gender (female) | 28 (55.0) | |
| Age (years) | 36.2 (10.3) | |
| Born in Denmark | 44 (86.3) | |
| Length of service in current job (years) | 3.6 (1.2) | |
| Length of service in current profession (years) | 10.3 (7.6) | |
| Job title | ||
| Childcare worker | 28 (54.9) | |
| Childcare assistant | 20 (39.2) | |
| Other | 3 (5.9) | |
| Average alcohol intake (standard drinks/week) | 1.8 (0.7) | |
| Current smokers (yes) | 12 (23.5) | |
| Self-reported time in moderate to vigorous physical activity (h/week) | 5.3 (4.9) | |
| Blood pressure (mmHg) | ||
| Systolic | 126.5 (13.0) | |
| Diastolic | 82.6 (9.5) | |
| BMI (kg/m2) | 25.0 (5.2) | |
| Maximal oxygen uptake (mL/kg∙min) * | 44.9 (12.4) | |
| Female | 37.6 (8.7) | |
| Male | 53.7 (10.1) |
| Behaviors | Work Time | Leisure Time | Awake Time | Sleep Time | |||
|---|---|---|---|---|---|---|---|
| Minutes (SD) | % (SD) | Minutes (SD) | % (SD) | Minutes (SD) | % (SD) | Minutes (SD) | |
| Sedentary | 178.1 (51.2) | 43.0 (10.5) | 310.6 (76.5) | 59.4 (11.5) | 488.7 (91.3) | 52.2 (7.1) | - |
| Standing | 163.7 (40.0) | 39.6 (8.0) | 144.0 (52.7) | 27.9 (9.1) | 307.7 (63.6) | 33.0 (5.6) | - |
| Active | 72.1 (20.8) | 17.4 (4.1) | 66.8 (28.4) | 12.7 (4.5) | 138.9(36.0) | 14.8 (3.3) | - |
| Sleep | - | - | - | - | - | - | 459.0 (64.4) |
| Intensity | Work Time | Leisure Time | Awake Time | |||
|---|---|---|---|---|---|---|
| Minutes (SD) | % (SD) | Minutes (SD) | % (SD) | Minutes (SD) | % (SD) | |
| ≤25% HRR | 159.2 (91.4) | 44.1 (25.7) | 254.2 (97.9) | 55.1 (20.0) | 413.3 (175.6) | 50.1 (20.8) |
| >25–<60% HRR | 198.2 (92.1) | 55.2 (25.3) | 191.6 (91.0) | 41.5 (18.9) | 389.7 (162.2) | 47.7 (20.2) |
| ≥60% HRR | 2.3 (3.4) | 0.7 (1.0) | 15.3 (13.0) | 3.4 (3.1) | 17.6 (14.8) | 2.2 (2.0) |
| Behavior by Bout | Work Time | Leisure Time | Awake Time | |||
|---|---|---|---|---|---|---|
| Minutes (SD) | % (SD) | Minutes (SD) | % (SD) | Minutes (SD) | % (SD) | |
| Sedentary < 5 min | 54.2 (17.7) | 13.1 (3.9) | 32.7 (13.1) | 6.6 (3.8) | 86.9 (24.1) | 9.4 (2.8) |
| Sedentary 5–30 min | 95.9 (32.4) | 23.1 (7.3) | 114.2 (42.2) | 21.7 (7.9) | 210.1 (50.8) | 22.4 (4.9) |
| Sedentary > 30 min | 28.0 (37.0) | 6.7 (8.4) | 163.8 (76.4) | 31.0 (14.0) | 191.8 (90.2) | 20.3 (9.1) |
| Standing < 5 min | 152.8 (35.6) | 36.9 (7.2) | 112.9 (38.5) | 22.0 (7.4) | 265.7 (48.7) | 28.5 (4.5) |
| Standing 5–30 min | 11.9 (9.1) | 2.8 (2.1) | 30.4 (24.7) | 5.7 (4.5) | 42.2 (26.5) | 4.5 (2.7) |
| Standing > 30 min | 0.2 (1.1) | 0.0 (0.2) | 1.3 (5.4) | 0.2 (1.1) | 1.4 (5.5) | 0.2 (0.6) |
| Active < 5 min | 70.4 (20.0) | 16.9 (4.0) | 52.8 (18.3) | 10.1 (3.1) | 123.1 (27.9) | 13.2 (2.6) |
| Active 5–30 min | 1.9 (3.4) | 0.4 (0.8) | 12.8 (14.7) | 2.4 (2.6) | 14.6 (15.7) | 1.5 (1.6) |
| Active > 30 min | 0.0 (0.0) | 0.0 (0.0) | 1.4 (6.2) | 0.2 (1.0) | 1.4 (6.2) | 0.1 (0.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmidt, K.G.; Kildedal, R.; Lerche, A.F.; Vilhelmsen, M.; Rasmussen, C.L.; Mathiassen, S.E.; Straker, L.; Holtermann, A. Does Childcare Work Promote Cardiorespiratory Fitness and Health? A Cross-Sectional Study of Danish Childcare Workers Based on Accelerometry and Heart Rate Measurements. Int. J. Environ. Res. Public Health 2021, 18, 12496. https://doi.org/10.3390/ijerph182312496
Schmidt KG, Kildedal R, Lerche AF, Vilhelmsen M, Rasmussen CL, Mathiassen SE, Straker L, Holtermann A. Does Childcare Work Promote Cardiorespiratory Fitness and Health? A Cross-Sectional Study of Danish Childcare Workers Based on Accelerometry and Heart Rate Measurements. International Journal of Environmental Research and Public Health. 2021; 18(23):12496. https://doi.org/10.3390/ijerph182312496
Chicago/Turabian StyleSchmidt, Kathrine Greby, Rasmus Kildedal, Anders Fritz Lerche, Maja Vilhelmsen, Charlotte Lund Rasmussen, Svend Erik Mathiassen, Leon Straker, and Andreas Holtermann. 2021. "Does Childcare Work Promote Cardiorespiratory Fitness and Health? A Cross-Sectional Study of Danish Childcare Workers Based on Accelerometry and Heart Rate Measurements" International Journal of Environmental Research and Public Health 18, no. 23: 12496. https://doi.org/10.3390/ijerph182312496