
Clinical Outcomes and Oral Health-Related Quality of Life after Periodontal Treatment with Community Health Worker Strategy in Patients with Type 2 Diabetes: A Randomized Controlled Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Randomization and Blinding
2.3. Outcome Measures
2.3.1. Periodontal Index
2.3.2. Glycated Hemoglobin
2.3.3. OHQoL
2.3.4. Oral Self-Care Behaviors
2.3.5. Oral Health-Related Knowledge
2.3.6. Attitude toward Periodontal Health
2.4. Covariates
2.5. CHWs Recruitment and Training
2.6. Intervention
2.7. Data Collection
2.8. Statistical Analysis
3. Results
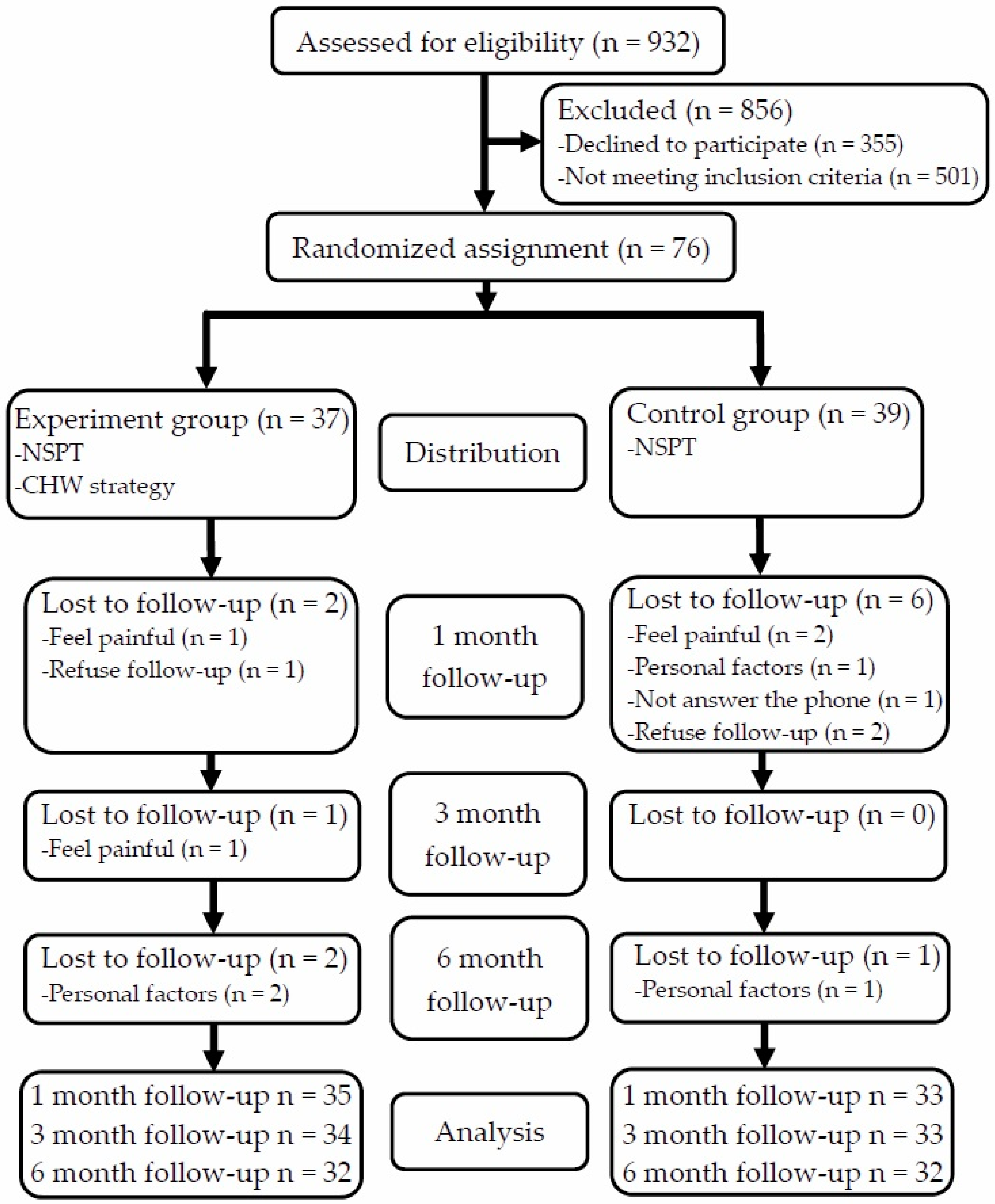
3.1. Recruitment
3.2. Baseline Information between the Two Groups
3.3. Intervention Effects on Knowledge, Attitude, and Behaviors
3.4. Intervention Effects on Periodontal Parameters
3.5. Intervention Effects on OHQoL and HbA1c
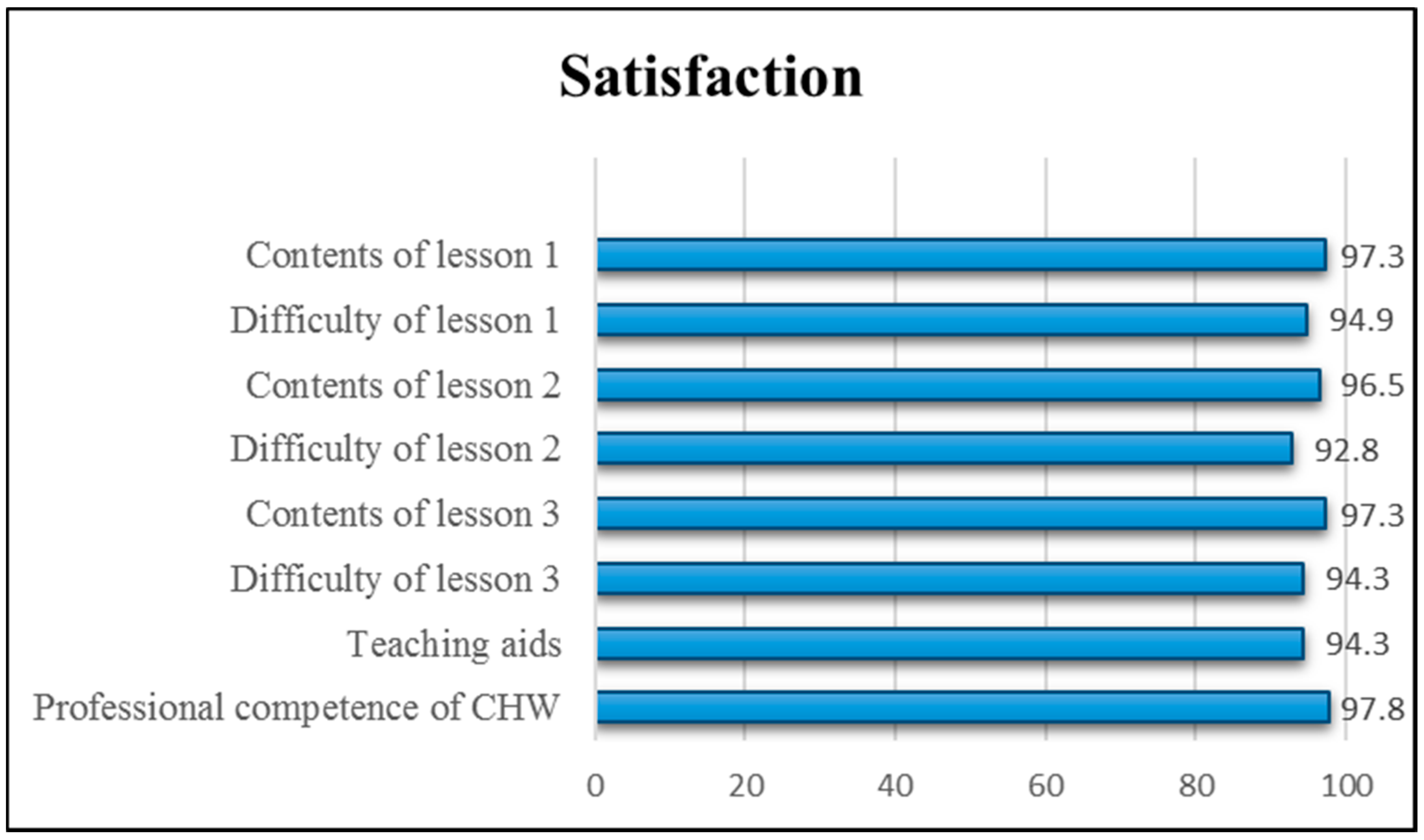
3.6. Satisfaction Survey of the Intervention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sheen, Y.J.; Hsu, C.C.; Jiang, Y.D.; Huang, C.N.; Liu, J.S.; Sheu, W.H. Trends in prevalence and incidence of diabetes mellitus from 2005 to 2014 in Taiwan. J. Formos. Med. Assoc. 2019, 118 (Suppl. 2), S66–S73. [Google Scholar] [CrossRef]
- Grossi, S.G.; Genco, R.J. Periodontal disease and diabetes mellitus: A two-way relationship. Ann. Periodontol. 1998, 3, 51–61. [Google Scholar] [CrossRef]
- Mealey, B.L.; Oates, T.W.; American Academy of, P. Diabetes mellitus and periodontal diseases. J. Periodontol. 2006, 77, 1289–1303. [Google Scholar] [CrossRef]
- Noack, B.; Genco, R.J.; Trevisan, M.; Grossi, S.; Zambon, J.J.; De Nardin, E. Periodontal infections contribute to elevated systemic C-reactive protein level. J. Periodontol. 2001, 72, 1221–1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salman, S.; Khan, K.; Salman, F.; Hameed, M. Effect of Non-Surgical Periodontal Treatment on Glycemic Control among Type 2 Diabetes Mellitus Patients with Periodontitis. J. Ayub Med. Coll. Abbottabad 2016, 28, 442–445. [Google Scholar] [PubMed]
- Li, Q.; Hao, S.; Fang, J.; Xie, J.; Kong, X.H.; Yang, J.X. Effect of non-surgical periodontal treatment on glycemic control of patients with diabetes: A meta-analysis of randomized controlled trials. Trials 2015, 16, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsobgny-Tsague, N.-F.; Lontchi-Yimagou, E.; Nana, A.R.N.; Tankeu, A.T.; Katte, J.C.; Dehayem, M.Y.; Bengondo, C.M.; Sobngwi, E. Effects of nonsurgical periodontal treatment on glycated haemoglobin on type 2 diabetes patients (PARODIA 1 study): A randomized controlled trial in a sub-Saharan Africa population. BMC Oral Health 2018, 18, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiran, M.; Arpak, N.; Unsal, E.; Erdogan, M.F. The effect of improved periodontal health on metabolic control in type 2 diabetes mellitus. J. Clin. Periodontol. 2005, 32, 266–272. [Google Scholar] [CrossRef]
- Katagiri, S.; Nitta, H.; Nagasawa, T.; Uchimura, I.; Izumiyama, H.; Inagaki, K.; Kikuchi, T.; Noguchi, T.; Kanazawa, M.; Matsuo, A.; et al. Multi-center intervention study on glycohemoglobin (HbA1c) and serum, high-sensitivity CRP (hs-CRP) after local anti-infectious periodontal treatment in type 2 diabetic patients with periodontal disease. Diabetes Res. Clin. Pract. 2009, 83, 308–315. [Google Scholar] [CrossRef]
- Koromantzos, P.A.; Makrilakis, K.; Dereka, X.; Katsilambros, N.; Vrotsos, I.A.; Madianos, P.N. A randomized, controlled trial on the effect of non-surgical periodontal therapy in patients with type 2 diabetes. Part I: Effect on periodontal status and glycaemic control. J. Clin. Periodontol. 2011, 38, 142–147. [Google Scholar] [CrossRef]
- Hsu, Y.J.; Lin, K.D.; Chen, J.H.; Lee, M.Y.; Lin, Y.C.; Yen, F.C.; Huang, H.L. Periodontal Treatment Experience Associated with Oral Health-Related Quality of Life in Patients with Poor Glycemic Control in Type 2 Diabetes: A Case-Control Study. Int. J. Environ. Res. Public Health 2019, 16, 4011. [Google Scholar] [CrossRef] [Green Version]
- Shanmukappa, S.M.; Nadig, P.; Puttannavar, R.; Ambareen, Z.; Gowda, T.M.; Mehta, D.S. Knowledge, Attitude, and Awareness among Diabetic Patients in Davangere about the Association between Diabetes and Periodontal Disease. J. Int. Soc. Prev. Community Dent. 2017, 7, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Al Habashneh, R.; Khader, Y.; Hammad, M.M.; Almuradi, M. Knowledge and awareness about diabetes and periodontal health among Jordanians. J. Diabetes Complicat. 2010, 24, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Olaniran, A.; Smith, H.; Unkels, R.; Bar-Zeev, S.; van den Broek, N. Who is a community health worker?—A systematic review of definitions. Glob. Health Action 2017, 10, 1272223. [Google Scholar] [CrossRef] [Green Version]
- Scott, K.; Beckham, S.W.; Gross, M.; Pariyo, G.; Rao, K.D.; Cometto, G.; Perry, H.B. What do we know about community-based health worker programs? A systematic review of existing reviews on community health workers. Hum. Resour. Health 2018, 16, 39. [Google Scholar] [CrossRef]
- Lee, H.; Ho, P.S.; Wang, W.C.; Hu, C.Y.; Lee, C.H.; Huang, H.L. Effectiveness of a health belief model intervention using a lay health advisor strategy on mouth self-examination and cancer screening in remote aboriginal communities: A randomized controlled trial. Patient Educ. Couns. 2019, 102, 2263–2269. [Google Scholar] [CrossRef]
- Hughes, M.M.; Yang, E.; Ramanathan, D.; Benjamins, M.R. Community-Based Diabetes Community Health Worker Intervention in an Underserved Chicago Population. J. Community Health 2016, 41, 1249–1256. [Google Scholar] [CrossRef]
- Ursua, R.A.; Aguilar, D.E.; Wyatt, L.C.; Katigbak, C.; Islam, N.S.; Tandon, S.D.; Nur, P.R.; Van Devanter, N.; Rey, M.J.; Trinh-Shevrin, C. A community health worker intervention to improve management of hypertension among Filipino Americans in New York and New Jersey: A pilot study. Ethn. Dis. 2014, 24, 67–76. [Google Scholar] [PubMed]
- Egbujie, B.A.; Delobelle, P.A.; Levitt, N.; Puoane, T.; Sanders, D.; van Wyk, B. Role of community health workers in type 2 diabetes mellitus self-management: A scoping review. PLoS ONE 2018, 13, e0198424. [Google Scholar] [CrossRef] [PubMed]
- Spencer, M.S.; Kieffer, E.C.; Sinco, B.; Piatt, G.; Palmisano, G.; Hawkins, J.; Lebron, A.; Espitia, N.; Tang, T.; Funnell, M.; et al. Outcomes at 18 Months From a Community Health Worker and Peer Leader Diabetes Self-Management Program for Latino Adults. Diabetes Care 2018, 41, 1414–1422. [Google Scholar] [CrossRef] [Green Version]
- Kane, E.P.; Collinsworth, A.W.; Schmidt, K.L.; Brown, R.M.; Snead, C.A.; Barnes, S.A.; Fleming, N.S.; Walton, J.W. Improving diabetes care and outcomes with community health workers. Fam. Pract. 2016, 33, 523–528. [Google Scholar] [CrossRef] [Green Version]
- Brown, H.S., 3rd; Wilson, K.J.; Pagan, J.A.; Arcari, C.M.; Martinez, M.; Smith, K.; Reininger, B. Cost-effectiveness analysis of a community health worker intervention for low-income Hispanic adults with diabetes. Prev. Chronic Dis. 2012, 9, E140. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Diabetes and Oral Health Problems. Available online: http://archives.diabetes.org/living-with-diabetes/treatment-and-care/oral-health-and-hygiene/diabetes-and-oral-health.html (accessed on 6 July 2021).
- Shibayama, T.; Kudoh, R.; Hidaka, K. Factors associated with the practice of periodontal management by diabetes educator nurses for outpatients with diabetes: A nationwide survey in Japan. Prim. Care Diabetes 2021, in press. [Google Scholar]
- Peretz, P.J.; Islam, N.; Matiz, L.A. Community Health Workers and Covid-19—Addressing Social Determinants of Health in Times of Crisis and Beyond. N. Engl. J. Med. 2020, 383, e108. [Google Scholar] [CrossRef]
- Sweeting, L.A.; Davis, K.; Cobb, C.M. Periodontal Treatment Protocol (PTP) for the general dental practice. J. Dent. Hyg. 2008, 82 (Suppl. 3), 16–26. [Google Scholar] [PubMed]
- Kotrlik, J.; Williams, H. The incorporation of effect size in information technology, learning, information technology, learning, and performance research and performance research. Inf. Technol. Learn. Perform. J. 2003, 21, 1. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Loe, H.; Silness, J. Periodontal Disease in Pregnancy. I. Prevalence and Severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef]
- Silness, J.; Loe, H. Periodontal Disease in Pregnancy. Ii. Correlation between Oral Hygiene and Periodontal Condtion. Acta Odontol. Scand. 1964, 22, 121–135. [Google Scholar] [CrossRef]
- Nathan, D.M.; Turgeon, H.; Regan, S. Relationship between glycated haemoglobin levels and mean glucose levels over time. Diabetologia 2007, 50, 2239–2244. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D.; Group, C. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Goel, K.; Baral, D. A Comparison of Impact of Chronic Periodontal Diseases and Nonsurgical Periodontal Therapy on Oral Health-Related Quality of Life. Int. J. Dent. 2017, 2017, 9352562. [Google Scholar] [CrossRef] [Green Version]
- Wong, R.M.; Ng, S.K.; Corbet, E.F.; Keung Leung, W. Non-surgical periodontal therapy improves oral health-related quality of life. J. Clin. Periodontol. 2012, 39, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Saito, A.; Hosaka, Y.; Kikuchi, M.; Akamatsu, M.; Fukaya, C.; Matsumoto, S.; Ueshima, F.; Hayakawa, H.; Fujinami, K.; Nakagawa, T. Effect of initial periodontal therapy on oral health-related quality of life in patients with periodontitis in Japan. J. Periodontol. 2010, 81, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Yuen, H.K.; Onicescu, G.; Hill, E.G.; Jenkins, C. A survey of oral health education provided by certified diabetes educators. Diabetes Res. Clin. Pract. 2010, 88, 48–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashkenazi, M.; Kessler-Baruch, O.; Levin, L. Oral hygiene instructions provided by dental hygienists: Results from a self-report cohort study and a suggested protocol for oral hygiene education. Quintessence Int. 2014, 45, 265–269. [Google Scholar] [PubMed]
- Kawamura, M.; Tsurumoto, A.; Fukuda, S.; Sasahara, H. Health behaviors and their relation to metabolic control and periodontal status in type 2 diabetic patients: A model tested using a linear structural relations program. J. Periodontol. 2001, 72, 1246–1253. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, R.I.; Horwitz, S.M. Adherence to treatment and health outcomes. Arch. Intern. Med. 1993, 153, 1863–1868. [Google Scholar] [CrossRef]
- Martin, L.R.; Williams, S.L.; Haskard, K.B.; Dimatteo, M.R. The challenge of patient adherence. Ther. Clin. Risk Manag. 2005, 1, 189–199. [Google Scholar]
- Engebretson, S.P.; Hyman, L.G.; Michalowicz, B.S.; Schoenfeld, E.R.; Gelato, M.C.; Hou, W.; Seaquist, E.R.; Reddy, M.S.; Lewis, C.E.; Oates, T.W.; et al. The effect of nonsurgical periodontal therapy on hemoglobin A1c levels in persons with type 2 diabetes and chronic periodontitis: A randomized clinical trial. JAMA 2013, 310, 2523–2532. [Google Scholar] [CrossRef] [Green Version]
- Simpson, T.C.; Weldon, J.C.; Worthington, H.V.; Needleman, I.; Wild, S.H.; Moles, D.R.; Stevenson, B.; Furness, S.; Iheozor-Ejiofor, Z. Treatment of periodontal disease for glycaemic control in people with diabetes mellitus. Cochrane Database Syst. Rev. 2015, CD004714. [Google Scholar] [CrossRef]
- Chen, Y.F.; Zhan, Q.; Wu, C.Z.; Yuan, Y.H.; Chen, W.; Yu, F.Y.; Li, Y.; Li, L.J. Baseline HbA1c Level Influences the Effect of Periodontal Therapy on Glycemic Control in People with Type 2 Diabetes and Periodontitis: A Systematic Review on Randomized Controlled Trails. Diabetes Ther. 2021, 12, 1249–1278. [Google Scholar] [CrossRef] [PubMed]
- Nathan, D.M.; Buse, J.B.; Davidson, M.B.; Ferrannini, E.; Holman, R.R.; Sherwin, R.; Zinman, B.; American Diabetes, A.; European Association for Study of, D. Medical management of hyperglycemia in type 2 diabetes: A consensus algorithm for the initiation and adjustment of therapy: A consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2009, 32, 193–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| EG (n = 35) | CG (n = 33) | ||||
|---|---|---|---|---|---|
| N | % | N | % | p | |
| Gender | |||||
| Male | 18 | (51.4) | 22 | (66.7) | 0.202 |
| Female | 17 | (48.6) | 11 | (33.3) | |
| Age, mean ± SD † | 54.7 ± 6.1 | 54.8 ± 6.9 | 0.932 | ||
| Duration of diabetes (year) | |||||
| <5 | 16 | 48.5 | 12 | 36.4 | 0.273 |
| 5–10 | 10 | 30.3 | 8 | 24.2 | |
| >10 | 7 | 21.2 | 13 | 39.4 | |
| Baseline HbA1c(%), mean ± SD † | 6.9 ± 1.3 | 6.9 ± 1.2 | 0.969 | ||
| BMI (kg/m2), mean ± SD † | 27.1 ± 4.5 | 26.9 ± 4.2 | 0.826 | ||
| Education level | |||||
| Less than junior high school | 7 | 20.0 | 6 | 18.2 | 0.976 |
| High school | 17 | 48.6 | 16 | 48.5 | |
| College and above | 11 | 31.4 | 11 | 33.3 | |
| Drinking | |||||
| Yes | 5 | 14.3 | 6 | 18.2 | 0.663 |
| No | 30 | 85.7 | 27 | 81.8 | |
| Betel nut chewing | |||||
| Yes | 2 | 5.7 | 1 | 3.0 | 0.590 |
| No | 33 | 97.3 | 32 | 97.0 | |
| Smoking | |||||
| Yes | 5 | 14.3 | 6 | 18.2 | 0.663 |
| No | 30 | 85.7 | 27 | 81.8 | |
| Self-perceived oral health status | |||||
| Very good/Good | 8 | 22.9 | 4 | 12.1 | 0.172 |
| Common | 20 | 57.1 | 16 | 48.5 | |
| Very poor/Poor | 7 | 20.0 | 13 | 39.4 | |
| EG (n = 35) | CG (n = 33) | ||||||
|---|---|---|---|---|---|---|---|
| Diff ± SD † | Diff ± SD † | Effect Size d | β/aOR | (95% CI) | |||
| Oral health-related knowledge (0–13) | |||||||
| Group (EG) × Time (second) | 5.6 ± 2.8 | 0.9 ± 2.4 | 1.82 | 4.5 | (3.42, 5.54) | ||
| Group (EG) × Time (third) | 5.8 ± 2.8 | 2.2 ± 2.5 | 1.36 | 3.4 | (2.05, 4.66) | ||
| Group (EG) × Time (fourth) | 6.1 ± 2.7 | 2.4 ± 2.4 | 1.44 | 3.5 | (2.04, 4.89) | ||
| Effect size a | 2.02 | 0.39 | |||||
| Effect size b | 2.09 | 0.85 | |||||
| Effect size c | 2.25 | 0.98 | |||||
| Attitude toward periodontal health (7–35) | |||||||
| Group (EG) × Time (second) | 4.8 ± 3.5 | 1.5 ± 2.9 | 1.02 | 3.2 | (1.58, 4.75) | ||
| Group (EG) × Time (third) | 5.4 ± 3.9 | 1.7 ± 3.0 | 1.05 | 3.6 | (1.66, 5.45) | ||
| Group (EG) × Time (fourth) | 5.7 ± 3.7 | 2.8 ± 3.8 | 0.79 | 3.0 | (1.01, 5.08) | ||
| Effect size a | 1.40 | 0.52 | |||||
| Effect size b | 1.39 | 0.57 | |||||
| Effect size c | 1.55 | 0.73 | |||||
| Oral self–care behaviors | |||||||
| Use modified Bass brushing technique (n, %) ‡ | |||||||
| Group (EG) × Time (second) | 23 | 65.7 | 7 | 21.2 | 12.2 | (2.31, 64.98) | |
| Group (EG) × Time (third) | 23 | 67.7 | 15 | 45.5 | 11.6 | (1.15, 116.64) | |
| Group (EG) × Time (fourth) | 20 | 62.5 | 13 | 40.6 | 7.2 | (0.98, 53.32) | |
| Use interdental brush (n, %) ‡ | |||||||
| Group (EG) × Time (second) | 19 | 54.3 | 8 | 24.2 | 4.1 | (1.02, 16.29) | |
| Group (EG) × Time (third) | 18 | 52.9 | 11 | 33.3 | 1.9 | (0.36, 9.90) | |
| Group (EG) × Time (fourth) | 14 | 43.8 | 10 | 31.3 | 1.2 | (0.20, 6.98) | |
| EG (n = 35) | CG (n = 33) | ||||
|---|---|---|---|---|---|
| Diff ± SD † | Diff ± SD † | Effect Size d | β | (95% CI) | |
| PPD | |||||
| Group (EG) × Time (second) | −0.5 ± 0.4 | −0.2 ± 0.3 | 0.61 | −0.2 | (−0.41, −0.08) |
| Group (EG) × Time (third) | −0.5 ± 0.5 | −0.4 ± 0.4 | 0.22 | −0.1 | (−0.34, 0.07) |
| Group (EG) × Time (fourth) | −0.4 ± 0.5 | −0.3 ± 0.5 | 0.18 | −0.1 | (−0.36, 0.11) |
| Effect size a | 1.19 | 0.73 | |||
| Effect size b | 0.94 | 0.85 | |||
| Effect size c | 0.80 | 0.67 | |||
| CAL | |||||
| Group (EG) × Time (second) | −0.4 ± 0.4 | −0.1 ± 0.3 | 0.59 | −0.2 | (−0.39, −0.06) |
| Group (EG) × Time (third) | −0.3 ± 0.4 | −0.2 ± 0.4 | 0.14 | −0.1 | (−0.30, 0.14) |
| Group (EG) × Time (fourth) | −0.3 ± 0.5 | −0.2 ± 0.5 | 0.15 | −0.1 | (−0.37, 0.16) |
| Effect size a | 0.89 | 0.41 | |||
| Effect size b | 0.69 | 0.55 | |||
| Effect size c | 0.59 | 0.43 | |||
| GI | |||||
| Group (EG) × Time (second) | −0.8 ± 0.5 | −0.8 ± 0.8 | 0.01 | 0.0 | (−0.27, 0.30) |
| Group (EG) × Time (third) | −0.9 ± 0.7 | −1.1 ± 0.6 | 0.30 | 0.2 | (−0.16, 0.50) |
| Group (EG) × Time (fourth) | −0.8 ± 0.8 | −1.0 ± 0.8 | 0.22 | 0.2 | (−0.17, 0.51) |
| Effect size a | 1.56 | 1.05 | |||
| Effect size b | 1.24 | 1.67 | |||
| Effect size c | 1.03 | 1.22 | |||
| PI | |||||
| Group (EG) × Time (second) | −0.6 ± 0.6 | −0.8 ± 0.8 | 0.24 | 0.2 | (−0.12, 0.46) |
| Group (EG) × Time (third) | −0.7 ± 0.7 | −1.0 ± 0.9 | 0.44 | 0.3 | (−0.04, 0.63) |
| Group (EG) × Time (fourth) | −0.7 ± 0.7 | −1.0 ± 0.8 | 0.32 | 0.2 | (−0.14, 0.58) |
| Effect size a | 1.07 | 0.98 | |||
| Effect size b | 0.93 | 1.17 | |||
| Effect size c | 0.92 | 1.17 | |||
| BOP (%) | |||||
| Group (EG) × Time (second) | −26.5 ± 19.5 | −20.5 ± 26.0 | 0.26 | −5.7 | (−15.98, 3.88) |
| Group (EG) × Time (third) | −29.5 ± 23.0 | −28.7 ± 26.4 | 0.03 | −1.6 | (−12.66, 9.47) |
| Group (EG) × Time (fourth) | −30.4 ± 26.9 | −26.1 ± 29.8 | 0.15 | −0.3 | (−12.04, 11.35) |
| Effect size a | 1.36 | 0.79 | |||
| Effect size b | 1.28 | 1.09 | |||
| Effect size c | 1.13 | 0.88 |
| EG (n = 35) | CG (n = 33) | ||||
|---|---|---|---|---|---|
| Diff ± SD † | Diff ± SD † | Effect Size d | β | (95% CI) | |
| Oral health-related quality of life | |||||
| Group (EG) × Time (second) | −0.9 ± 4.5 | −4.0 ± 6.5 | 0.56 | 3.2 | (0.90, 5.46) |
| Group (EG) × Time (third) | −2.9 ± 4.8 | −4.1 ± 6.1 | 0.22 | 1.2 | (−1.70, 4.07) |
| Group (EG) × Time (fourth) | −3.2 ± 5.2 | −4.3 ± 6.5 | 0.19 | 1.0 | (−2.29, 4.19) |
| Effect size a | 0.19 | 0.62 | |||
| Effect size b | 0.60 | 0.67 | |||
| Effect size c | 0.62 | 0.67 | |||
| HbA1c | |||||
| Group (EG) × Time (third) | −0.1 ± 1.1 | −0.1 ± 0.8 | 0.02 | 0.1 | (−0.64, 0.83) |
| Group (EG) × Time (fourth) | 0.1 ± 1.1 | 0.1 ± 0.4 | 0.04 | 0.2 | (−0.67, 1.07) |
| Effect size b | 0.07 | 0.12 | |||
| Effect size c | 0.09 | 0.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, Y.-J.; Chen, Y.-H.; Lin, K.-D.; Lee, M.-Y.; Lee, Y.-L.; Yu, C.-K.; Kabasawa, Y.; Huang, H.-L. Clinical Outcomes and Oral Health-Related Quality of Life after Periodontal Treatment with Community Health Worker Strategy in Patients with Type 2 Diabetes: A Randomized Controlled Study. Int. J. Environ. Res. Public Health 2021, 18, 8371. https://doi.org/10.3390/ijerph18168371
Hsu Y-J, Chen Y-H, Lin K-D, Lee M-Y, Lee Y-L, Yu C-K, Kabasawa Y, Huang H-L. Clinical Outcomes and Oral Health-Related Quality of Life after Periodontal Treatment with Community Health Worker Strategy in Patients with Type 2 Diabetes: A Randomized Controlled Study. International Journal of Environmental Research and Public Health. 2021; 18(16):8371. https://doi.org/10.3390/ijerph18168371
Chicago/Turabian StyleHsu, Yuan-Jung, Yi-Hui Chen, Kun-Der Lin, Mei-Yueh Lee, Yu-Li Lee, Chih-Kai Yu, Yuji Kabasawa, and Hsiao-Ling Huang. 2021. "Clinical Outcomes and Oral Health-Related Quality of Life after Periodontal Treatment with Community Health Worker Strategy in Patients with Type 2 Diabetes: A Randomized Controlled Study" International Journal of Environmental Research and Public Health 18, no. 16: 8371. https://doi.org/10.3390/ijerph18168371