
Non-Preferred Work and the Incidence of Spinal Pain and Psychological Distress—A Prospective Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
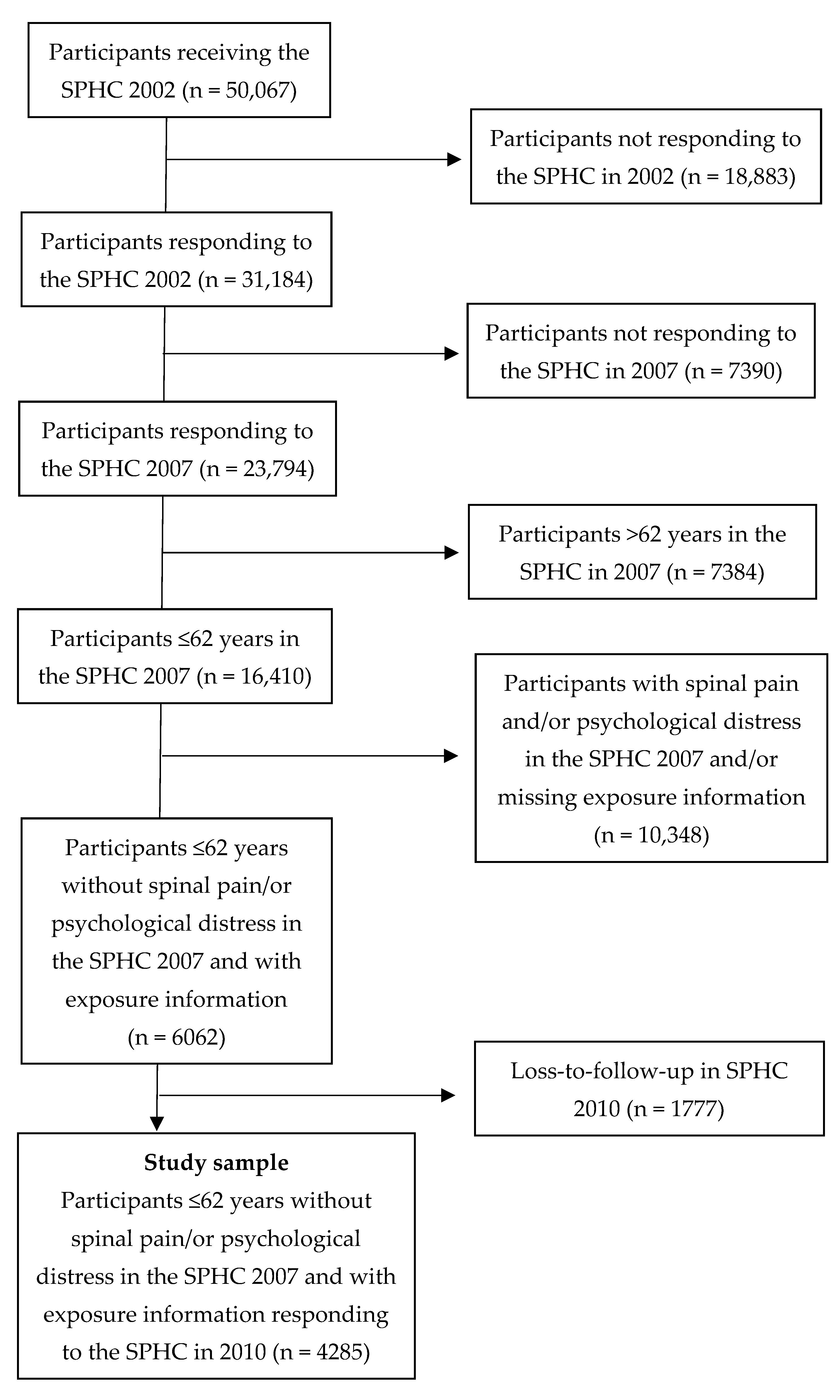
2.1. Study Design and Sample
2.2. Exposure and Potential Effect Modifier
- -
- Preferred work was equal to answering “Yes” (a) to questions 1 and 2, regardless of the answer to question 3;
- -
- Non-preferred work with a high possibility to change was equal to answering “No” (b) to question 1 and/or “No” (b) to question 2 and answering “Very good” (a) or “Good” (b) to question 3;
- -
- Non-preferred work with low possibility to change was equal to answering “No” (b) to questions 1 and/or 2 and “Poor” (c) or “Very poor” (d) to question 3.
2.3. Outcomes
- (a)
- “During the past 6 months, have you felt pain in your upper back or neck at least a couple of days per week?” (yes/no);
- (b)
- “During the past 6 months, have you felt pain in your lower back at least a couple of days per week?” (yes/no).
2.4. Potential Confounders
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef]
- Hurwitz, E.L.; Randhawa, K.; Yu, H.; Côté, P.; Haldeman, S. The Global Spine Care Initiative: A summary of the global burden of low back and neck pain studies. Eur. Spine J. 2018, 27, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Försäkringskassan. Rapport—Uppföljning av Sjukfrånvarons Utveckling 2018; Försäkringskassan: Stockholm, Sweden, 2018; Volume 002671-2018, Available online: https://www.forsakringskassan.se/wps/wcm/connect/d3d2d056-0ae7-46d9-b350-ac87e4696f1c/rapport-uppfoljning-av-sjukfranvarons-utveckling-2018-svar-pa-regeringsuppdrag-dnr-002671-2018.pdf?MOD=AJPERES&CVID= (accessed on 3 May 2021).
- Bevan, S. Economic impact of musculoskeletal disorders (MSDs) on work in Europe. Best Pract. Res. Clin. Rheumatol. 2015, 29, 356–373. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Smit, F. Subthreshold depression as a risk indicator for major depressive disorder: A systematic review of prospective studies. Acta Psychiatr. Scand. 2004, 109, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Shankman, S.A.; Lewinsohn, P.M.; Klein, D.N.; Small, J.W.; Seeley, J.R.; Altman, S.E. Subthreshold conditions as precursors for full syndrome disorders: A 15-year longitudinal study of multiple diagnostic classes. J. Child Psychol. Psychiatry 2009, 50, 1485–1494. [Google Scholar] [CrossRef] [Green Version]
- Folkhälsomyndigheten. Psykisk ohälsa bland högskole- och universitetsstudenter kan förebyggas. 2018. Available online: https://www.folkhalsomyndigheten.se/publicerat-material/publikationsarkiv/p/psykisk-ohalsa-bland-hogskole--och-universitetsstudenter-kan-forebyggas/?pub=53659#53663 (accessed on 3 May 2021).
- Paanalahti, K.; Holm, L.W.; Magnusson, C.; Carroll, L.; Nordin, M.; Skillgate, E. The sex-specific interrelationship between spinal pain and psychological distress across time in the general population. Results from the Stockholm Public Health Study. Spine J. 2014, 14, 1928–1935. [Google Scholar] [CrossRef]
- Campbell, P.; Hope, K.; Dunn, K.M. The pain, depression, disability pathway in those with low back pain: A moderation analysis of health locus of control. J. Pain Res. 2017, 10, 2331–2339. [Google Scholar] [CrossRef] [Green Version]
- Hansson, E.K.; Hansson, T.H. The costs for persons sick-listed more than one month because of low back or neck problems. A two-year prospective study of Swedish patients. Eur. Spine J. 2004, 14, 337–345. [Google Scholar] [CrossRef] [Green Version]
- Patrick, N.; Emanski, E.; Knaub, M.A. Acute and Chronic Low Back Pain. Med. Clin. N. Am. 2016, 100, 169–181. [Google Scholar] [CrossRef]
- Rasmussen-Barr, E.; Grooten, W.J.; Hallqvist, J.; Holm, L.W.; Skillgate, E. Are job strain and sleep disturbances prognostic factors for neck/shoulder/arm pain? A cohort study of a general population of working age in Sweden. BMJ Open 2014, 4, e005103. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen-Barr, E.; Grooten, W.; Hallqvist, J.; Holm, L.; Skillgate, E. Are job strain and sleep disturbances prognostic factors for low-back pain? A cohort study of a general population of working age in Sweden. J. Rehabilitation Med. 2017, 49, 591–597. [Google Scholar] [CrossRef] [Green Version]
- Loghmani, A.; Golshiri, P.; Zamani, A.; Kheirmand, M.; Jafari, N. Musculoskeletal symptoms and job satisfaction among office-workers: A Cross- sectional study from Iran. Acta Med. Acad. 2013, 42, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Jun, D.; Zoe, M.; Johnston, V.; O’Leary, S. Physical risk factors for developing non-specific neck pain in office workers: A systematic review and meta-analysis. Int. Arch. Occup. Environ. Health 2017, 90, 373–410. [Google Scholar] [CrossRef]
- Bonde, J.P.E. Psychosocial factors at work and risk of depression: A systematic review of the epidemiological evidence. Occup. Environ. Med. 2008, 65, 438–445. [Google Scholar] [CrossRef]
- Muhonen, T. Feeling double locked-in at work: Implications for health and job satisfaction among municipal employees. Work 2010, 37, 199–204. [Google Scholar] [CrossRef] [Green Version]
- Fahlén, G.; Goine, H.; Edlund, C.; Arrelöv, B.; Knutsson, A.; Peter, R. Effort-reward imbalance, “locked in” at work, and long-term sick leave. Int. Arch. Occup. Environ. Health 2009, 82, 191–197. [Google Scholar] [CrossRef]
- Stengård, J.; Bernhard-Oettel, C.; Berntson, E.; Leineweber, C.; Aronsson, G. Stuck in a job: Being “locked-in” or at risk of becoming locked-in at the workplace and well-being over time. Work. Stress 2016, 30, 152–172. [Google Scholar] [CrossRef] [Green Version]
- Jonsson, J.; Matilla-Santander, N.; Kreshpaj, B.; Johansson, G.; Kjellberg, K.; Burström, B.; Östergren, P.-O.; Nilsson, K.; Strömdahl, S.; Orellana, C.; et al. Precarious employment and general, mental and physical health in Stockholm, Sweden: A cross-sectional study. Scand. J. Public Health 2021, 49, 228–236. [Google Scholar] [CrossRef]
- Matilla-Santander, N.; Martín-Sánchez, J.C.; González-Marrón, A.; Cartanyà-Hueso, À.; Lidón-Moyano, C.; Martínez-Sánchez, J.M. Precarious employment, unemployment and their association with health-related outcomes in 35 European countries: A cross-sectional study. Crit. Public Health 2020, 31, 404–415. [Google Scholar] [CrossRef]
- Finan, P.H.; Goodin, B.R.; Smith, M.T. The Association of Sleep and Pain: An Update and a Path Forward. J. Pain 2013, 14, 1539–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lautenbacher, S.; Kundermann, B.; Krieg, J.C. Sleep deprivation and pain perception. Sleep Med. Rev. 2006, 10, 357–369. [Google Scholar] [CrossRef]
- Smith, M.T.; Haythornthwaite, J.A. How do sleep disturbance and chronic pain inter-relate? Insights from the longitudinal and cognitive-behavioral clinical trials literature. Sleep Med. Rev. 2004, 8, 119–132. [Google Scholar] [CrossRef]
- Anderson, K.; Bradley, A.J. Sleep disturbance in mental health problems and neurodegenerative disease. Nat. Sci. Sleep 2013, 5, 61–75. [Google Scholar] [CrossRef] [Green Version]
- SBU. Arbetsmiljöns Betydelse för Sömnstörningar: En Systematisk Litteraturöversikt; Rapport; 216; Swedish Council on Health Technology Assessment (SBU): Stockholm, Sweden, 2013; Available online: https://www.sbu.se/contentassets/aaa2cf8e553e4f66a00bf402ed7cf0cc/arbetsmiljo_somn_2013.pdf (accessed on 3 May 2021).
- Svensson, A.C.; Fredlund, P.; Laflamme, L.; Hallqvist, J.; Alfredsson, L.; Ekbom, A.; Feychting, M.; Forsberg, B.; Pedersen, N.L.; Vågerö, D.; et al. Cohort Profile: The Stockholm Public Health Cohort. Int. J. Epidemiol. 2013, 42, 1263–1272. [Google Scholar] [CrossRef]
- McDowell, I. Measuring Health: A Guide to Rating Scales and Questionnaires, 3rd ed.; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Sconfienza, G.; Mätning av Psykiskt Välbefinnande Bland Ungdomar i Sverige, Användningen av GHQ-12. Arbetslivsinstitutet, Arbete och Hälsa 1998:22. Available online: http://hdl.handle.net/2077/4181 (accessed on 3 May 2021).
- Rai, D.; Kosidou, K.; Lundberg, M.; Araya, R.; Lewis, G.; Magnusson, C. Psychological distress and risk of long-term disability: Population-based longitudinal study. J. Epidemiology Community Health 2011, 66, 586–592. [Google Scholar] [CrossRef]
- Montazeri, A.; Harirchi, A.M.; Shariati, M.; Garmaroudi, G.; Ebadi, M.; Fateh, A. The 12-item General Health Questionnaire (GHQ-12): Translation and validation study of the Iranian version. Health Qual. Life Outcomes 2003, 1, 66. [Google Scholar] [CrossRef] [Green Version]
- Pevalin, D.J. Multiple applications of the GHQ-12 in a general population sample: An investigation of long-term retest effects. Soc. Psychiatry Psychiatr. Epidemiol. 2000, 35, 508–512. [Google Scholar] [CrossRef]
- SBU. Preventiva Insatser vid Akut Smärta Från Rygg och Nacke: En Systematisk Översikt och Utvärdering av Medicinska, Hälsoekonomiska och Etiska Aspekter; Rapport; 245; Statens Beredning för Medicinsk och Social Utvärdering (SBU): Stockholm, Sweden, 2016; Available online: https://www.sbu.se/contentassets/fc9b009a51834b69b2dbc25f80fef475/prevention_smarta_160607.pdf (accessed on 3 May 2021).
- SBU. Ont i Ryggen, ont i Nacken: En Systematisk Litteraturöversikt; Statens Beredning för Medicinsk Utvärdering: Stockholm, Sweden, 2000; Available online: https://www.sbu.se/contentassets/a1c7fd6945514079bf0db408269e6685/ont_ryggen_ont_nacken_fulltext.pdf (accessed on 3 May 2021).
- Gureje, O.; Von Korff, M.; Kola, L.; Demyttenaere, K.; He, Y.; Posada-Villa, J.; Lepine, J.P.; Angermeyer, M.C.; Levinson, D.; de Girolamo, G.; et al. The relation between multiple pains and mental disorders: Results from the World Mental Health Surveys. Pain 2008, 135, 82–91. [Google Scholar] [CrossRef] [Green Version]
- Roy-Byrne, P.P.; Davidson, K.W.; Kessler, R.C.; Asmundson, G.J.; Goodwin, R.D.; Kubzansky, L.; Lydiard, R.B.; Massie, M.J.; Katon, W.; Laden, S.K.; et al. Anxiety disorders and comorbid medical illness. Gen. Hosp. Psychiatry 2008, 30, 208–225. [Google Scholar] [CrossRef] [PubMed]
- Canivet, C.; Aronsson, G.; Bernhard-Oettel, C.; Leineweber, C.; Moghaddassi, M.; Stengård, J.; Westerlund, H.; Östergren, P.-O. The negative effects on mental health of being in a non-desired occupation in an increasingly precarious labour market. SSM Popul. Health 2017, 3, 516–524. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Questions | Answer Alternatives | ||||
|---|---|---|---|---|---|
| a | b | c | d | ||
| 1 | Are you currently working in a profession that you believe is right for you? | Yes | No | - | - |
| 2 | Are you working at a workplace that is right for you? | Yes | No | - | - |
| 3 | How do you view your possibility to change job? | Very good | Good | Poor | Very poor |
| Variable | All, n (%) | Preferred Work, n (%) | Non-Preferred Work, High Possibility to Change, n (%) | Non-Preferred Work, Low Possibility to Change, n (%) |
|---|---|---|---|---|
| All | 4285 (100) | 3462 (80.8) | 476 (11.1) | 347 (8.1) |
| Women | 2298 (53.6) | 1829 (79.6) | 272 (11.8) | 197 (8.6) |
| Age, mean (SD) | 46 (10) | 47 (10) | 39 (10) | 48 (10) |
| Country of birth | ||||
| Sweden | 3739 (87.6) | 3059 (81.8) | 418 (11.2) | 262 (7.0) |
| Elsewhere | 527 (12.4) | 391 (74.2) | 52 (9.9) | 84 (15.9) |
| Socioeconomic status a | ||||
| Blue-collar workers | 943 (22.7) | 737 (78.2) | 108 (11.4) | 98 (10.4) |
| White-collar workers | 3069 (74.1) | 2495 (81.3) | 345 (11.2) | 230 (7.5) |
| Self-employed/unclassified | 131 (3.2) | 113 (86.3) | 11 (8.4) | 7 (5.3) |
| Sleep disturbance | 1220 (28.5) | 950 (77.9) | 133 (10.9) | 137 (11.2) |
| Alcohol consumption past 12 months | ||||
| Never | 205 (4.8) | 156 (76.1) | 27 (13.2) | 22 (10.7) |
| >1–4 times/month | 2441 (57.2) | 1946 (79.7) | 300 (12.3) | 195 (8.0) |
| ≥2 times/week | 1623 (38.0) | 1346 (82.9) | 148 (9.2) | 129 (8.0) |
| Exercise past 12 months | ||||
| <1 h/week | 1539 (36.2) | 1259 (81.8) | 149 (9.7) | 131 (8.5) |
| 1–2 h/week | 1287 (30.3) | 1045 (81.2) | 141 (11.0) | 101 (7.8) |
| 2–3 h/week | 755 (17.8) | 598 (79.2) | 97 (12.8) | 60 (7.9) |
| >3 h/week | 671 (15.8) | 535 (79.7) | 86 (12.8) | 50 (7.5) |
| Long-term illness | 747 (17.7) | 586 (78.5) | 85 (11.4) | 76 (10.2) |
| Working hours | ||||
| >45 h/week | 746 (18.4) | 650 (87.1) | 48 (6.4) | 48 (6.4) |
| 36–45 h/week | 2650 (65.3) | 2116 (79.9) | 315 (11.9) | 219 (8.3) |
| 20–35 h/week | 553 (13.6) | 437 (79.0) | 63 (11.4) | 53 (9.6) |
| 1–19 h/week | 82 (2.0) | 51 (62.2) | 23 (28.1) | 8 (9.8) |
| Other working hours | 28 (0.7) | 22 (78.6) | 4 (14.3) | 2 (7.1) |
| Household work past 12 months | ||||
| <1 h/day | 1283 (30.0) | 1024 (79.8) | 152 (11.9) | 107 (8.3) |
| 1–2 h/day | 2065 (48.3) | 1676 (81.2) | 231 (11.2) | 158 (7.7) |
| >2 h/day | 931 (21.7) | 756 (81.2) | 93 (9.9) | 82 (8.8) |
| Outcomes | Cases/Total | Crude RR (95% CI) | Adjusted RR a (95% CI) |
|---|---|---|---|
| Spinal pain | |||
| Preferred work | 146/3414 | 1 | 1 |
| Non-preferred work, high possibility to change | 27/472 | 1.3 (0.9–2.0) | 1.4 (0.9–2.1) |
| Non-preferred work, low possibility to change | 26/342 | 1.8 (1.2–2.7) | 1.8 (1.2–2.6) |
| Psychological distress | |||
| Preferred work | 309/3375 | 1 | 1 |
| Non-preferred work, high possibility to change | 71/460 | 1.7 (1.3–2.1) | 1.3 (1.0–1.7) |
| Non-preferred work, low possibility to change | 54/330 | 1.8 (1.4–2.3) | 1.8 (1.4–2.4) |
| Spinal pain and psychological distress | |||
| Preferred work | 27/3331 | 1 | |
| Non-preferred work | 12/784 | 1.9 (1.0–3.7) |
| Outcomes | No Sleep Disturbance | Sleep Disturbance | ||||
|---|---|---|---|---|---|---|
| Cases/ Total | Crude RR (95% CI) | Adjusted RR a (95% CI) | Cases/Total | Crude RR (95% CI) | Adjusted RR a (95% CI) | |
| Spinal pain | ||||||
| Preferred work | 80/2473 | 1 | 1 | 65/935 | 1 | 1 |
| Non-preferred work | 31/547 | 1.8 (1.2–2.6) | 1.8 (1.2–2.7) | 22/264 | 1.2 (0.8–1.9) | 1.2 (0.8–2.0) |
| Psychological distress | ||||||
| Preferred work | 207/2444 | 1 | 1 | 102/925 | 1 | 1 |
| Non-preferred work | 78/535 | 1.7 (1.3–2.2) | 1.5 (1.1–1.9) | 46/252 | 1.7 (1.2–2.3) | 1.5 (1.1–2.0) |
| Spinal pain and psychological distress | ||||||
| Preferred work | 15/2415 | 1 | 12/910 | 1 | ||
| Non-preferred work | 6/533 | 1.8 (0.7–4.6) | 6/248 | 1.8 (0.7–4.8) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skillgate, E.; Isacson Hjortzberg, M.; Strömwall, P.; Hallqvist, J.; Onell, C.; Holm, L.W.; Bohman, T. Non-Preferred Work and the Incidence of Spinal Pain and Psychological Distress—A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 10051. https://doi.org/10.3390/ijerph181910051
Skillgate E, Isacson Hjortzberg M, Strömwall P, Hallqvist J, Onell C, Holm LW, Bohman T. Non-Preferred Work and the Incidence of Spinal Pain and Psychological Distress—A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(19):10051. https://doi.org/10.3390/ijerph181910051
Chicago/Turabian StyleSkillgate, Eva, My Isacson Hjortzberg, Petra Strömwall, Johan Hallqvist, Clara Onell, Lena W. Holm, and Tony Bohman. 2021. "Non-Preferred Work and the Incidence of Spinal Pain and Psychological Distress—A Prospective Cohort Study" International Journal of Environmental Research and Public Health 18, no. 19: 10051. https://doi.org/10.3390/ijerph181910051