
Systematic Review of the Literature on Dental Caries and Periodontal Disease in Socio-Economically Disadvantaged Individuals

 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- There are no differences regarding carious pathology and periodontal disease between socio-economically disadvantaged subjects and the normal population.
- There are no differences concerning caries and periodontal disease between different categories of socio-economically disadvantaged and vulnerable individuals.
- There are no differences in terms of caries and periodontal disease in socio-economically disadvantaged individuals who combine different types of socio-economic vulnerability.
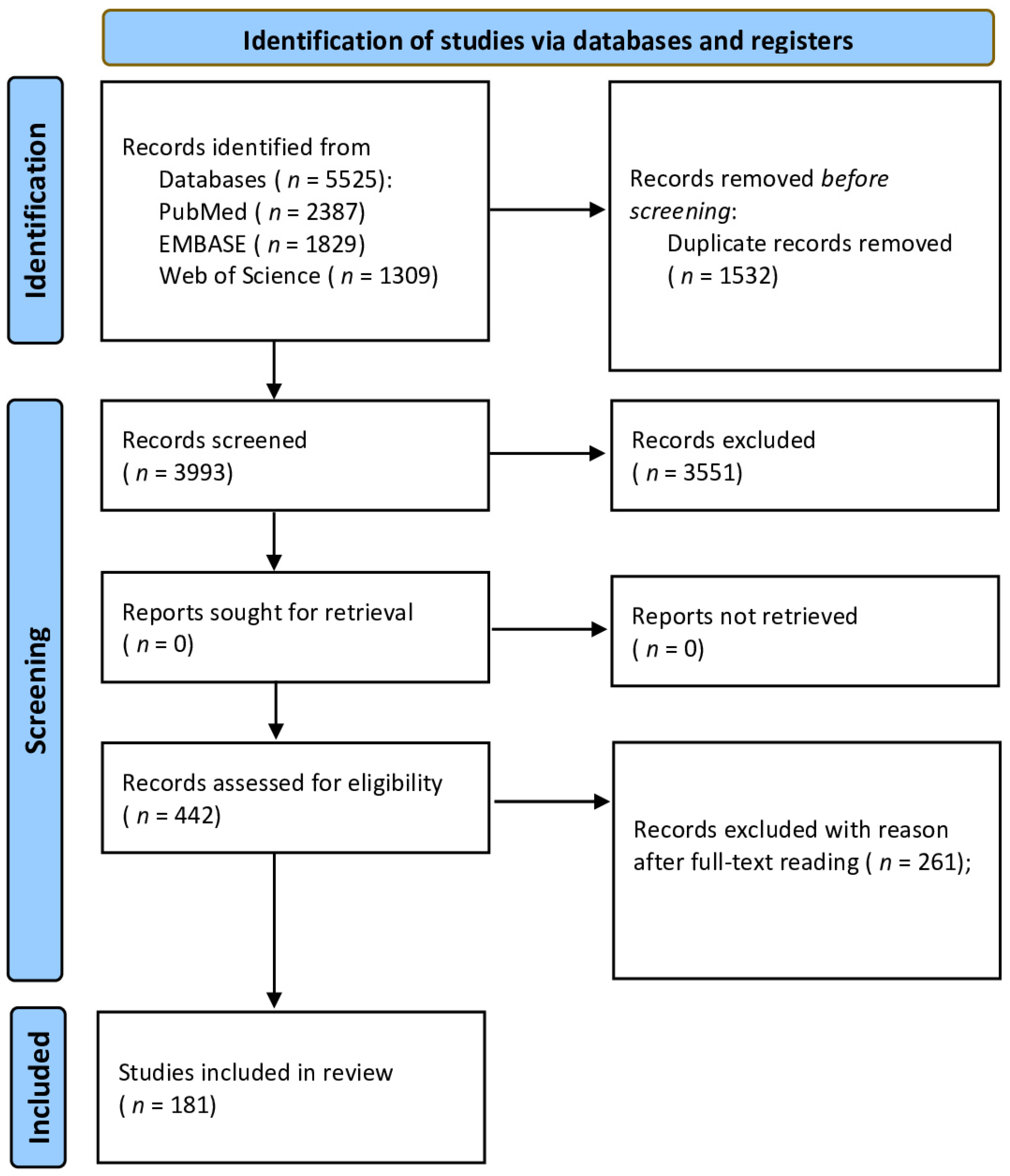
2. Materials and Methods
3. Results
3.1. Prevalence of Caries
3.2. Caries Experience (DMFT)
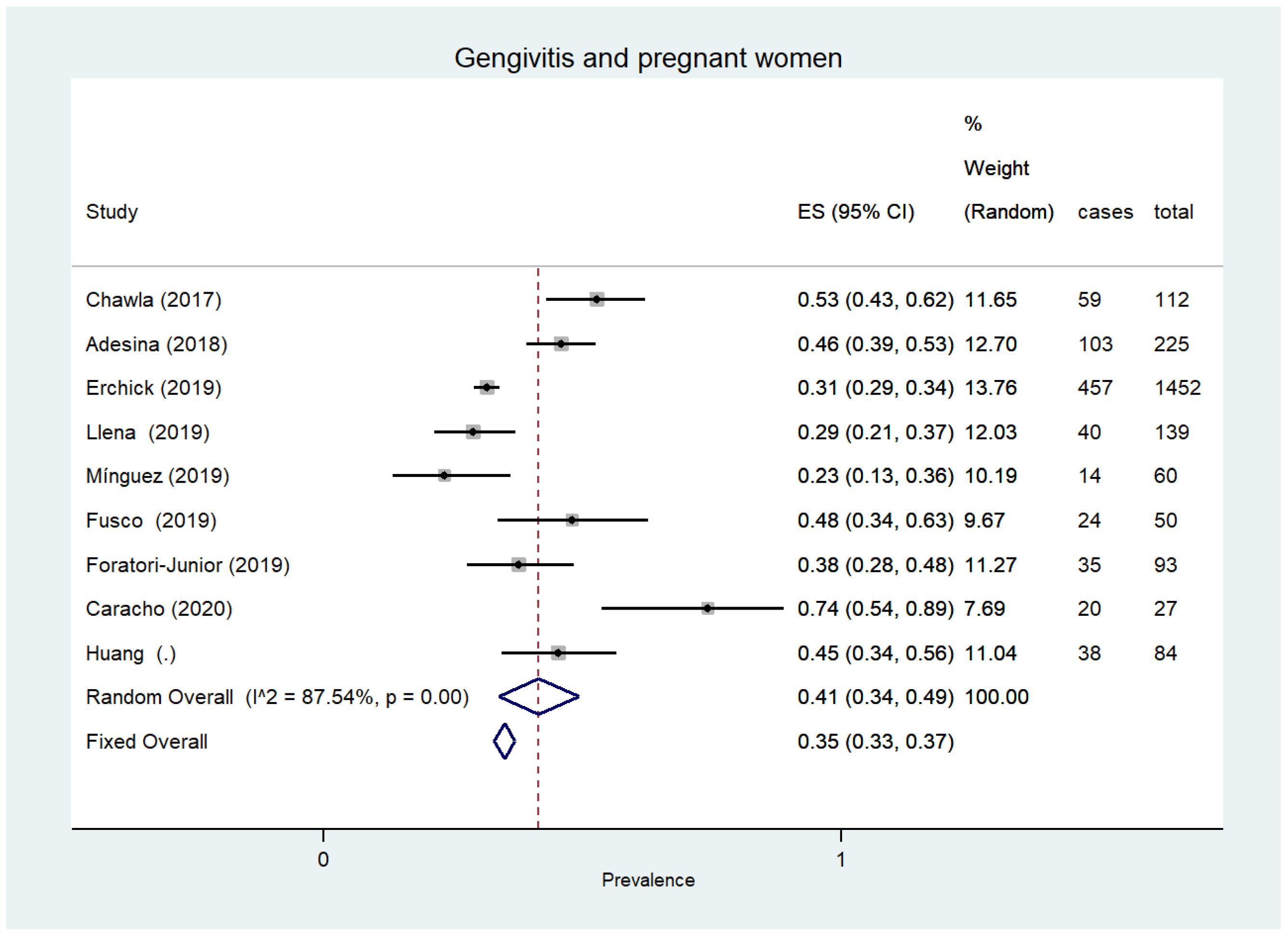
3.3. Gingivitis
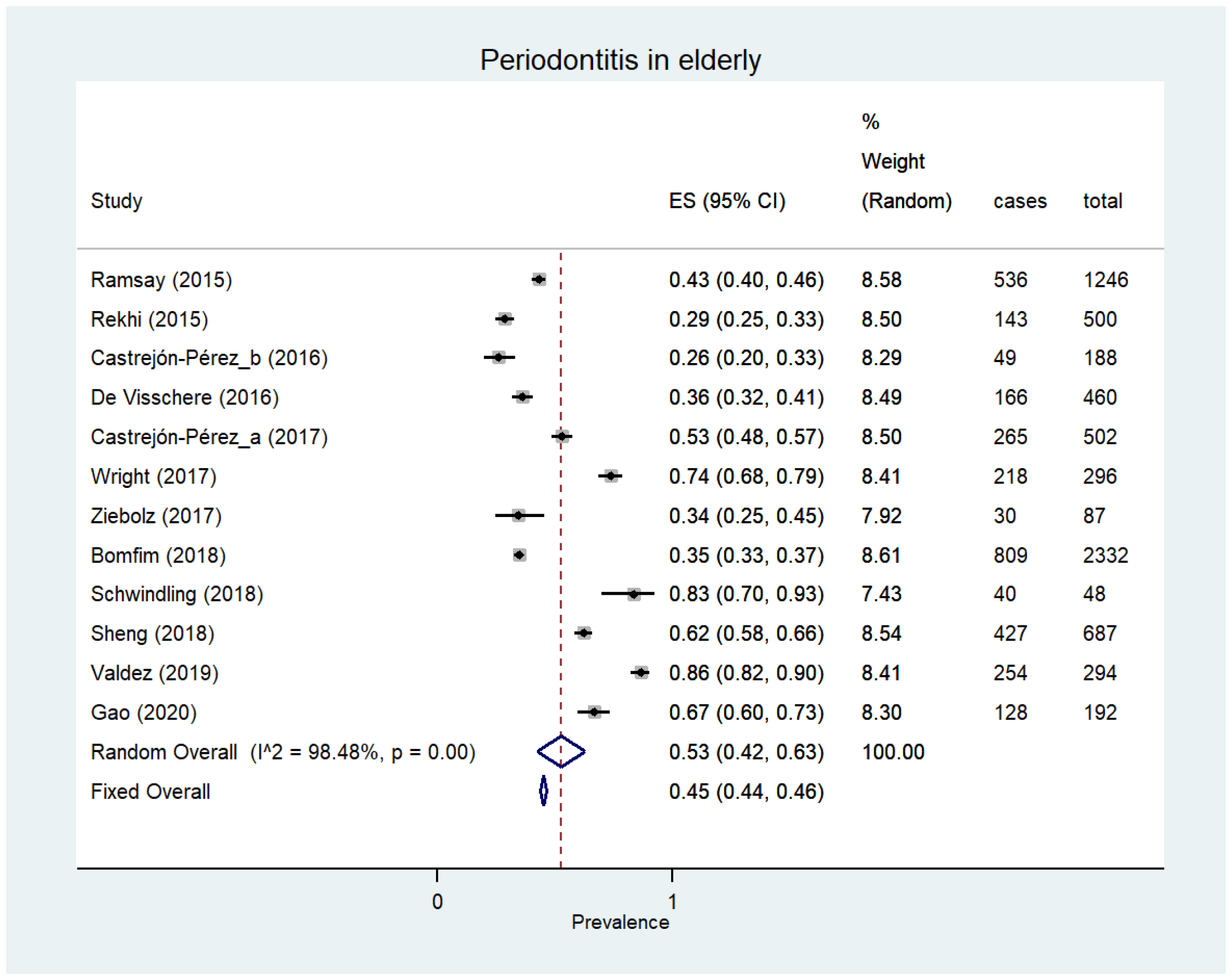
3.4. Periodontitis
3.5. Complete Edentulism
3.6. Partial Tooth Loss (Partial Edentulism)
3.6.1. The Elderly
3.6.2. Low-Education People
3.6.3. Low-Income People
3.6.4. Ethnic/Race Minorities
3.6.5. Populations Living in Rural Areas
3.6.6. Subjects with Precarious/Unhealthy Working Conditions
3.6.7. Subjects with Negative Experiences in Childhood
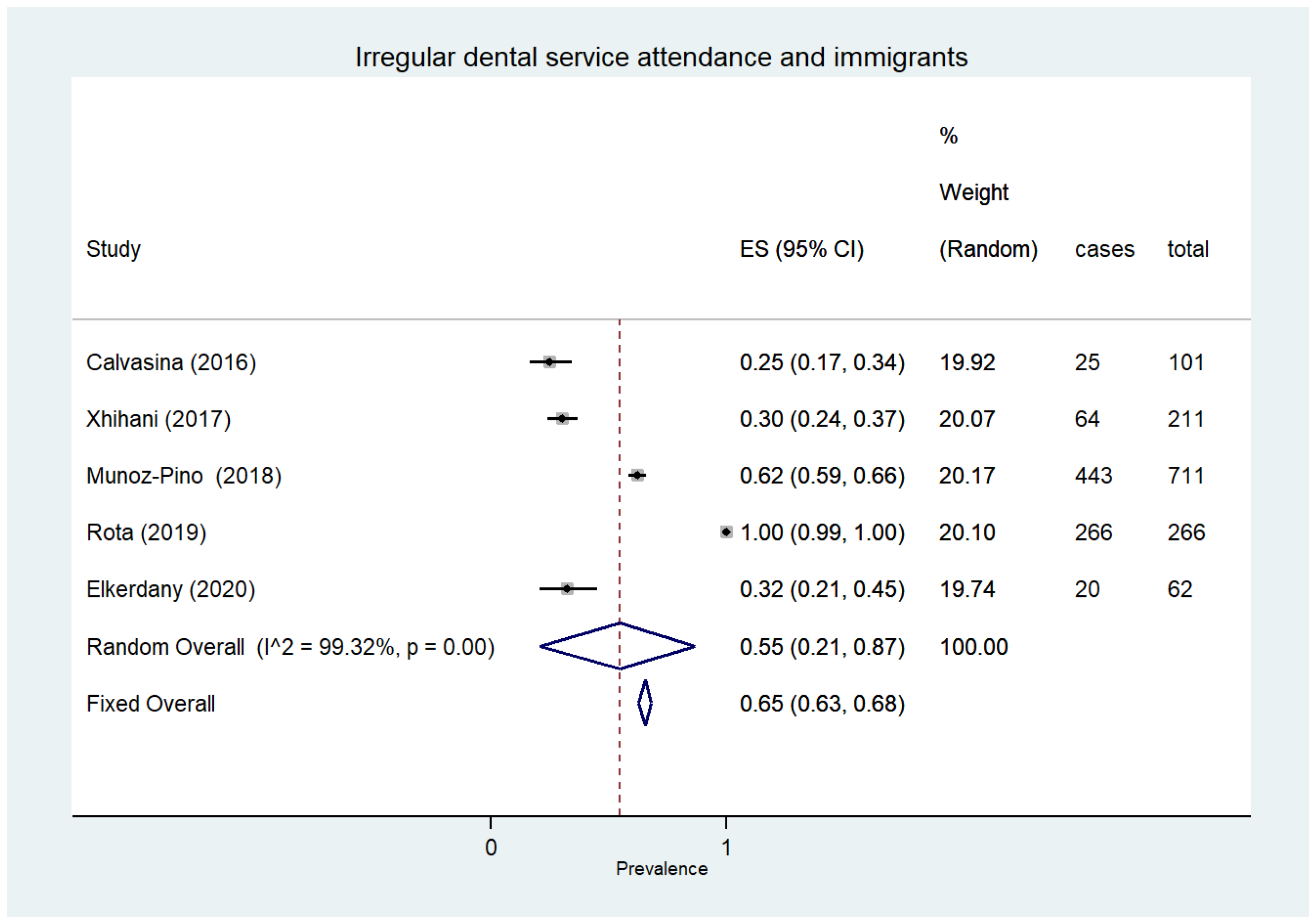
3.7. Dental Service Attendance
3.8. Oral Health-Related Quality of Life (OHRQoL)
3.9. Oral Health Perception
3.10. Emergency Room Treatments Due to Non-Traumatic Injuries
3.11. People with Multiple Social Vulnerabilities
3.12. Quality Assessment of Included Studies
4. Discussion
Limitations
- Considering the scope of providing an overall view of dental–periodontal health involving all types of socially vulnerable subjects, this review does not present a complete picture for two reasons. The first reason is that in the literature (consequently in our review), not all types of vulnerable subjects are mentioned in relation to their dental–periodontal health. The second reason is that in many groups of vulnerable subjects, not all the dental–periodontal health outcomes (those indicated in the “Materials and Methods” section of this review) were described, and in some cases even the primary ones were missing.
- The high level of heterogeneity (I2 > 90%) of results relative to the majority of the outcomes in this review reduces the reliability of conclusions on the dental–periodontal health of vulnerable subjects, who were the focus of our research
- This systematic review did not take into account the differences between developing and underdeveloped countries in the assessment of socially vulnerable people. This was to limit any subgroup analysis (especially in some groups of vulnerable subjects described by only a few studies with a reduced number of participants) in order to avoid the risk of compromising the accuracy of the results by reducing the sample size of enrolled individuals.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Marmot, M. Social determinants of health inequalities. Lancet 2005, 365, 1099–1104. [Google Scholar] [CrossRef]
- Kåks, P.; Målqvist, M. Peer support for disadvantaged parents: A narrative review of strategies used in home visiting health interventions in high-income countries. BMC Health Serv. Res. 2020, 20, 682. [Google Scholar] [CrossRef]
- Stormacq, C.; Van den Broucke, S.; Wosinski, J. Does health literacy mediate the relationship between socioeconomic status and health disparities? Integrative review. Health Promot. Int. 2019, 34, e1–e17. [Google Scholar] [CrossRef] [PubMed]
- Rune, H.C.; Nielsen, H.O. Disparities in Quality of Work Linked to Education and Socioeconomic Status; European Foundation for the Improvement of Living and Working Conditions: Dublin, Ireland, 2009. [Google Scholar]
- Mabhala, M.A.; Yohannes, A.; Griffith, M. Social conditions of becoming homelessness: Qualitative analysis of life stories of homeless peoples. Int. J. Equity Health 2017, 16, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frick, K.; Bopp, A. Poverty: Insurance Theory and the Medically Uninsured. Atl. Econ. J. 2005, 33, 451–459. [Google Scholar] [CrossRef]
- Rechel, B.; Mladovsky, P.; Ingleby, D.; Mackenbach, J.P.; McKee, M. Migration and health in an increasingly diverse Europe. Lancet 2013, 381, 1235–1245. [Google Scholar] [CrossRef]
- Aldridge, R.W.; Story, A.; Hwang, S.W.; Nordentoft, M.; Luchenski, S.A.; Hartwell, G.; Tweed, E.J.; Lewer, D.; VittalKatikireddi, S.; Hayward, A.C. Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: A systematic review and meta-analysis. Lancet 2018, 391, 241–250. [Google Scholar] [CrossRef] [Green Version]
- Moghaddam, L.F.; Vettore, M.V.; Bayani, A.; Bayat, A.H.; Ahounbar, E.; Hemmat, M.; Armoon, B.; Fakhri, Y. The Association of Oral Health Status, demographic characteristics and socioeconomic determinants with Oral health-related quality of life among children: A systematic review and Meta-analysis. BMC Pediatr. 2020, 20, 489. [Google Scholar] [CrossRef]
- Valtorta, N.K.; Moore, D.C.; Barron, L.; Stow, D.; Hanratty, B. Older Adults’ Social Relationships and Health Care Utilization: A Systematic Review. Am. J. Public Health 2018, 108, e1–e10. [Google Scholar] [CrossRef]
- Van der Zande, I.S.E.; van der Graaf, R.; Oudijk, M.A.; van Delden, J.J.M. Vulnerability of pregnant women in clinical research. J Med. Ethics 2017, 43, 657–663. [Google Scholar] [CrossRef]
- Waisel, D.B. Vulnerable populations in healthcare. Curr. Opin. Anaesthesiol. 2013, 26, 186–192. [Google Scholar] [CrossRef]
- Brooks, H.; Llewellyn, C.D.; Nadarzynski, T.; Pelloso, F.C.; De Souza Guilherme, F.; Pollard, A.; Jones, C.J. Sexual orientation disclosure in health care: A systematic review. Br. J. Gen.Pract. 2018, 68, e187–e196. [Google Scholar] [CrossRef]
- Allen, L.; Williams, J.; Townsend, N.; Mikkelsen, B.; Roberts, N.; Foster, C.; Wickramasinghe, K. Socioeconomic status and non-communicable disease behavioural risk factors in low-income and lower-middle-income countries: A systematic review. Lancet Glob. Health 2017, 5, e277–e289. [Google Scholar] [CrossRef] [Green Version]
- Probst, L.F.; Pucca Junior, G.A.; Pereira, A.C.; Carli, A.D. Impact of financial crises on oral health indicators: An integrative review of the literature. Cien. Saude Colet. 2019, 24, 4437–4448. [Google Scholar] [CrossRef] [PubMed]
- Hurley, R. Legalise and regulate illicit drugs to reduce poverty, say campaigners. BMJ 2019, 364, l317. [Google Scholar] [CrossRef]
- Jepsen, S.; Blanco, J.; Buchalla, W.; Carvalho, J.C.; Dietrich, T.; Dörfer, C.; Eaton, K.A.; Figuero, E.; Frencken, J.E.; Graziani, F.; et al. Prevention and control of dental caries and periodontal diseases at individual and population level: Consensus report of group 3 of joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J. Clin. Periodontol. 2017, 44 (Suppl.18), S85–S93. [Google Scholar] [CrossRef]
- González Navarro, B.; Pintó Sala, X.; Jané Salas, E. Relationship between cardiovascular disease and dental pathology. Systematic review. Med. Clin. 2017, 149, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Philadelphia, PA, USA, 2020. [Google Scholar]
- Priwe, C.; Carlsson, P. Oral Health Status of Male Swedish Citizens at Admission to Prison. J. Correct Health Care 2018, 24, 382–394. [Google Scholar] [CrossRef]
- Fotedar, S.; Chauhan, A.; Bhardwaj, V.; Manchanda, K.; Fotedar, V. Association between oral health status and oral health-related quality of life among the prison inmate population of kanda model jail, Shimla, Himachal Pradesh, India. Indian J. Public Health 2016, 60, 150–153. [Google Scholar] [CrossRef]
- Soares, G.H.; Mendonça, I.; Michel-Crosato, E.; Moysés, S.J.; Moysés, S.T.; Werneck, R.I. Impact of oral conditions on the quality of life of incarcerated women in Brazil. Health Care Women Int. 2019, 40, 776–787. [Google Scholar] [CrossRef] [PubMed]
- Álvarez, L.; Liberman, J.; Abreu, S.; Mangarelli, C.; Correa, M.B.; Demarco, F.F.; Lorenzo, S.; Nascimento, G.G. Dental caries in Uruguayan adults and elders: Findings from the first Uruguayan National Oral Health Survey. Cad. Saude Publica 2015, 31, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Martin, N.R.; Kelly, S.M.; Brown, H.A. Oral Health Status of Older Adults Attending Senior Centers and Congregate Meal Sites in New Hampshire. J. Dent. Hyg. 2016, 90, 128–134. [Google Scholar] [PubMed]
- Andersson, P.; Renvert, S.; Sjogren, P.; Zimmerman, M. Dental status in nursing home residents with domiciliary dental care in Sweden. Community Dent. Health 2017, 34, 203–207. [Google Scholar]
- De Visschere, L.; Janssens, B.; De Reu, G.; Duyck, J.; Vanobbergen, J. An oral health survey of vulnerable older people in Belgium. Clin. Oral Investig. 2016, 20, 1903–1912. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.B.; Hu, T.; Zhou, X.D.; Shao, R.; Cheng, R.; Wang, G.S.; Yang, Y.M.; Li, X.; Yuan, B.; Xu, T.; et al. How Root Caries Differs between Middle-aged People and the Elderly: Findings from the 4th National Oral Health Survey of China. Chin. J. Dent. Res. 2018, 21, 221–229. [Google Scholar]
- Gao, Y.B.; Hu, T.; Zhou, X.D.; Shao, R.; Cheng, R.; Wang, G.S.; Yang, Y.M.; Li, X.; Yuan, B.; Xu, T.; et al. Dental Caries in Chinese Elderly People: Findings from the 4th National Oral Health Survey. Chin. J. Dent. Res. 2018, 21, 213–220. [Google Scholar]
- Głowacka, B.; Konopka, T. Needs for gerodontological treatment in the elderly living in Lower Silesia. Dent. Med. Probl. 2019, 56, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Hoeksema, A.R.; Peters, L.L.; Raghoebar, G.M.; Meijer, H.J.A.; Vissink, A.; Visser, A. Health and quality of life differ between community living older people with and without remaining teeth who recently received formal home care: A cross sectional study. Clin. Oral Investig. 2018, 22, 2615–2622. [Google Scholar] [CrossRef] [Green Version]
- Hoeksema, A.R.; Spoorenberg, S.; Peters, L.L.; Meijer, H.; Raghoebar, G.M.; Vissink, A.; Wynia, K.; Visser, A. Elderly with remaining teeth report less frailty and better quality of life than edentulous elderly: A cross-sectional study. Oral. Dis. 2017, 23, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Janssens, B.; Vanobbergen, J.; Petrovic, M.; Jacquet, W.; Schols, J.M.G.A.; De Visschere, L. The oral health condition and treatment needs assessment of nursing home residents in Flanders (Belgium). Community Dent. Health 2017, 34, 143–151. [Google Scholar]
- León, S.; Bravo-Cavicchioli, D.; Giacaman, R.A.; Correa-Beltrán, G.; Albala, C. Validation of the Spanish version of the oral health impact profile to assess an association between quality of life and oral health of elderly Chileans. Gerodontology 2016, 33, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.L.; Boyd, L.D.; Tapias-Perdigón, H.; LaSpina, L.M. Oral Health Status of Independent Older Adults in Texas: An observational study comparing urban and rural areas. J. Dent. Hyg. 2017, 91, 40–47. [Google Scholar]
- Monaghan, N.; Karki, A.; Playle, R.; Johnson, I.; Morgan, M. Measuring oral health impact among care home residents in Wales. Community Dent. Health 2017, 34, 14–18. [Google Scholar] [PubMed]
- Niesten, D.; Witter, D.; Bronkhorst, E.; Creugers, N. Oral health-related quality of life and associated factors in a care-dependent and a care-independent older population. J. Dent. 2016, 55, 33–39. [Google Scholar] [CrossRef]
- Olerud, E.; Hagman-Gustavsson, M.L.; Gabre, P. Oral health status in older immigrants in a medium-sized Swedish city. Spec Care Dentist. 2016, 36, 328–334. [Google Scholar] [CrossRef]
- Rekhi, A.; Marya, C.M.; Nagpal, R.; Oberoi, S.S. Assessment of Oral Health Related Quality of Life Among the Institutionalised Elderly in Delhi, India. Oral Health Prev Dent. 2018, 16, 59–66. [Google Scholar]
- Rosa, R.W.; Samot, J.; Helmer, C.; Pourtau, G.; Dupuis, V.; Fricain, J.C.; Georget, A.; Dartigues, J.F.; Arrivé, E. Important oral care needs of older French people: A cross-sectional study. Rev. Epidemiol. SantePublique 2020, 68, 83–90. [Google Scholar] [CrossRef]
- Saintrain, M.V.L.; Saintrain, S.V.; Sampaio, E.G.M.; Ferreira, B.S.P.; Nepomuceno, T.C.; Frota, M.A.; Vieira-Meyer, A.P. Older adults’ dependence in activities of daily living: Implications for oral health. Public Health Nurs. 2018, 35, 473–481. [Google Scholar] [CrossRef]
- Sheng, X.; Xiao, X.; Song, X.; Qiao, L.; Zhang, X.; Zhong, H. Correlation between oral health and quality of life among the elderly in Southwest China from 2013 to 2015. Medicine 2018, 97, e10777. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Purohit, B.M.; Masih, N. Geriatric oral health predicaments in New Delhi, India. Geriatr. Gerontol. Int. 2016, 16, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Souza, J.G.S.; Costa Oliveira, B.E.; Sampaio, A.A.; Lages, V.A.; Romão, D.A.; Martins, A.M.E.B.L. Contextual and Individual Determinants of Root Caries in Older People. Caries Res. 2018, 52, 253–261. [Google Scholar] [CrossRef]
- Tapias Perdigon, H.; Schneiderman, E.; Opperman, L.A. Oral health assessment of independent elders in Texas. Spec. Care Dentist. 2019, 39, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Valdez, E.; Wright, F.A.C.; Naganathan, V.; Milledge, K.; Blyth, F.M.; Hirani, V.; Le Couteur, D.G.; Handelsman, D.J.; Waite, L.M.; Cumming, R.G. Frailty and oral health: Findings from the Concord Health and Ageing in Men Project. Gerodontology 2020, 37, 28–37. [Google Scholar] [CrossRef]
- Wang, L.; Cheng, L.; Yuan, B.; Hong, X.; Hu, T. Association between socio-economic status and dental caries in elderly people in Sichuan Province, China: A cross-sectional study. BMJ Open 2017, 7, e016557. [Google Scholar] [CrossRef] [Green Version]
- Sordi, M.B.; Massochin, R.C.; Camargo, A.R.; Lemos, T.; Munhoz, E.A. Oral health assessment for users of marijuana and cocaine/crack substances. Braz. Oral Res. 2017, 31, e102. [Google Scholar] [CrossRef] [Green Version]
- Shetty, V.; Harrell, L.; Murphy, D.A.; Vitero, S.; Gutierrez, A.; Belin, T.R.; Dye, B.A.; Spolsky, V.W. Dental disease patterns in methamphetamine users: Findings in a large urban sample. J. Am. Dent. Assoc. 2015, 146, 875–885. [Google Scholar] [CrossRef] [Green Version]
- Muñoz-Pino, N.; Vives-Cases, C.; Agudelo-Suárez, A.A.; Ronda-Pérez, E. Comparing Oral Health Services Use in the Spanish and Immigrant Working Population. J. Immigr. Minor. Health 2018, 20, 809–815. [Google Scholar] [CrossRef]
- Høyvik, A.C.; Lie, B.; Grjibovski, A.M.; Willumsen, T. Oral Health Challenges in Refugees from the Middle East and Africa: A Comparative Study. J. Immigr. Minor Health 2019, 21, 443–450. [Google Scholar] [CrossRef] [Green Version]
- Adesina, K.T.; Ernest, M.A.; Tobin, A.O.; Isiaka-Lawal, S.A.; Adeyemi, M.F.; Olarinoye, A.O.; Ezeoke, G.G. Oral health status of pregnant women in Ilorin, Nigeria. J. Obstet. Gynaecol. 2018, 38, 1093–1098. [Google Scholar] [CrossRef]
- Chawla, R.M.; Shetiya, S.H.; Agarwal, D.R.; Mitra, P.; Bomble, N.A.; Narayana, D.S. Knowledge, Attitude, and Practice of Pregnant Women regarding Oral Health Status and Treatment Needs following Oral Health Education in Pune District of Maharashtra: A Longitudinal Hospital-based Study. J. Contemp. Dent. Pract. 2017, 18, 371–377. [Google Scholar] [CrossRef]
- Llena, C.; Nakdali, T.; Sanz, J.L.; Forner, L. Oral Health Knowledge and Related Factors among Pregnant Women Attending to a Primary Care Center in Spain. Int. J. Environ Res. Public Health 2019, 16, 5049. [Google Scholar] [CrossRef] [Green Version]
- Lambert, M.; De Reu, G.; De Visschere, L.; Declerck, D.; Bottenberg, P.; Vanobbergen, J. Social gradient in caries experience of Belgian adults 2010. Community Dent. Health 2018, 35, 160–166. [Google Scholar] [PubMed]
- Nogueira, J.S.; Pereira, A.C.; Frias, A.C.; Ambrosano, G.M.B.; Cortellazzi, K.L.; Guerra, L.M.; Cavalcante, D.F.B.; Bulgareli, J.V. Social capital and factors associated with the caries experience in adults—A population-based study in Brazil. Braz. Oral Res. 2019, 33, e118. [Google Scholar] [CrossRef] [PubMed]
- Wilson, F.A.; Wang, Y.; Borrell, L.N.; Bae, S.; Stimpson, J.P. Disparities in oral health by immigration status in the United States. J. Am. Dent. Assoc. 2018, 149, 414–421.e3. [Google Scholar] [CrossRef]
- Tafere, Y.; Chanie, S.; Dessie, T.; Gedamu, H. Assessment of prevalence of dental caries and the associated factors among patients attending dental clinic in Debre Tabor general hospital: A hospital-based cross-sectional study. BMC Oral Health 2018, 18, 119. [Google Scholar] [CrossRef] [Green Version]
- Janssens, B.; Vanobbergen, J.; Petrovic, M.; Jacquet, W.; Schols, J.M.; De Visschere, L. The impact of a preventive and curative oral healthcare program on the prevalence and incidence of oral health problems in nursing home residents. PLoS ONE 2018, 13, e0198910. [Google Scholar] [CrossRef] [Green Version]
- Klotz, A.L.; Zajac, M.; Ehret, J.; Kilian, S.; Rammelsberg, P.; Zenthöfer, A. Short-Term Effects of a Deterioration of General Health on the Oral Health of Nursing-Home Residents. Clin. Interv. Aging 2020, 15, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Mulic, A.; Tveit, A.B.; Stenhagen, K.R.; Oscarson, N.; Staxrud, F.; Jönsson, B. The frequency of enamel and dentin caries lesions among elderly Norwegians. Acta Odontol. Scand. 2020, 78, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Puturidze, S.; Margvelashvili, M.; Bilder, L.; Kalandadze, M.; Margvelashvili, V. Correlation of oral health status with general health in elderly living at residential homes in georgia. Georgian Med. News 2019, 292–293, 21–25. [Google Scholar]
- Sáez-Prado, B.; Haya-Fernández, M.C.; Sanz-García, M.T. Oral health and quality of life in the municipal senior citizen’s social clubs for people over 65 of Valencia, Spain. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e672–e678. [Google Scholar]
- Skośkiewicz-Malinowska, K.; Noack, B.; Kaderali, L.; Malicka, B.; Lorenz, K.; Walczak, K.; Weber, M.T.; Mendak-Ziółko, M.; Hoffmann, T.; Ziętek, M.; et al. Oral Health and Quality of Life in Old Age: A Cross-Sectional Pilot Project in Germany and Poland. Adv. Clin. Exp. Med. 2016, 25, 951–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, F.A.C.; Law, G.; Chu, S.K.; Cullen, J.S.; Le Couteur, D.G. Residential age care and domiciliary oral health services: Reach-OHT-The development of a metropolitan oral health programme in Sydney, Australia. Gerodontology 2017, 34, 420–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stormon, N.; Pradhan, A.; McAuliffe, A.; Ford, P.J. Does a facilitated pathway improve access to dental services for homeless and disadvantaged adults? Eval. Program Plann. 2018, 71, 46–50. [Google Scholar] [CrossRef] [Green Version]
- Doughty, J.; Stagnell, S.; Shah, N.; Vasey, A.; Gillard, C. The Crisis at Christmas Dental Service: A review of an annual volunteer-led dental service for homeless and vulnerably housed people in London. Br. Dent. J. 2018, 224, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Aukštakalnis, R.; Jurgelevičius, T. The oral health status and behaviour of methadone users in Lithuania. Stomatologija 2018, 20, 27–31. [Google Scholar]
- Clague, J.; Belin, T.R.; Shetty, V. Mechanisms underlying methamphetamine-related dental disease. J. Am. Dent. Assoc. 2017, 148, 377–386. [Google Scholar] [CrossRef]
- Ye, T.; Sun, D.; Dong, G.; Xu, G.; Wang, L.; Du, J.; Ren, P.; Yu, S. The effect of methamphetamine abuse on dental caries and periodontal diseases in an Eastern China city. BMC Oral Health 2018, 18, 8. [Google Scholar] [CrossRef]
- Rafat, S.; Tessma, M.; Klinge, B.; Borg, S.; De Palma, P. Oral Health Among Swedish Patients with Substance Use Disorders—A Comparative, Cross-Sectional Study. Oral Health Prev. Dent. 2020, 18, 229–237. [Google Scholar]
- Manicone, P.F.; Tarli, C.; Mirijello, A.; Raffaelli, L.; Vassallo, G.A.; Antonelli, M.; Rando, M.M.; Mosoni, C.; Cossari, A.; Lavorgna, L.; et al. Dental health in patients affected by alcohol use disorders: A cross-sectional study. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 5021–5027. [Google Scholar]
- Marques, T.C.; Sarracini, K.L.; Cortellazzi, K.L.; Mialhe, F.L.; de Castro Meneghim, M.; Pereira, A.C.; Ambrosano, G.M. The impact of oral health conditions, socioeconomic status and use of specific substances on quality of life of addicted persons. BMC Oral Health 2015, 15, 38. [Google Scholar] [CrossRef] [Green Version]
- Rommel, N.; Rohleder, N.H.; Koerdt, S.; Wagenpfeil, S.; Härtel-Petri, R.; Wolff, K.D.; Kesting, M.R. Sympathomimetic effects of chronic methamphetamine abuse on oral health: A cross-sectional study. BMC Oral Health 2016, 16, 59. [Google Scholar] [CrossRef] [Green Version]
- Arrica, M.; Carta, G.; Cocco, F.; Cagetti, M.G.; Campus, G.; Ierardo, G.; Ottolenghi, L.; Sale, S.; Strohmenger, L. Does a social/behavioural gradient in dental health exist among adults? A cross-sectional study. J. Int. Med. Res. 2017, 45, 451–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nouaman, M.N.; Meless, D.G.; Coffie, P.A.; Arrivé, E.; Tchounga, B.K.; Ekouévi, D.K.; Anoma, C.; Eholié, S.P.; Dabis, F.; Jaquet, A.; et al. Oral health and HIV infection among female sex workers in Abidjan, Côte d’Ivoire. BMC Oral Health 2015, 15, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, B.V.; Suresh Babu, A.M.; Kamalsha, S.K.; Rao, M.S.; Karthik, K. Oral Health Status and Treatment Needs of Gunj Marketing Yard Laborers of Raichur City, Karnataka. J. Pharm.Bioallied. Sci. 2017, 9, 195–200. [Google Scholar] [CrossRef]
- Yoshino, K.; Suzuki, S.; Ishizuka, Y.; Takayanagi, A.; Sugihara, N.; Kamijyo, H. Relationship between job stress and subjective oral health symptoms in male financial workers in Japan. Ind. Health 2017, 55, 119–126. [Google Scholar] [CrossRef] [Green Version]
- Yoshino, K.; Suzuki, S.; Ishizuka, Y.; Takayanagi, A.; Sugihara, N.; Kamijyo, H. Relationship between amount of overtime work and untreated decayed teeth in male financial workers in Japan. J. Occup Health 2017, 59, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Ziebolz, D.; Werner, C.; Schmalz, G.; Nitschke, I.; Haak, R.; Mausberg, R.F.; Chenot, J.F. Oral Health and nutritional status in nursing home residents-results of an explorative cross-sectional pilot study. BMC Geriatr. 2017, 17, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, F.; Chu, S.Y.; Milledge, K.L.; Valdez, E.; Law, G.; Hsu, B.; Naganathan, V.; Hirani, V.; Blyth, F.M.; Le Couteur, D.G.; et al. Oral health of community-dwelling older Australian men: The Concord Health and Ageing in Men Project (CHAMP). Aust. Dent. J. 2018, 63, 55–65. [Google Scholar] [CrossRef]
- Caracho, R.A.; Foratori-Junior, G.A.; Fusco, N.D.S.; Jesuino, B.G.; Missio, A.L.T.; Sales-Peres, S.H.C. Systemic conditions and oral health-related quality of life of pregnant women of normal weight and who are overweight. Int. Dent. J. 2020, 70, 287–295. [Google Scholar] [CrossRef]
- Erchick, D.J.; Rai, B.; Agrawal, N.K.; Khatry, S.K.; Katz, J.; LeClerq, S.C.; Reynolds, M.A.; Mullany, L.C. Oral hygiene, prevalence of gingivitis, and associated risk factors among pregnant women in Sarlahi District, Nepal. BMC Oral Health 2019, 19, 2. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; DerGarabedian, B.P.; He, L.; Sha, Y.; Chen, Z.; Kang, J.; Cai, Y.; Gao, P. Impact of Periodonto-pathogenic Microbiota and Sociodemographic Variables on Periodontal Status during Pregnancy and Postpartum Period. Oral Health Prev. Dent. 2020, 18, 855–864. [Google Scholar]
- Gil, L.; Mínguez, I.; Caffesse, R.; Llambés, F. Periodontal Disease in Pregnancy: The Influence of General Factors and Inflammatory Mediators. Oral Health Prev. Dent. 2019, 17, 69–73. [Google Scholar] [PubMed]
- Fusco, N.D.S.; Foratori-Junior, G.A.; Missio, A.L.T.; Jesuino, B.G.; Sales-Peres, S.H.C. Systemic and oral conditions of pregnant women with excessive weight assisted in a private health system. Int. Dent. J. 2019, 69, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Foratori-Junior, G.A.; da Silva, B.M.; da Silva Pinto, A.C.; Honório, H.M.; Groppo, F.C.; de Carvalho Sales-Peres, S.H. Systemic and periodontal conditions of overweight/obese patients during pregnancy and after delivery: A prospective cohort. Clin. Oral Investig. 2020, 24, 157–165. [Google Scholar] [CrossRef]
- Bomfim, R.A.; Frias, A.C.; Pannuti, C.M.; Zilbovicius, C.; Pereira, A.C. Socio-economic factors associated with periodontal conditions among Brazilian elderly people—Multilevel analysis of the SBSP-15 study. PLoS ONE 2018, 13, e0206730. [Google Scholar]
- Castrejón-Pérez, R.C.; Jiménez-Corona, A.; Bernabé, E.; Villa-Romero, A.R.; Arrivé, E.; Dartigues, J.F.; Gutiérrez-Robledo, L.M.; Borges-Yáñez, S.A. Oral Disease and 3-Year Incidence of Frailty in Mexican Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 951–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, S.S.; Chen, K.J.; Duangthip, D.; Lo, E.C.M.; Chu, C.H. The Oral Health Status of Chinese Elderly People with and without Dementia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 1913. [Google Scholar] [CrossRef] [Green Version]
- Ramsay, S.E.; Whincup, P.H.; Watt, R.G.; Tsakos, G.; Papacosta, A.O.; Lennon, L.T.; Wannamethee, S.G. Burden of poor oral health in older age: Findings from a population-based study of older British men. BMJ Open 2015, 5, e009476. [Google Scholar] [CrossRef] [Green Version]
- Rantzow, V.; Andersson, P.; Lindmark, U. Occurrence of oral health problems and planned measures in dependent older people in nursing care. J. Clin. Nurs. 2018, 27, 4381–4389. [Google Scholar] [CrossRef]
- Rekhi, A.; Marya, C.M.; Oberoi, S.S.; Nagpal, R.; Dhingra, C.; Kataria, S. Periodontal status and oral health-related quality of life in elderly residents of aged care homes in Delhi. Geriatr. Gerontol. Int. 2016, 16, 474–480. [Google Scholar] [CrossRef]
- Hakeem, F.F.; Sabbah, W. Is there socioeconomic inequality in periodontal disease among adults with optimal behaviours. Acta Odontol. Scand. 2019, 77, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Han, K.; Vu, D.; Cho, K.H.; Lee, S.H. Number of remaining teeth and its association with socioeconomic status in South Korean adults: Data from the Korean National Health and Nutrition Examination Survey 2012–2013. PLoS ONE 2018, 13, e0196594. [Google Scholar]
- Castrejón-Pérez, R.C.; Borges-Yáñez, S.A.; Irigoyen-Camacho, M.E.; Cruz-Hervert, L.P. Negative impact of oral health conditions on oral health related quality of life of community dwelling elders in Mexico city, a population based study. Geriatr. Gerontol. Int. 2017, 17, 744–752. [Google Scholar] [CrossRef] [PubMed]
- Schwindling, F.S.; Krisam, J.; Hassel, A.J.; Rammelsberg, P.; Zenthöfer, A. Long-term success of oral health intervention among care-dependent institutionalized seniors: Findings from a controlled clinical trial. Community Dent. Oral Epidemiol. 2018, 46, 109–117. [Google Scholar] [CrossRef]
- Luo, H.; Hybels, C.F.; Wu, B. Acculturation, depression and oral health of immigrants in the USA. Int. Dent. J. 2018, 68, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.H.; Han, D.H. Exposure to occupational noise and periodontitis in Korean workers. J. Periodontol. 2018, 89, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Antoniazzi, R.P.; Zanatta, F.B.; Rösing, C.K.; Feldens, C.A. Association Among Periodontitis and the Use of Crack Cocaine and Other Illicit Drugs. J. Periodontol. 2016, 87, 1396–1405. [Google Scholar] [CrossRef]
- Lee, J.H.; Yi, S.K.; Kim, S.Y.; Kim, J.S.; Kim, H.N.; Jeong, S.H.; Kim, J.B. Factors Related to the Number of Existing Teeth among Korean Adults Aged 55-79 Years. Int. J. Environ. Res. Public Health 2019, 16, 3927. [Google Scholar] [CrossRef] [Green Version]
- Bhat, M.; Do, L.G.; Roberts-Thomson, K. Risk indicators for prevalence, extent and severity of periodontitis among rural Indian population aged 35–54 years. Int. J. Dent. Hyg. 2018, 16, 492–502. [Google Scholar] [CrossRef]
- Celeste, R.K.; Oliveira, S.C.; Junges, R. Threshold-effect of income on periodontitis and interactions with race/ethnicity and education. Rev. Bras. Epidemiol. 2019, 22, e190001. [Google Scholar] [CrossRef]
- Aida, J.; Kondo, K.; Yamamoto, T.; Saito, M.; Ito, K.; Suzuki, K.; Osaka, K.; Kawachi, I. Is Social Network Diversity Associated with Tooth Loss among Older Japanese Adults? PLoS ONE 2016, 11, e0159970. [Google Scholar] [CrossRef]
- Andrade, F.B.; Teixeira, D.S.D.C.; Frazão, P.; Duarte, Y.A.O.; Lebrão, M.L.; Antunes, J.L.F. Oral health profile among community-dwelling elderly and its association with self-rated oral health. Rev. Bras. Epidemiol. 2019, 21 (Suppl. 2), e180012. [Google Scholar]
- Bachkati, K.H.; Mortensen, E.L.; Brønnum-Hansen, H.; Holm-Pedersen, P. Midlife Cognitive Ability, Education, and Tooth Loss in Older Danes. J. Am. Geriatr. Soc. 2017, 65, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Bakker, M.H.; Vissink, A.; Spoorenberg, S.L.W.; Jager-Wittenaar, H.; Wynia, K.; Visser, A. Are Edentulousness, Oral Health Problems and Poor Health-Related Quality of Life Associated with Malnutrition in Community-Dwelling Elderly (Aged 75 Years and Over)? A Cross-Sectional Study. Nutrients 2018, 10, 1965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakker, M.H.; Vissink, A.; Spoorenberg, S.L.W.; Wynia, K.; Visser, A. Self-reported oral health problems and the ability to organize dental care of community-dwelling elderly aged ≥75 years. BMC Oral Health 2020, 20, 185. [Google Scholar] [CrossRef]
- Beker, N.; van der Maarel-Wierink, C.D.; de Baat, C.; Holstege, H. Self-reported oral health in the Dutch 100-plus Study of cognitively healthy centenarians: An observational cohort study. BMC Geriatr. 2019, 19, 355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiesi, F.; Grazzini, M.; Innocenti, M.; Giammarco, B.; Simoncini, E.; Garamella, G.; Zanobini, P.; Perra, C.; Baggiani, L.; Lorini, C.; et al. Older People Living in Nursing Homes: An Oral Health Screening Survey in Florence, Italy. Int. J. Environ. Res. Public Health 2019, 16, 3492. [Google Scholar] [CrossRef] [Green Version]
- Chiu, C.T.; Malhotra, R.; Tan, S.M.; Lim, J.; Chan, A.; Teoh, K.H.; Gan, S.T.; Saito, Y. Dental health status of community-dwelling older Singaporeans: Findings from a nationally representative survey. Gerodontology 2017, 34, 57–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cocco, F.; Campus, G.; Strohmenger, L.; Ardizzone, V.C.; Cagetti, M.G. The burden of tooth loss in Italian elderly population living in nursing homes. BMC Geriatr. 2018, 18, 76. [Google Scholar] [CrossRef]
- da Veiga Pessoa, D.M.; Roncalli, A.G.; de Lima, K.C. Economic and sociodemographic inequalities in complete denture need among older Brazilian adults: A cross-sectional population-based study. BMC Oral Health 2016, 17, 5. [Google Scholar] [CrossRef] [Green Version]
- Delwel, S.; Scherder, E.J.A.; Perez, R.S.G.M.; Hertogh, C.M.P.M.; Maier, A.B.; Lobbezoo, F. Oral function of older people with mild cognitive impairment or dementia. J. Oral Rehabil. 2018, 45, 990–997. [Google Scholar] [CrossRef] [PubMed]
- El Osta, N.; El Osta, L.; Khabbaz, L.R.; Saad, R.; Abi-Ghosn, C.; Hennequin, M.; Tubert-Jeannin, S.; Fakhouri, J. Social inequalities in oral health in a group of older people in a Middle Eastern country: A cross-sectional survey. Aging Clin. Exp. Res. 2018, 30, 1513–1521. [Google Scholar] [CrossRef]
- Furuta, M.; Takeuchi, K.; Adachi, M.; Kinoshita, T.; Eshima, N.; Akifusa, S.; Kikutani, T.; Yamashita, Y. Tooth loss, swallowing dysfunction and mortality in Japanese older adults receiving home care services. Geriatr. Gerontol. Int. 2018, 18, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.O.; Griffin, P.M.; Li, C.H.; Bailey, W.D.; Brunson, D.; Jones, J.A. Changes in Older Adults’ Oral Health and Disparities: 1999 to 2004 and 2011 to 2016. J. Am. Geriatr. Soc. 2019, 67, 1152–1157. [Google Scholar] [CrossRef]
- Han, D.H.; Khang, Y.H.; Choi, H.J. Association of parental education with tooth loss among Korean Elders. Community Dent. Oral Epidemiol. 2015, 43, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Heredia-Ponce, E.; Irigoyen-Camacho, A.E.; Sánchez-García, S. Oral Health Status of Institutionalized Older Women from Different Socioeconomic Positions. J. Health Care Poor Underserved 2017, 28, 1462–1476. [Google Scholar] [CrossRef]
- Hoeksema, A.R.; Peters, L.L.; Raghoebar, G.M.; Meijer, H.J.A.; Vissink, A.; Visser, A. Oral health status and need for oral care of care-dependent indwelling elderly: From admission to death. Clin. Oral Investig. 2017, 21, 2189–2196. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.N.; Jang, Y.E.; Kim, C.B.; Kim, N.H. Socioeconomic status and self-reported periodontal symptoms in community-dwelling individuals: Data from the Korea Community Health Surveys of 2011 and 2013. Int. Dent. J. 2018, 68, 411–419. [Google Scholar] [CrossRef]
- Koistinen, S.; Olai, L.; Ståhlnacke, K.; Fält, A.; Ehrenberg, A. Oral health-related quality of life and associated factors among older people in short-term care. Int. J. Dent. Hyg. 2020, 18, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Laguzzi, P.N.; Schuch, H.S.; Medina, L.D.; de Amores, A.R.; Demarco, F.F.; Lorenzo, S. Tooth loss and associated factors in elders: Results from a national survey in Uruguay. J. Public Health Dent. 2016, 76, 143–151. [Google Scholar] [CrossRef]
- Maille, G.; Saliba-Serre, B.; Ferrandez, A.M.; Ruquet, M. Objective and perceived oral health status of elderly nursing home residents: A local survey in southern France. Clin. Interv. Aging. 2019, 14, 1141–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maille, G.; Saliba-Serre, B.; Ferrandez, A.M.; Ruquet, M. Use of care and the oral health status of people aged 60 years and older in France: Results from the National Health and Disability Survey. Clin. Interv. Aging. 2017, 12, 1159–1166. [Google Scholar] [CrossRef] [Green Version]
- Matsuyama, Y.; Jürges, H.; Listl, S. The Causal Effect of Education on Tooth Loss: Evidence from United Kingdom Schooling Reforms. Am. J. Epidemiol. 2019, 188, 87–95. [Google Scholar] [CrossRef]
- Mehr, K.; Olszanecka-Glinianowicz, M.; Chudek, J.; Szybalska, A.; Mossakowska, M.; Zejda, J.; Wieczorowska-Tobis, K.; Grodzicki, T.; Piotrowski, P. Dental status in the Polish senior population and its correlates-Results of the national survey PolSenior. Gerodontology 2018, 35, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Nakahori, N.; Sekine, M.; Yamada, M.; Tatsuse, T.; Kido, H.; Suzuki, M. Socioeconomic status and remaining teeth in Japan: Results from the Toyama dementia survey. BMC Public Health 2019, 19, 691. [Google Scholar] [CrossRef] [Green Version]
- Nihtilä, A.; Tuuliainen, E.; Komulainen, K.; Autonen-Honkonen, K.; Nykänen, I.; Hartikainen, S.; Ahonen, R.; Tiihonen, M.; Suominen, A.L. Preventive oral health intervention among old home care clients. Age Ageing 2017, 46, 846–851. [Google Scholar] [CrossRef] [Green Version]
- Saito, M.; Shimazaki, Y.; Nonoyama, T.; Tadokoro, Y. Associations of number of teeth with medical costs and hospitalization duration in an older Japanese population. Geriatr. Gerontol. Int. 2019, 19, 335–341. [Google Scholar] [CrossRef]
- Silva, A.E.R.; Echeverria, M.S.; Custódio, N.B.; Cascaes, A.M.; Camargo, M.B.J.; Langlois, C.O. Regular use of dental services and dental loss among the elderly. Cien. Saude. Colet. 2018, 23, 4269–4276. [Google Scholar] [CrossRef]
- Tiwari, T.; Scarbro, S.; Bryant, L.L.; Puma, J. Factors Associated with Tooth Loss in Older Adults in Rural Colorado. J. Community Health 2016, 41, 476–481. [Google Scholar] [CrossRef]
- Yoon, M.N.; Ickert, C.; Slaughter, S.E.; Lengyel, C.; Carrier, N.; Keller, H. Oral health status of long-term care residents in Canada: Results of a national cross-sectional study. Gerodontology 2018, 35, 359–364. [Google Scholar] [CrossRef]
- Zhang, Q.; Jing, Q.; Gerritsen, A.E.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H. Dental status of an institutionalized elderly population of 60 years and over in Qingdao, China. Clin. Oral Investig. 2016, 20, 1021–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, S.; Austin, S.; Cohen, L.; Reed, D.; Poole, P.; Ward, K.; Sloane, P.D. Readily Identifiable Risk Factors of Nursing Home Residents’ Oral Hygiene: Dementia, Hospice, and Length of Stay. J. Am. Geriatr. Soc. 2017, 65, 2516–2521. [Google Scholar] [CrossRef] [PubMed]
- Rouxel, P.; Tsakos, G.; Demakakos, P.; Zaninotto, P.; Chandola, T.; Watt, R.G. Is Social Capital a Determinant of Oral Health among Older Adults? Findings from the English Longitudinal Study of Ageing. PLoS ONE 2015, 10, e0125557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weintraub, J.A.; Orleans, B.; Fontana, M.; Phillips, C.; Jones, J.A. Factors Associated With Becoming Edentulous in the US Health and Retirement Study. J. Am. Geriatr. Soc. 2019, 67, 2318–2324. [Google Scholar] [CrossRef]
- Caldwell, J.T.; Lee, H.; Cagney, K.A. The Role of Primary Care for the Oral Health of Rural and Urban Older Adults. J. Rural Health 2017, 33, 409–418. [Google Scholar] [CrossRef]
- Dahl, K.E.; Calogiuri, G.; Jönsson, B. Perceived oral health and its association with symptoms of psychological distress, oral status and socio-demographic characteristics among elderly in Norway. BMC Oral Health 2018, 18, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koistinen, S.; Olai, L.; Ståhlnacke, K.; Fält, A.; Ehrenberg, A. Oral health and oral care in short-term care: Prevalence, related factors and coherence between older peoples’ and professionals’ assessments. Scand. J. Caring Sci. 2019, 33, 712–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.S.; Kim, H.G.; Hur, J.Y.; Yang, K. Oral Health in Low-Income Older Adults in Korea. J. Community Health Nurs. 2016, 33, 98–106. [Google Scholar] [CrossRef]
- Mochida, Y.; Yamamoto, T.; Fuchida, S.; Aida, J.; Kondo, K. Does poor oral health status increase the risk of falls? The JAGES Project Longitudinal Study. PLoS ONE 2018, 13, e0192251. [Google Scholar]
- Nilsson, H.; Berglund, J.S.; Renvert, S. Periodontitis, tooth loss and cognitive functions among older adults. Clin. Oral Investig. 2018, 22, 2103–2109. [Google Scholar] [CrossRef]
- Okamoto, N.; Amano, N.; Nakamura, T.; Yanagi, M. Relationship between tooth loss, low masticatory ability, and nutritional indices in the elderly: A cross-sectional study. BMC Oral Health 2019, 19, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, C.G.; Cascaes, A.M.; Silva, A.E.; Seerig, L.M.; Nascimento, G.G.; Demarco, F.F. Edentulism, Severe Tooth Loss and Lack of Functional Dentition in Elders: A Study in Southern Brazil. Braz. Dent. J. 2016, 27, 345–352. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, S.; Konta, T.; Susa, S.; Kitabatake, K.; Ishizawa, K.; Togashi, H.; Tsuya, A.; Ueno, Y.; Kubota, I.; Yamashita, H.; et al. Risk factors for tooth loss in community-dwelling Japanese aged 40 years and older: The Yamagata (Takahata) study. Clin. Oral Investig. 2019, 23, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Gomes Filho, V.V.; Gondinho, B.V.C.; Silva-Junior, M.F.; Cavalcante, D.F.B.; Bulgareli, J.V.; Sousa, M.D.L.R.; Frias, A.C.; Batista, M.J.; Pereira, A.C. Tooth loss in adults: Factors associated with the position and number of lost teeth. Rev. Saude Publica 2019, 53, 105. [Google Scholar]
- Rodriguez, F.R.; Paganoni, N.; Weiger, R.; Walter, C. Lower Educational Level is a Risk Factor for Tooth Loss—Analysis of aSwiss Population (KREBS Project). Oral Health Prev. Dent. 2017, 15, 139–145. [Google Scholar] [PubMed]
- Novrinda, H.; Han, D.H.; Jung-Choi, K.; Ryu, J.I. Neo-Marxian social class inequalities in oral health among the South Korean population. Community Dent. Oral Epidemiol. 2019, 47, 162–170. [Google Scholar] [CrossRef]
- Wennström, A.; Boman, U.W.; Ahlqwist, M.; Björkelund, C.; Hakeberg, M. Perceived mental stress in relation to oral health over time in middle-aged Swedish women. Community Dent Health 2015, 32, 241–246. [Google Scholar]
- Song, I.S.; Han, K.; Choi, Y.J.; Ryu, J.J.; Park, J.B. Influence of oral health behavior and sociodemographic factors on remaining teeth in Korean adults: 2010–2012 Korea national health and nutrition examination survey. Medicine 2016, 95, e5492. [Google Scholar] [CrossRef]
- Steele, J.; Shen, J.; Tsakos, G.; Fuller, E.; Morris, S.; Watt, R.; Guarnizo-Herreño, C.; Wildman, J. The Interplay between socioeconomic inequalities and clinical oral health. J. Dent. Res. 2015, 94, 19–26. [Google Scholar] [CrossRef]
- Roberto, L.L.; Silveira, M.F.; de Paula, A.M.B.; Ferreira, E.; Ferreira, E.; Martins, A.M.E.B.L.; Haikal, D.S. Contextual and individual determinants of tooth loss in adults: A multilevel study. BMC Oral Health 2020, 20, 73. [Google Scholar] [CrossRef]
- Duijster, D.; Oude Groeniger, J.; van der Heijden, G.J.M.G.; van Lenthe, F.J. Material, behavioural, cultural and psychosocial factors in the explanation of socioeconomic inequalities in oral health. Eur. J. Public Health 2018, 28, 590–597. [Google Scholar] [CrossRef] [Green Version]
- Hach, M.; Christensen, L.B.; Lange, T.; Hvidtfeldt, U.A.; Danielsen, B.; Diderichsen, F.; Osler, M.; Prescott, E.; Andersen, I. Social inequality in tooth loss, the mediating role of smoking and alcohol consumption. Community Dent. Oral Epidemiol. 2019, 47, 416–423. [Google Scholar] [CrossRef]
- Goulart Mde, A.; Vettore, M.V. Is the relative increase in income inequality related to tooth loss in middle-aged adults? J. Public Health Dent. 2016, 76, 65–75. [Google Scholar] [CrossRef]
- Chalub, L.L.; Martins, C.C.; Ferreira, R.C.; Vargas, A.M. Functional Dentition in Brazilian Adults: An Investigation of Social Determinants of Health (SDH) Using a Multilevel Approach. PLoS ONE 2016, 11, e0148859. [Google Scholar] [CrossRef] [PubMed]
- Naorungroj, S.; Slade, G.D.; Divaris, K.; Heiss, G.; Offenbacher, S.; Beck, J.D. Racial differences in periodontal disease and 10-year self-reported tooth loss among late middle-aged and older adults: The dental ARIC study. J. Public Health Dent. 2017, 77, 372–382. [Google Scholar] [CrossRef]
- Kim, H.N.; Ha, T.G.; Kim, M.J.; Jun, E.J.; Jeong, S.H.; Kim, J.B. Factors related to number of present teeth in Korean elderly adults aged 55-84 years. Int. J. Dent. Hyg. 2016, 14, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Fantin, R.; Delpierre, C.; Kelly-Irving, M.; Barboza Solís, C. Early socioeconomic conditions and severe tooth loss in middle-aged Costa Ricans. Community Dent. Oral Epidemiol. 2018, 46, 178–184. [Google Scholar] [CrossRef]
- Suzuki, S.; Yoshino, K.; Takayanagi, A.; Ishizuka, Y.; Satou, R.; Kamijo, H.; Sugihara, N. Comparison of risk factors for tooth loss between professional drivers and white-collar workers: An internet survey. Ind. Health 2016, 54, 246–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, Y.; Tsuboya, T.; Watt, R.G.; Aida, J.; Osaka, K. Temporary employment and tooth loss: A cross-sectional study from the J-SHINE study. BMC Oral Health 2018, 18, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, E.M.; Azevedo, J.A.P.; Martins, R.F.M.; Alves, C.M.C.; Ribeiro, C.C.C.; Thomaz, E.B.A.F. Anemia and Dental Caries in Pregnant Women: A Prospective Cohort Study. Biol Trace Elem Res. 2017, 177, 241–250. [Google Scholar] [CrossRef]
- Umer, A.; Haile, Z.T.; Ahmadi-Montecalvo, H.; Chertok, I.R. Factors Associated with Receipt of Pre-pregnancy Preventive Dental Care Among Women in West Virginia: Pregnancy Risk Assessment Monitoring System (PRAMS) Survey 2009–2010. Oral Health Prev. Dent. 2016, 14, 413–422. [Google Scholar] [PubMed]
- Rio, R.; Sampaio-Maia, B.; Pereira, M.L.; Silva, M.J.; Azevedo, Á. Pregnancy as a Period of Enhanced Risk for Non-Cavitated Caries Lesions. Oral Health Prev. Dent. 2020, 18, 387–393. [Google Scholar]
- Martínez-Beneyto, Y.; Montero-Martin, J.; Garcia-Navas, F.; Vicente-Hernandez, A.; Ortiz-Ruiz, A.J.; Camacho-Alonso, F. Influence of a preventive program on the oral health-related quality of life (OHRQoL) of European pregnant women: A cohort study. Odontology 2019, 107, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Kateeb, E.; Momany, E. Dental caries experience and associated risk indicators among Palestinian pregnant women in the Jerusalem area: A cross-sectional study. BMC Oral Health 2018, 18, 170. [Google Scholar] [CrossRef]
- Calvasina, P.; Lawrence, H.P.; Hoffman-Goetz, L.; Norman, C.D. Brazilian immigrants’ oral health literacy and participation in oral health care in Canada. BMC Oral Health 2016, 16, 18. [Google Scholar] [CrossRef] [Green Version]
- Xhihani, B.; Rainchuso, L.; Smallidge, D.; Dominick, C. Oral Health Beliefs, Attitudes, and Practices of Albanian Immigrants in the United States. J. Community Health 2017, 42, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Rota, K.; Spanbauer, C.; Szabo, A.; Okunseri, C.E. Oral Health Practices, Beliefs and Dental Service Utilization of Albanian Immigrants in Milwaukee, Wisconsin: A Pilot Study. J.Immigr. Minor. Health 2019, 21, 315–323. [Google Scholar] [CrossRef] [Green Version]
- Elkerdany, A.; Gurenlian, J.; Freudenthal, J. Measuring Oral Health Literacy of Refugees: Associations with Dental Care Utilization and Oral Health Self-Efficacy. J. Dent. Hyg. 2020, 94, 9–17. [Google Scholar]
- Chahar, P.; Mohanty, V.R.; Aswini, Y.B. Oral health-related quality of life among elderly patients visiting special clinics in public hospitals in Delhi, India: A cross-sectional study. Indian J. Public Health 2019, 63, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Chae, S.; Lee, Y.; Kim, J.; Chun, K.H.; Lee, J.K. Factors associated with perceived unmet dental care needs of older adults. Geriatr. Gerontol. Int. 2017, 17, 1936–1942. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.S.; Yi, Y.J.; Donnelly, L.R. Oral health of older residents in care and community dwellers: Nursing implications. Int. Nurs. Rev. 2017, 64, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Blasi, P.R.; Krakauer, C.; Anderson, M.L.; Nelson, J.; Bush, T.; Catz, S.L.; McClure, J.B. Factors associated with future dental care utilization among low-income smokers overdue for dental visits. BMC Oral Health 2018, 18, 183. [Google Scholar] [CrossRef]
- Berglund, E.; Westerling, R.; Lytsy, P. Social and health-related factors associated with refraining from seeking dental care: A cross-sectional population study. Community Dent. Oral Epidemiol. 2017, 45, 258–265. [Google Scholar] [CrossRef]
- Piotrowska, D.E.; Jankowska, D.; Huzarska, D.; Szpak, A.S.; Pędziński, B. Socioeconomic inequalities in use and non-use of dental services in Poland. Int. J. Public Health 2020, 65, 637–647. [Google Scholar] [CrossRef]
- Akintobi, T.H.; Hoffman, L.M.; McAllister, C.; Goodin, L.; Hernandez, N.D.; Rollins, L.; Miller, A. Assessing the Oral Health Needs of African American Men in Low-Income, Urban Communities. Am. J. Mens. Health 2018, 12, 326–337. [Google Scholar] [CrossRef]
- Kailembo, A.; Preet, R.; Stewart Williams, J. Socioeconomic inequality in self-reported unmet need for oral health services in adults aged 50 years and over in China, Ghana, and India. Int. J. Equity Health 2018, 17, 99. [Google Scholar] [CrossRef]
- Srivastava, P.; Chen, G.; Harris, A. Oral Health, Dental Insurance and Dental Service use in Australia. Health Econ. 2017, 26, 35–53. [Google Scholar] [CrossRef]
- Teusner, D.N.; Brennan, D.S.; Spencer, A.J. Associations between level of private dental insurance cover and favourable dental visiting by household income. Aust. Dent. J. 2015, 60, 479–489. [Google Scholar] [CrossRef]
- Rampa, S.; Wilson, F.A.; Allareddy, V. Trends in dental-related emergency department visits in the State of California from 2005 to 2011. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, C.; Manso, A.C.; Escoval, A.; Salvado, F.; Nunes, C. Self-perception of oral health in older adults from an urban population in Lisbon, Portugal. Rev. Saude Publica 2016, 50, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalcanti, Y.W.; de Almeida, L.F.D.; de Lucena, E.H.G.; Probst, L.F.; Cavalcante, D.F.B.; Frias, A.C.; Bulgareli, J.V.; Pereira, A.C. Factors that influence the oral impact on daily performance of older people in Brazil: A cross-sectional population-based study. Gerodontology 2020, 37, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.J.F.; Lins, C.A.A.; Macedo, L.P.V.; Sousa, V.P.S.; Duque, J.A.; Souza, M.C. Clinical and self-perceived oral health assessment of elderly residents in urban, rural, and institutionalized communities. Clinics 2019, 74, e972. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Abrahamsson, I.; Wide, U.; Hakeberg, M. Periodontal disease among older people and its impact on oral health-related quality of life. Gerodontology 2018, 35, 382–390. [Google Scholar] [CrossRef]
- Zusman, S.P.; Kushnir, D.; Natapov, L.; Goldsmith, R.; Dichtiar, R. Oral Health-Related Quality of Life in the Elderly in Israel--Results from the National Health and Nutrition Survey of the Elderly 2005–2006. Oral Health Prev. Dent. 2016, 14, 117–123. [Google Scholar] [PubMed]
- Abu-Awwad, M.; Al-Omoush, S.; Shqaidef, A.; Hilal, N.; Hassona, Y. Oral health-related quality of life among Syrian refugees in Jordan: A cross-sectional study. Int. Dent. J. 2020, 70, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Freiberg, A.; Wienke, A.; Bauer, L.; Niedermaier, A.; Führer, A. Dental Care for Asylum-Seekers in Germany: A Retrospective Hospital-Based Study. Int. J. Environ. Res. Public Health 2020, 17, 2672. [Google Scholar] [CrossRef]
- Grover, V.; Malhotra, R.; Dhawan, S.; Kaur, G. Comparative Assessment of Oral Health Related Quality of Life in Chronic Periodontitis Patients of Rural and Urban Populations in Punjab. Oral Health Prev. Dent. 2016, 14, 235–240. [Google Scholar]
- Zhang, J.; Sardana, D.; Wong, M.C.M.; Leung, K.C.M.; Lo, E.C.M. Factors Associated with Dental Root Caries: A Systematic Review. JDR Clin. Trans. Res. 2020, 5, 13–29. [Google Scholar] [CrossRef]
- Lee, D.R.; Santo, E.C.; Lo, J.C.; Ritterman Weintraub, M.L.; Patton, M.; Gordon, N.P. Understanding functional and social risk characteristics of frail older adults: A cross-sectional survey study. BMC Fam. Pract. 2018, 19, 170. [Google Scholar] [CrossRef] [Green Version]
- Niesten, D.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H.J. Oral health care behavior and frailty-related factors in a care-dependent older population. J. Dent. 2017, 61, 39–47. [Google Scholar] [CrossRef]
- Chen, M.Y. Misperception of Oral Health among Adults in Rural Areas: A Fundamental but Neglected Issue in Primary Healthcare. Int. J. Environ. Res. Public Health 2018, 15, 2187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mejia, G.C.; Elani, H.W.; Harper, S.; Murray Thomson, W.; Ju, X.; Kawachi, I.; Kaufman, J.S.; Jamieson, L.M. Socioeconomic status, oral health and dental disease in Australia, Canada, New Zealand and the United States. BMC Oral Health 2018, 18, 176. [Google Scholar] [CrossRef] [PubMed]
- Capurro, D.A.; Davidsen, M. Socioeconomic inequalities in dental health among middle-aged adults and the role of behavioral and psychosocial factors: Evidence from the Spanish National Health Survey. Int. J. Equity Health 2017, 16, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hicks, T.A.; Wilson, S.M.; Thomas, S.P.; Dennis, P.A.; Neal, J.M.; Calhoun, P.S. Low Income as a Multiplicative Risk Factor for Oral Pain and Dental Problems Among, U.S. Veteran Smokers. Int. J. Behav. Med. 2018, 25, 67–73. [Google Scholar] [CrossRef]
- Bassim, C.W.; MacEntee, M.I.; Nazmul, S.; Bedard, C.; Liu, S.; Ma, J.; Griffith, L.E.; Raina, P. Self-reported oral health at baseline of the Canadian Longitudinal Study on Aging. Community Dent. Oral Epidemiol. 2020, 48, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Laniado, N.; Brow, A.R.; Tranby, E.; Badner, V.M. Trends in non-traumatic dental emergency department use in New York and New Jersey: A look at Medicaid expansion from both sides of the Hudson River. J. Public Health Dent. 2020, 80, 9–13. [Google Scholar] [CrossRef] [PubMed]
- DeLia, D.; Lloyd, K.; Feldman, C.A.; Cantor, J.C. Patterns of emergency department use for dental and oral health care: Implications for dental and medical care coordination. J. Public Health Dent. 2016, 76, 1–8. [Google Scholar] [CrossRef]
- Franciscatto, G.J.; Brennan, D.S.; Gomes, M.S.; Rossi-Fedele, G. Association between pulp and periapical conditions and dental emergency visits involving pain relief: Epidemiological profile and risk indicators in private practice in Australia. Int. Endod. J. 2020, 53, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Srisilapanan, P.; Korwanich, N.; Lalloo, R. Associations between social inequality and tooth loss in a household sample of elderly Thai people aged ≥60 years old. Gerodontology 2016, 33, 201–208. [Google Scholar] [CrossRef]
- Ramsay, S.E.; Papachristou, E.; Watt, R.G.; Lennon, L.T.; Papacosta, A.O.; Whincup, P.H.; Wannamethee, S.G. Socioeconomic disadvantage across the life-course and oral health in older age: Findings from a longitudinal study of older British men. J. Public Health 2018, 40, e423–e430. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Bernabé, E.; Liu, X.; Gallagher, J.E.; Zheng, S. Do contextual factors have a role in periodontal disease? J. Clin. Periodontol. 2017, 44, 13–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2017 Oral Disorders Collaborators; Bernabe, E.; Marcenes, W.; Hernandez, C.R.; Bailey, J.; Abreu, L.G.; Alipour, V.; Amini, S.; Arabloo, J.; Arefi, Z.; et al. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar]
- Cianetti, S.; Pagano, S.; Nardone, M.; Lombardo, G. Model for Taking Care of Patients with Early Childhood Caries during the SARS-CoV-2 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 3751. [Google Scholar] [CrossRef]
- Ostberg, A.L.; Andersson, P.; Hakeberg, M. Oral impacts on daily performances: Associations with self-reported general health and medication. Acta Odontol. Scand. 2009, 67, 370–376. [Google Scholar] [CrossRef]
- D’Addazio, G.; Santilli, M.; Sinjari, B.; Xhajanka, E.; Rexhepi, I.; Mangifesta, R.; Caputi, S. Access to Dental Care-A Survey from Dentists, People with Disabilities and Caregivers. Int. J. Environ. Res. Public Health 2021, 18, 1556. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.S. From focal sepsis to periodontal medicine: A century of exploring the role of the oral microbiome in systemic disease. J. Physiol. 2017, 595, 465–476. [Google Scholar] [CrossRef]
- Leira, Y.; Seoane, J.; Blanco, M.; Rodríguez-Yáñez, M.; Takkouche, B.; Blanco, J.; Castillo, J. Association between periodontitis and ischemic stroke: A systematic review and meta-analysis. Eur. J. Epidemiol. 2017, 32, 43–53. [Google Scholar] [CrossRef]
- Puertas, A.; Magan-Fernandez, A.; Blanc, V.; Revelles, L.; O’Valle, F.; Pozo, E.; León, R.; Mesa, F. Association of periodontitis with preterm birth and low birth weight: A comprehensive review. J. Matern. Fetal Neonatal. Med. 2018, 31, 597–602. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Alba, A.L.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spanemberg, J.C.; Cardoso, J.A.; Slob, E.M.G.B.; López-López, J. Quality of life related to oral health and its impact in adults. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cianetti, S.; Valenti, C.; Orso, M.; Lomurno, G.; Nardone, M.; Lomurno, A.P.; Pagano, S.; Lombardo, G. Systematic Review of the Literature on Dental Caries and Periodontal Disease in Socio-Economically Disadvantaged Individuals. Int. J. Environ. Res. Public Health 2021, 18, 12360. https://doi.org/10.3390/ijerph182312360
Cianetti S, Valenti C, Orso M, Lomurno G, Nardone M, Lomurno AP, Pagano S, Lombardo G. Systematic Review of the Literature on Dental Caries and Periodontal Disease in Socio-Economically Disadvantaged Individuals. International Journal of Environmental Research and Public Health. 2021; 18(23):12360. https://doi.org/10.3390/ijerph182312360
Chicago/Turabian StyleCianetti, Stefano, Chiara Valenti, Massimiliano Orso, Giuseppe Lomurno, Michele Nardone, Anna Palma Lomurno, Stefano Pagano, and Guido Lombardo. 2021. "Systematic Review of the Literature on Dental Caries and Periodontal Disease in Socio-Economically Disadvantaged Individuals" International Journal of Environmental Research and Public Health 18, no. 23: 12360. https://doi.org/10.3390/ijerph182312360