
Loneliness and Depression among Women in Poland during the COVID-19 Pandemic


Abstract
:1. Introduction
2. Aim of the Study
3. Materials and Methods
3.1. Participants
3.2. Measurement
3.2.1. Socio-Demographic Questionnaire
3.2.2. Hospital Anxiety and Depression Scale (HADS-M)
3.2.3. R-UCLA
3.2.4. Statistical Method
4. Results
4.1. Characteristics of the Study Group
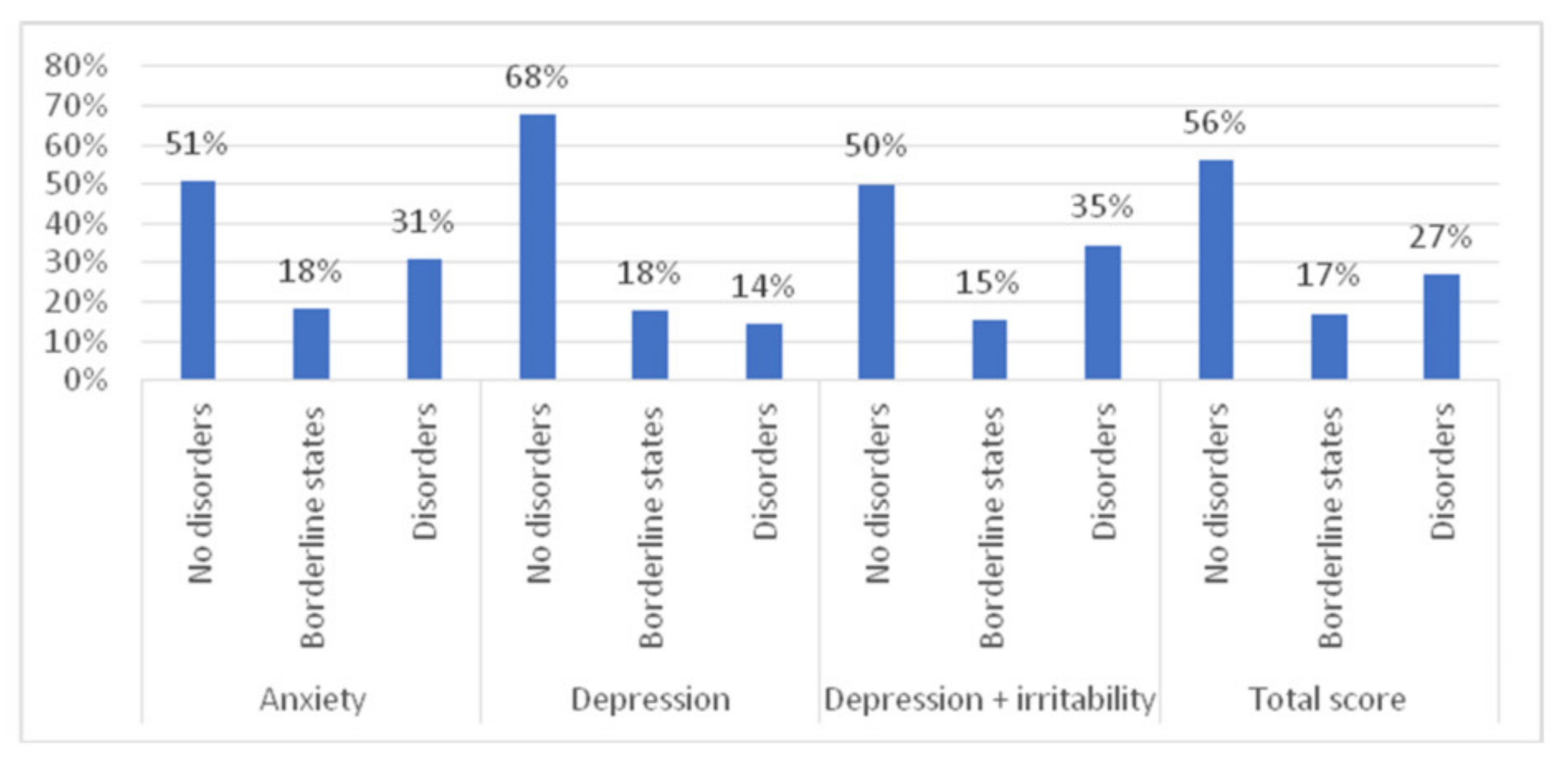
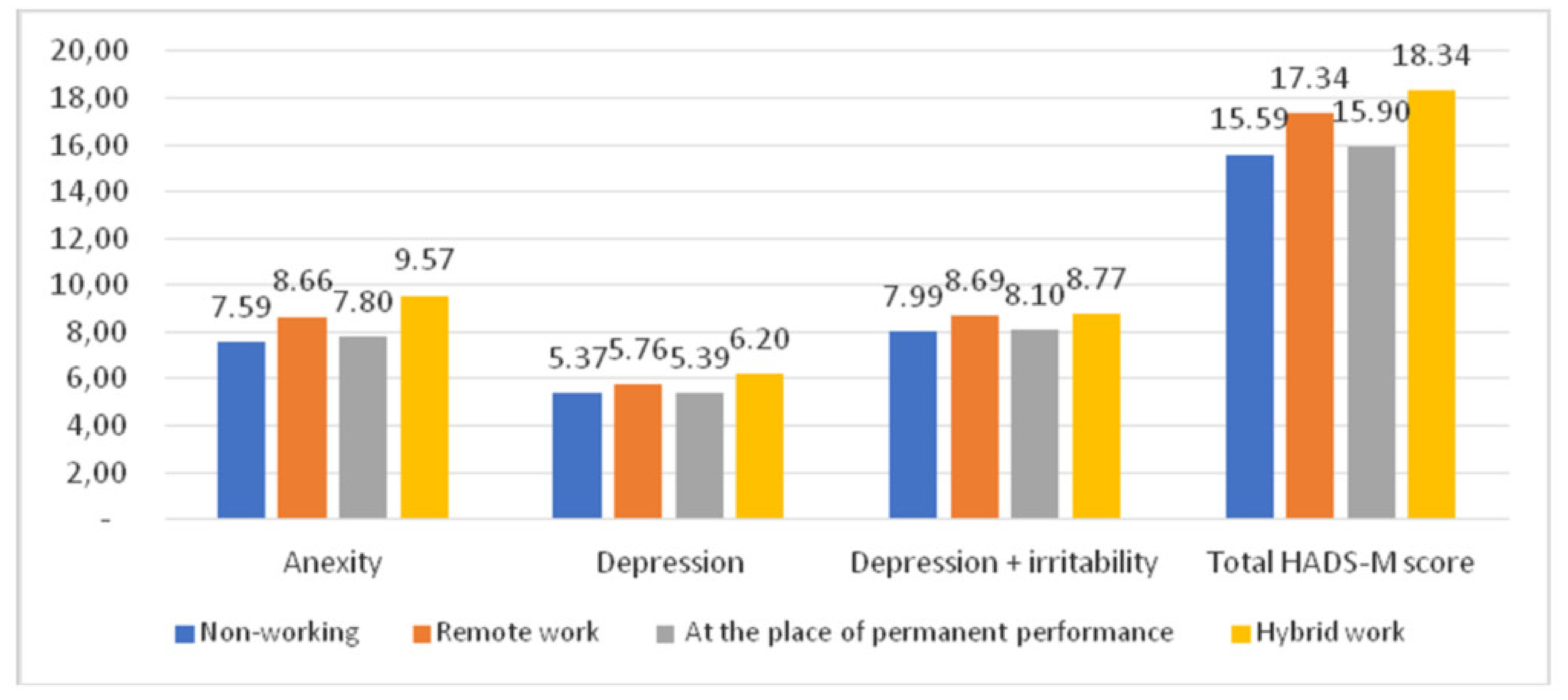
4.2. Anxiety, Depression, and Irritability
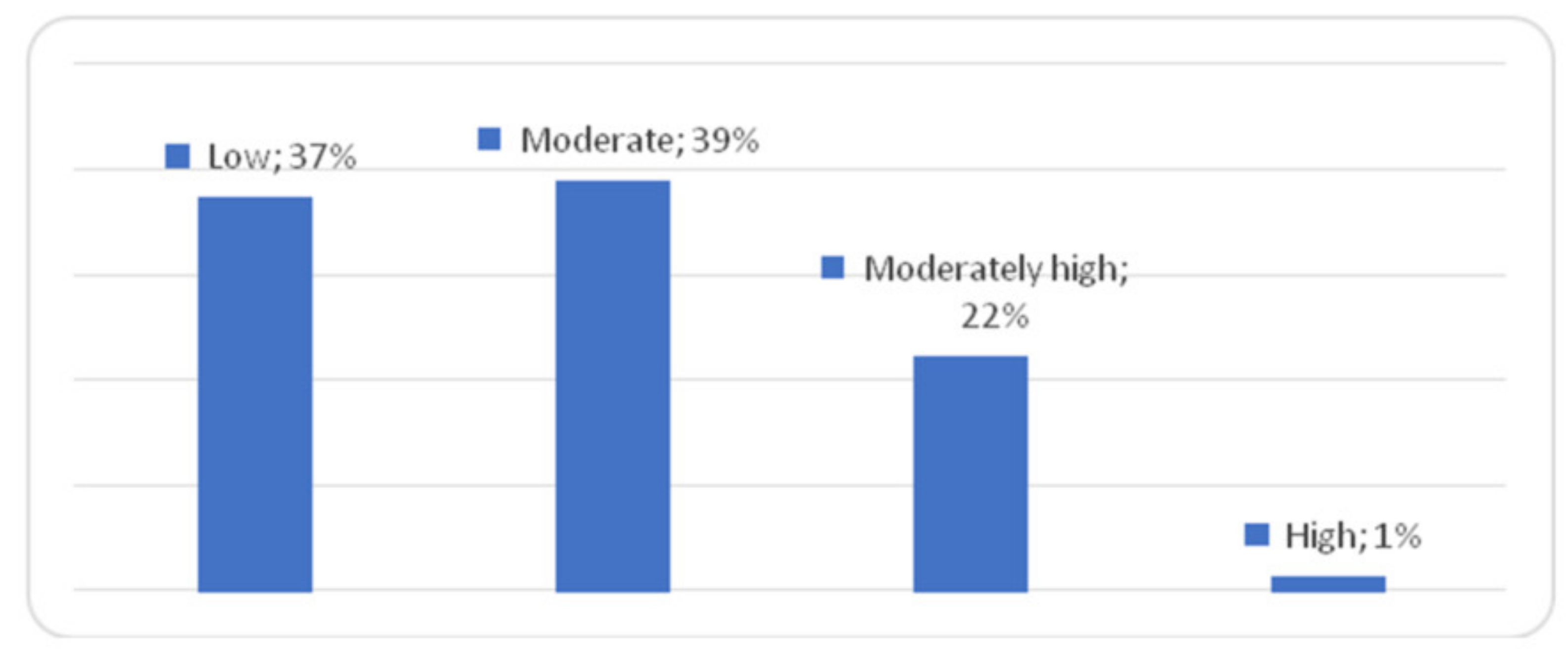
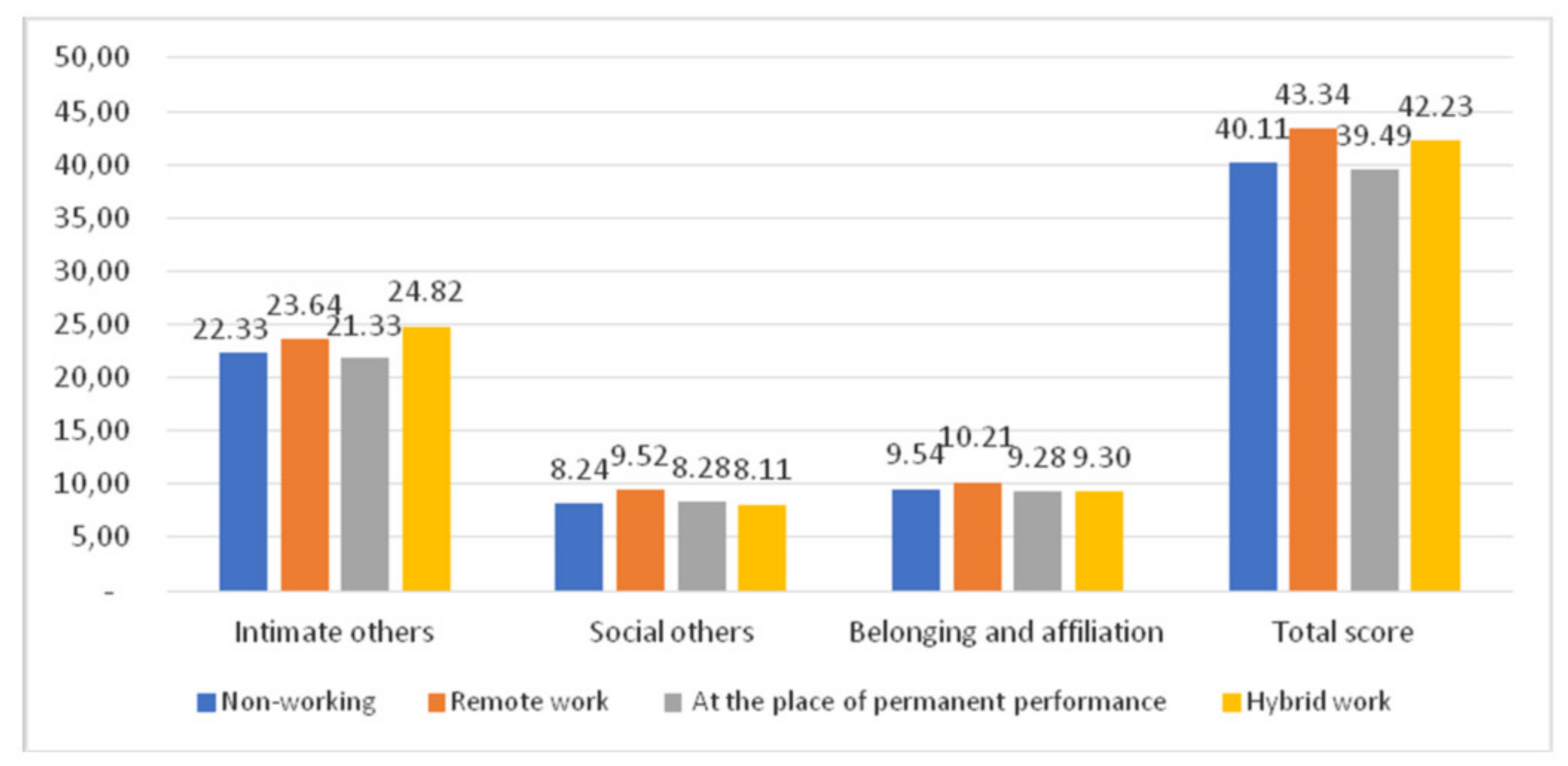
4.3. Loneliness
4.4. Correlations between Loneliness and Anxiety, Depression, and Irritability
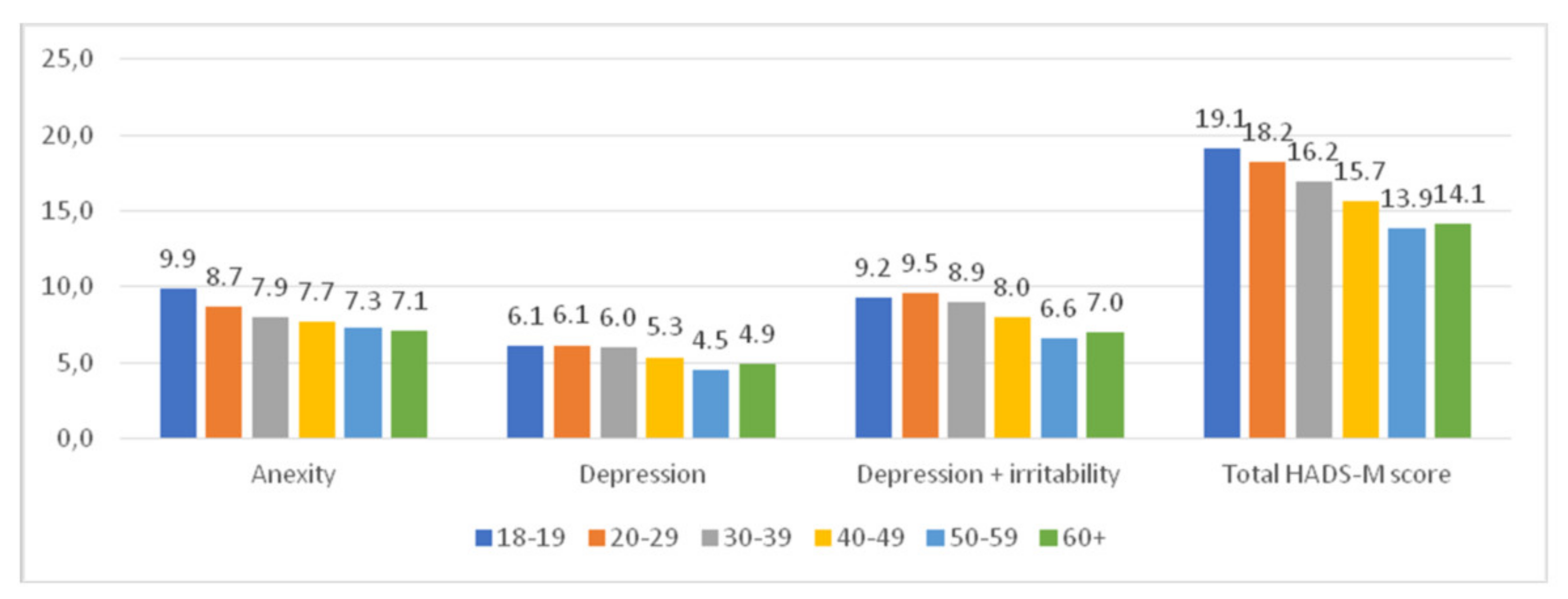
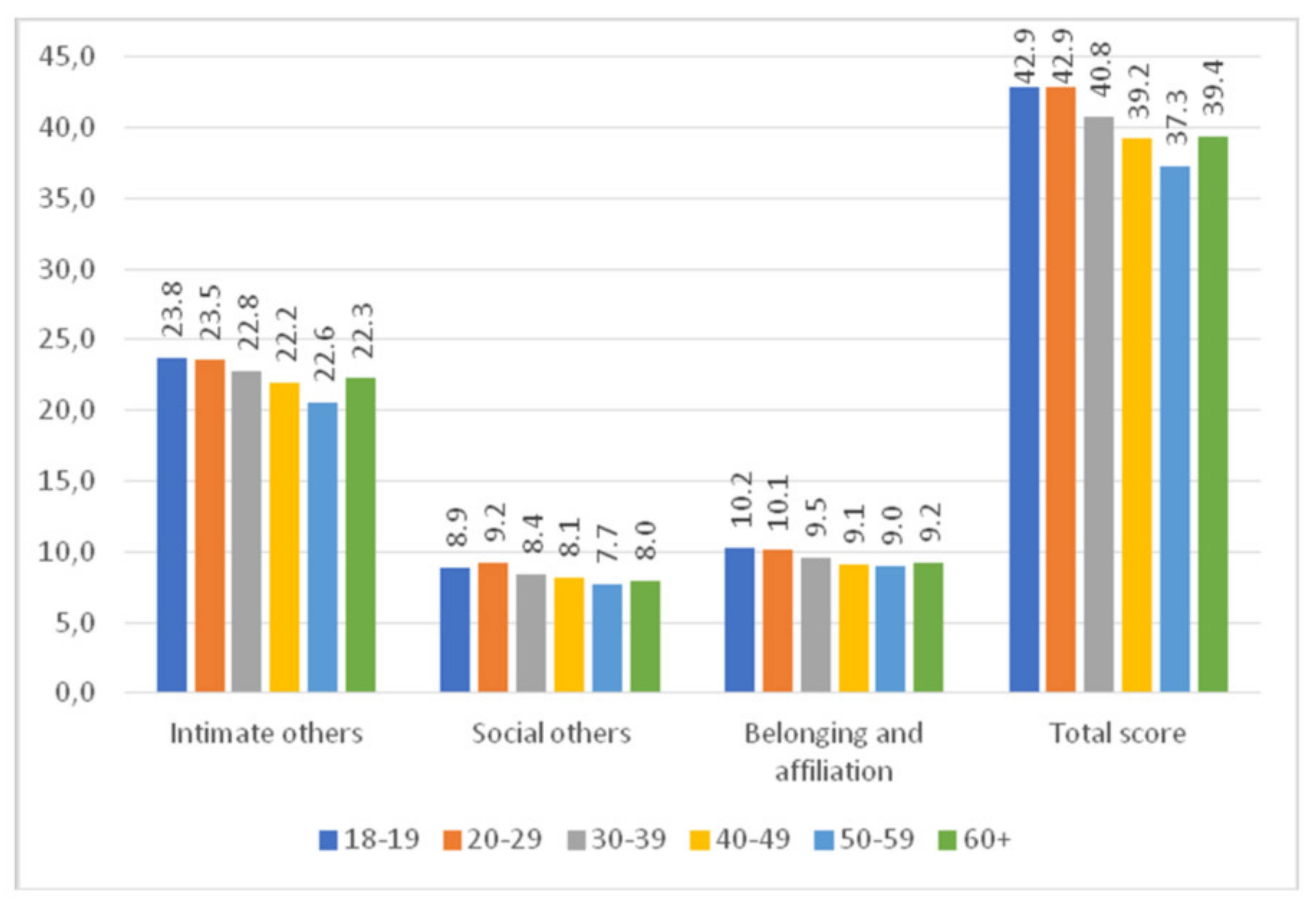
4.5. Sociodemographic Variables and the Severity of Anxiety, Depression, Irritation, and Loneliness
4.6. Health Variables and the Severity of Anxiety, Depression, Irritability, and Loneliness
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Roy, D.; Tripathy, S.; Kar, S.K.; Sharma, N.; Verma, S.K.; Kaushal, V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J. Psychiatr. 2020, 51, 102083. [Google Scholar] [CrossRef]
- Valtorta, N.; Hanratty, B. Loneliness, isolation and the health of older adults: Do we need a new research agenda? J. R. Soc. Med. 2012, 105, 518–522. [Google Scholar] [CrossRef] [Green Version]
- Tanskanen, J.; Anttila, T. A Prospective Study of Social Isolation, Loneliness, and Mortality in Finland. Am. J. Public Health 2016, 106, 2042–2048. [Google Scholar] [CrossRef] [PubMed]
- Dragan, M. Report: Mental Health during the COVID-19 Pandemic. Available online: http://psych.uw.edu.pl/2020/05/04/zdrowie-psychiczne-w-czasie-pandemii-covid-19-raport-wstepny-z-badania-naukowego-kierowanego-przez-dr-hab-malgorzate-dragan/ (accessed on 30 April 2021).
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heitzman, J. Impact of COVID-19 pandemic on mental health. Psychiatr. Pol. 2020, 54, 187–198. [Google Scholar] [CrossRef]
- Jia, R.; Ayling, K.; Chalder, T.; Massey, A.; Broadbent, E.; Coupland, C.; Vedhara, K. Mental health in the UK during the COVID-19 pandemic: Cross-sectional analyses from a community cohort study. BMJ Open 2020, 10, e040620. [Google Scholar] [CrossRef]
- Erzen, E.; Cikrikci, O. The effect of loneliness on depression: A meta-analysis. Int. J. Soc. Psychiatry 2018, 64, 427–435. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Cacioppo, S.; Capitanio, J.P.; Cole, S.W. The neuroendocrinology of social isolation. Annu. Rev. Psychol. 2015, 66, 733–767. [Google Scholar] [CrossRef] [Green Version]
- Sokół-Szawłowska, M. Mental health impact of quarantine during the COVID-19 pandemic. Psychiatria 2021, 18, 57–62. [Google Scholar] [CrossRef]
- Hossain, M.M.; Sultana, A.; Purohit, N. Mental health outcomes of quarantine and isolation for infection prevention: A systematic umbrella review of the global evidence. Epidemiol. Health 2020, 42, e2020038. [Google Scholar] [CrossRef]
- Meng, H.; Xu, Y.; Dai, J.; Zhang, Y.; Liu, B.; Yang, H. Analyze the psychological impact of COVID-19 among the elderly population in China and make corresponding suggestions. Psychiatry Res. 2020, 289, 112983. [Google Scholar] [CrossRef]
- Lipiec, A. Depression in Poland—What is the Scale of the Problem? National Health Fund Report. Available online: https://www.medonet.pl/zdrowie,depresja-w-polsce---jaka-jest-skala-problemu--raport-nfz,artykul,26023010.html (accessed on 26 April 2021).
- It is Responsible for More than 5000 Suicides in Poland. Available online: https://www.medonet.pl/zdrowie,who--depresja-w-czolowce-chorob-na-swiecie,artykul,1724647.html (accessed on 26 April 2021).
- Mental Health in the EU Chancellery of the Senate of the Republic of Poland Report. 2019. Available online: https://orka.sejm.gov.pl/przeglad.nsf/0/F30DBEBD573465A1C125857A005DB92E/$file/13.Varia.pdf (accessed on 25 July 2021).
- United Nations. Policy Brief: COVID-19 and the Need for Action on Mental Health. Available online: https://unsdg.un.org/sites/default/files/2020-05/UN-Policy-Brief-COVID-19-and-mental-health.pdf (accessed on 26 April 2021).
- Holbrook, T.L.; Hoyt, D.B. The impact of major trauma: Quality-of-life outcomes are worse in women than in men, independent of mechanism and injury severity. J. Trauma 2004, 56, 284–290. [Google Scholar] [CrossRef]
- Holbrook, T.L.; Hoyt, D.B.; Stein, M.B.; Sieber, W.J. Gender differences in long-term posttraumatic stress disorder outcomes after major trauma: Women are at higher risk of adverse outcomes than men. J. Trauma 2002, 53, 882–888. [Google Scholar] [CrossRef] [PubMed]
- McQuaid, R.J.; Cox, S.; Ogunlana, A.; Jaworska, N. The burden of loneliness: Implications of the social determinants of health during COVID-19. Psychiatry Res. 2021, 296, 113648. [Google Scholar] [CrossRef] [PubMed]
- Solomou, I.; Constantinidou, F. Prevalence and Predictors of Anxiety and Depression Symptoms during the COVID-19 Pandemic and Compliance with Precautionary Measures: Age and Sex Matter. Int. J. Environ. Res. Public Health 2020, 17, 4924. [Google Scholar] [CrossRef] [PubMed]
- Majkowicz, M. Practical assessment of the effectiveness of palliative care—Selected research techniques. In Assessment of Palliative Care Quality in Theory and Pracice, 1st ed.; De Walden-Gałuszko, K., Majkowicz, M., Eds.; Akademia Medyczna: Gdańsk, Poland, 2000; pp. 21–42. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwiatkowska, M.M.; Rogoza, R.; Kwiatkowska, K. Analysis of the psychometric properties of the Revised UCLA Loneliness Scale in a Polish adolescent sample. Curr. Issues Personal. Psychol. 2018, 6, 164–170. [Google Scholar] [CrossRef] [Green Version]
- Russell, D.; Peplau, L.A.; Cutrona, C.E. The revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. J. Pers. Soc. Psychol. 1980, 39, 472–480. [Google Scholar] [CrossRef]
- Perry, G. Loneliness and coping among tertiary level adult cancer patients in the home. Cancer Nurs. 1990, 13, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Guilford, J.P. Fundamental Statistics in Psychology and Education; McGraw-Hill Book Company: New York, NY, USA, 1956; Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/sce.3730410357 (accessed on 26 April 2021).
- Wenham, C.; Smith, J.; Morgan, R. COVID-19: The gendered impacts of the outbreak. Lancet 2020, 395, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Asmundson, G.J.G.; Taylor, S. Coronaphobia: Fear and the 2019-nCoV outbreak. J. Anxiety Disord. 2020, 70, 102196. [Google Scholar] [CrossRef] [PubMed]
- Tull, M.T.; Edmonds, K.E.; Scamaldo, K.M.; Richmond, J.R.; Rose, J.P.; Gratz, K.L. Psychological Outcomes Associated with Stay-at-Home Orders and the Perceived Impact of COVID-19 on Daily Life. Psychiatry Res. 2020, 289, 113098. [Google Scholar] [CrossRef]
- Bartoszek, A.; Walkowiak, D.; Bartoszek, A.; Kardas, G. Mental Well-Being (Depression, Loneliness, Insomnia, Daily Life Fatigue) during COVID-19 Related Home-Confinement-A Study from Poland. Int. J. Environ. Res. Public Health 2020, 17, 7417. [Google Scholar] [CrossRef]
- Moghanibashi-Mansourieh, A. Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian J. Psychiatr. 2020, 51, 102076. [Google Scholar] [CrossRef]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: Immediate psychological responses and associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef]
- Shi, L.; Lu, Z.A.; Que, J.Y.; Huang, X.L.; Liu, L.; Ran, M.S. Prevalence of and risk factors associated with mental health symptoms among the general population in China during the coronavirus disease 2019 pandemic. JAMA Netw. Open 2020, 3, e2014053. [Google Scholar] [CrossRef]
- Robb, C.E.; Jager, C.A.; Ahmadi-Abhari, S.; Giannakopoulou, P.; Udeh-Momoh, C.; McKeand, J.; Price, G.; Car, J.; Majeed, A.; Ward, H.; et al. Associations of social isolation with anxiety and depression during the early COVID-19 pandemic: A Survey of older adults in London UK. Front. Psychiatry 2020, 11, 591120. [Google Scholar] [CrossRef] [PubMed]
- Parlapani, E.; Holeva, V.; Nikopoulou, V.A.; Sereslis, K.; Athanasiadou, M.; Godosidis, A.; Stephanou, T.; Diakogiannis, I. Intolerance of uncertainty and loneliness in older adults during the COVID-19 pandemic. Front. Psychiatry 2020, 11, 842. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Zhang, F.; Wei, C.; Jia, Y.; Shang, Z.; Sun, L.; Wu, L.; Sun, Z.; Zhou, Y.; Wang, Y.; et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Res. 2020, 287, 112921. [Google Scholar] [CrossRef]
- Wu, M.; Han, H.; Lin, T.; Chen, M.; Wu, J.; Du, X.; Su, G.; Wu, D.; Chen, F.; Zhang, Q.; et al. Prevalence and risk factors of mental distress in China during the outbreak of COVID-19: A national cross-sectional survey. Brain Behav. 2020, 10, e01818. [Google Scholar] [CrossRef]
- Freeman, A.; Tyrovolas, S.; Koyanagi, A.; Chatterji, S.; Leonardi, M.; Ayuso-Mateos, J.L.; Tobiasz-Adamczyk, B.; Koskinen, S.; Rummel-Kluge, C.; Haro, J.M. The role of socio-economic status in depression: Results from the COURAGE (aging survey in Europe). BMC Public Health 2016, 16, 1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorant, V.; Croux, C.; Weich, S.; Deliège, D.; Mackenbach, J.; Ansseau, M. Depression and socio-economic risk factors: 7-year longitudinal population study. Br. J. Psychiatry 2007, 190, 293–298. [Google Scholar] [CrossRef]
- Christensen, A.V.; Juel, K.; Ekholm, O.; Thrysøe, L.; Thorup, C.B.; Borregaard, B.; Mols, R.E.; Rasmussen, T.B.; Berg, S.K. Significantly increased risk of all-cause mortality among cardiac patients feeling lonely. Heart 2020, 106, 140–146. [Google Scholar] [CrossRef]
- Rodriguez-Rey, R.; Garrido-Hernansaiz, H.; Collado, S. Psychological impact and associated factors during the initial stage of the Coronavirus (COVID-19) pandemic among the general population in Spain. Front. Psychol. 2020, 11, 154. [Google Scholar] [CrossRef]
- Tian, F.; Li, H.; Tian, S.; Yang, J.; Shao, J.; Tian, C. Psychological symptoms of ordinary Chinese citizens based on SCL-90 during the level I emergency response to COVID-19. Psychiatry Res. 2020, 288, 112992. [Google Scholar] [CrossRef]
- Losda-Baltar, A.; Jiménez-Gonzalo, L.; Gallego-Alberto, L.; Pedroso-Chaparro, M.D.S.; Fernandes-Pires, J.; Márquez-González, M. “We’re staying at home.” Association of self-perceptions of aging, personal and family resources and loneliness with psychological distress during the lock-down period of COVID-19. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 76, 10–16. [Google Scholar] [CrossRef] [Green Version]
- WHO Mental Health Action Plan 2013–2020. Available online: www.who.int/publications/i/item/9789241506021 (accessed on 25 July 2021).
- García-Fernández, L.; Romero-Ferreiro, V.; López-Roldán, P.D.; Padilla, S.; Rodriguez-Jimenez, R. Mental Health in Elderly Spanish People in Times of COVID-19 Outbreak. Am. J. Geriatr. Psychiatry 2020, 28, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Fancourt, D.; Steptoe, A.; Bu, F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: A longitudinal observational study. Lancet Psychiatry 2021, 8, 141–149. [Google Scholar] [CrossRef]
- Sundström, G.; Fransson, E.; Malmberg, B.; Davey, A. Loneliness among older Europeans. Eur. J. Aging 2009, 6, 267. [Google Scholar] [CrossRef] [PubMed]
- Röhr, S.; Reininghaus, U.; Riedel-Heller, S.G. Mental wellbeing in the German old age population largely unaltered during COVID-19 lockdown: Results of a representative survey. BMC Geriatr. 2020, 20, 489. [Google Scholar] [CrossRef]
- Shevlin, M.; McBride, O.; Murphy, J.; Miller, J.G.; Hartman, T.K.; Levita, L.; Mason, L.; Martinez, A.P.; McKay, S.T.V.A. Anxiety, depression, traumatic stress, and COVID-19 related anxiety in the UK general population during the COVID-19 pandemic. BJPsych Open 2020, 6, e125. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; Abel, K.M. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Sonderskov, K.M.; Dinesen, P.T.; Santini, Z.I.; Ostergaard, S.D. The depressive state of Denmark during the COVID-19 pandemic. Acta Neuropsychiatr. 2020, 32, 226–228. [Google Scholar] [CrossRef] [Green Version]
- González-Sanguino, C.; Ausín, B.; Castellanos M, Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef]
- Ozamiz-Etxebarria, N.; Dosil-Santamaria, M.; Picaza-Gorrochategui, M.; Idoiaga-Mondragon, N. Stress, anxiety, and depression levels in the initial stage of the COVID-19 outbreak in a population sample in the northern Spain. Cad. Saude Publica 2020, 36, e00054020. [Google Scholar] [CrossRef]
- Vahia, I.V.; Blazer, D.G.; Smith, G.S.; Karp, J.F.; Steffens, D.C.; Forester, B.P.; Tampi, R.; Agronin, M.; Jeste, D.V.; Reynolds, C.F., III; et al. COVID-19, mental health and aging: A need for new knowledge to bridge science and service. Am. J. Geriatr. Psychiatry 2020, 28, 695–697. [Google Scholar] [CrossRef]
- Jahanshahi, A.A.; Dinani, M.M.; Madavani, A.N.; Li, J.; Zhang, S.X. The distress of Iranian adults during the COVID-19 pandemic—More distressed than the Chinese and with different predictors. Brain Behav. Immun. 2020, 87, 124–125. [Google Scholar] [CrossRef]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. 2017. Available online: https://apps.who.int/iris/handle/10665/254610 (accessed on 25 July 2021).
- Gambin, M.; Sękowski, M.; Woźniak-Prus, M.; Cudo, H.K.; Gorgol, J.K.; Huflejt-Łukasik, M.; Kmita, G.; Kubicka, K.; Łyś, A.E.; Maison, D.; et al. Determinants of Depression and Generalized Anxiety Symptoms in Adult Poles during the Covid-19 Epidemic—Report from the First Wave of a Longitudinal Study. Available online: http://psych.uw.edu.pl/wpcontent/uploads/sites/98/2020/05/Uwarunkowania_objawow_depresji_leku_w_trakcie_pandemii_raport.pdf2020 (accessed on 26 April 2021).
- Lee, H.S.; Dean, D.; Baxter, T.; Griffith, T.; Park, S. Deterioration of mental health despite successful control of the COVID-19 pandemic in South Korea. Psychiatry Res. 2021, 295, 113570. [Google Scholar] [CrossRef] [PubMed]
- Tobiasz-Adamczyk, B.; Zawisza, K. Urban-rural differences in social capital in relation to self-rated health and subjective well-being in older residents of six regions in Poland. Ann. Agric. Environ. Med. 2017, 24, 162–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahid, Z.; Kalayanamitra, R.; McClafferty, B.; Kepko, D.; Ramgobin, D.; Patel, R.; Aggarwal, C.S.; Vunnam, R.; Sahu, N.; Bhatt, D.; et al. COVID-19 and older adults: What we know. J. Am. Geriatr. 2020, 68, 926–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q. Prevalence of comorbidities and its effects in coronavirus disease 2019 patients: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does comorbidity increase the risk of patients with COVID-19: Evidence from meta-analysis. Aging 2020, 12, 6049–6057. [Google Scholar] [CrossRef] [PubMed]
- Yanguas, J.; Pinazo-Henandis, S.; Tarazona-Santabalbina, F.J. The complexity of loneliness. Acta Biomed. 2018, 89, 302–314. [Google Scholar] [CrossRef] [PubMed]
- Özdin, S.; Özdin, S.B. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–551. [Google Scholar] [CrossRef]
- Feter, N.; Caputo, E.L.; Doring, I.R.; Leite, J.S.; Cassuriaga, J.; Reichert, F.F.; da Silva, M.C.; Coombes, J.S.; Rombaldi, A.J. Sharp increase in depression and anxiety among Brazilian adults during the COVID-19 pandemic: Findings from the PAMPA cohort. Public Health 2021, 190, 101–107. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | M | Median | Min. | Max. | SD | |
|---|---|---|---|---|---|---|
| HADS-M | Anxiety | 7.90 | 7.00 | 0.0 | 21.0 | 4.76 |
| Depression | 5.47 | 5.00 | 0.0 | 20.0 | 4.28 | |
| Depression + Irritability | 8.14 | 7.50 | 0.0 | 26.0 | 5.36 | |
| Total score | 16.0 | 15.00 | 0.0 | 47.0 | 9.66 |
| Variable | M | Median | Min. | Max. | SD | |
|---|---|---|---|---|---|---|
| R-UCLA | Belonging and affiliation | 9.46 | 9.00 | 5.00 | 19.00 | 2.86 |
| Intimate others | 22.48 | 22.00 | 10.00 | 40.00 | 6.93 | |
| Social others | 8.34 | 8.00 | 5.00 | 20.00 | 3.05 | |
| Total score | 40.29 | 39.00 | 20.00 | 69.00 | 10.82 |
| HADS-M | R-UCLA | |||
|---|---|---|---|---|
| Intimate Others | Social Others | Belonging and Affiliation | Total Score | |
| Anxiety | r = 0.46 | r = 0.38 | r = 0.35 | r = 0.49 |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | |
| Depression | r = 0.48 | r = 0.47 | r = 0.42 | r = 0.55 |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | |
| Depression + irritability | r = 0.49 | r = 0.45 | r = 0.39 | r = 0.54 |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | |
| Total HADS-M score | r = 0.50 | r = 0.44 | r = 0.39 | r = 0.55 |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | |
| Parameter | % of All Subjects | HADS-M | R-UCLA | ||||
|---|---|---|---|---|---|---|---|
| M | SD | t/H/r | M | SD | t/H/r | ||
| Age | 100.00 | 16.5 | 9.66 | p < 0.001 r = −0.17 | 40.29 | 10.82 | p = 0.004 r = −0.13 |
| Marital status | |||||||
| In a relationship | 70.3 | 10.64 | 9.50 | p = 0.259 t = 1.11 | 39.05 | 10.24 | p < 0.001 t = 3.28 |
| Single | 29.7 | 16.76 | 9.79 | 42.90 | 11.62 | ||
| Education | |||||||
| Primary/vocational/lower secondary | 30.2 | 18.92 | 11.50 | H = 6.95 p = 0.073 | 41.38 | 10.77 | H = 1.24 p = 0.742 |
| Secondary/post-secondary | 52.8 | 15.43 | 9.74 | 40.64 | 11.11 | ||
| Higher | 17.0 | 15.06 | 15.06 | 38.96 | 9.94 | ||
| Employment status | |||||||
| Old-age pensioner/incapacitated pensioner | 25.3 | 14.12 | 10.32 | H = 7.36 p = 0.061 | 39.70 | 10.50 | H = 3.56 p = 0.312 |
| Unemployed | 16.3 | 16.41 | 9.00 | 39.00 | 9.89 | ||
| Employed | 48.0 | 16.41 | 9.63 | 40.44 | 11.40 | ||
| Students | 10.4 | 17.18 | 9.60 | 43.25 | 10.85 | ||
| Place of residence | |||||||
| Rural area | 38.0 | 16.42 | 9.67 | r = 0.050 p = 0.279 | 39.41 | 9.99 | r = 0.035 p = 0.445 |
| City of up to 20,000 inhabitants | 10.0 | 18.22 | 10.90 | 41.12 | 11.69 | ||
| City of 21,000–50,000 inhabitants | 13.5 | 14.25 | 9.28 | 39.01 | 9.94 | ||
| City of 51,000–100,000 inhabitants | 9.2 | 15.26 | 9.82 | 39.93 | 11.07 | ||
| City of 101,000–200,000 inhabitants | 9.0 | 15.76 | 9.33 | 39.66 | 10.89 | ||
| City of 201,000–500,000 inhabitants | 8.3 | 14.93 | 10.68 | 41.12 | 13.26 | ||
| City of over 500,000 inhabitants | 12.0 | 16.06 | 8.79 | 42.51 | 11.85 | ||
| Person with whom one currently resides | |||||||
| Alone | 10.6 | 13.74 | 10.66 | H = 7.95 p = 0.018 | 42.06 | 12.12 | H = 1.40 p = 0.494 |
| With spouse/partner only | 25.8 | 15.01 | 9.89 | 39.56 | 10.27 | ||
| With family (children, relatives) | 63.6 | 16.84 | 9.30 | 40.05 | 10.67 | ||
| Financial situation rating | |||||||
| Very good | 3.7 | 14.47 | 10.45 | r = −0.280 p < 0.001 | 34.94 | 11.87 | r = −0.194 p < 0.001 |
| Quite good | 34.4 | 13.57 | 8.74 | 38.80 | 10.42 | ||
| Neither good nor poor | 41.5 | 15.49 | 8.75 | 40.20 | 10.55 | ||
| Quite poor | 14.3 | 20.07 | 10.53 | 42.43 | 10.61 | ||
| Very poor | 6.1 | 27.58 | 8.53 | 48.95 | 11.00 | ||
| Pair of Variables | Spearman Rank Correlation Test | |||
|---|---|---|---|---|
| Self-Rating of Health Status before the Pandemic | Self-Rating of Change in Health during the Pandemic | |||
| R Spearman | p | R Spearman | p | |
| Physical health and anxiety | 0.29 | 0.000 | 0.12 | 0.012 |
| Physical health and depression | 0.32 | 0.000 | 0.11 | 0.015 |
| Physical health and depression + irritability | 0.30 | 0.000 | 0.12 | 0.013 |
| Physical health and total HADS-M score | 0.31 | 0.000 | 0.12 | 0.011 |
| Physical health and intimate others | 0.20 | 0.000 | 0.12 | 0.008 |
| Physical health and social others | 0.20 | 0.000 | 0.05 | 0.295 |
| Physical health and belonging and affiliation | 0.20 | 0.000 | 0.09 | 0.065 |
| Physical health and total score | 0.23 | 0.000 | 0.10 | 0.031 |
| Mental health and anxiety | 0.55 | 0.000 | 0.36 | 0.000 |
| Mental health and depression | 0.56 | 0.000 | 0.32 | 0.000 |
| Mental health and depression + irritability | 0.56 | 0.000 | 0.30 | 0.000 |
| Mental health and total HADS-M score | 0.58 | 0.000 | 0.34 | 0.000 |
| Mental health and intimate others | 0.37 | 0.000 | 0.15 | 0.000 |
| Mental health and social others | 0.32 | 0.000 | 0.15 | 0.000 |
| Mental health and belonging and affiliation | 0.32 | 0.000 | 0.20 | 0.000 |
| Mental health and total score | 0.39 | 0.000 | 0.18 | 0.001 |
| Parameter | % Yes | HADS-M | R-UCLA | ||||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | Z | p | M | SD | Z | p | ||
| Cardiovascular diseases | 2.7 | 16.32 | 11.03 | 0.151 | 0.879 | 40.25 | 11.53 | 0.220 | 0.825 |
| Respiratory diseases | 10.5 | 19.67 | 11.17 | 2.153 | 0.024 | 41.81 | 11.25 | 0.890 | 0.373 |
| Endocrine diseases | 24.0 | 17.08 | 10.43 | 0.745 | 0.456 | 42.51 | 11.20 | 2.043 | 0.041 |
| Cancer | 3.4 | 17.53 | 11.17 | 0.551 | 0.581 | 40.33 | 10.32 | 0.082 | 0.934 |
| Kidney disease | 3.9 | 19.23 | 9.58 | 1.486 | 0.137 | 43.58 | 10.45 | 1.295 | 0.194 |
| Mental disorders | 5.8 | 27.00 | 9.75 | 5.099 | 0.000 | 48.76 | 10.82 | 3.685 | 0.001 |
| None of the above | 49.7 | 17.31 | 10.25 | 2.263 | 0.023 | 41.27 | 10.91 | 1.837 | 0.066 |
| Variables | M Yes | M No | SD | t | p |
|---|---|---|---|---|---|
| Anxiety | 7.99 | 7.84 | 4.87 | 0.28 | 0.774 |
| Depression | 5.27 | 5.50 | 4.08 | 0.49 | 0.624 |
| Depression + irritability | 8.12 | 8.11 | 5.37 | 0.01 | 0.991 |
| Total HADS m score | 16.10 | 15.95 | 9.77 | 0.14 | 0.883 |
| Intimate others | 21.64 | 22.54 | 6.34 | 1.21 | 0.224 |
| Social others | 7.88 | 8.54 | 2.82 | 2.02 | 0.043 |
| Belonging and affiliation | 8.82 | 9.72 | 2.91 | 2.88 | 0.004 |
| Total R-UCLA score | 38.34 | 40.81 | 10.61 | 2.08 | 0.037 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Idzik, A.; Leńczuk-Gruba, A.; Kobos, E.; Pietrzak, M.; Dziedzic, B. Loneliness and Depression among Women in Poland during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10698. https://doi.org/10.3390/ijerph182010698
Idzik A, Leńczuk-Gruba A, Kobos E, Pietrzak M, Dziedzic B. Loneliness and Depression among Women in Poland during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(20):10698. https://doi.org/10.3390/ijerph182010698
Chicago/Turabian StyleIdzik(199), Anna, Anna Leńczuk-Gruba, Ewa Kobos, Mariola Pietrzak, and Beata Dziedzic. 2021. "Loneliness and Depression among Women in Poland during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 20: 10698. https://doi.org/10.3390/ijerph182010698