
Recruiting Cancer Survivors to a Mobile Mindfulness Intervention in the United States: Exploring Online and Face-to-Face Recruitment Strategies

 , ,
, ,
Abstract
:1. Introduction
1.1. Background
1.2. Strengths and Limitations of Online Recruitment Methods
1.3. The Current Study
- Does the recruitment method impact retention rates?
- Does the recruitment method influence sample demographics and characteristics?
- Which recruitment methods prove most effective in recruiting and retaining participants?
2. Materials and Methods
2.1. Mobile Mindfulness Intervention to Promote the Well-Being of Cancer Survivors
2.2. Participants
2.3. Measures
2.3.1. Participant Demographics
2.3.2. Recruitment Method
2.3.3. Baseline PROs
2.3.4. Retention
2.4. Recruitment Strategies
2.4.1. Traditional Recruitment Methods
2.4.2. Web-Based Recruitment Methods
2.5. Statistical Analysis
3. Results
3.1. Participant Demographics and PROs
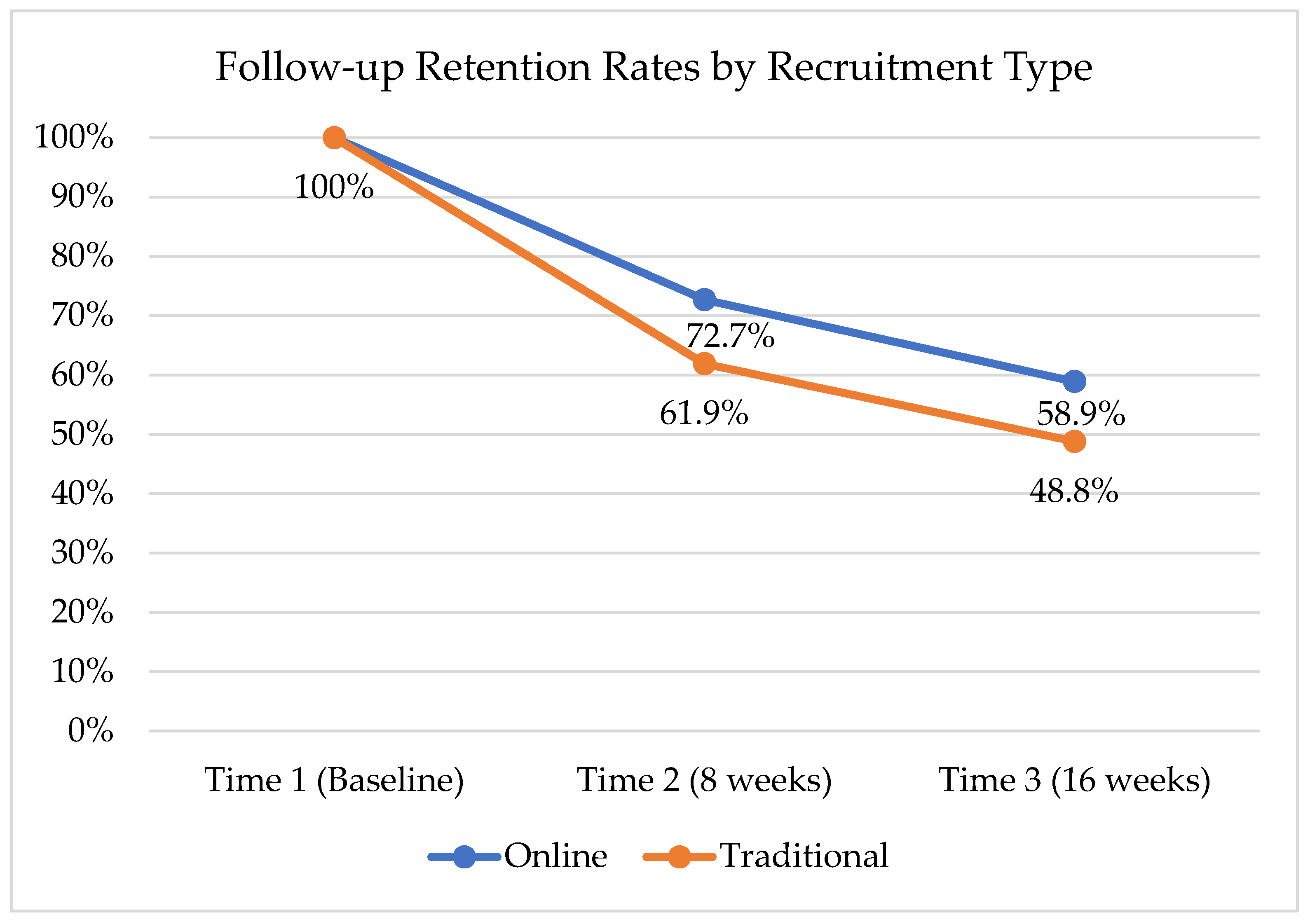
3.2. Retention
4. Discussion
4.1. Participant Demographics and PROs
4.2. Retention
4.3. Strengths and Limitations
4.3.1. Impact of COVID-19
4.3.2. Fraudulent Users
4.4. Suggestions and Future Directions for Online Recruitment
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mph, K.D.M.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [Green Version]
- Hulbert-Williams, N.J.; Pendrous, R.; Hulbert-Williams, L.; Swash, B. Recruiting cancer survivors into research studies using online methods: A secondary analysis from an international cancer survivorship cohort study. Ecancermedicalscience 2019, 13, 990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Befort, C.A.; Bennett, L.; Christifano, D.; Klemp, J.R.; Krebill, H. Effective recruitment of rural breast cancer survivors into a lifestyle intervention. Psycho-Oncology 2015, 24, 487–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Lankveld, J.J.; Fleer, J.; Schroevers, M.J.; Sanderman, R.; Oudsten, B.L.D.; Dekker, J. Recruitment problems in psychosocial oncology research. Psycho-Oncology 2018, 27, 2296–2298. [Google Scholar] [CrossRef] [PubMed]
- Benedict, C.; Hahn, A.L.; Diefenbach, M.A.; Ford, J.S. Recruitment via social media: Advantages and potential biases. Digit. Health 2019, 5, 2055207619867223. [Google Scholar] [CrossRef] [Green Version]
- Rabin, C.; Horowitz, S.; Marcus, B. Recruiting Young Adult Cancer Survivors for Behavioral Research. J. Clin. Psychol. Med. Settings 2012, 20, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Kayrouz, R.; Dear, B.; Karin, E.; Titov, N. Facebook as an effective recruitment strategy for mental health research of hard to reach populations. Internet Interv. 2016, 4, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Lane, T.S.; Armin, J.; Gordon, J.S. Online Recruitment Methods for Web-Based and Mobile Health Studies: A Review of the Literature. J. Med. Internet Res. 2015, 17, e183. [Google Scholar] [CrossRef] [Green Version]
- Morgan, A.J.; Jorm, A.F.; Mackinnon, A. Internet-Based Recruitment to a Depression Prevention Intervention: Lessons from the Mood Memos Study. J. Med. Internet Res. 2013, 15, e31. [Google Scholar] [CrossRef]
- May, C.N.; Jake-Schoffman, D.E.; Evans, M.; Silfee, V.J.; Zhang, F.F.; Blok, A.C.; Carey, J.L.; Ding, E.; Pritschmann, R.K. Interest in and barriers to participation in a Facebook-delivered weight loss program among female cancer survivors with overweight or obesity. mHealth 2019, 5, 28. [Google Scholar] [CrossRef] [Green Version]
- Fredman, S.J.; Baucom, D.H.; Gremore, T.M.; Castellani, A.M.; Kallman, T.A.; Porter, L.S.; Kirby, J.S.; Dees, E.C.; Klauber-Demore, N.; Peppercorn, J.; et al. Quantifying the recruitment challenges with couple-based interventions for cancer: Applications to early-stage breast cancer. Psycho-Oncology 2008, 18, 667–673. [Google Scholar] [CrossRef] [Green Version]
- Gorman, J.R.; Roberts, S.C.; Dominick, S.A.; Malcarne, V.L.; Dietz, A.C.; Su, H.I. A Diversified Recruitment Approach Incorporating Social Media Leads to Research Participation Among Young Adult-Aged Female Cancer Survivors. J. Adolesc. Young-Adult Oncol. 2014, 3, 59–65. [Google Scholar] [CrossRef] [Green Version]
- Burke-Garcia, A.; Scally, G. Trending now: Future directions in digital media for the public health sector. J. Public Health 2014, 36, 527–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, T.; Riis, A.H.; Hatch, E.E.; Wise, L.A.; Nielsen, M.G.; Rothman, K.J.; Sørensen, H.T.; Mikkelsen, E.M.; Harris, K.; Nelson, E. Costs and Efficiency of Online and Offline Recruitment Methods: A Web-Based Cohort Study. J. Med. Internet Res. 2017, 19, e58. [Google Scholar] [CrossRef] [PubMed]
- Topolovec-Vranic, J.; Natarajan, K. The Use of Social Media in Recruitment for Medical Research Studies: A Scoping Review. J. Med. Internet Res. 2016, 18, e286. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, C.J.; Stevelink, S.; Fear, N.T. The Use of Facebook in Recruiting Participants for Health Research Purposes: A Systematic Review. J. Med. Internet Res. 2017, 19, e290. [Google Scholar] [CrossRef] [Green Version]
- Keaver, L.; McGough, A.; Du, M.; Chang, W.; Chomitz, V.; Allen, J.D.; Attai, D.J.; Gualtieri, L.; Zhang, F.F. Potential of Using Twitter to Recruit Cancer Survivors and Their Willingness to Participate in Nutrition Research and Web-Based Interventions: A Cross-Sectional Study. JMIR Cancer 2019, 5, e7850. [Google Scholar] [CrossRef]
- Owen, J.E.; Bantum, E.O.; Criswell, K.; Bazzo, J.; Gorlick, A.; Stanton, A.L. Representativeness of two sampling procedures for an internet intervention targeting cancer-related distress: A comparison of convenience and registry samples. J. Behav. Med. 2013, 37, 630–641. [Google Scholar] [CrossRef] [Green Version]
- Layi, G.; Albright, C.A.; Berenberg, J.; Plant, K.; Ritter, P.; Laurent, D.; Lorig, K.; Bantum, E.O. UH Cancer Center Hotline: Recruiting Cancer Survivors for an Online Health-Behavior Change Intervention: Are Different Strategies More Beneficial? Hawaii Med. J. 2011, 70, 222–223. [Google Scholar]
- Pilkonis, P.A.; Choi, S.W.; Reise, S.P.; Stover, A.; Riley, W.T.; Cella, D.; PROMIS Cooperative Group. Item Banks for Measuring Emotional Distress from the Patient-Reported Outcomes Measurement Information System (PROMIS®): Depression, Anxiety, and Anger. Assessment 2011, 18, 263–283. [Google Scholar] [CrossRef]
- Krebs, E.E.; Lorenz, K.A.; Bair, M.J.; Damush, T.M.; Wu, J.; Sutherland, J.M.; Asch, S.M.; Kroenke, K. Development and Initial Validation of the PEG, a Three-item Scale Assessing Pain Intensity and Interference. J. Gen. Intern. Med. 2009, 24, 733–738. [Google Scholar] [CrossRef] [Green Version]
- Mendoza, T.R.; Wang, X.S.; Cleeland, C.S.; Morrissey, M.; Johnson, B.A.; Wendt, J.K.; Huber, S.L. The Rapid Assessment of Fatigue Severity in Cancer Patients: Use of the Brief Fatigue Inventory. Cancer 1999, 85, 1186–1196. [Google Scholar] [CrossRef]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and Standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the General Population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using Self-Report Assessment Methods to Explore Facets of Mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Cancer Institute Adolescents and Young Adults (AYAs) with Cancer—National Cancer Institute. Available online: https://www.cancer.gov/types/aya (accessed on 16 August 2021).
- Carson, J.W.; Carson, K.M.; Olsen, M.K.; Sanders, L.; Porter, L.S. Mindful Yoga for women with metastatic breast cancer: Design of a randomized controlled trial. BMC Complement. Altern. Med. 2017, 17, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koutoukidis, D.; Beeken, R.; Manchanda, R.; Michalopoulou, M.; Burnell, M.; Knobf, M.T.; Lanceley, A. Recruitment, adherence, and retention of endometrial cancer survivors in a behavioural lifestyle programme: The Diet and Exercise in Uterine Cancer Survivors (DEUS) parallel randomised pilot trial. BMJ Open 2017, 7, e018015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantrell, M.A.; Conte, T.; Hudson, M.; Shad, A.; Ruble, K.; Herth, K.; Canino, A.; Kemmy, S. Recruitment and retention of older adolescent and young adult female survivors of childhood cancer in longitudinal research. Oncol. Nurs. Forum 2012, 39, 483–490. [Google Scholar] [CrossRef] [Green Version]
- United States Census Bureau. U.S. Census Bureau QuickFacts: Hawaii. Available online: https://www.census.gov/quickfacts/HI (accessed on 23 August 2021).
- Doraiswamy, S.; Abraham, A.; Mamtani, R.; Cheema, S. Use of Telehealth during the COVID-19 Pandemic: Scoping Review. J. Med. Internet Res. 2020, 22, e24087. [Google Scholar] [CrossRef]
- Wijesooriya, N.R.; Mishra, V.; Brand, P.L.; Rubin, B.K. COVID-19 and telehealth, education, and research adaptations. Paediatr. Respir. Rev. 2020, 35, 38–42. [Google Scholar] [CrossRef]
- Mehrotra, A.; Chernew, M.E.; Linetsky, D.; Hatch, H.; Cutler, D.A.; Schneider, E.C. The Impact of the COVID-19 Pandemic on Outpatient Visits: Changing Patterns of Care in the Newest COVID-19 Hot Spots. Available online: https://doi.org/10.26099/yaqe-q550 (accessed on 25 May 2021).
- Demeke, H.B.; Merali, S.; Marks, S.; Pao, L.Z.; Romero, L.; Sandhu, P.; Clark, H.; Clara, A.; McDow, K.B.; Tindall, E.; et al. Trends in Use of Telehealth Among Health Centers During the COVID-19 Pandemic—United States, June 26–November 6, 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Heffner, J.L.; Wyszynski, C.M.; Comstock, B.; Mercer, L.D.; Bricker, J. Overcoming recruitment challenges of web-based interventions for tobacco use: The case of web-based acceptance and commitment therapy for smoking cessation. Addict. Behav. 2013, 38, 2473–2476. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Traditional | Online | |||||||
|---|---|---|---|---|---|---|---|---|
| (N = 43) | (N = 77) | |||||||
| Variable | Value | N | % | N | % | χ2 | df | p |
| Group | Control | 21 | 48.8 | 37 | 48.1 | 0.0 | 1 | 0.93 |
| Mindfulness App | 22 | 51.2 | 40 | 51.9 | ||||
| Recruitment source | ||||||||
| Clinical recruitment | 17 | 39.5 | ||||||
| Traditional support group | 12 | 27.9 | ||||||
| Friend/family | 14 | 32.6 | ||||||
| 25 | 32.5 | |||||||
| Social media | 47 | 61.0 | ||||||
| Other online method | 5 | 6.5 | ||||||
| Retention | ||||||||
| Completed T2 Survey | No | 16 | 38.1 | 21 | 27.3 | 1.5 | 1 | 0.22 |
| Yes | 26 | 61.9 | 56 | 72.7 | ||||
| Completed T3 Survey | No | 21 | 51.2 | 30 | 41.1 | 1.1 | 1 | 0.30 |
| Yes | 20 | 48.8 | 43 | 58.9 | ||||
| Participant Demographics | ||||||||
| Sex | Female | 33 | 76.7 | 67 | 87.0 | 2.1 | 1 | 0.15 |
| Male | 10 | 23.3 | 10 | 13.0 | ||||
| Age | 18–34 | 2 | 4.7 | 23 | 29.9 | 10.6 | 2 | 0.005 |
| 35–54 | 22 | 51.2 | 29 | 37.7 | ||||
| 55+ | 19 | 44.2 | 25 | 32.5 | ||||
| Currently Live | Hawai‘i | 26 | 60.5 | 25 | 32.5 | 9.4 | 2 | 0.009 |
| Continental U.S. | 15 | 34.9 | 49 | 63.6 | ||||
| Other | 2 | 4.7 | 3 | 3.9 | ||||
| Ethnicity | Asian | 12 | 27.9 | 10 | 13.0 | 16.1 | 3 | 0.001 |
| Caucasian | 16 | 37.2 | 56 | 72.7 | ||||
| Hawaiian/part-Hawaiian | 6 | 14.0 | 2 | 2.6 | ||||
| Other | 9 | 20.9 | 9 | 11.7 | ||||
| Education | No college degree | 15 | 34.9 | 16 | 20.8 | 4.7 | 2 | 0.09 |
| College degree | 20 | 46.5 | 34 | 44.2 | ||||
| Graduate degree | 8 | 18.6 | 27 | 35.1 | ||||
| Employment | Full-time | 18 | 41.9 | 36 | 46.8 | 0.3 | 3 | 0.95 |
| Part-time | 6 | 14.0 | 11 | 14.3 | ||||
| Retired | 8 | 18.6 | 13 | 16.9 | ||||
| Unemployed | 11 | 25.6 | 17 | 22.1 | ||||
| Marital Status | Living with a partner | 5 | 11.6 | 12 | 15.6 | 4.5 | 3 | 0.21 |
| Married | 25 | 58.1 | 40 | 51.9 | ||||
| Past partner | 8 | 18.6 | 7 | 9.1 | ||||
| Single, never married | 5 | 11.6 | 18 | 23.4 | ||||
| Years Since Diagnosis | 0–2 | 12 | 29.3 | 18 | 23.4 | 8.4 | 2 | 0.02 |
| 2–5 | 23 | 56.1 | 28 | 36.4 | ||||
| 5+ | 6 | 14.6 | 31 | 40.3 | ||||
| Years Since Treatment | 0–2 | 27 | 65.9 | 32 | 42.7 | 8.8 | 2 | 0.01 |
| 2–5 | 11 | 26.8 | 21 | 28.0 | ||||
| 5+ | 3 | 7.3 | 22 | 29.3 | ||||
| Cancer Type | Blood | 1 | 2.3 | 10 | 13.0 | 18.6 | 4 | 0.0009 |
| Breast | 22 | 51.2 | 25 | 32.5 | ||||
| Colorectal | 4 | 9.3 | 5 | 6.5 | ||||
| Lung | 5 | 11.6 | 0 | 0.0 | ||||
| Other | 11 | 25.6 | 37 | 48.1 | ||||
| Stage | 0–1 | 22 | 53.7 | 18 | 26.5 | 8.3 | 3 | 0.04 |
| 2 | 9 | 22.0 | 22 | 32.4 | ||||
| 3 | 8 | 19.5 | 21 | 30.9 | ||||
| 4 | 2 | 4.9 | 7 | 10.3 | ||||
| Type of Treatment Received | ||||||||
| Surgery | No | 9 | 20.9 | 13 | 16.9 | 0.3 | 1 | 0.58 |
| Yes | 34 | 79.1 | 64 | 83.1 | ||||
| Chemotherapy | No | 8 | 18.6 | 18 | 23.4 | 0.4 | 1 | 0.54 |
| Yes | 35 | 81.4 | 59 | 76.6 | ||||
| Radiation | No | 21 | 48.8 | 41 | 53.2 | 0.2 | 1 | 0.64 |
| Yes | 22 | 51.2 | 36 | 46.8 | ||||
| Hormonal | No | 26 | 60.5 | 53 | 68.8 | 0.9 | 1 | 0.35 |
| Yes | 17 | 39.5 | 24 | 31.2 | ||||
| Other Medical Conditions | ||||||||
| Arthritis | No | 29 | 80.6 | 49 | 89.1 | 1.3 | 1 | 0.26 |
| Yes | 7 | 19.4 | 6 | 10.9 | ||||
| Asthma | No | 26 | 72.2 | 40 | 72.7 | 0.0 | 1 | 0.96 |
| Yes | 10 | 27.8 | 15 | 27.3 | ||||
| Back Problems | No | 26 | 72.2 | 42 | 76.4 | 0.2 | 1 | 0.66 |
| Yes | 10 | 27.8 | 13 | 23.6 | ||||
| Diabetes | No | 32 | 88.9 | 50 | 90.9 | 0.1 | 1 | 0.75 |
| Yes | 4 | 11.1 | 5 | 9.1 | ||||
| Emphysema | No | 36 | 100.0 | 54 | 98.2 | 0.7 | 1 | 0.42 |
| Yes | 0 | 0.0 | 1 | 1.8 | ||||
| Heart Disease | No | 34 | 94.4 | 54 | 98.2 | 1.0 | 1 | 0.33 |
| Yes | 2 | 5.6 | 1 | 1.8 | ||||
| High Blood Pressure | No | 20 | 55.6 | 42 | 76.4 | 4.3 | 1 | 0.04 |
| Yes | 16 | 44.4 | 13 | 23.6 | ||||
| Other Problems | No | 21 | 58.3 | 33 | 60.0 | 0.0 | 1 | 0.87 |
| Yes | 15 | 41.7 | 22 | 40.0 | ||||
| Traditional | Online | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PRO | N | Mean | SD | Min | Max | N | Mean | SD | Min | Max | p |
| PHQ-9 | 43 | 19.7 | 4.8 | 10 | 30 | 77 | 18.8 | 5.1 | 9 | 34 | 0.32 |
| GAD-7 | 43 | 16.7 | 3.9 | 11 | 28 | 77 | 16.7 | 4.1 | 8 | 28 | 0.93 |
| PCL-5 | 43 | 44.2 | 12.3 | 26 | 73 | 77 | 41.8 | 13.1 | 23 | 82 | 0.32 |
| PEG-3 | 43 | 12.6 | 7.2 | 0 | 30 | 76 | 9.3 | 7.8 | 0 | 30 | 0.02 |
| BFI-9 | 43 | 44.5 | 19.5 | 6 | 86 | 76 | 38.1 | 20.2 | 1 | 84 | 0.09 |
| FFMQ-O 8 1 | 43 | 26.3 | 5.0 | 13 | 37 | 77 | 25.3 | 5.3 | 13 | 38 | 0.33 |
| FFMQ-D 8 2 | 43 | 26.7 | 6.2 | 16 | 40 | 77 | 27.4 | 6.3 | 15 | 40 | 0.57 |
| FFMQ-A 8 3 | 43 | 24.5 | 4.0 | 14 | 35 | 77 | 24.2 | 5.1 | 15 | 40 | 0.77 |
| FFMQ-NJ 8 4 | 43 | 24.8 | 7.8 | 14 | 40 | 77 | 26.1 | 6.2 | 10 | 39 | 0.37 |
| FFMQ-NR 7 5 | 43 | 21.0 | 3.4 | 13 | 28 | 77 | 20.2 | 3.6 | 10 | 29 | 0.19 |
| FFMQ-39 6 | 43 | 123.3 | 15.2 | 101 | 168 | 77 | 123.1 | 17.0 | 84 | 166 | 0.96 |
| Variable | Value | Statistic | Total | No | Yes | χ2 | df | p |
|---|---|---|---|---|---|---|---|---|
| Completed T2 Follow-up | ||||||||
| Total | N (%) | 122 | 37 (30.3) | 85 (69.7) | ||||
| Group | Control | N (%) | 58 | 12 (20.7) | 46 (79.3) | 4.9 | 1 | 0.03 |
| Mindfulness App | N (%) | 64 | 25 (39.1) | 39 (60.9) | ||||
| Recruitment Method | Traditional | N (%) | 42 | 16 (38.1) | 26 (61.9) | 1.5 | 1 | 0.22 |
| Online | N (%) | 77 | 21 (27.3) | 56 (72.7) | ||||
| Missing data | N (%) | 3 | 0 (0.00) | 3 (7.1) | ||||
| Completed T3 Follow-up | ||||||||
| Total | N (%) | 117 | 52 (44.4) | 65 (55.6) | ||||
| Group | Control | N (%) | 54 | 20 (37.0) | 34 (63.0) | 2.2 | 1 | 0.14 |
| Mindfulness App | N (%) | 63 | 32 (50.8) | 31 (49.2) | ||||
| Recruitment Method | Traditional | N (%) | 41 | 21 (51.2) | 20 (48.8) | 1.1 | 1 | 0.30 |
| Online | N (%) | 73 | 30 (41.1) | 43 (58.9) | ||||
| Missing data | N (%) | 3 | 1 (0.9) | 2 (1.7) | ||||
| Completed T2 Follow-Up | No | N (%) | 37 | 37 (100.0) | 0 (0.00) | 67.6 | 1 | <0.0001 |
| Yes | N (%) | 80 | 15 (18.8) | 65 (81.3) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arnobit, C.I.; Loo, K.; Pagano, I.; Uchiyama, M.; Fukui, J.; Braun-Inglis, C.; Bantum, E.O. Recruiting Cancer Survivors to a Mobile Mindfulness Intervention in the United States: Exploring Online and Face-to-Face Recruitment Strategies. Int. J. Environ. Res. Public Health 2021, 18, 10136. https://doi.org/10.3390/ijerph181910136
Arnobit CI, Loo K, Pagano I, Uchiyama M, Fukui J, Braun-Inglis C, Bantum EO. Recruiting Cancer Survivors to a Mobile Mindfulness Intervention in the United States: Exploring Online and Face-to-Face Recruitment Strategies. International Journal of Environmental Research and Public Health. 2021; 18(19):10136. https://doi.org/10.3390/ijerph181910136
Chicago/Turabian StyleArnobit, Celine Isabelle, Kiana Loo, Ian Pagano, Mai Uchiyama, Jami Fukui, Christa Braun-Inglis, and Erin O’Carroll Bantum. 2021. "Recruiting Cancer Survivors to a Mobile Mindfulness Intervention in the United States: Exploring Online and Face-to-Face Recruitment Strategies" International Journal of Environmental Research and Public Health 18, no. 19: 10136. https://doi.org/10.3390/ijerph181910136