
Intersections of Sex Work, Mental Ill-Health, IPV and Other Violence Experienced by Female Sex Workers: Findings from a Cross-Sectional Community-Centric National Study in South Africa

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Measures
2.3. Data Analysis
2.4. Ethics Approval
3. Results
3.1. Participant Demographic Characteristics
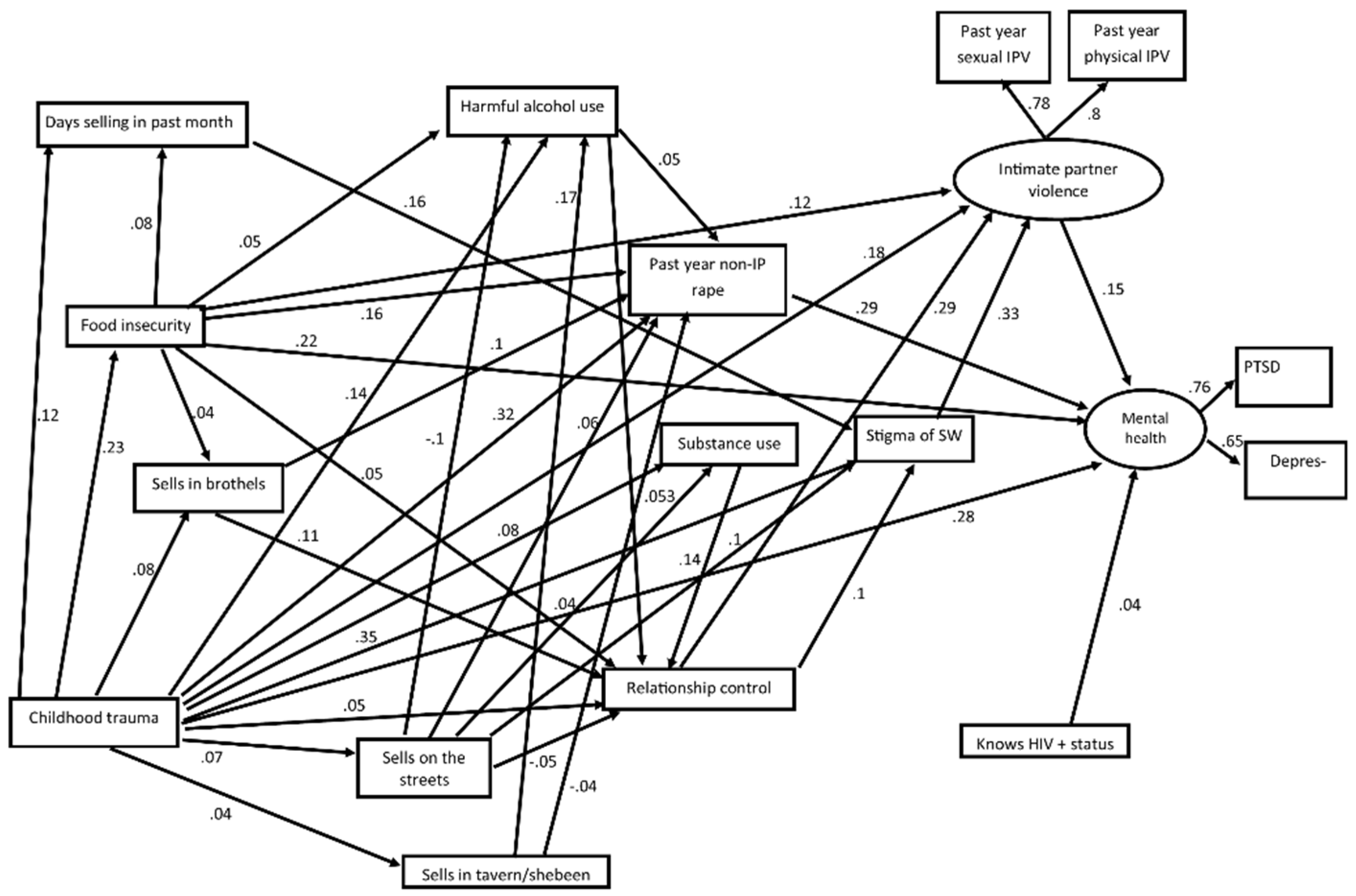
3.2. Structural Equation Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cuadros, D.F.; Tomita, A.; Vandormael, A.; Slotow, R.; Burns, J.K.; Tanser, F. Spatial structure of depression in South Africa: A longitudinal panel survey of a nationally representative sample of households. Sci. Rep. 2019, 9, 979. [Google Scholar] [CrossRef] [PubMed]
- Coetzee, J.; Gray, G.E.; Jewkes, R. Prevalence and patterns of victimization and polyvictimization among female sex workers in Soweto, a South African township: A cross-sectional, respondent-driven sampling study. Glob. Health Action 2017, 10, 1403815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gould, C.; Fick, N. Selling Sex in Cape Town: Sex Work and Human Trafficking in a South African City; Institute for Security Studies: Pretoria/Tshwane, South Africa, 2008. [Google Scholar]
- Platt, L.; Grenfell, P.; Meiksin, R.; Elmes, J.; Sherman, S.G.; Sanders, T.; Mwangi, P.; Crago, A.L. Associations between sex work laws and sex workers’ health: A systematic review and meta-analysis of quantitative and qualitative studies. PLoS Med. 2018, 15, e1002680. [Google Scholar] [CrossRef] [PubMed]
- Coetzee, J.; Buckley, J.; Otwombe, K.; Milovanovic, M.; Gray, G.E.; Jewkes, R. Depression and Post Traumatic Stress amongst female sex workers in Soweto, South Africa: A cross sectional, respondent driven sample. PLoS ONE 2018, 13, e0196759. [Google Scholar] [CrossRef]
- Poliah, V.; Paruk, S. Depression, anxiety symptoms and substance use amongst sex workers attending a non-governmental organisation in KwaZulu-Natal, South Africa. S. Afr. Fam. Pract. 2017, 59, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Machisa, M.T.; Christofides, N.; Jewkes, R. Mental ill health in structural pathways to women’s experiences of intimate partner violence. PLoS ONE 2017, 12, e0175240. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.K.; Saggurti, N.; Pachauri, S.; Prabhakar, P. Correlates of Mental Depression Among Female Sex Workers in Southern India. Asia Pac. J. Public Health 2015, 27, 809–819. [Google Scholar] [CrossRef]
- Sagtani, R.A.; Bhattarai, S.; Adhikari, B.R.; Baral, D.; Yadav, D.K.; Pokharel, P.K. Violence, HIV risk behaviour and depression among female sex workers of eastern Nepal. BMJ Open 2013, 3, e002763. [Google Scholar] [CrossRef] [Green Version]
- Chudakov, B.; Ilan, K.; Belmaker, R.H.; Cwikel, J. The Motivation and Mental Health of Sex Workers. J. Sex Marital. Ther. 2002, 28, 305–315. [Google Scholar] [CrossRef]
- Roxburgh, A.; Degenhardt, L.; Copeland, J. Posttraumatic stress disorder among female street-based sex workers in the greater Sydney area, Australia. BMC Psychiatry 2006, 6, 24. [Google Scholar] [CrossRef] [Green Version]
- Willis, B. The global public health burden of sex work: A call for research. Lancet Glob. Health 2013, 1, e68. [Google Scholar] [CrossRef] [Green Version]
- James, J.; Meyerding, J. Early sexual experience and prostitution. Am. J. Psychiatry 1977, 134, 1381–1385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tschoeke, S.; Borbé, R.; Steinert, T.; Bichescu-Burian, D. A Systematic Review of Dissociation in Female Sex Workers. J. Trauma Dissociation 2019, 20, 242–257. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Lau, J.; Li, M.; Li, H.; Gao, Q.; Feng, X.; Bai, Y.; Hao, C.; Hao, Y. Socio-ecological factors associated with depression, suicidal ideation and suicidal attempt among female injection drug users who are sex workers in China. Drug Alcohol Depend. 2014, 144, 102–110. [Google Scholar] [CrossRef] [Green Version]
- Deering, K.N.; Amin, A.; Shoveller, J.; Nesbitt, A.; Garcia-Moreno, C.; Duff, P.; Argento, A.; Shannon, K. A systematic review of the correlates of violence against sex workers. Am. J. Public Health 2014, 104, e42–e54. [Google Scholar] [CrossRef] [PubMed]
- Wechsberg, W.M.; Zule, W.A.; Luseno, W.K.; Kline, T.L.; Browne, F.A.; Novak, S.P.; Ellerson, R.M. Effectiveness of an Adapted Evidence-Based Woman-Focused Intervention for Sex Workers and Non-Sex Workers: The Women’s Health CoOp in South Africa. J. Drug Issues 2011, 41, 233–252. [Google Scholar] [CrossRef]
- Maher, L.; Mooney-Somers, J.; Phlong, P.; Couture, M.C.; Stein, E.; Evans, J.; Cockroft, M.; Sansothy, N.; Nemoto, T.; Page, K.; et al. Selling sex in unsafe spaces: Sex work risk environments in Phnom Penh, Cambodia. Harm Reduct. J. 2011, 8, 30. [Google Scholar] [CrossRef] [Green Version]
- Jewkes, R.; Fulu, E.; Naved, R.T.; Chirwa, E.; Dunkle, K.; Haardörfer, R.; Garcia-Moreno, C. Women’s and men’s reports of past-year prevalence of intimate partner violence and rape and women’s risk factors for intimate partner violence: A multicountry cross-sectional study in Asia and the Pacific. PLoS Med. 2017, 14, e1002381. [Google Scholar] [CrossRef] [Green Version]
- Farley, M.; Barkan, H. Prostitution, Violence Against Women, and Posttraumatic Stress Disorder. Women Health 1998, 27, 37–49. [Google Scholar] [CrossRef]
- Beattie, T.S.; Bhattacharjee, P.; Ramesh, B.M.; Gurnani, V.; Anthony, J.; Isac, S.; Mohan, H.; Ramakrishnan, A.; Wheeler, T.; Bradley, J.; et al. Violence against female sex workers in Karnataka State, South India: Impact on health, and reductions in violence following an intervention program. BMC Public Health 2010, 10, e1–e11. [Google Scholar] [CrossRef] [Green Version]
- Trevillion, K.; Oram, S.; Feder, G.; Howard, L.M. Experiences of domestic violence and mental disorders: A systematic review and meta-analysis. PLoS ONE 2012, 7, e51740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scorgie, F.; Nakato, D.; Akoth, D.O.; Netchivhambe, M.; Chakuvinga, P.; Nkomo, P.; Abdalla, P.; Sibanda, S.; Richter, M. “I Expect to Be Abused and I Have Fear”: Sex Workers’ Experiences of Human Rights Violations and Barriers to Accessing Healthcare in Four African Countries. Available online: https://www.eldis.org/document/A59250 (accessed on 10 November 2020).
- Richter, M. Erotic Labour in Hillbrow: Sex Work, Johannesburg’s ‘Den of Iniquity’ and HIV/AIDS. Available online: http://www.hst.org.za/uploads/files/richter_paper.pdf. (accessed on 10 November 2020).
- Beattie, T.S.; Smilenova, B.; Krishnaratne, S.; Mazzuca, A. Mental health problems among female sex workers in low- and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2020, 17, e1003297. [Google Scholar] [CrossRef]
- McKay, M.T.; Cannon, M.; Chambers, D.; Conroy, R.M.; Coughlan, H.; Dodd, P.; Healy, C.; O’Donnell, L.; Clarke, M.C. Childhood trauma and adult mental disorder: A systematic review and meta-analysis of longitudinal cohort studies. Acta Psychiatr. Scand. 2021, 143, 189–205. [Google Scholar] [CrossRef] [PubMed]
- Trudell, J.P.; Burnet, M.L.; Ziegler, B.R.; Luginaah, I. The impact of food insecurity on mental health in Africa: A systematic review. Soc. Sci. Med. 2021, 278, 113953. [Google Scholar] [CrossRef]
- Gibbs, A.; Jewkes, R.; Willan, S.; Washington, L. Associations between poverty, mental health and substance use, gender power, and intimate partner violence amongst young (18–30) women and men in urban informal settlements in South Africa: A cross-sectional study and structural equation model. PLoS ONE 2018, 13, e0204956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. WHO Multicountry Study on Women’s Health and Domestric Violence: Core Questionnaire and WHO Instrument; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Bernstein, D.P.; Fink, L.; Handelsman, L.; Foote, J.; Lovejoy, M.; Wenzel, K.; Sapareto, E.; Ruggiero, J. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am. J. Psychiatry 1994, 151, 1132–1136. [Google Scholar] [CrossRef]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; De La Fuente, J.R.; Grant, M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption-II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L. The CES-D Scale: A self report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Hansen, M.; Andersen, T.E.; Armour, C.; Elklit, A.; Palic, S.; Mackrill, T. PTSD-8: A Short PTSD Inventory. Clin. Pr. Epidemiol. Ment. Health 2010, 6, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Pulerwitz, J.; Gortmaker, S.L.; DeJong, W. Measuring Sexual Relationship Power in HIV/STD Research. Sex Roles 2000, 42, 637–660. [Google Scholar] [CrossRef]
- Dunkle, K.L.; Jewkes, R.; Brown, H.C.; Gray, G.E.; McIntryre, J.A.; Harlow, S.D. Gender-based violence, relationship power, and risk of HIV infection in women attending antenatal clinics in South Africa. Lancet 2004, 363, 1415–1421. [Google Scholar] [CrossRef]
- Ncitakalo, N.; Mabaso, M.; Joska, J.; Simbayi, L. Factors associated with external HIV-related stigma and psychological distress among people living with HIV in South Africa. SSM Popul. Health. 2021, 14, 100809. [Google Scholar] [CrossRef] [PubMed]
- Enders, C.K.; Bandalos, D.L. The Relative Performance of Full Information Maximum Likelihood Estimation for Missing Data in Structural Equation Models. Struct. Equ. Model. A Multidiscip. J. 2001, 8, 430–457. [Google Scholar] [CrossRef]
- Tucker, L.R.; Lewis, C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika 1973, 38, 1–10. [Google Scholar] [CrossRef]
- Steiger, J. Structural model equation and modification: An interval estimation approach. Multivar. Behav. Res. 1990, 25, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Ruan, M.; Chen, J.; Fang, Y. Major Depressive Disorder: Advances in Neuroscience Research and Translational Applications. Neurosci. Bull. 2021, 37, 863–880. [Google Scholar] [CrossRef]
- Doroszkiewicz, C.; Gold, D.; Green, R.; Tartaglia, M.C.; Ma, J.; Tator, C.H. Anxiety, Depression, and Quality of Life: A Long-Term Follow-Up Study of Patients with Persisting Concussion Symptoms. J. Neurotrauma 2021, 38, 493–505. [Google Scholar] [CrossRef] [PubMed]
- National Department of Health (NDoH); Statistics South Africa (Stats SA); Research SAM; Council (SAMRC); ICF. South Africa Demographic and Health Survey 2016; NDOH: Pretoria, South Africa; Rockville, MD, USA, 2019.
- Jewkes, R.; Morrell, R.; Sikweyiya, Y.; Dunkle, K.; Penn-Kekana, L. Men, sex and the provider role: Crime, violence, correlated psychological attributes associated with South African men’s engagement in prostitution and transactional sex in South Africa. PLoS ONE 2012, 7, e40821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satyanarayana, V.A.; Chandra, P.S.; Vaddiparti, K. Mental health consequences of violence against women and girls. Curr. Opin. Psychiatry 2015, 28, 350–356. [Google Scholar] [CrossRef]
- Gibbs, A.; Dunkle, K.; Ramsoomar, L.; Willan, S.; Jama Shai, N.; Chatterji, S.; Naved, R.; Jewkes, R. New learnings on drivers of men’s physical and/or sexual violence against their female partners, and women’s experiences of this, and the implications for prevention interventions. Glob. Health Action 2020, 13, 1739845. [Google Scholar] [CrossRef] [Green Version]
- Campbell, C. Selling sex in the time of AIDS: The psycho-social context of condom use by southern Africa sex workers. Soc. Sci Med. 2000, 50, 479–494. [Google Scholar] [CrossRef] [Green Version]
- Wojcicki, J. Commercial sex work or ukuphanda? Sex-for-money exchange in Soweto and Hammanskrall area, South Africa. Cult. Med. Psychiatry 2002, 26, 339–370. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. INSPIRE: Seven Strategies for Ending Violence Against Children; World Health Organisation: Geneva, Switzerland, 2016. [Google Scholar]
- Wechsberg, W.M.; Luseno, W.K.; Lam, W.K.; Parry, C.D.H.; Morojele, N. Substance use, sexual risk, and violence: Findings from an HIV prevention pilot intervention with sex workers in Pretoria. AIDS Behav. 2006, 10, 131–137. [Google Scholar] [CrossRef]
- Wechsberg, W.M.; Bonner, C.P.; Zule, W.A.; van der Horst, C.; Ndirangu, J.; Browne, F.A.; Kline, T.L.; Howard, B.N.; Rodman, N.F. Addressing the nexus of risk: Biobehavioral outcomes from a cluster randomized trial of the Women’s Health CoOp Plus in Pretoria, South Africa. Drug Alcohol Depend. 2019, 195, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Minnis, A.M.; Doherty, I.A.; Kline, T.L.; Zule, W.A.; Myers, B.; Carney, T.; Wechsberg, W.M. Relationship power, communication, and violence among couples: Results of a cluster-randomized HIV prevention study in a South African township. Int. J. Women’s Health 2015, 7, 517–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandyopadhyay, K.; Banerjee, S.; Goswami, D.N.; Dasgupta, A.; Jana, S. Predictors of Inconsistent Condom Use among Female Sex Workers: A Community-Based Study in a Red-Light Area of Kolkata, India. Indian J. Community Med. 2018, 43, 274–278. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| VARIABLE NAME | ALPHA | MEASURE | DETAILS |
|---|---|---|---|
| Sexual IPV and non-partner rape (asked separately for partner, police, clients (paying partners), other men) | WHO violence against women [29], adapted for non-partner violence against FSWs [2] | Three items asking about being physically forced to have sex when she did not want to or agreeing to sex when she did not want to because she was threatened or afraid of what he might do, or otherwise being forced to have sex. | |
| Physical violence by intimate partner | WHO violence against women [29], adapted for non-partner violence against FSWs [2] | Five items asking about: slapped, pushed, something thrown; hit with a fist or other object; kicked, dragged, beaten, choked or burnt; threaten to use or used a gun, knife or other weapon; feeling she may or would be killed. | |
| Food security | 0.90 | Three items | Asking about having no food, sleeping hungry and going a whole day and night without eating. |
| Childhood Experiences | 0.81 | Childhood Trauma Questionnaire (short version) (CTQ) [30] | Five dimensions: neglect (physical and emotional) and abuse (emotional, physical and sexual); 12 items. |
| Alcohol and Drug Use | 0.91 | Alcohol Use Disorder Identification Test (AUDIT) C version [31]. Self-report drug use. | Measures binge drinking with volumes adjusted for the population. Drug use asked about locally relevant drugs and measure dichotomised. |
| Depression | 0.90 | CES-D 20 item scale [32] | CES-D scores over 20 were considered to indicate depression (i.e., a 20/21 cut point). Otherwise used as a score. |
| Post-Traumatic Stress Disorder | 0.92 | A short inventory (PTSD-8) [33], based upon the Harvard Trauma Questionnaire | Eight items directly linked to the DSM-IV PTSD criteria with 4-point Likert scale. A score ≥ 3 for each of the three sub-scales (intrusion, avoidance or hypervigilance) indicated PTSD. In the SEM it is used as a continuous variable. |
| Relationship control scale | 0.83 | Locally developed from the South African adaptation of the SRPS [34,35] | Six items designed with the community for use among FSWs. Typical item: my partner worries when I dress up that I am going to sell sex. Items summed. |
| Sex work stigma | 0.74 | Adapted for sex work from the People Living with HIV stigma index [36]. | Five measures on a 4-point Likert scale asked about verbal, physical and sexual violence and stigma from health care workers and police. A typical question was: how often within the past year have you experienced sexual abuse because you are a sex worker. Items were summed. |
| Depression | PTSD | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Overall (n = 3005) | Yes (n = 1584) | No (n = 1421) | p-Value | Yes (n = 1611) | No (n = 1388) | p-Value |
| n, Age Mean (STD) | 3005, 33.3 (7.95) | 1584, 33.7 (7.98) | 1421, 32.7 (7.88) | 0.004 | 1611, 33.3 (7.84) | 1388, 33.2 (8.06) | 0.850 |
| Education level | |||||||
| Matric or higher (%) | 668 (22.3) | 364 (23.0) | 304 (21.4) | 0.336 | 357 (22.2) | 311 (22.4) | 0.933 |
| Incomplete schooling (%) | 2334 (77.8) | 1219 (77.0) | 1115 (78.6) | 1252 (77.8) | 1077 (77.6) | ||
| n, Childhood trauma MEAN (STD) (range 0–36) | 3002, 20.0 (5.79) | 1584, 21.6 (5.92) | 1418,18.3 (5.09) | <0.0001 | 1611, 21.5 (5.76) | 1388, 18.4 (5.38) | <0.0001 |
| Food insecurity | |||||||
| No (%) | 1643 (54.8) | 681 (43.1) | 962 (67.9) | <0.0001 | 742 (46.2) | 897 (64.7) | <0.0001 |
| Yes (%) | 1355 (45.2) | 901 (57.0) | 454 (32.1) | 864 (53.8) | 490 (35.3) | ||
| Work Circumstances | |||||||
| Sells sex on the streets/outdoor location | |||||||
| No (%) | 1064 (35.4) | 558 (35.2) | 506 (35.6) | 0.827 | 590 (36.6) | 471 (33.9) | 0.124 |
| Yes (%) | 1941 (64.6) | 1026 (64.8) | 915 (64.4) | 1021 (63.4) | 917 (66.1) | ||
| Normally sells in a taverns/Shebeens | |||||||
| No (%) | 1914 (63.7) | 975 (61.6) | 939 (66.1) | 0.123 | 994 (61.7) | 914 (65.9) | 0.108 |
| Yes (%) | 1091 (36.3) | 609 (38.5) | 482 (33.9) | 617 (38.3) | 474 (34.2) | ||
| Normally sells in a brothel | |||||||
| No (%) | 2611 (86.9) | 1350 (85.2) | 1261 (88.7) | 0.085 | 1352 (83.9) | 1254 (90.4) | <0.0001 |
| Yes (%) | 394 (13.1) | 234 (14.8) | 160 (11.5) | 259 (16.1) | 134 (9.7) | ||
| n, Days selling in past month MEAN (STD) | 2988, 19.1 (7.88) | 1578, 20.1 (8.00) | 1410, 18.1 (7.61) | <0.0001 | 1606, 20.1 (7.82) | 1382, 18.1 (7.82) | <0.0001 |
| Harmful alcohol drinking and substance use | |||||||
| Uses substances to enable sex work | |||||||
| No (%) | 2393 (79.9) | 1198 (75.8) | 1195 (84.5) | <0.0001 | 1224 (76.1) | 1168 (84.2) | <0.0001 |
| Yes (%) | 603 (20.1) | 383 (24.2) | 220 (15.6) | 384 (23.9) | 219 (15.8) | ||
| n, Harmful alcohol use score MEAN (STD) | 2995, 6.32 (0.20) | 1583, 6.75 (0.21) | 1412, 5.84 (0.23) | <0.0001 | 1611, 6.89 (0.20) | 1384, 5.66 (0.22) | <0.0001 |
| Suidal thoughts and stigma | |||||||
| Suicidal thoughts in the past month | |||||||
| No (%) | 2114 (70.5) | 966 (61.0) | 1148 (81.3) | <0.0001 | 987 (61.3) | 1127 (81.2) | <0.0001 |
| Yes (%) | 883 (29.5) | 618 (39.0) | 265 (18.8) | 622 (38.7) | 261 (18.8) | ||
| n, SW-related stigma MEAN (STD) | 3000, 18.3 (5.45) | 1584, 19.5 (5.69) | 1416, 17.0 (4.83) | <0.0001 | 1611, 19.1 (5.74) | 1388, 17.4 (4.95) | <0.0001 |
| Partner controlling behaviour | |||||||
| n, Relationship control MEAN (STD) (higher =more controlling) | 3002, 7.8 (0.16) | 1584, 8.3 (0.23) | 1418, 7.5 (0.16) | 0.015 | 1611, 8.2 (0.23) | 1388, 7.6 (0.16) | 0.077 |
| Gender-based violence | |||||||
| Past year non-intimate partner rape | |||||||
| None (%) | 1317 (44.0) | 508 (32.1) | 809 (57.4) | <0.0001 | 466 (29.0) | 850 (61.5) | <0.0001 |
| Some (%) | 1676 (56.0) | 1075 (67.9) | 601 (42.6) | 1143 (71.0) | 533 (38.5) | ||
| Intimate partner sexual violence in the past year | |||||||
| None (%) | 2060 (68.7) | 996 (62.9) | 1064 (75.1) | <0.0001 | 966 (60.0) | 1093 (78.8) | <0.0001 |
| Some (%) | 940 (31.3) | 588 (37.1) | 352 (24.9) | 645 (40.0) | 294 (21.2) | ||
| Intimate partner physical violence in the past year | |||||||
| None (%) | 1870 (62.4) | 882 (55.8) | 988 (69.8) | <0.0001 | 885 (55.1) | 983 (70.9) | <0.0001 |
| Some (%) | 1127 (37.6) | 700 (44.3) | 427 (30.2) | 722 (44.9) | 404 (29.1) | ||
| HIV | |||||||
| Knows HIV+ status | |||||||
| No (%) | 1236 (43.0) | 625 (40.8) | 611 (45.5) | 0.094 | 680 (43.4) | 556 (42.5) | 0.735 |
| Yes (%) | 1638 (57.0) | 907 (59.2) | 731 (54.5) | 887 (56.6) | 751 (57.5) | ||
| Direct Effects | Indirect Effects | Total Effects | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Path | Standardized Coef | LCL | UCL | p-Value | Standardized Coef | LCL | UCL | p-Value | Standardized Coef | LCL | UCL | p-Value |
| Childhood trauma ->food insecurity | 0.227 | 0.191 | 0.264 | <0.001 | 0.227 | 0.191 | 0.264 | <0.001 | ||||
| Childhood trauma ->harmful alcohol use | 0.139 | 0.103 | 0.176 | <0.001 | 0.01 | −0.002 | 0.021 | 0.098 | 0.149 | 0.113 | 0.185 | <0.001 |
| Food insecurity ->harmful alcohol use | 0.046 | 0.008 | 0.083 | 0.016 | 0.046 | 0.008 | 0.083 | 0.016 | ||||
| Sells on the street ->harmful alcohol use | −0.096 | −0.131 | −0.061 | <0.001 | −0.096 | −0.131 | −0.061 | <0.001 | ||||
| Sells in taverns -> harmful alcohol use | 0.167 | 0.132 | 0.202 | <0.001 | 0.167 | 0.132 | 0.202 | <0.001 | ||||
| Food insecurity ->past year non-partner rape | 0.155 | 0.12 | 0.191 | <0.001 | 0.006 | 0.002 | 0.01 | 0.006 | 0.161 | 0.126 | 0.197 | <0.001 |
| Harmful alcohol use ->past year non-partner rape | 0.045 | 0.011 | 0.08 | 0.011 | 0.045 | 0.011 | 0.08 | 0.011 | ||||
| Sells in brothels ->past year non-partner rape | 0.100 | 0.069 | 0.131 | <0.001 | 0.100 | 0.069 | 0.131 | <0.001 | ||||
| Sells on the street ->past year non-partner rape | 0.063 | 0.03 | 0.097 | <0.001 | −0.004 | −0.008 | −0.001 | 0.02 | 0.059 | 0.025 | 0.093 | 0.001 |
| Sells in taverns->past year non-partner rape | −0.035 | −0.069 | −0.002 | 0.039 | 0.008 | 0.002 | 0.014 | 0.013 | −0.028 | −0.061 | 0.005 | 0.099 |
| Childhood trauma ->past year non-partner rape | 0.316 | 0.279 | 0.353 | <0.001 | 0.054 | 0.042 | 0.066 | <0.001 | 0.37 | 0.334 | 0.406 | <0.001 |
| Food insecurity ->sells in a brothel | 0.04 | 0.006 | 0.073 | 0.022 | 0.04 | 0.006 | 0.073 | 0.022 | ||||
| Childhood trauma ->sells in a brothel | 0.077 | 0.041 | 0.113 | <0.001 | 0.009 | 0.001 | 0.017 | 0.024 | 0.086 | 0.051 | 0.121 | <0.001 |
| Food insecurity ->days selling in past month | 0.083 | 0.046 | 0.12 | <0.001 | 0.083 | 0.046 | 0.12 | <0.001 | ||||
| Childhood trauma->days selling in past month | 0.121 | 0.08 | 0.162 | <0.001 | 0.019 | 0.01 | 0.028 | <0.001 | 0.14 | 0.099 | 0.18 | <0.001 |
| Food insecurity->relationship control | 0.048 | 0.011 | 0.085 | 0.011 | 0.006 | 0.002 | 0.011 | 0.009 | 0.054 | 0.017 | 0.091 | 0.004 |
| Harmful alcohol use->relationship control | 0.042 | 0.007 | 0.077 | 0.019 | 0.042 | 0.007 | 0.077 | 0.019 | ||||
| Sells in a brothel->relationship control | 0.108 | 0.071 | 0.144 | <0.001 | 0.108 | 0.071 | 0.144 | <0.001 | ||||
| Substance use->relationship control | 0.142 | 0.105 | 0.179 | <0.001 | 0.142 | 0.105 | 0.179 | <0.001 | ||||
| Sells on the streets->relationship control | −0.048 | −0.083 | −0.013 | 0.007 | 0.002 | −0.004 | 0.008 | 0.493 | −0.046 | −0.081 | −0.011 | 0.01 |
| Childhood trauma-> relationship control | 0.052 | 0.01 | 0.094 | 0.015 | 0.034 | 0.02 | 0.048 | <0.001 | 0.086 | 0.045 | 0.128 | <0.001 |
| Sells on the streets-> drug use | 0.044 | 0.009 | 0.078 | 0.013 | 0.044 | 0.009 | 0.078 | 0.013 | ||||
| Childhood trauma-> drug use | 0.075 | 0.038 | 0.113 | <0.001 | 0.003 | 0.001 | 0.006 | 0.036 | 0.079 | 0.041 | 0.116 | <0.001 |
| Childhood trauma-> sells on the streets | 0.07 | 0.035 | 0.105 | <0.001 | 0.07 | 0.035 | 0.105 | <0.001 | ||||
| Childhood trauma-> sells in taverns | 0.036 | −0.001 | 0.073 | 0.058 | 0.036 | −0.001 | 0.073 | 0.058 | ||||
| Days selling in past month->stigma of SW | 0.164 | 0.129 | 0.199 | <0.001 | 0.164 | 0.129 | 0.199 | <0.001 | ||||
| Relationship control ->stigma of SW | 0.096 | 0.059 | 0.132 | <0.001 | 0.096 | 0.059 | 0.132 | <0.001 | ||||
| Sells on the streets->stigma of SW | 0.104 | 0.071 | 0.136 | <0.001 | −0.004 | −0.008 | −0.001 | 0.019 | 0.099 | 0.067 | 0.132 | <0.001 |
| Childhood trauma->stigma of SW | 0.346 | 0.309 | 0.384 | <0.001 | 0.038 | 0.028 | 0.049 | <0.001 | 0.385 | 0.347 | 0.422 | <0.001 |
| Food insecurity-> mental health | 0.224 | 0.18 | 0.267 | <0.001 | 0.066 | 0.051 | 0.082 | <0.001 | 0.29 | 0.247 | 0.333 | <0.001 |
| Part year non-partner rape -> mental health | 0.287 | 0.24 | 0.333 | <0.001 | 0.287 | 0.24 | 0.333 | <0.001 | ||||
| Violence -> mental health | 0.146 | 0.096 | 0.196 | <0.001 | 0.146 | 0.096 | 0.196 | <0.001 | ||||
| Childhood trauma -> mental health | 0.281 | 0.236 | 0.326 | <0.001 | 0.209 | 0.183 | 0.235 | <0.001 | 0.49 | 0.45 | 0.531 | <0.001 |
| Knows HIV+ status -> mental health | 0.041 | 0.002 | 0.08 | 0.038 | 0.041 | 0.002 | 0.08 | 0.038 | ||||
| Food insecurity ->violence | 0.115 | 0.075 | 0.156 | <0.001 | 0.022 | 0.009 | 0.034 | 0.001 | 0.137 | 0.094 | 0.18 | <0.001 |
| Relationship control ->violence | 0.291 | 0.25 | 0.332 | <0.001 | 0.031 | 0.019 | 0.044 | <0.001 | 0.322 | 0.28 | 0.365 | <0.001 |
| Stigma of SW-> violence | 0.326 | 0.28 | 0.371 | <0.001 | 0.326 | 0.28 | 0.371 | <0.001 | ||||
| Childhood trauma ->violence | 0.182 | 0.136 | 0.228 | <0.001 | 0.177 | 0.15 | 0.203 | <0.001 | 0.359 | 0.312 | 0.405 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jewkes, R.; Milovanovic, M.; Otwombe, K.; Chirwa, E.; Hlongwane, K.; Hill, N.; Mbowane, V.; Matuludi, M.; Hopkins, K.; Gray, G.; et al. Intersections of Sex Work, Mental Ill-Health, IPV and Other Violence Experienced by Female Sex Workers: Findings from a Cross-Sectional Community-Centric National Study in South Africa. Int. J. Environ. Res. Public Health 2021, 18, 11971. https://doi.org/10.3390/ijerph182211971
Jewkes R, Milovanovic M, Otwombe K, Chirwa E, Hlongwane K, Hill N, Mbowane V, Matuludi M, Hopkins K, Gray G, et al. Intersections of Sex Work, Mental Ill-Health, IPV and Other Violence Experienced by Female Sex Workers: Findings from a Cross-Sectional Community-Centric National Study in South Africa. International Journal of Environmental Research and Public Health. 2021; 18(22):11971. https://doi.org/10.3390/ijerph182211971
Chicago/Turabian StyleJewkes, Rachel, Minja Milovanovic, Kennedy Otwombe, Esnat Chirwa, Khuthadzo Hlongwane, Naomi Hill, Venice Mbowane, Mokgadi Matuludi, Kathryn Hopkins, Glenda Gray, and et al. 2021. "Intersections of Sex Work, Mental Ill-Health, IPV and Other Violence Experienced by Female Sex Workers: Findings from a Cross-Sectional Community-Centric National Study in South Africa" International Journal of Environmental Research and Public Health 18, no. 22: 11971. https://doi.org/10.3390/ijerph182211971