
Increasing Disaster Medical Assistance Teams’ Intent to Engage with Specific Hazards

 ,
,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
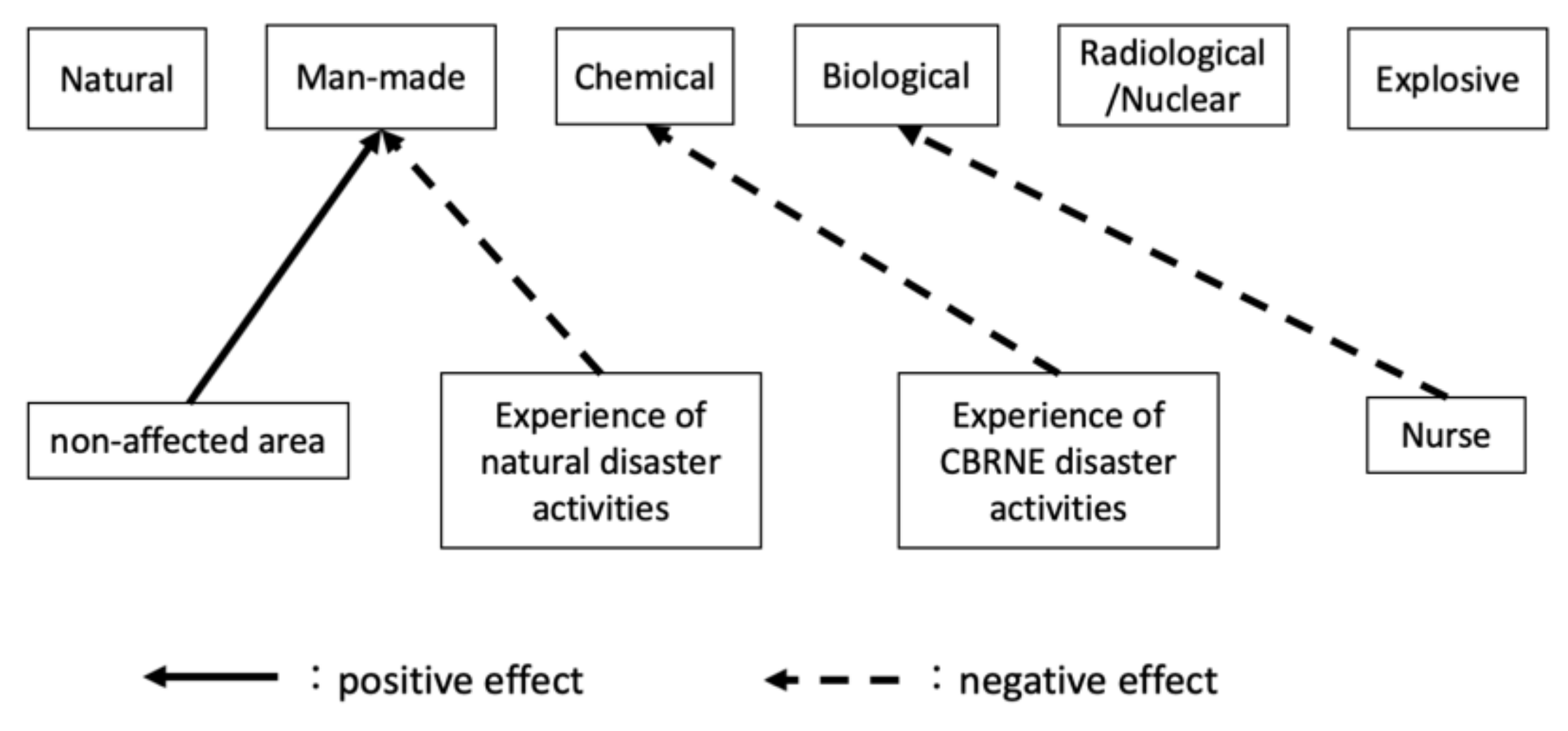
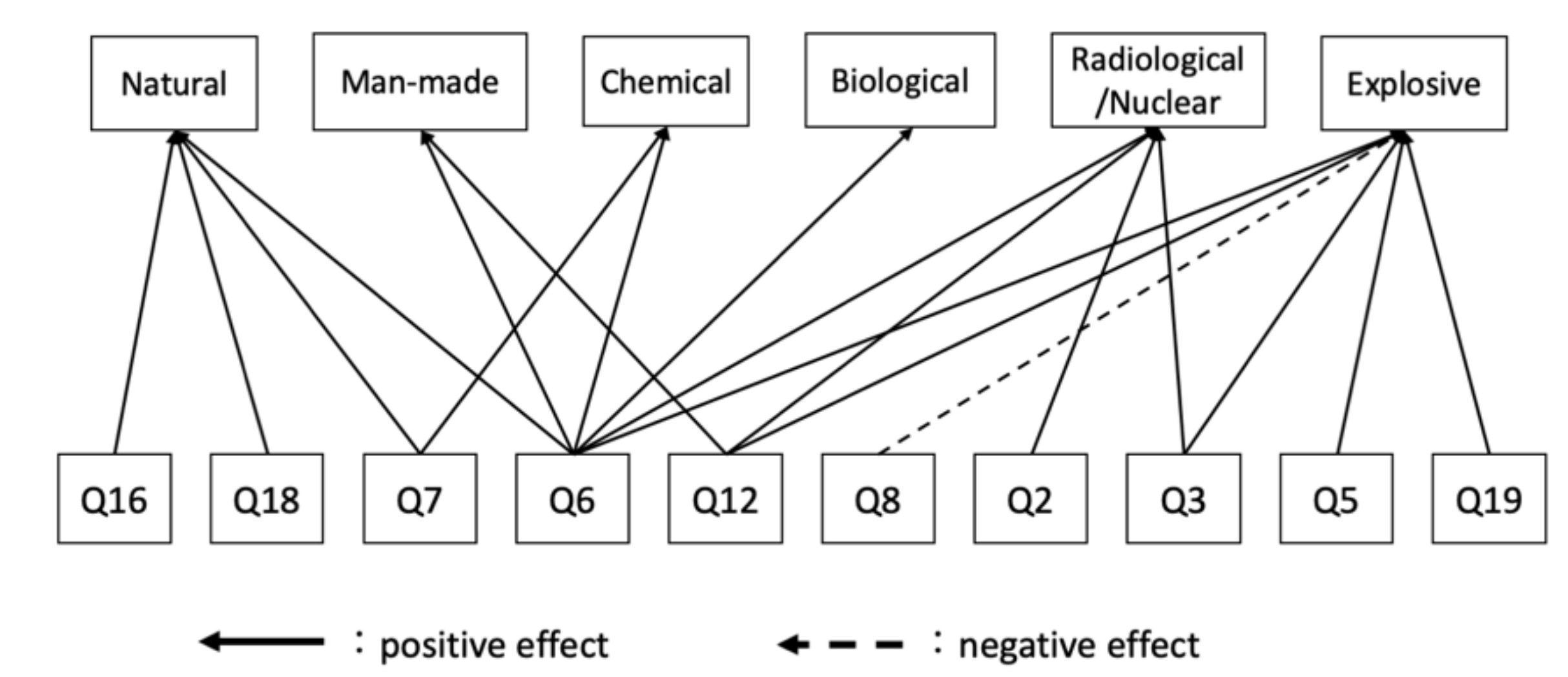
4.1. Factors Commonly Influencing Intent to Engage in Multiple Hazards
4.2. Factors Affecting Intent to Engage That Are Unique to Each Hazard
4.2.1. Natural Hazards
4.2.2. Man-Made Hazards
4.2.3. Chemical Incidents
4.2.4. Biological Incident
4.2.5. Radiological/Nuclear Incidents
4.2.6. Explosive Incidents
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Natural | Man-Made | Chemical | Biological | Radiological/Nuclear | Explosive | p Value (ANOVA) | |
|---|---|---|---|---|---|---|---|
| Q1 | 82.2 a | 81.7 a | 50.0 bc | 47.4 c | 57.6 b | 52.4 bc | <0.01 |
| Q2 | 94.1 a | 88.3 ab | 77.6 c | 77.0 c | 81.6 bc | 75.9 c | <0.01 |
| Q3 | 88.6 a | 85.8 a | 65.2 b | 63.6 b | 70.8 b | 64.5 b | <0.01 |
| Q4 | 70.2 a | 59.5 b | 34.9 c | 34.9 c | 56.4 b | 32.6 c | <0.01 |
| Q5 | 89.5 a | 84.3 a | 64.2 c | 64.4 c | 73.7 b | 66.0 bc | <0.01 |
| Q6 | 90 a | 87.9 a | 67.6 b | 67.3 b | 74.4 b | 68.3 b | <0.01 |
| Q7 | 82.5 a | 82.7 a | 49.9 b | 49.8 b | 54.6 b | 51.4 b | <0.01 |
| Q8 | 98.1 a | 97.4 a | 97.4 a | 97.3 a | 97.4 a | 96.4 a | 0.80 |
| Q9 | 93.6 a | 90.9 ab | 77.7 c | 78.4 c | 83.1 bc | 78.8 c | <0.01 |
| Q10 | 52.6 a | 36.9 b | 15.2 c | 17.3 c | 38.5 b | 15.6 c | <0.01 |
| Q11 | 82.4 a | 69.1 b | 34.5 d | 34.0 d | 48.4 c | 44.6 c | <0.01 |
| Q12 | 58.4 a | 52.5 a | 15.0 c | 16.9 c | 31.8 b | 19.0 c | <0.01 |
| Q13 | 74.0 a | 71.4 a | 88.5 b | 88.6 b | 81.9 b | 89.2 b | <0.01 |
| Q14 | 90.4 a | 91.4 a | 93.2 a | 93.3 a | 92.3 a | 92.9 a | 0.66 |
| Q15 | 90.6 a | 86.8 a | 73.4 a | 73.9 b | 78.5 b | 73.8 b | <0.01 |
| Q16 | 90.0 a | 86.2 ab | 70.8 c | 71.5 c | 77.8 bc | 70.0 c | <0.01 |
| Q17 | 65.4 a | 56.1 ab | 32.9 c | 34.2 c | 51.4 b | 32.3 c | <0.01 |
| Q18 | 90.6 a | 87.0 ab | 71.4 c | 71.7 c | 78.6 bc | 71.4 c | <0.01 |
| Q19 | 29.5 a | 24.8 ab | 19.8 ab | 20.2 ab | 23.1 ab | 19.1 b | 0.02 |
| Q20 | 99.1 a | 97.6 a | 95.9 a | 96.2 a | 96.7 a | 95.5 a | 0.10 |
Appendix B
| Natural | Man-Made | Chemical | Biological | Radiological/ Nuclear | Explosive | |
|---|---|---|---|---|---|---|
| Adjusted R2 | 0.46 | 0.50 | 0.61 | 0.56 | 0.64 | 0.67 |
| Background factors | ||||||
| Nonaffected area | 0.05 | 0.12 | −0.06 | −0.03 | −0.06 | −0.05 |
| Occupation vs. administrative and nonmedical staff | ||||||
| Physician | 0.00 | −0.01 | 0.12 | 0.11 | 0.00 | 0.10 |
| Nurse | 0.03 | 0.09 | −0.12 | −0.15 | −0.07 | −0.04 |
| Other medical staff | −0.04 | −0.11 | −0.11 | −0.13 | −0.07 | −0.09 |
| Female | −0.05 | −0.04 | −0.09 | −0.06 | −0.01 | −0.11 |
| Age < 40 | −0.04 | 0.00 | −0.03 | −0.07 | −0.07 | 0.02 |
| Family—with | −0.10 | −0.07 | 0.01 | 0.00 | 0.01 | −0.04 |
| Disaster base hospital—No | 0.02 | 0.05 | 0.00 | −0.02 | 0.03 | −0.01 |
| Experience in natural disaster response activities—Yes | 0.07 | −0.14 | −0.04 | −0.05 | −0.02 | −0.05 |
| Experience in CBRNE disaster response activities—Yes | −0.07 | −0.03 | −0.12 | −0.09 | −0.07 | −0.08 |
| Questionnaire answers | ||||||
| Q2 | 0.02 | 0.14 | 0.07 | 0.02 | 0.17 | 0.06 |
| Q3 | 0.00 | 0.11 | 0.07 | 0.09 | 0.17 | 0.19 |
| Q4 | 0.06 | 0.04 | 0.05 | 0.11 | 0.03 | −0.05 |
| Q5 | 0.05 | 0.13 | − | − | − | 0.37 |
| Q6 | 0.31 | 0.18 | 0.42 | 0.43 | 0.28 | 0.31 |
| Q7 | 0.28 | 0.11 | 0.17 | 0.14 | 0.10 | 0.05 |
| Q8 | 0.01 | 0.07 | −0.09 | −0.09 | −0.07 | −0.13 |
| Q9 | −0.08 | −0.07 | −0.02 | −0.05 | −0.04 | −0.04 |
| Q10 | −0.10 | 0.02 | 0.06 | −0.01 | 0.04 | 0.04 |
| Q11 | 0.03 | 0.05 | 0.05 | 0.02 | −0.11 | 0.01 |
| Q12 | 0.09 | 0.18 | 0.08 | 0.10 | 0.21 | 0.11 |
| Q13 | −0.01 | −0.09 | −0.07 | −0.05 | 0.00 | 0.00 |
| Q14 | −0.03 | −0.02 | 0.02 | 0.01 | −0.05 | 0.03 |
| Q15 | −0.06 | −0.01 | 0.05 | 0.07 | 0.05 | 0.05 |
| Q16 | 0.16 | −0.13 | −0.04 | −0.08 | −0.08 | −0.14 |
| Q17 | −0.07 | −0.09 | −0.06 | −0.08 | 0.01 | 0.01 |
| Q18 | 0.20 | 0.17 | 0.11 | 0.13 | 0.14 | − |
| Q19 | 0.04 | −0.01 | 0.08 | 0.09 | 0.06 | 0.15 |
| Q20 | 0.00 | 0.08 | 0.02 | 0.07 | 0.04 | −0.03 |
References
- Lee, A.; Bishop, G.; Hillman, K.M.; Daffurn, K. The Medical Emergency Team. Anaesth. Intensive Care 1995, 23, 183–186. [Google Scholar] [CrossRef] [Green Version]
- Buist, M.D.; Moore, G.E.; Bernard, S.A.; Waxman, B.P.; Anderson, J.N.; Nguyen, T.V. Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: Preliminary study. BMJ 2002, 324, 387–390. [Google Scholar] [CrossRef] [Green Version]
- Jones, D.A.; DeVita, M.A.; Bellomo, R. Rapid-response teams. N. Engl. J. Med. 2011, 365, 139–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritchie, H. “Natural Disasters”. Available online: https://ourworldindata.org/natural-disasters (accessed on 23 October 2021).
- U.S. Geological Survey. New Earthquake Hazards Program. Available online: https://www.usgs.gov/natural-hazards/earthquake-hazards/lists-maps-and-statistics (accessed on 23 October 2021).
- Japan Meteorological Agency. Earthquake Intensity Database (In Japanese). Available online: https://www.data.jma.go.jp/svd/eqdb/data/shindo/index.html (accessed on 23 October 2021).
- National Consortium for the Study of Terrorism and Responses to Terrorism. Global Terrorism Overview: Terrorism in 2019. Available online: https://www.start.umd.edu/pubs/START_GTD_GlobalTerrorismOverview2019_July2020.pdf (accessed on 23 October 2021).
- Stevens, G.; Jones, A.; Smith, G.; Nelson, J.; Agho, K.; Taylor, M.; Raphael, B. Determinants of paramedic response readiness for CBRNE threats. Biosecur. Bioterror. 2010, 8, 193–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razak, S.; Hignett, S.; Barnes, J. Emergency Department Response to Chemical, Biological, Radiological, Nuclear, and Explosive Events: A Systematic Review. Prehospital Disaster Med. 2018, 33, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Khorram-Manesh, K.; Goniewicz, K.; Hertelendy, A.; Dulebenets, M. Handbook of Disaster and Emergency Management, 2nd ed.; Kompendiet: Gothenburg, Sweden, 2021. [Google Scholar] [CrossRef]
- The National Diet of Japan, the Fukushima Nuclear Accident Independent Investigation Commission. The Official Report of The Fukushima Nuclear Accident Independent Investigation Commission. Available online: https://warp.da.ndl.go.jp/info:ndljp/pid/3856371/naiic.go.jp/en/report/ (accessed on 23 October 2021).
- Iyama, K.; Kakamu, T.; Yamashita, K.; Shimada, J.; Tasaki, O.; Hasegawa, A. Survey about Intention to Engage in Specific Disaster Activities among Disaster Medical Assistance Team Members. Prehospital Disaster Med. 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Lanzilotti, S.S.; Galanis, D.; Leoni, N.; Craig, B. Hawaii medical professionals assessment. Hawaii Med. J. 2002, 61, 162–173. [Google Scholar] [PubMed]
- Kaya, E.; Altintas, H. Willingness of Firefighting Program Students to Work in Disasters-Turkey. Prehospital Disaster Med. 2018, 33, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.C.; Burkle, F.M., Jr.; Archer, F.L. Fear, familiarity, and the perception of risk: A quantitative analysis of disaster-specific concerns of paramedics. Disaster Med. Public Health Prep. 2011, 5, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Iyama, K.; Takano, Y.; Takahashi, T.; Hasegawa, A. Factors associated with the intention to participate in activities during a nuclear disaster situation among firefighters. J. Radiat. Res. 2020, 61, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Cabinet Office, Government of Japan. Disaster Management in Japan. Available online: http://www.bousai.go.jp/1info/pdf/saigaipamphlet_je.pdf (accessed on 23 October 2021).
- Ministry of Health, Labour and Welfare Japan. Damages and Response to Great East Japan Earthquake. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10800000-Iseikyoku/0000103405.pdf (accessed on 23 October 2021).
- Fishbein, M.; Ajzen, I. Belief, Attitude, Intention and Behaviour: An Introduction to Theory and Research. Available online: https://people.umass.edu/aizen/f&a1975.html (accessed on 23 October 2021).
- Ajzen, I.; Driver, B.L. Prediction of Leisure Participation from Behavioral, Normative, and Control Beliefs: An Application of the Theory of Planned Behavior. Leis. Sci. 1991, 13, 185–204. [Google Scholar] [CrossRef]
- Takahashi, T.; Iyama, K.; Murakami, M.; Hasegawa, A. Factors affecting the intention of nuclear disaster response activities in paramedic students. J. Jpn. Soc. Emerg. Med. 2021, 24, 320–330. [Google Scholar] [CrossRef]
- Nishi, D.; Koido, Y.; Nakaya, N.; Sone, T.; Noguchi, H.; Hamazaki, K.; Hamazaki, T.; Matsuoka, Y. Peritraumatic distress, watching television, and posttraumatic stress symptoms among rescue workers after the Great East Japan earthquake. PLoS ONE 2012, 7, e35248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Police Agency. White Paper on Police Excerpt (In Japanese). Available online: https://www.npa.go.jp/hakusyo/h30/data.html (accessed on 23 October 2021).
- Automobile Inspection & Registration Information Association. Number of Private Passenger Cars in Use in Japan (In Japanese). Available online: https://www.airia.or.jp/publish/statistics/mycar.html (accessed on 23 October 2021).
- Japanese Nursing Association. Survey Results on the Actual Status of Nurses’ Responses to COVID-19. Available online: https://www.nurse.or.jp/jna/english/news/pdf/2021nr_34.pdf (accessed on 23 October 2021).
- Nursing Times. Nursing Times Survey Reveals Negative Impact of Covid-19 on Nurse Mental Health. Available online: https://www.nursingtimes.net/news/mental-health/exclusive-survey-reveals-negative-impact-of-covid-19-on-nurse-mental-health-29-04-2020/ (accessed on 23 October 2021).
- Li, R.; Chen, Y.; Lv, J.; Liu, L.; Zong, S.; Li, H.; Li, H. Anxiety and related factors in frontline clinical nurses fighting COVID-19 in Wuhan. Med. Baltim. 2020, 99, e21413. [Google Scholar] [CrossRef] [PubMed]
- Nozaki, H.; Hori, S.; Shinozawa, Y.; Fujishima, S.; Takuma, K.; Sagoh, M.; Kimura, H.; Ohki, T.; Suzuki, M.; Aikawa, N. Secondary exposure of medical staff to sarin vapor in the emergency room. Intensive Care Med. 1995, 21, 1032–1035. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Zhang, F. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Wagner, R.H.; Boles, M.A.; Henkin, R.E. Treatment of radiation exposure and contamination. Radiographics 1994, 14, 387–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| n = 178 | |
|---|---|
| Area, n (%) | |
| Nuclear-disaster-affected area | 79 (44.4) |
| Nonaffected area | 99 (55.6) |
| Sex, n (%) | |
| Female | 128 (71.9) |
| Male | 80 (28.1) |
| Age (years), n (%) | |
| 20−29 | 14 (7.9) |
| 30−39 | 70 (39.3) |
| 40−49 | 67 (37.6) |
| Over 50 | 27 (15.2) |
| Occupation, n (%) | |
| Physician | 41 (23.0) |
| Nurse | 69 (38.8) |
| Other medical staff | 26 (14.6) |
| Administrative staff (nonmedical) | 42 (23.6) |
| Family, n (%) | |
| With | 135 (75.8) |
| Without | 43 (24.2) |
| Disaster base hospital, n (%) | |
| Yes | 141 (79.2) |
| No | 37 (20.8) |
| Experience in natural disaster response activities, n (%) | |
| Yes | 123 (69.1) |
| No | 55 (30.9) |
| Experience in CBRNE disaster response activities, n (%) | |
| Yes | 14 (7.9) |
| No | 164 (92.1) |
| Q1 | Would you Willingly Actively Engage in Response Activities during a D hazard? |
|---|---|
| Q2 | Would you willingly collect information preparing for a D hazard? |
| Q3 | Do you think that your occupation should actively response to a D hazard? |
| Q4 | How much opportunities do you have to learn about D hazards in your environment? |
| Q5 | How much interest do you have in D hazards? |
| Q6 | Will you engage in D disaster response activities if there are incentives, such as insurance and special salaries? |
| Q7 | How much do you think your family will understand about your activity during a D hazard? |
| Q8 | Do you think that education and training are indispensable for D disaster response activities? |
| Q9 | If your colleagues are preparing for D hazards (e.g., education or training), do you think you should take action as well? |
| Q10 | Does your workplace offer seminars on D disaster response? |
| Q11 | How often do you think a D hazard will occur in your area? |
| Q12 | Do you have self-confidence in D disaster response activities? |
| Q13 | Are you anxious about the activities in a D hazard situation? |
| Q14 | Do you feel sorry to your family if you are exposed to D hazards? |
| Q15 | Would you willingly actively work on D hazard countermeasures? |
| Q16 | Do you think that your own occupation should be routinely educated and trained on D hazards to meet the expectations of citizens? |
| Q17 | At your own workplace, is it easy to obtain information about seminars for D disaster response? |
| Q18 | Would you willingly actively participate in seminars on D hazards? |
| Q19 | If your family is safe, can you be exposed to D hazards during a disaster response? |
| Q20 | How much do you think it is important to prepare for a D hazard (e.g., education or training)? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iyama, K.; Kakamu, T.; Yamashita, K.; Sato, Y.; Shimada, J.; Tasaki, O.; Hasegawa, A. Increasing Disaster Medical Assistance Teams’ Intent to Engage with Specific Hazards. Int. J. Environ. Res. Public Health 2021, 18, 11630. https://doi.org/10.3390/ijerph182111630
Iyama K, Kakamu T, Yamashita K, Sato Y, Shimada J, Tasaki O, Hasegawa A. Increasing Disaster Medical Assistance Teams’ Intent to Engage with Specific Hazards. International Journal of Environmental Research and Public Health. 2021; 18(21):11630. https://doi.org/10.3390/ijerph182111630
Chicago/Turabian StyleIyama, Keita, Takeyasu Kakamu, Kazunori Yamashita, Yoshinobu Sato, Jiro Shimada, Osamu Tasaki, and Arifumi Hasegawa. 2021. "Increasing Disaster Medical Assistance Teams’ Intent to Engage with Specific Hazards" International Journal of Environmental Research and Public Health 18, no. 21: 11630. https://doi.org/10.3390/ijerph182111630