
The Effect of Magnesium Supplementation on Endothelial Function: A Randomised Cross-Over Pilot Study



Abstract
:1. Introduction
2. Methods
2.1. Subject Recruitment
2.2. Study Design
2.3. Weight and Height
2.4. Dietary Intake
2.5. Blood Pressure
2.6. FMD
2.7. FMD Analysis
2.8. Laboratory Analysis
2.9. Ethics
2.10. Statistical Analysis
3. Results
3.1. Effect of Supplementation on Magnesium Status
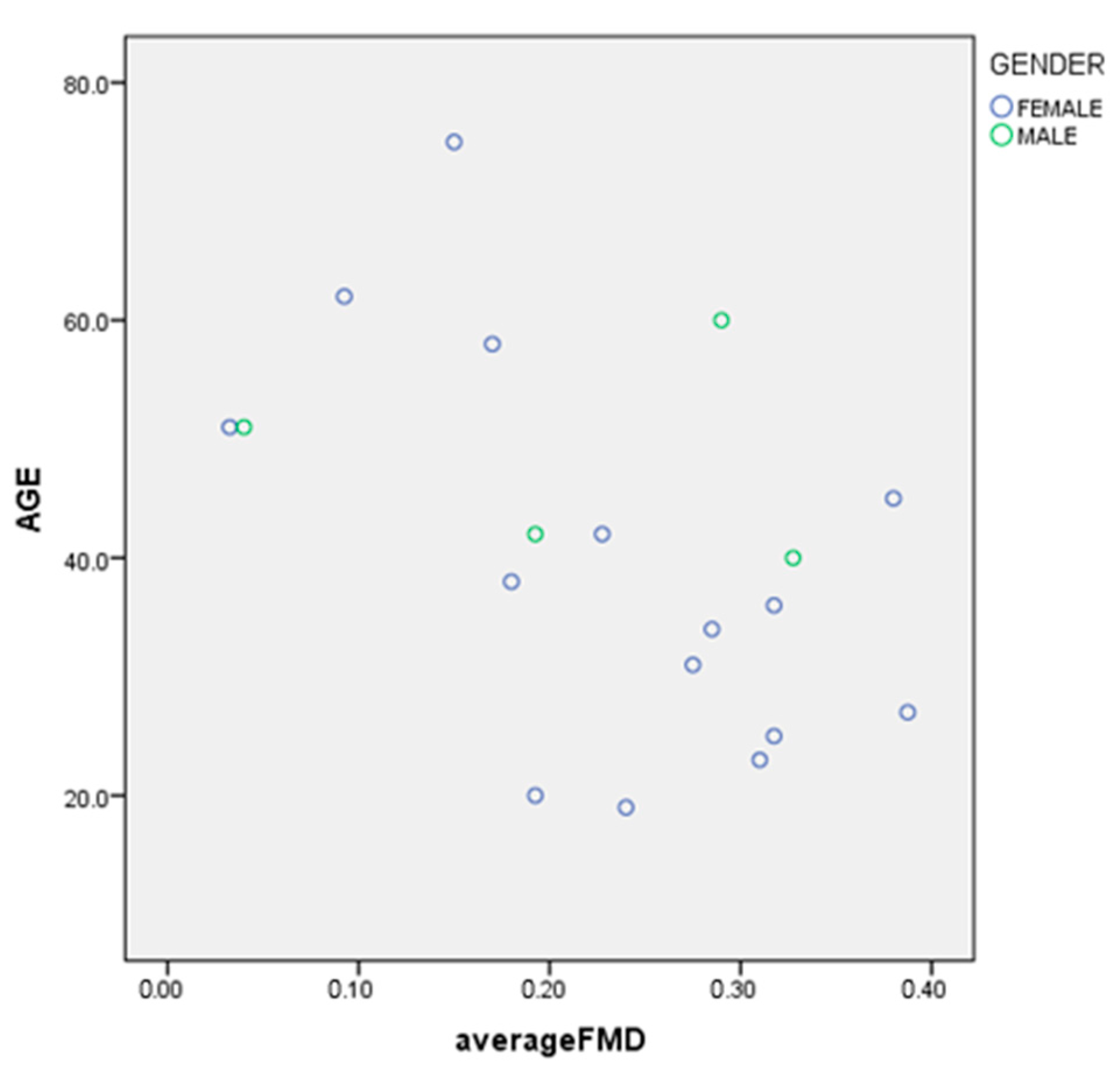
3.2. Primary and Secondary Endpoints
| Correlation Coefficient | −0.496 |
| Significance | p = 0.031 |
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, W.; Iso, H.; Ohira, T.; Date, C.; Tamakoshi, A. Associations of dietary magnesium intake with mortality from cardiovascular disease: The JACC study. Atherosclerosis 2012, 221, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; He, P.; Chen, J.; Liu, Y.; Liu, D.; Qin, G.; Tan, N. Magnesium Levels in Drinking Water and Coronary Heart Disease Mortality Risk: A Meta-Analysis. Nutrients 2016, 8, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiuve, S.E.; Sun, Q.; Curhan, G.C.; Taylor, E.N.; Spiegelman, D.; Willett, W.C.; Manson, J.E.; Rexrode, K.M.; Albert, C.M. Dietary and plasma magnesium and risk of coronary heart disease among women. J. Am. Heart Assoc. 2013, 2, e000114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Delaimy, W.K.; Rimm, E.B.; Willett, W.C.; Stampfer, M.J.; Hu, F.B. Magnesium Intake and Risk of Coronary Heart Disease among Men. J. Am. Coll. Nutr. 2004, 23, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Abbott, R.D.; Ando, F.; Masaki, K.H.; Tung, K.H.; Rodriguez, B.L.; Petrovitch, H.; Yano, K.; Curb, J.D. Dietary magnesium intake and the future risk of coronary heart disease (the Honolulu Heart Program). Am. J. Cardiol. 2003, 92, 665–669. [Google Scholar] [CrossRef]
- Song, Y.; Manson, J.E.; Cook, N.R.; Albert, C.M.; Buring, J.E.; Liu, S. Dietary magnesium intake and risk of cardiovascular disease among women. Am. J. Cardiol. 2005, 96, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Liao, F.; Folsom, A.R.; Brancati, F.L. Is low magnesium concentration a risk factor for coronary heart disease? The Atherosclerosis Risk in Communities (ARIC) Study. Am. Heart J. 1998, 136, 480–490. [Google Scholar] [CrossRef]
- Kieboom, B.C.T.; Niemeijer, M.N.; Leening, M.J.G.; van den Berg, M.E.; Franco, O.H.; Deckers, J.W.; Hofman, A.; Zietse, R.; Stricker, B.H.; Hoorn, E.J. Serum Magnesium and the Risk of Death From Coronary Heart Disease and Sudden Cardiac Death. J. Am. Heart Assoc. 2016, 5, e002707. [Google Scholar] [CrossRef] [Green Version]
- Joosten, M.M.; Gansevoort, R.T.; Mukamal, K.J.; van der Harst, P.; Geleijnse, J.M.; Feskens, E.J.; Navis, G.; Bakker, S.J.; Group, P.S. Urinary and plasma magnesium and risk of ischemic heart disease. Am. J. Clin. Nutr. 2013, 97, 1299–1306. [Google Scholar] [CrossRef] [Green Version]
- Ford, E.S. Serum magnesium and ischaemic heart disease: Findings from a national sample of US adults. Int. J. Epidemiol. 1999, 28, 645–651. [Google Scholar] [CrossRef]
- Kanbay, M.; Yilmaz, M.I.; Apetrii, M.; Saglam, M.; Yaman, H.; Unal, H.U.; Gok, M.; Caglar, K.; Oguz, Y.; Yenicesu, M.; et al. Relationship between serum magnesium levels and cardiovascular events in chronic kidney disease patients. Am. J. Nephrol. 2012, 36, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Jahnen-Dechent, W.; Ketteler, M. Magnesium basics. Clin. Kidney J. 2012, 5, i3–i14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.; Li, T.Y.; van Dam, R.M.; Manson, J.E.; Hu, F.B. Magnesium intake and plasma concentrations of markers of systemic inflammation and endothelial dysfunction in women. Am. J. Clin. Nutr. 2007, 85, 1068–1074. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Garcia, E.; Schulze, M.B.; Fung, T.T.; Meigs, J.B.; Rifai, N.; Manson, J.E.; Hu, F.B. Major dietary patterns are related to plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2004, 80, 1029–1035. [Google Scholar] [CrossRef] [Green Version]
- Chacko, S.A.; Song, Y.; Nathan, L.; Tinker, L.; de Boer, I.H.; Tylavsky, F.; Wallace, R.; Liu, S. Relations of dietary magnesium intake to biomarkers of inflammation and endothelial dysfunction in an ethnically diverse cohort of postmenopausal women. Diabetes Care 2010, 33, 304–310. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Ryu, J.-H.; Kim, S.-J.; Ryu, D.-R.; Kang, D.-H.; Choi, K.B. The Relationship between Magnesium and Endothelial Function in End-Stage Renal Disease Patients on Hemodialysis. Yonsei Med. J. 2016, 57, 1446–1453. [Google Scholar] [CrossRef]
- Davignon, J.; Ganz, P. Role of endothelial dysfunction in atherosclerosis. Circulation 2004, 109, III27–III32. [Google Scholar] [CrossRef] [Green Version]
- Ras, R.T.; Streppel, M.T.; Draijer, R.; Zock, P.L. Flow-mediated dilation and cardiovascular risk prediction: A systematic review with meta-analysis. Int. J. Cardiol. 2013, 168, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Shechter, M.; Sharir, M.; Labrador, M.J.; Forrester, J.; Silver, B.; Bairey Merz, C.N. Oral magnesium therapy improves endothelial function in patients with coronary artery disease. Circulation 2000, 102, 2353–2358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbagallo, M.; Dominguez, L.J.; Galioto, A.; Pineo, A.; Belvedere, M. Oral magnesium supplementation improves vascular function in elderly diabetic patients. Magnes. Res. 2010, 23, 131–137. [Google Scholar] [CrossRef]
- Cosaro, E.; Bonafini, S.; Montagnana, M.; Danese, E.; Trettene, M.S.; Minuz, P.; Delva, P.; Fava, C. Effects of magnesium supplements on blood pressure, endothelial function and metabolic parameters in healthy young men with a family history of metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 1213–1220. [Google Scholar] [CrossRef] [PubMed]
- Joris, P.J.; Plat, J.; Bakker, S.J.L.; Mensink, R.P. Effects of long-term magnesium supplementation on endothelial function and cardiometabolic risk markers: A randomized controlled trial in overweight/obese adults. Sci. Rep. 2017, 7, 106. [Google Scholar] [CrossRef]
- Cunha, A.R.; D’El-Rei, J.; Medeiros, F.; Umbelino, B.; Oigman, W.; Touyz, R.M.; Neves, M.F. Oral magnesium supplementation improves endothelial function and attenuates subclinical atherosclerosis in thiazide-treated hypertensive women. J. Hypertens. 2017, 35, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Mortazavi, M.; Moeinzadeh, F.; Saadatnia, M.; Shahidi, S.; McGee, J.C.; Minagar, A. Effect of magnesium supplementation on carotid intima-media thickness and flow-mediated dilatation among hemodialysis patients: A double-blind, randomized, placebo-controlled trial. Eur. Neurol. 2013, 69, 309–316. [Google Scholar] [CrossRef]
- Australian National Health and Medical Research Council. Magnesium|Nutrient Reference Values. Available online: https://www.nrv.gov.au/nutrients/magnesium (accessed on 13 February 2017).
- Harris, R.A.; Nishiyama, S.K.; Wray, D.W.; Richardson, R.S. Ultrasound Assessment of Flow-Mediated Dilation. Hypertension 2010, 55, 1075–1085. [Google Scholar] [CrossRef]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Kizhakekuttu, T.J.; Gutterman, D.D.; Phillips, S.A.; Jurva, J.W.; Arthur, E.I.; Das, E.; Widlansky, M.E. Measuring FMD in the brachial artery: How important is QRS gating? J. Appl. Physiol. 2010, 109, 959–965. [Google Scholar] [CrossRef]
- Blanch, N.; Clifton, P.M.; Petersen, K.S.; Willoughby, S.R.; Keogh, J.B. Effect of high potassium diet on endothelial function. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 983–989. [Google Scholar] [CrossRef]
- St. James’s Hospital. Laboratory Medicine: Creatiine. Available online: http://search.stjames.ie/sjhservlet/Record.jsp?li=2&rf=as (accessed on 13 February 2017).
- Verma, H.; Garg, R. Effect of magnesium supplementation on type 2 diabetes associated cardiovascular risk factors: A systematic review and meta-analysis. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2017. [Google Scholar] [CrossRef] [PubMed]
- Kass, L.; Weekes, J.; Carpenter, L. Effect of magnesium supplementation on blood pressure: A meta-analysis. Eur. J. Clin. Nutr. 2012, 66, 411–418. [Google Scholar] [CrossRef]
- Dickinson, H.O.; Nicolson, D.; Campbell, F.; Cook, J.V.; Beyer, F.R.; Ford, G.A.; Mason, J. Magnesium supplementation for the management of primary hypertension in adults. Cochrane Database Syst. Rev. 2006. [Google Scholar] [CrossRef]
- Joris, P.J.; Plat, J.; Bakker, S.J.; Mensink, R.P. Long-term magnesium supplementation improves arterial stiffness in overweight and obese adults: Results of a randomized, double-blind, placebo-controlled intervention trial. Am. J. Clin. Nutr. 2016, 103, 1260–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosanoff, A.; Plesset, M.R. Oral magnesium supplements decrease high blood pressure (SBP>155 mmHg) in hypertensive subjects on anti-hypertensive medications: A targeted meta-analysis. Magnes. Res. 2013, 26, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Suárez-Cuenca, J.A.; De La Peña-Sosa, G.; De La Vega-Moreno, K.; Zaineff Banderas-Lares, D.; Salamanca-García, M.; Martínez-Hernández, J.E.; Vera-Gómez, E.; Hernández-Patricio, A.; Zamora-Alemán, C.R.; Domínguez-Pérez, G.A.; et al. Enlarged adipocytes from subcutaneous vs. visceral adipose tissue differentially contribute to metabolic dysfunction and atherogenic risk of patients with obesity. Sci. Rep. 2021, 11, 1831. [Google Scholar] [CrossRef] [PubMed]
- Keogh, J.B.; Grieger, J.A.; Noakes, M.; Clifton, P.M. Flow-Mediated Dilatation Is Impaired by a High–Saturated Fat Diet but Not by a High-Carbohydrate Diet. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1274–1279. [Google Scholar] [CrossRef] [Green Version]
- Fuentes, F.; López-Miranda, J.; Sánchez, E.; Sánchez, F.; Paez, J.; Paz-Rojas, E.; Marín, C.; Gómez, P.; Jimenez, F.F.; Ordovás, J.M.; et al. Mediterranean and low-fat diets improve endothelial function in hypercholesterolemic men. Ann. Intern. Med. 2001, 134, 1115–1119. [Google Scholar] [CrossRef]
- Dickinson, K.M.; Clifton, P.M.; Keogh, J.B. A reduction of 3 g/day from a usual 9 g/day salt diet improves endothelial function and decreases endothelin-1 in a randomised cross_over study in normotensive overweight and obese subjects. Atherosclerosis 2014, 233, 32–38. [Google Scholar] [CrossRef]
- Marques, B.; Klein, M.; da Cunha, M.R.; de Souza Mattos, S.; de Paula Nogueira, L.; de Paula, T.; Correa, F.M.; Oigman, W.; Neves, M.F. Effects of Oral Magnesium Supplementation on Vascular Function: A Systematic Review and Meta-analysis of Randomized Controlled Trials. High Blood Press. Cardiovasc. Prev. 2020, 27, 19–28. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Minimum | Maximum | Mean/Median | SD/IQR | |
|---|---|---|---|---|
| Age (years) | 19 | 75 | 39 | 16.04 |
| Weight (kg) | 45.04 | 98.51 | 59.3 (median) | 14.40 (IQR) |
| BMI (kg/m2) | 17.9 | 31.7 | 21.2 (median) | 5.59 (IQR) |
| SBP(mmHg) | 93 | 120 | 109 | 7.29 |
| DBP (mmHg) | 55 | 80 | 67 | 7.30 |
| MAP | 66 | 93 | 77 | 7.17 |
| Serum Mg (mmol/L) | 0.76 | 0.94 | 0.85 | 0.05 |
| Urinary Mg (mmol/24 h) | 2.03 | 5.23 | 3.23 (median) | 1.33 (IQR) |
| Urinary Cr (mmol/24 h) | 3.64 | 20 | 8.82 (median) | 3.19 (IQR) |
| Mg/Cr Ratio | 0.19 | 0.70 | 0.38 (median) | 0.17 (IQR) |
| Dietary Intake mg/day (mmol/day) | Minimum | Maximum | Mean/Median | Std. Deviation/IQR |
|---|---|---|---|---|
| Mg intake | 138 (5.68) | 510 (20.99) | 339 (13.95) | 106.75 |
| Male Mg intake (N = 4) | 199 (8.19) | 429 (17.65) | 328 (13.50) | 51.03 |
| Female Mg intake (N = 15) | 138 (5.68) | 510 (20.99) | 343 (14.12) | 97.76 |
| Overall Ca intake | 328 | 1808 | 782 (median) | 580 (IQR) |
| Male Ca intake | 416 | 1242 | 1170 (median) | 649 (IQR) |
| Female Ca intake | 328 | 1808 | 726 (median) | 447 (IQR) |
| Ca/Mg Ratio | 0.92 | 5.26 | 2.21 (median) | 1.74 (IQR) |
| Sodium | 769 | 4409 | 1672 (median) | 730 (IQR) |
| Potassium | 1325 | 4388 | 2887 | 790 |
| Saturated fat (% energy) | 5.44 | 18.17 | 11.55 | 3.26 |
| PUFA fat (% energy) | 1.94 | 8.64 | 5.33 | 2.04 |
| Serum Mg mmol/L (SD) | Urinary Mg mmol/24 (SD) | Urinary Mg/Cr Ratio | Urinary Cr Excretion mmol/24 h(SD) | |
|---|---|---|---|---|
| N = 19 | ||||
| Control | 0.85 (0.05) | 3.39 (0.86) | 0.3936 (0.13) | 9.34 (3.56) |
| Intervention | 0.86 (0.05) | 4.26 (1.65) | 0.4868 (0.10) | 8.84 (3.05) |
| Significance | p = 0.19 | p = 0.064 | p = 0.009 | p = 0.059 |
| N = 17 | ||||
| Control | 0.085 (0.05) | 3.51 (0.86) | 0.3655 (0.11) | 10.13 (3.37) |
| Intervention | 0.087 (0.06) | 4.48 (1.61) | 0.4729 (0.09) | 9.41 (2.68) |
| Significance | p = 0.2 | p = 0.03 | p = 0.005 | p = 0.102 |
| Change in FMD (mm) (SD) | Percent Change in FMD (%) (SD) | SBP (mmHg) (SD) | DBP (mmHg) (SD) | MAP (mmHg) (SD) | |
|---|---|---|---|---|---|
| Control | 0.24 (0.11) | 6.77 (3.38) | 109 (7.16) | 66 (7.00) | 76 (6.49) |
| Intervention | 0.22 (0.12) | 6.21 (3.83) | 110 (8.70) | 66 (7.53) | 76 (7.40) |
| Significance | p = 0.3 | p = 0.4 | p = 0.5 | p = 0.3 | p = 0.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byrne, J.; Murphy, C.; Keogh, J.B.; Clifton, P.M. The Effect of Magnesium Supplementation on Endothelial Function: A Randomised Cross-Over Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 8169. https://doi.org/10.3390/ijerph18158169
Byrne J, Murphy C, Keogh JB, Clifton PM. The Effect of Magnesium Supplementation on Endothelial Function: A Randomised Cross-Over Pilot Study. International Journal of Environmental Research and Public Health. 2021; 18(15):8169. https://doi.org/10.3390/ijerph18158169
Chicago/Turabian StyleByrne, Jennifer, Caitríona Murphy, Jennifer B. Keogh, and Peter M. Clifton. 2021. "The Effect of Magnesium Supplementation on Endothelial Function: A Randomised Cross-Over Pilot Study" International Journal of Environmental Research and Public Health 18, no. 15: 8169. https://doi.org/10.3390/ijerph18158169