
The Role of Physical Activity-Related Health Competence and Leisure-Time Physical Activity for Physical Health and Metabolic Syndrome: A Structural Equation Modeling Approach for German Office Workers


Abstract
:1. Introduction
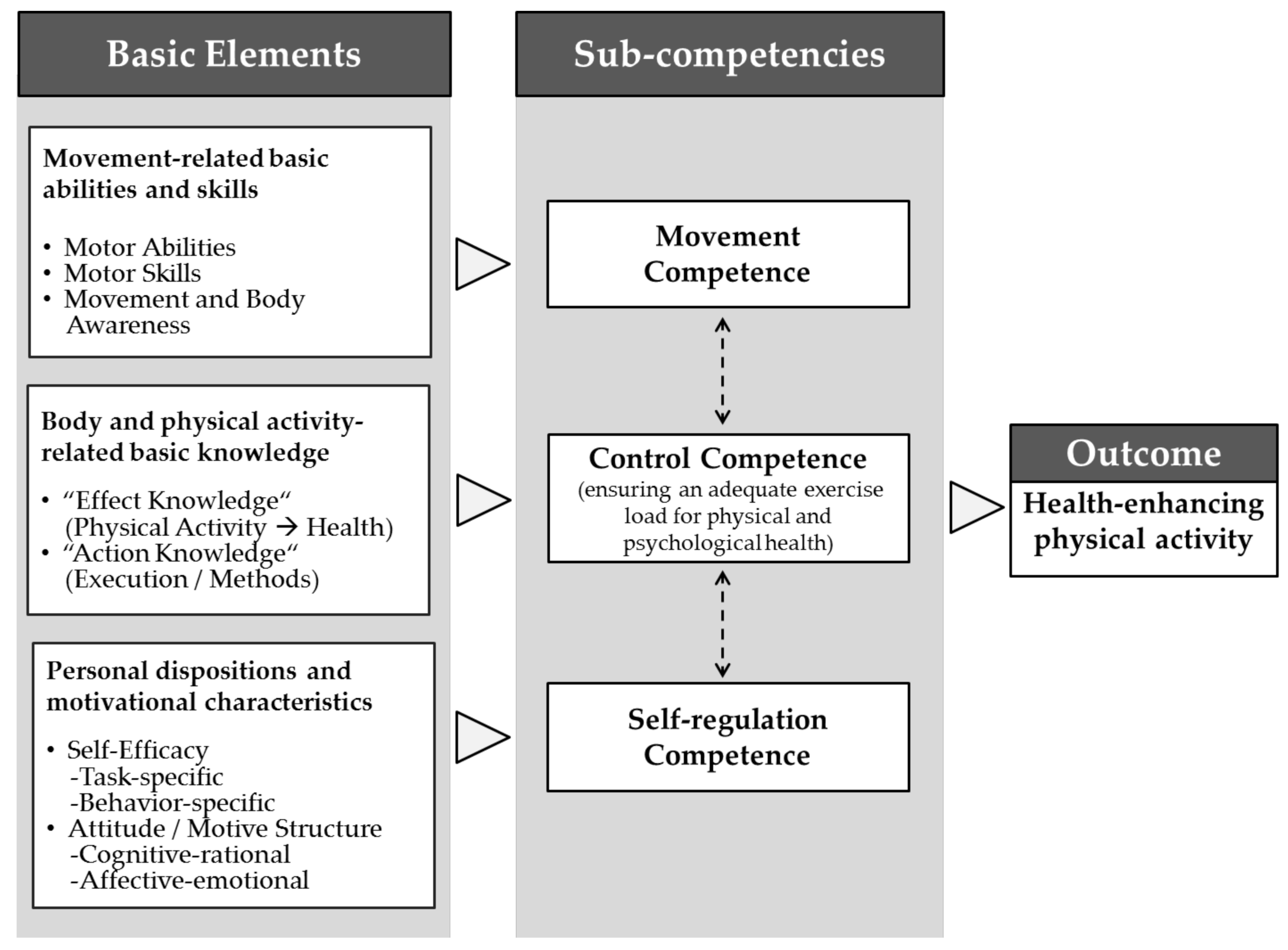
1.1. Introducing Physical Activity-Related Health Competence
1.2. Current Research on the Role of PAHCO in PA and Health
1.3. Research Goals and Hypotheses
- PAHCO has a direct positive relationship with leisure-time PA in OWs.
- PAHCO has a direct positive relationship with physical and metabolic health in OWs.
- PAHCO has an indirect relationship with physical and metabolic health mediated by leisure-time PA in OWs.
2. Methods
2.1. Participants
2.2. Materials
2.2.1. Self-Report Measures
- (1)
- The Questionnaire on the PAHCO model developed by Sudeck and Pfeifer [36] contains the three subscales of control competence for physical training, PA-specific affect regulation, and PA-specific self-regulation with a total of 13 items and responses on a 4-point Likert scale. Control competence for physical training (e.g., “If I want to enhance my health by strengthening my trunk muscles (back, stomach), I am confident that I know the right exercises to do”) consists of six items (Cronbach’s α = 0.87). PA-specific affect regulation (e.g., “If I am feeling down, I can distract myself well through physical activity”) is assessed with four items (Cronbach’s α = 0.88). PA-specific self-regulation (e.g., “When I decide to do more exercise, I am very disciplined in implementing this plan.”) comprises three items (Cronbach’s α = 0.84). The PAHCO questionnaire comprises mean scores on the three subscales and a total mean score of all 13 items ranging from 1 to 4. Higher mean scores resemble better PAHCO for the total mean value and the subscales (Cronbach’s α = 0.88).The subcompetence of movement competence is not part of the questionnaire because, at the time of data collection, no scale on PAHCO existed that included movement competence [39]. The absence of movement competence in this measure of PAHCO may also be due to the difficulty of universally valid assessment tools for motor competence measured across different populations [48].
- (2)
- Participants completed the work dimension of the Baecke Physical Activity Questionnaire [49] with eight items (e.g., “What is your main occupation?”) to strictly include OWs in this study and assess the sample’s PA level during work. The questionnaire examines occupational PA with a weighted mean score ranging from 1 to 5, with low values indicating low occupational PA.
- (3)
- The Godin–Shepard Leisure-Time Physical Activity Questionnaire (GSLTPAQ) [50] has six items that determine individuals’ PA during leisure time at mild, moderate, and vigorous intensity (e.g., “Over the last 7 days (i.e., the last week), how many times on average did you do the following kinds of exercise for more than 30 min during your free time?”). The GSLTPAQ results in the cumulative weighted leisure score index, which displays the amount of leisure-time PA, with values >24 indicating sufficient leisure-time PA [51].
- (4)
- Physical and mental health was operationalized by the Short-Form Health Survey (SF-12) version 2.0 [47,52], which examines self-reported health with a weighted and standardized component score on physical (Cronbach’s α = 0.79) and mental (Cronbach’s α = 0.86) dimensions, with six items each. The mental component score and the physical component score range from 0–100, with a mean of 50 and a standard deviation of 10. High values indicate better self-reported health.
2.2.2. Objective Measures
2.3. Procedures
2.4. Data Analysis
3. Results
3.1. Bivariate Correlations and Multivariate Linear Regressions
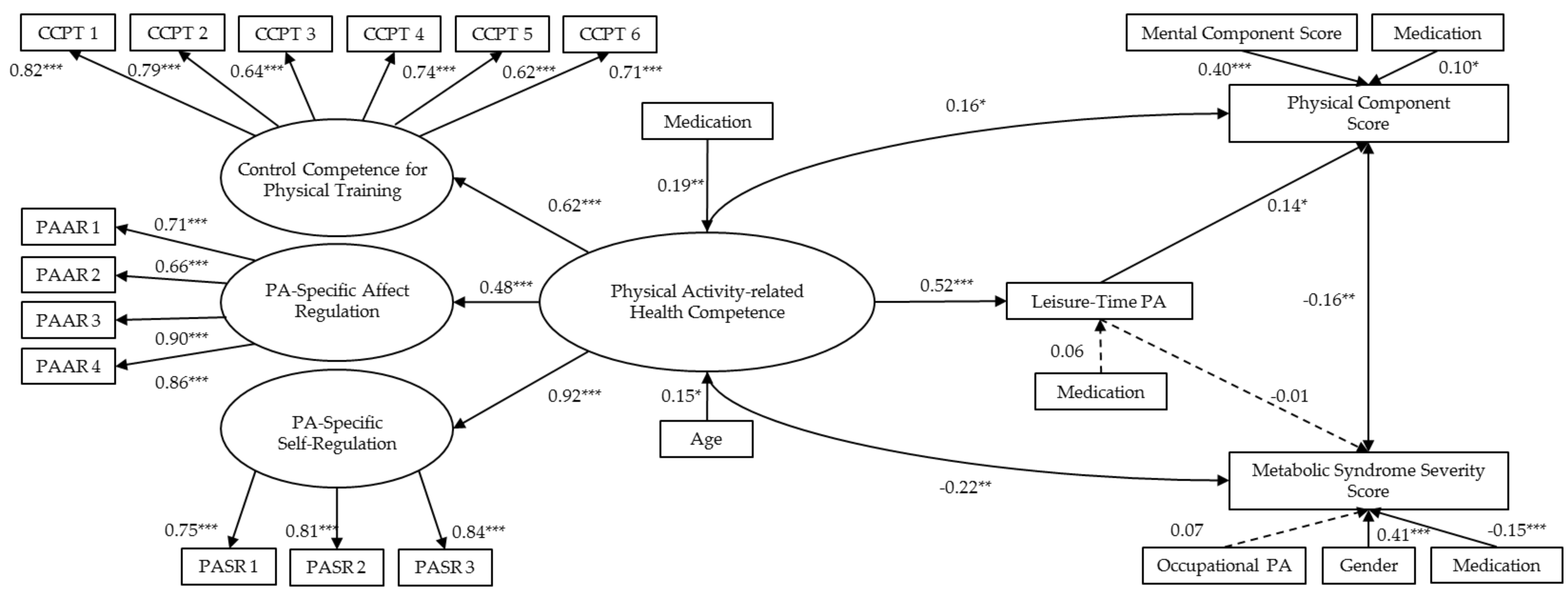
3.2. SEM of the Second-Order PAHCO Factor
4. Discussion
4.1. Direct Relationship between PAHCO and Leisure-Time PA
4.2. Direct Relationship between PAHCO and Physical and Metabolic Health
4.3. Mediating Role of Leisure-Time PA on the Relationship between PAHCO and Physical and Metabolic Health
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| PAHCO | Leisure-Time PA | Physical Component Score | MetSSS | ||
|---|---|---|---|---|---|
| Intercept | β | −0.71 | −0.17 | −1.08 | −0.39 |
| 95% CI | (−0.78, 0.63) | (−0.88, 0.54) | (−0.80, 0.59) | (−1.02, 0.25) | |
| Gender (ref. = female) | |||||
| Male | β | −0.09 | 0.05 | 0.16 | 1.02 *** |
| 95% CI | (−0.36, 0.18) | (−0.21, 0.32) | (−0.10, 0.43) | (0.78, 1.26) | |
| Age | β | 0.13 * | 0.02 | −0.00 | −0.05 |
| 95% CI | (0.02, 0.25) | (−0.10, 0.13) | (−0.12, 0.11) | (−0.15, 0.05) | |
| Relationship status (ref. = relationship) | |||||
| No relationship | β | 0.22 | 0.08 | −0.08 | 0.18 |
| 95% CI | (−0.06, 0.51) | (−0.21, 0.37) | (−0.36, 0.20) | (−0.07, 0.44) | |
| Education (ref. = primary) | |||||
| Secondary | β | −0.07 | −0.12 | −0.35 | −0.13 |
| 95% CI | (−0.79, 0.65) | (−0.84, 0.61) | (−1.06, 0.36) | (−0.78, 0.53) | |
| Tertiary | β | −0.02 | 0.01 | −1.0 | −0.28 |
| 95% CI | (−0.73, 0.69) | (−0.70, 0.73) | (−0.80, 0.60) | (−0.93, 0.36) | |
| Medication intake (ref. = Medication) | |||||
| No medication | β | 0.29 * | 0.32 ** | 0.40 *** | −0.42 *** |
| 95% CI | (0.06, 0.51) | (0.09, 0.54) | (0.18, 0.62) | (−0.63, 0.22) |
Appendix B

References
- Finlay, B.B. Are noncommunicable diseases communicable? Science 2020, 367, 250–251. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, J. Modelling and prediction of global non-communicable diseases. BMC Public Health 2020, 20, 822. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Model. Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Simmons, R.K.; Alberti, K.G.M.M.; Gale, E.A.M.; Colagiuri, S.; Tuomilehto, J.; Qiao, Q.; Ramachandran, A.; Tajima, N.; Brajkovich Mirchov, I.; Ben-Nakhi, A.; et al. The metabolic syndrome: Useful concept or clinical tool? Report of a WHO Expert Consultation. Diabetology 2010, 53, 600–605. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Janssen, I.; Bredin, S.S.D.; Warburton, D.E.R.; Bauman, A. Physical activity: Health impact, prevalence, correlates and interventions. Psychol. Health 2017, 32, 942–975. [Google Scholar] [CrossRef]
- Cerletti, P.; Keidel, D.; Imboden, M.; Schindler, C.; Probst-Hensch, N. The modifying role of physical activity in the cross-sectional and longitudinal association of health-related quality of life with physiological functioning-based latent classes and metabolic syndrome. Health Qual. Life Outcomes 2020, 18, 345. [Google Scholar] [CrossRef]
- Breda, J.; Jakovljevic, J.; Rathmes, G.; Mendes, R.; Fontaine, O.; Hollmann, S.; Rütten, A.; Gelius, P.; Kahlmeier, S.; Galea, G. Promoting health-enhancing physical activity in Europe: Current state of surveillance, policy development and implementation. Health Policy 2018, 122, 519–527. [Google Scholar] [CrossRef]
- Reiner, M.; Niermann, C.; Jekauc, D.; Woll, A. Long-term health benefits of physical activity—A systematic review of longitudinal studies. BMC Public Health 2013, 13, 813. [Google Scholar] [CrossRef] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1,9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Wallmann-Sperlich, B.; Froboese, I. Physical activity during work, transport and leisure in Germany—Prevalence and socio-demographic correlates. PLoS ONE 2014, 9, e112333. [Google Scholar] [CrossRef]
- Finger, J.D.; Mensink, G.; Lange, C.; Manz, K. Health-enhancing physical activity during leisure time among adults in Germany. J. Health Monit. 2017, 35–42. [Google Scholar] [CrossRef]
- Olson, M.H. Remote office work: Changing work patterns in space and time. Commun. ACM 1983, 26, 182–187. [Google Scholar] [CrossRef]
- Backé, E.M.; Kreis, L.; Latza, U. Interventionen am Arbeitsplatz, die zur Veränderung des Sitzverhaltens anregen. Zbl. Arbeitsmed. 2019, 69, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Prince, S.A.; Elliott, C.G.; Scott, K.; Visintini, S.; Reed, J.L. Device-measured physical activity, sedentary behaviour and cardiometabolic health and fitness across occupational groups: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 30. [Google Scholar] [CrossRef]
- Strauss, M.; Foshag, P.; Przybylek, B.; Horlitz, M.; Lucia, A.; Sanchis-Gomar, F.; Leischik, R. Occupation and metabolic syndrome: Is there correlation? A cross sectional study in different work activity occupations of German firefighters and office workers. Diabetol. Metab. Syndr. 2016, 8, 57. [Google Scholar] [CrossRef] [Green Version]
- Hoe, V.C.W.; Urquhart, D.M.; Kelsall, H.L.; Zamri, E.N.; Sim, M.R. Ergonomic interventions for preventing work-related musculoskeletal disorders of the upper limb and neck among office workers. Cochrane Database Syst. Rev. 2018, 2018, Cd008570. [Google Scholar] [CrossRef]
- Collins, K.H.; Herzog, W.; MacDonald, G.Z.; Reimer, R.A.; Rios, J.L.; Smith, I.C.; Zernicke, R.F.; Hart, D.A. Obesity, Metabolic Syndrome, and Musculoskeletal Disease: Common Inflammatory Pathways Suggest a Central Role for Loss of Muscle Integrity. Front. Physiol. 2018, 9, 112. [Google Scholar] [CrossRef]
- Holzgreve, F.; Maltry, L.; Hänel, J.; Schmidt, H.; Bader, A.; Frei, M.; Filmann, N.; Groneberg, D.A.; Ohlendorf, D.; van Mark, A. The Office Work and Stretch Training (OST) Study: An Individualized and Standardized Approach to Improve the Quality of Life in Office Workers. Int. J. Environ. Res. Public Health 2020, 17, 4522. [Google Scholar] [CrossRef]
- Ryu, H.; Jung, J.; Cho, J.; Chin, D.L. Program development and effectiveness of workplace health promotion program for preventing metabolic syndrome among office workers. Int. J. Environ. Res. Public Health 2017, 14, 878. [Google Scholar] [CrossRef] [Green Version]
- Strauss, M.; Foshag, P.; Leischik, R. Prospective Evaluation of Cardiovascular, Cardiorespiratory, and Metabolic Risk of German Office Workers in Comparison to International Data. Int. J. Environ. Res. Public Health 2020, 17, 1590. [Google Scholar] [CrossRef] [Green Version]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Jirathananuwat, A.; Pongpirul, K. Promoting physical activity in the workplace: A systematic meta-review. J. Occup. Health 2017, 59, 385–393. [Google Scholar] [CrossRef]
- Holtermann, A.; Hansen, J.V.; Burr, H.; Søgaard, K.; Sjøgaard, G. The health paradox of occupational and leisure-time physical activity. Br. J. Sports Med. 2012, 46, 291–295. [Google Scholar] [CrossRef] [Green Version]
- Holtermann, A.; Krause, N.; van der Beek, A.J.; Straker, L. The physical activity paradox: Six reasons why occupational physical activity (OPA) does not confer the cardiovascular health benefits that leisure time physical activity does. Br. J. Sports Med. 2018, 52, 149–150. [Google Scholar] [CrossRef] [Green Version]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Rhodes, R.; McEwan, D.; Rebar, A. Theories of physical activity behaviour change: A history and synthesis of approaches. Psychol. Sport Exerc. 2019, 42, 100–109. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Whitehead, M. Physical Literacy: Philosophical Considerations in Relation to Developing a Sense of Self, Universality and Propositional Knowledge. Sport Ethics Philos. 2007, 1, 281–298. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.S.; Wallston, K.A.; Smith, C.A. The development and validation of the Perceived Health Competence Scale. Health Educ. Res. 1995, 10, 51–64. [Google Scholar] [CrossRef]
- Carl, J.; Sudeck, G.; Pfeifer, K. Competencies for a Healthy Physically Active Lifestyle-Reflections on the Model of Physical Activity-Related Health Competence. J. Phys. Act. Health 2020, 17, 688–697. [Google Scholar] [CrossRef]
- Cairney, J.; Dudley, D.; Kwan, M.; Bulten, R.; Kriellaars, D. Physical Literacy, Physical Activity and Health: Toward an Evidence-Informed Conceptual Model. Sports Med. 2019, 49, 371–383. [Google Scholar] [CrossRef]
- Haible, S.; Volk, C.; Demetriou, Y.; Höner, O.; Thiel, A.; Sudeck, G. Physical Activity-Related Health Competence, Physical Activity, and Physical Fitness: Analysis of Control Competence for the Self-Directed Exercise of Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 39. [Google Scholar] [CrossRef] [Green Version]
- Sudeck, G.; Pfeifer, K. Physical activity-related health competence as an integrative objective in exercise therapy and health sports—Conception and validation of a short questionnaire. Sportwissenschaft 2016, 46, 74–87. [Google Scholar] [CrossRef]
- Carl, J.; Sudeck, G.; Pfeifer, K. Competencies for a Healthy Physically Active Lifestyle: Second-Order Analysis and Multidimensional Scaling. Front. Psychol. 2020, 11, 3267. [Google Scholar] [CrossRef]
- Sudeck, G.; Jeckel, S.; Schubert, T. Individual Differences in the Competence for Physical-Activity-Related Affect Regulation Moderate the Activity-Affect Association in Real-Life Situations. J. Sport. Exerc. Psychol. 2018, 40, 196–205. [Google Scholar] [CrossRef]
- Carl, J.; Sudeck, G.; Geidl, W.; Schultz, K.; Pfeifer, K. Competencies for a Healthy Physically Active Lifestyle-Validation of an Integrative Model. Res. Q. Exerc. Sport 2021, 92, 514–528. [Google Scholar] [CrossRef]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef]
- Carl, J.; Grüne, E.; Popp, J.; Pfeifer, K. Physical Activity Promotion for Apprentices in Nursing Care and Automotive Mechatronics–Competence Counts More than Volume. Int. J. Environ. Res. Public Health 2020, 17, 793. [Google Scholar] [CrossRef] [Green Version]
- Schmid, J.; Haible, S.; Sudeck, G. Patterns of physical activity-related health competence: Stability over time and associations with subjective health indicators. Ger. J. Exerc. Sport Res. 2020, 50, 218–228. [Google Scholar] [CrossRef] [Green Version]
- Warburton, D.E.; Bredin, S.S. Reflections on Physical Activity and Health: What Should We Recommend? Can. J. Cardiol. 2016, 32, 495–504. [Google Scholar] [CrossRef] [Green Version]
- Thivel, D.; Tremblay, A.; Genin, P.M.; Panahi, S.; Rivière, D.; Duclos, M. Physical Activity, Inactivity, and Sedentary Behaviors: Definitions and Implications in Occupational Health. Front. Public Health 2018, 6, 288. [Google Scholar] [CrossRef]
- Wagner, P.; Singer, R. Ein Fragebogen zur Erfassung der habituellen körperlichen Aktivität verschiedener Bevölkerungsgruppen. Sportwissenschaft 2003, 33, 383–397. [Google Scholar]
- Fleig, L.; Lippke, S.; Pomp, S.; Schwarzer, R. Intervention effects of exercise self-regulation on physical exercise and eating fruits and vegetables: A longitudinal study in orthopedic and cardiac rehabilitation. Prev. Med. 2011, 53, 182–187. [Google Scholar] [CrossRef]
- Wirtz, M.A.; Morfeld, M.; Glaesmer, H.; Brähler, E. Konfirmatorische Prüfung der Skalenstruktur des SF-12 Version 2.0 in einer deutschen bevölkerungs-repräsentativen Stichprobe. Diagnostica 2017, 64, 84–96. [Google Scholar] [CrossRef]
- Sigmundsson, H.; Lorås, H.; Haga, M. Assessment of Motor Competence Across the Life Span: Aspects of Reliability and Validity of a New Test Battery. SAGE Open 2016, 6. [Google Scholar] [CrossRef] [Green Version]
- Baecke, J.A.; Burema, J.; Frijters, J.E. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am. J. Clin. Nutr. 1982, 36, 936–942. [Google Scholar] [CrossRef]
- Godin, G.; Shephard, R.J. A simple method to assess exercise behavior in the community. Can. J. Appl. Sport Sci. 1985, 10, 141–146. [Google Scholar]
- Amireault, S.; Godin, G. The Godin-Shephard Leisure-Time Physical Activity Questionnaire: Validity Evidence Supporting its Use for Classifying Healthy Adults into Active and Insufficiently Active Categories. Percept. Mot. Skills. 2015, 120, 604–622. [Google Scholar] [CrossRef]
- Ware, J.; Ma, K.; Tuner-Bowker, D.; Gandek, B. How to Score Version 2 of the SF-12 Health Survey (With a Supplement Documenting Version 1); QualityMetric Incorporated: Lincoln, NE, USA, 2002. [Google Scholar]
- Grundy, S.M.; Cleeman, J.I.; Merz, C.N.B.; Brewer, H.B.; Clark, L.T.; Hunninghake, D.B.; Pasternak, R.C.; Smith, S.C.; Stone, N.J. Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. Circulation 2004, 110, 227–239. [Google Scholar]
- Gurka, M.J.; Lilly, C.L.; Oliver, M.N.; DeBoer, M.D. An examination of sex and racial/ethnic differences in the metabolic syndrome among adults: A confirmatory factor analysis and a resulting continuous severity score. Metabolism 2014, 63, 218–225. [Google Scholar] [CrossRef] [Green Version]
- DeBoer, M.D.; Gurka, M.J. Clinical utility of metabolic syndrome severity scores: Considerations for practitioners. Diabetes Metab. Syndr. Obes. 2017, 10, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Luthra, R.R. Explaining Ethnic Inequality in the German Labor Market: Labor Market Institutions, Context of Reception, and Boundaries. Eur. Sociol. Rev. 2013, 29, 1095–1107. [Google Scholar] [CrossRef] [Green Version]
- Buuren, S.V. Flexible Imputation of Missing Data; CRC Press: Boca Raton, FL, USA, 2018. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; Pearson Education: Boston, MA, USA, 2013. [Google Scholar]
- Ernst, A.F.; Albers, C.J. Regression assumptions in clinical psychology research practice—A systematic review of common misconceptions. Peer J. 2017, 5, e3323. [Google Scholar] [CrossRef] [Green Version]
- VanderWeele, T.J.; Mathur, M.B. Some Desirable Properties of the Bonferroni Correction: Is the Bonferroni Correction Really so Bad? Am. J. Epidemiol. 2018, 188, 617–618. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Team R Core. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Abula, K.; Gröpel, P.; Chen, K.; Beckmann, J. Does knowledge of physical activity recommendations increase physical activity among Chinese college students? Empirical investigations based on the transtheoretical model. J. Sport Health Sci. 2018, 7, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Prochaska, J.O.; DiClemente, C.C. Stages and processes of self-change of smoking: Toward an integrative model of change. J. Consult. Clin. Psychol. 1983, 51, 390–395. [Google Scholar] [CrossRef]
- Young, M.D.; Plotnikoff, R.C.; Collins, C.E.; Callister, R.; Morgan, P.J. Social cognitive theory and physical activity: A systematic review and meta-analysis. Obes. Rev. 2014, 15, 983–995. [Google Scholar] [CrossRef]
- Svendsen, M.T.; Bak, C.K.; Sørensen, K.; Pelikan, J.; Riddersholm, S.J.; Skals, R.K.; Mortensen, R.N.; Maindal, H.T.; Bøggild, H.; Nielsen, G.; et al. Associations of health literacy with socioeconomic position, health risk behavior, and health status: A large national population-based survey among Danish adults. BMC Public Health 2020, 20, 565. [Google Scholar] [CrossRef]
- Edwards, L.C.; Bryant, A.S.; Keegan, R.J.; Morgan, K.; Jones, A.M. Definitions, Foundations and Associations of Physical Literacy: A Systematic Review. Sports Med. 2017, 47, 113–126. [Google Scholar] [CrossRef] [Green Version]
- Schreuder, K.J.; Roelen, C.A.; Koopmans, P.C.; Groothoff, J.W. Job demands and health complaints in white and blue collar workers. Work 2008, 31, 425–432. [Google Scholar]
- Brandt, M.; Sundstrup, E.; Andersen, L.L.; Wilstrup, N.M.; Ajslev, J.Z.N. Safety climate as a predictor of work ability problems in blue-collar workers: Prospective cohort study. BMJ Open 2021, 11, e040885. [Google Scholar] [CrossRef]
- Besharati, A.; Daneshmandi, H.; Zareh, K.; Fakherpour, A.; Zoaktafi, M. Work-related musculoskeletal problems and associated factors among office workers. Int. J. Occup. Saf. Ergon. 2020, 26, 632–638. [Google Scholar] [CrossRef]
- Enwald, H.; Hirvonen, N.; Huotari, M.-L.; Korpelainen, R.; Pyky, R.; Savolainen, M.; Salonurmi, T.; Keränen, A.-M.; Jokelainen, T.; Niemelä, R. Everyday health information literacy among young men compared with adults with high risk for metabolic syndrome—A cross-sectional population-based study. J. Inf. Sci. 2016, 42, 344–355. [Google Scholar] [CrossRef]
- Yokokawa, H.; Fukuda, H.; Yuasa, M.; Sanada, H.; Hisaoka, T.; Naito, T. Association between health literacy and metabolic syndrome or healthy lifestyle characteristics among community-dwelling Japanese people. Diabetol. Metab. Syndr. 2016, 8, 30. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.-L.; Shu, J.-H.; Hsu, H.-C.; Liang, Y.; Chou, R.-H.; Hsu, P.-F.; Wang, Y.-J.; Ding, Y.-Z.; Liou, T.-L.; Wang, Y.-W.; et al. High health literacy is associated with less obesity and lower Framingham risk score: Sub-study of the VGH-HEALTHCARE trial. PLoS ONE 2018, 13, e0194813. [Google Scholar] [CrossRef]
- Bianchi, V.E.; Locatelli, V. Testosterone a key factor in gender related metabolic syndrome. Obes. Rev. 2018, 19, 557–575. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Rebar, A.L. Conceptualizing and Defining the Intention Construct for Future Physical Activity Research. Exerc. Sport Sci. Rev. 2017, 45, 209–216. [Google Scholar] [CrossRef]
- Froze, S.; Arif, M.T.; Saimon, R. Does Health Literacy Predict Preventive Lifestyle on Metabolic Syndrome? A Population-Based Study in Sarawak Malaysia. Open J. Prev. Med. 2018, 8, 14. [Google Scholar] [CrossRef] [Green Version]
- Rucker, D.D.; Preacher, K.J.; Tormala, Z.L.; Petty, R.E. Mediation Analysis in Social Psychology: Current Practices and New Recommendations. Soc. Personal. Psychol. Compass 2011, 5, 359–371. [Google Scholar] [CrossRef]
- Zhang, D.; Liu, X.; Liu, Y.; Sun, X.; Wang, B.; Ren, Y.; Zhao, Y.; Zhou, J.; Han, C.; Yin, L.; et al. Leisure-time physical activity and incident metabolic syndrome: A systematic review and dose-response meta-analysis of cohort studies. Metabolism 2017, 75, 36–44. [Google Scholar] [CrossRef]
- Pardo, A.; Román-Viñas, B.; Ribas-Barba, L.; Roure, E.; Vallbona, C.; Serra-Majem, L. Health-enhancing physical activity and associated factors in a Spanish population. J. Sci. Med. Sport 2014, 17, 188–194. [Google Scholar] [CrossRef]
- Sitthipornvorakul, E.; Janwantanakul, P.; van der Beek, A.J. Correlation between pedometer and the Global Physical Activity Questionnaire on physical activity measurement in office workers. BMC Res. Notes 2014, 7, 280. [Google Scholar] [CrossRef] [Green Version]
- Jancey, J.; Tye, M.; McGann, S.; Blackford, K.; Lee, A.H. Application of the Occupational Sitting and Physical Activity Questionnaire (OSPAQ) to office based workers. BMC Public Health 2014, 14, 762. [Google Scholar] [CrossRef] [Green Version]


| Total (N = 316) | Men (n = 236) | Women (n = 80) | |
|---|---|---|---|
| Age, M (SD) | 50.9 (6.4) | 51.4 (6.4) | 49.5 (6.2) |
| Relationship status | |||
| Relationship, n (%) | 256 (81.0) | 195 (82.6) | 61 (76.3) |
| Single, n (%) | 60 (19.0) | 41 (17.4) | 19 (23.7) |
| Education | |||
| Tertiary, n (%) | 203 (64.2) | 172 (72.9) | 31 (38.7) |
| Secondary, n (%) | 105 (33.2) | 60 (25.4) | 45 (56.3) |
| Primary, n (%) | 8 (2.5) | 4 (1.7) | 4 (5.0) |
| Medication intake | |||
| No medication, n (%) | 142 (44.9) | 109 (46.2) | 33 (41.2) |
| Medication, n (%) | 174 (55.1) | 127 (53.8) | 47 (58.8) |
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | |
|---|---|---|---|---|---|---|---|---|---|
| 1. PAHCO | |||||||||
| 2. CCPT | 0.84 *** | ||||||||
| 3. PAAR | 0.70 *** | 0.30 *** | |||||||
| 4. PASR | 0.74 *** | 0.47 *** | 0.38 *** | ||||||
| 5. Occupational PA | 0.03 | 0.01 | 0.04 | 0.04 | |||||
| 6. Leisure-time PA | 0.42 *** | 0.34 *** | 0.20 *** | 0.45 *** | 0.03 | ||||
| 7. Physical Component Score | 0.26 *** | 0.23 *** | 0.11 | 0.26 *** | −0.01 | 0.28 *** | |||
| 8. Mental Component Score | 0.12 * | 0.16 ** | −0.00 | 0.11 * | 0.11 | 0.10 | 0.45 *** | ||
| 9. MetSSS | −0.21 *** | −0.12 * | −0.17 *** | −0.22 * | 0.14 * | −0.13 * | −0.18 ** | −0.01 | |
| Mean | 2.68 | 2.64 | 2.78 | 2.60 | 1.66 | 18.42 | 49.01 | 45.97 | 0.06 |
| SD | 0.48 | 0.58 | 0.64 | 0.65 | 0.28 | 14.27 | 6.18 | 7.94 | 0.86 |
| Predictor | β | SE | 95% CI |
|---|---|---|---|
| Mediator: Leisure-time PA | |||
| PAHCO | 0.52 *** | 0.06 | (0.41, 0.62) |
| Medication intake | 0.06 | 0.05 | (−0.01, 0.17) |
| R2 = 0.29 | |||
| Criterion: Physical Component Score | |||
| Leisure-time PA | 0.14 * | 0.05 | (0.03, 0.25) |
| PAHCO | 0.16 * | 0.07 | (0.04, 0.29) |
| MetSSS | −0.16 ** | 0.06 | (−0.28, −0.04) |
| Mental Component Score | 0.40 *** | 0.05 | (0.32, 0.49) |
| Medication intake | 0.10 * | 0.05 | (0.00, 0.20) |
| R2 = 0.27 | |||
| Criterion: MetSSS | |||
| Leisure-time PA | −0.01 | 0.06 | (−0.13, 0.11) |
| PAHCO | −0.22 ** | 0.08 | (−0.37, −0.08) |
| Physical Component Score | −0.16 ** | 0.06 | (−0.28, −0.04) |
| Medication intake | −0.15 ** | 0.05 | (−0.24, −0.06) |
| Sex | 0.41 *** | 0.04 | (0.32, 0.49) |
| Occupational PA | 0.07 | 0.05 | (−0.03, 0.17) |
| R2 = 0.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blaschke, S.; Carl, J.; Ellinger, J.; Birner, U.; Mess, F. The Role of Physical Activity-Related Health Competence and Leisure-Time Physical Activity for Physical Health and Metabolic Syndrome: A Structural Equation Modeling Approach for German Office Workers. Int. J. Environ. Res. Public Health 2021, 18, 10153. https://doi.org/10.3390/ijerph181910153
Blaschke S, Carl J, Ellinger J, Birner U, Mess F. The Role of Physical Activity-Related Health Competence and Leisure-Time Physical Activity for Physical Health and Metabolic Syndrome: A Structural Equation Modeling Approach for German Office Workers. International Journal of Environmental Research and Public Health. 2021; 18(19):10153. https://doi.org/10.3390/ijerph181910153
Chicago/Turabian StyleBlaschke, Simon, Johannes Carl, Jan Ellinger, Ulrich Birner, and Filip Mess. 2021. "The Role of Physical Activity-Related Health Competence and Leisure-Time Physical Activity for Physical Health and Metabolic Syndrome: A Structural Equation Modeling Approach for German Office Workers" International Journal of Environmental Research and Public Health 18, no. 19: 10153. https://doi.org/10.3390/ijerph181910153