
Effectiveness of the Functional and Cognitive Occupational Therapy (FaCoT) Intervention for Improving Daily Functioning and Participation of Individuals with Mild Stroke: A Randomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
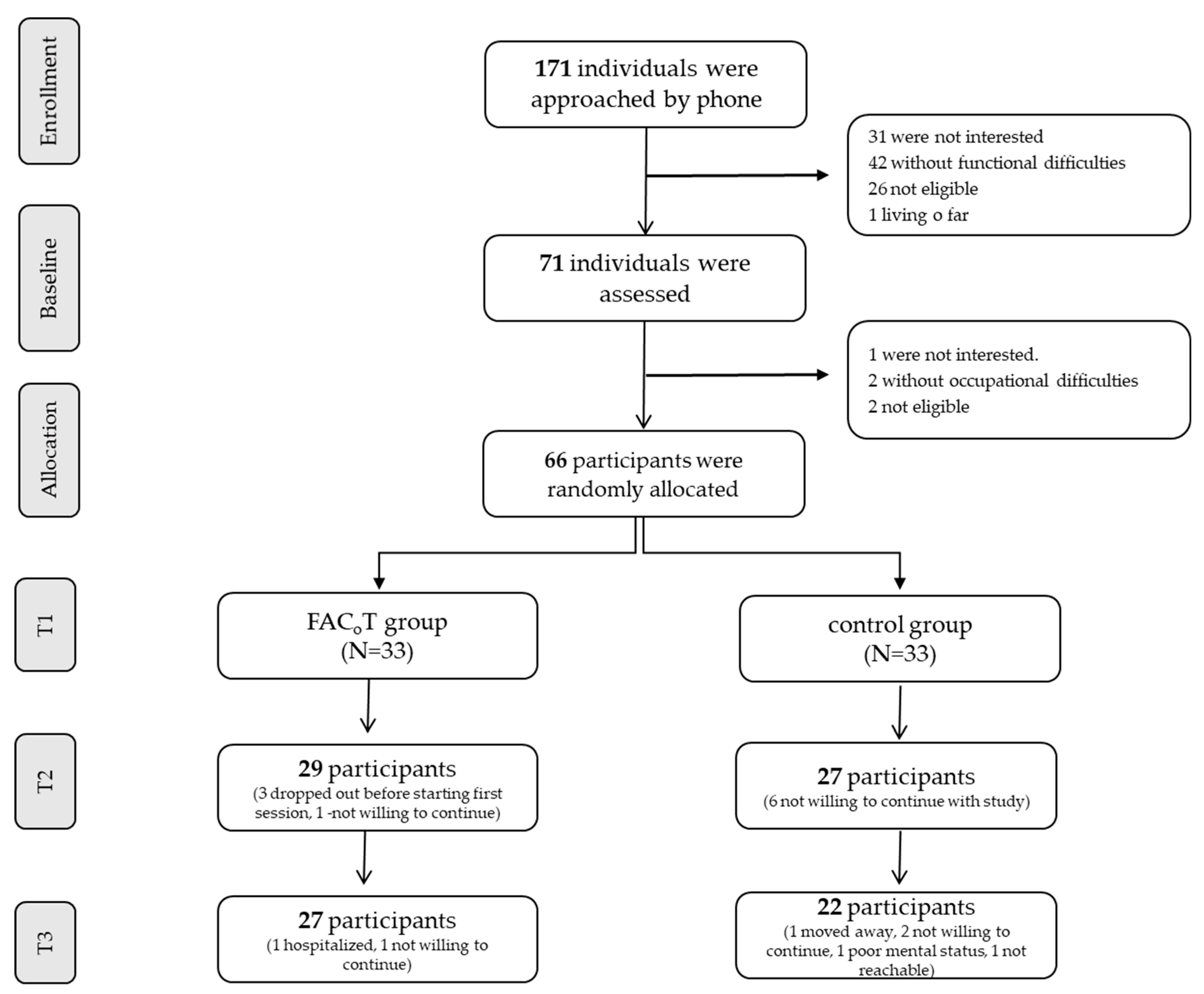
2.1. Participants
2.2. Randomization
2.3. Outcome Measures
2.4. Intervention
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Adams, H.P.; Leclerc, J.R.; Bluhmki, E.; Clarke, W.; Hansen, M.D.; Hacke, W. Measuring outcomes as a function of baseline severity of ischemic stroke. Cerebrovasc. Dis. 2004, 18, 124–129. [Google Scholar] [CrossRef]
- Carlsson, G.E.; Möller, A.; Blomstrand, C. Consequences of mild stroke in persons. Cerebrovasc. Dis. 2003, 16, 383–388. [Google Scholar] [CrossRef]
- Duncan, P.W.; Samsa, G.P.; Weinberger, M.; Goldstein, L.B.; Bonito, A.; Witter, D.M.; Enarson, C.; Matchar, D. Health status of individuals with mild stroke. Stroke 1997, 28, 740–745. [Google Scholar] [CrossRef] [PubMed]
- Terrill, A.L.; Schwartz, J.K.; Belagaje, S.R. Best Practices for The Interdisciplinary Rehabilitation Team: A Review of Mental Health Issues in Mild Stroke Survivors. Stroke Res. Treat. 2018, 2018, 1–8. [Google Scholar] [CrossRef]
- Della Vecchia, C.; Préau, M.; Carpentier, C.; Viprey, M.; Haesebaert, J.; Termoz, A.; Dima, A.L.; Schott, A.-M. Illness beliefs and emotional responses in mildly disabled stroke survivors: A qualitative study. PLoS ONE 2019, 14, e0223681. [Google Scholar] [CrossRef] [Green Version]
- Johansson, A.; Mishina, E.; Ivanov, A.; Björklund, A. Activities of daily living among St Petersburg women after mild stroke. Occup. Ther. Int. 2007, 14, 170–182. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health (ICF); World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Reed, K.; Hocking, C.; Smythe, L. The interconnected meanings of occupation: The call, being-with, possibilities. J. Occup. Sci. 2010, 17, 140–149. [Google Scholar] [CrossRef]
- Edwards, D.F.; Hahn, M.; Baum, C.; Dromerick, A.W. The Impact of Mild Stroke on Meaningful Activity and Life Satisfaction. J. Stroke Cerebrovasc. Dis. 2006, 15, 151–157. [Google Scholar] [CrossRef]
- Rochette, A.; Desrosiers, J.; Bravo, G.; St-Cyr-Tribble, D.; Bourget, A. Changes in Participation after a Mild Stroke: Quantitative and Qualitative Perspectives. Top. Stroke Rehabil. 2007, 14, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Muren, M.A.; Hütler, M.; Hooper, J. Functional Capacity and Health-Related Quality of Life in Individuals Post Stroke. Top. Stroke Rehabil. 2008, 15, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Muus, I.; Petzold, M.; Ringsberg, K.C. Health-related quality of life among Danish patients 3 and 12 months after TIA or mild stroke. Scand. J. Caring Sci. 2010, 24, 211–218. [Google Scholar] [CrossRef]
- Carlsson, G.E.; Möller, A.; Blomstrand, C. A qualitative study of the consequences of ’hidden dysfunctions’ one year after a mild stroke in persons <75 years. Disabil. Rehabil. 2004, 26, 1373–1380. [Google Scholar] [CrossRef]
- Jaillard, A.; Naegele, B.; Trabucco-Miguel, S.; LeBas, J.F.; Hommel, M. Hidden Dysfunctioning in Subacute Stroke. Stroke 2009, 40, 2473–2479. [Google Scholar] [CrossRef] [Green Version]
- Srikanth, V.K.; Thrift, A.; Saling, M.M.; Anderson, J.; Dewey, H.M.; MacDonell, R.A.; Donnan, G. Increased Risk of Cognitive Impairment 3 Months After Mild to Moderate First-Ever Stroke. Stroke 2003, 34, 1136–1143. [Google Scholar] [CrossRef]
- Lezak, M.D.; Howieson, D.B.; Bigler, E.D.; Tranel, D. Basic concept. In Neuropsychological Assessment, 5th ed.; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Jones, F.; Riazi, A. Self-efficacy and self-management after stroke: A systematic review. Disabil. Rehabil. 2011, 33, 797–810. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Korpershoek, C.; Van Der Bijl, J.; Hafsteinsdóttir, T.B. Self-efficacy and its influence on recovery of patients with stroke: A systematic review. J. Adv. Nurs. 2011, 67, 1876–1894. [Google Scholar] [CrossRef] [PubMed]
- Lewin, A.; Jöbges, M.; Werheid, K. The influence of self-efficacy, pre-stroke depression and perceived social support on self-reported depressive symptoms during stroke rehabilitation. Neuropsychol. Rehabil. 2013, 23, 546–562. [Google Scholar] [CrossRef]
- Rees, L.; Marshall, S.; Hartridge, C.; Mackie, D.; Weiser, M. Cognitive interventions post acquired brain injury. Brain Inj. 2007, 21, 161–200. [Google Scholar] [CrossRef] [PubMed]
- Rohilng, M.; Faust, M.E.; Beverly, B.; Demakis, G. Effectiveness of cognitive rehabilitation following acquired brain injury; a meta-analytic re-examination of cicerone et al.’s (2000, 2005) systematic reviews. Neuropsychology 2009, 23, 20–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Heugten, C.; Gregorio, G.W.; Wade, D. Evidence-based cognitive rehabilitation after acquired brain injury: A systematic review of content of treatment. Neuropsychol. Rehabil. 2012, 22, 653–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toglia, J.P. Generalization of treatment: A mulicontextual approach to cognitive perceptual impairment in the brain injured adult. Am. J. Occup. Ther. 1991, 45, 505–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polatajko, H.J.; McEwen, S.E.; Ryan, J.D.; Baum, C.M. Pilot randomized controlled trail investigating cognitive strategy use to improve goal performance after stroke. Am. J. Occup. Ther. 2012, 66, 104–109. [Google Scholar] [CrossRef] [Green Version]
- Toglia, J.P.; Rodger, S.Y.; Polatajko, H.J. Anatomy of cognitive strategies: A therapist’s primer for enabling occupational performance. Can. J. Occup. Ther. 2012, 79, 225–236. [Google Scholar] [CrossRef]
- Toglia, J.P.; Goverover, Y.; Johnston, M.V.; Dain, B. Application of the mulicontextual approach in promoting learning and transfer of strategy use in an individual with TBI and executive dysfunction. OTJR Occup. Particip. Health 2011, 31, S53–S60. [Google Scholar] [CrossRef]
- Baum, C.M.; Christiansen, C.H.; Bass, J.D. The Person-Environment-Occupation-Performance (PEOP) model. In Occupational Therapy: Performance, Participation, and Well-Being, 4th ed.; Christiansen, C.H., Baum, C.M., Bass, J.D., Eds.; SLACK Incorporated: Thorofare, NJ, USA, 2015. [Google Scholar]
- Polatajko, H.A.; Townsend, E.A.; Craik, J. Canadian model of occupational performance and engagement (CMOP-E). In Enabling Occupation II: Advancing an Occupational Therapy Vision for Health, Well-Being, & Justice through Occupation; Townsend, E.A., Pola-tajko, H.J., Eds.; CAOT Publications ACE: Ottawa, ON, Canada, 2007. [Google Scholar]
- Duncan, J. Attention, intelligence and the frontal lobes. In The Cognitive Neurosciences; Gazzanniga, M.S., Ed.; MIT Press: Cambridge, MA, USA, 1995. [Google Scholar]
- Norman, D.A.; Shallice, T. Attention to Action: Willed and Automatic Control of Behavior. In Consciousness and Self-Regulation: Advances in Research and Theory; Davidson, R.J., Schwartz, G.E., Shapiro, D., Eds.; Plenum Press: New York, NY, USA, 1986. [Google Scholar]
- Bandura, A. Self-Efficacy. In Social Foundations of Thought and Action: A Social Cognitive Theory; Bandura, A., Ed.; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Adamit, T.; Maeir, A.; Ben Assayag, E.; Bornstein, N.M.; Korczyn, A.D.; Katz, N. Impact of first-ever mild stroke on participation at 3 and 6 month post-event: The TABASCO study. Disabil. Rehabil. 2014, 37, 667–673. [Google Scholar] [CrossRef]
- Fride, Y.; Adamit, T.; Maeir, A.; Ben Assayag, E.; Bornstein, N.M.; Korczyn, A.D.; Katz, N. What are the correlates of cognition and participation to return to work after first ever mild stroke? Top. Stroke Rehabil. 2015, 22, 317–325. [Google Scholar] [CrossRef]
- Moher, D.; Schulz, K.F.; Altman, D.G. The CONSORT statement: Revised recommendations for improving the quality of reports of parallel-group randomised trails. Lancet 2001, 357, 1191–1194. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Update guidelines for reporting parallel group randomised trials. Trails 2010, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, A.S.; Be´dirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.; Gildeh, N.; Holmes, C. The Montreal Cognitive Assessment: Validity and Utility in a Memory Clinic Setting. Can. J. Psychiatry 2007, 52, 329–332. [Google Scholar] [CrossRef]
- Reeves, M.; Lisabeth, L.; Williams, L.; Katzan, I.; Kapral, M.; Deutsch, A.; Prvu-Bettger, J. Patient-Reported Outcome Measures (PROMs) for Acute Stroke: Rationale, Methods and Future Directions. Stroke 2018, 49, 1549–1556. [Google Scholar] [CrossRef]
- Law, M.; Baptiste, S.; McColl, M.; Opzoomer, A.; Polatajko, H.; Pollock, N. The Canadian Occupational Performance Measure: An Outcome Measure for Occupational Therapy. Can. J. Occup. Ther. 1990, 57, 82–87. [Google Scholar] [CrossRef]
- Bosomworth, H.; Rodgers, H.; Shaw, L.; Smith, L.; Aird, L.; Howel, D.; Wilson, N.; Alvarado, N.; Andole, S.; Cohen, D.L.; et al. Evaluation of the enhanced upeer limb therapy programme within the ROBOT-Assisted Training for the Upper-Limb after Stroke trail: Descriptive analysis of intervention fidelity, goal selection and goal achievement. Clin. Rehabil. 2020, 35, 119–134. [Google Scholar] [CrossRef] [PubMed]
- Cup, E.H.C.; Scholte op Reimer, W.J.M.; Thijssen, M.C.E.; van Kuyk-Minis, M.A.H. Reliability and validity of the Canadian occupational per-formance measure in stroke patients. Clin. Rehabil. 2003, 17, 402–409. [Google Scholar] [CrossRef]
- Wressle, E.; Samuelsson, K.; Henriksson, C. Responsiveness of the Swedish Version of the Canadian Occupational Performance Measure. Scand. J. Occup. Ther. 1999, 6, 84–89. [Google Scholar] [CrossRef]
- Wood-Dauphinee, S.L.; Opzoomer, M.A.; Williams, J.I.; Marchand, B.; Spitzer, W.O. Assessment of global function: The Reintegration to Normal Living Index. Arch. Phys. Med. Rehabil. 1988, 69, 583–590. [Google Scholar] [PubMed]
- Tooth, L.; McKenna, K.; Smith, M.; O’Rourke, P. Reliability of scores between stroke patients and significant others on the Reintegration to Normal Living (RNL) Index. Disabil. Rehabil. 2003, 25, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Pang, M.Y.C.; Lau, R.W.K.; Yeung, P.K.C.; Liao, L.-R.; Chung, R.C.K. Development and validation of the Chinese version of the Reintegration to Normal Living Index for use with stroke patients. J. Rehabil. Med. 2011, 43, 243–250. [Google Scholar] [CrossRef] [Green Version]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Suijker, J.J.; Van Rijn, M.; ter Riet, G.; Van Charante, E.P.M.; De Rooij, S.E.; Buurman, B.M. Minimal important change and minimal detectable change in activities of daily living in community-living older people. J. Nutr. Health Aging 2016, 21, 165–172. [Google Scholar] [CrossRef]
- Miles, J.; Shevlin, M. Applying Regression and Correlation: A Guide for Students and Researchers; SAGE: London, UK, 2001. [Google Scholar]
- Gupta, S.K. Intention-to-treat concept: A review. Perspect. Clin. Res. 2011, 2, 109–112. [Google Scholar] [CrossRef]
- Tellier, M.; Rochette, A. Falling Through the Cracks: A Literature Review to Understand the Reality of Mild Stroke Survivors. Top. Stroke Rehabil. 2009, 16, 454–462. [Google Scholar] [CrossRef]
- Long, Y.; Ouyang, R.G.; Zhang, J.Q. Effects of virtual reality training on occupational performance and self-efficacy of patients with stroke: A randomized controlled trial. J. NeuroEng. Rehabil. 2020, 17, 150. [Google Scholar] [CrossRef]
- Poulin, V.; Korner-Bitensky, N.; Bherer, L.; Lussier, M.; Dawson, D.R. Comparison of tow cognitive interventions for adults experiencing executive dysfunction post-stroke: A pilot study. Disabil. Rehabil. 2017, 39, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Henshaw, E.; Polatajko, H.; McEwen, S.; Ryan, J.D.; Baum, C.M. Cognitive approach to improving participation after stroke: Tow case studies. Am. J. Occup. Ther. 2011, 65, 55–63. [Google Scholar] [CrossRef] [Green Version]
- McEwen, S.E.; Polatajko, H.J.; Huijbregts, M.P.J.; Ryan, J.D. Exploring a cognitive-based treatment approach to improve motor-based skill performance in chronic stroke: Results of three single case experiments. Brain Inj. 2009, 23, 1041–1053. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, M.; Vaughan, B. Commentary: Statistical significance and clinical significance—A call to consider patient reported outcome measures, effect size, confidence interval and minimal clinically important difference (MCID). J. Bodyw. Mov. Ther. 2019, 23, 690–694. [Google Scholar] [CrossRef] [PubMed]
- Malec, J.F.; Ketchum, J.M. A Standard Method for Determining the Minimal Clinically Important Difference for Rehabilitation Measures. Arch. Phys. Med. Rehabil. 2020, 101, 1090–1094. [Google Scholar] [CrossRef] [PubMed]
- Schelly, D.; Ohl, A. Examining clinical meaningfulness in randomized controlled trails: Revisiting the well elderly II. Am. J. Occup. Ther. 2019, 73, 7301205120p1–7301205120p13. [Google Scholar] [CrossRef] [Green Version]
- Salter, K.L.; Foley, N.C.; Jutai, J.; Teasell, R.W. Assessment of participation outcomes in randomized controlled trials of stroke rehabilitation interventions. Int. J. Rehabil. Res. 2007, 30, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, A.; Lanctot, K.L.; Bayley, M.; Kiss, A.; Herrmann, N.; Murray, B.J.; Swartz, R.H. “Good outcome” isn’t good enough. Stroke 2017, 48, 1688–1690. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| FaCoT Group (n = 33) | Control Group (n = 33) | Differences between Groups | |
|---|---|---|---|
| Mean (SD) Min–Max | Mean (SD) Min–Max | t-Test t(p) * | |
| Age (years) | 64.6 (8.2) 49–77 | 64.4 (10.8) 48–84 | 0.1 (0.9) |
| Education (years) | 12.1 (1.9) 8–16 | 12.9 (2.8) 6–20 | −1.2 (0.2) |
| NIHSS (0–46) | 1.2 (1.2) 0–4 | 1.7 (1.6) 0–6 | −1.4 (0.2) |
| FIM (18–126) | 118.8 (7.2) 98–126 | 117.2 (7.1) 96–126 | 0.9 (0.4) |
| MoCA (0–30) | 21.5 (3.9) 11–29 | 21.8 (4.1) 14–28 | 0.2 (0.8) |
| n (%) | n (%) | Chi-square χ2 (p) | |
| Sex F | 11 (33.3) | 15 (45.5) | 1.0 (0.3) |
| First stroke | 20 (60.6) | 19 (57.6) | 0.1 (0.8) |
| Stroke side R/L | 13/18 (39.4/54.5) | 14/16 (42.4/48.5) | 0.14 (0.7) |
| Type of stroke—ischemic/hemorrhage | 32/0 (100/0) | 31/2 (93.9/6.1) | 2.0 (0.2) |
| Lesion—cortical/subcortical | 9/17 (27.3/51.5) | 8/19 (24.2/57.6) | 0.09 (0.8) |
| Chronic stage | 28 (84.8) | 26 (78.8) | 0.4 (0.5) |
| Received Inpatient rehabilitation | 5 (15.2) | 8 (24.2) | 0.87 (0.3) |
| Received Outpatient rehabilitation | 13 (39.4) | 9 (27.3) | 0.32 (0.6) |
| Returned to work since stroke (Participants who worked prior to the stroke) | 55% (n = 11/20) | 31% (n = 4/13) | 1.87 (0.2) |
| FaCoT Group (n = 33) Mean (SD) Min–Max | Control Group (n = 33) Mean (SD) Min–Max | Time X Group Effect | |||||||
|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T1 | T2 | T3 | F (df) | p | Partial Eta² | |
| COPM performance (0–10) | 3.1 (1.3) 1–5 | 6.0 (2.2) 2–10 | 6.2 (2.4) 1–10 | 3.7 (1.3) 0–8 | 4.7 (2.3) 1–10 | 4.7 (2.3) 0–10 | 11.75 (1.4, 90.3) | 0.000 | 0.15 |
| COPM satisfaction (0–10) | 2.4 (1.3) 1–6 | 5.9 (2.3) 1–10 | 6.4 (2.6) 1–10 | 3.1 (2.1) 0–9 | 4.1 (2.5) 1–10 | 4.4 (2.5) 0–10 | 15.70 (1.5, 96.8) | 0.000 | 0.20 |
| IADLq (0–23) | 17.7 (4.7) 8–23 | 19.6 (4.2) 7–23 | 19.6 (4.8) 7–23 | 17.6 (18.4) 6–23 | 18.4 (4.4) 7–23 | 18.3 (4.0) 7–23 | 1.21 (1.6, 103.6) | 0.3000 | 0.02 |
| RNL (0–100) | 72.1 (14.5) 43–100 | 80.8 (18.2) 20–100 | 79.9 (13.9) 54–100 | 64.2 (21.1) 20–100 | 66.2 (18.8) 25–95 | 64.9 (19.5) 27–100 | 2.60 (1.8, 114.3) | 0.078 | 0.04 |
| FaCoT Group (n = 33) Mean (SD) | Control Group (n = 33) Mean (SD) | |||
|---|---|---|---|---|
| % Change T1–T2 | % Change T1–T3 | % Change T1–T2 | % Change T1–T3 | |
| COPM performance | 138.6 (144.9) | 153.2 170.9) | 39.7 (124.6) | 53.0 (133.5) |
| COPM satisfaction | 207.4 (205.8) | 241.0 (248.4) | 55.6 (127.2) | 88.4 (161.9) |
| IADLq | 15.3 (29.8) | 15.0 (32.7) | 13.5 (51.4) | 11.2 (940.3) |
| RNL | 12.6 (22.2) | 13.7 (24.1) | 7.3 (25.6) | 6.9 (32.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adamit, T.; Shames, J.; Rand, D. Effectiveness of the Functional and Cognitive Occupational Therapy (FaCoT) Intervention for Improving Daily Functioning and Participation of Individuals with Mild Stroke: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 7988. https://doi.org/10.3390/ijerph18157988
Adamit T, Shames J, Rand D. Effectiveness of the Functional and Cognitive Occupational Therapy (FaCoT) Intervention for Improving Daily Functioning and Participation of Individuals with Mild Stroke: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(15):7988. https://doi.org/10.3390/ijerph18157988
Chicago/Turabian StyleAdamit, Tal, Jeffrey Shames, and Debbie Rand. 2021. "Effectiveness of the Functional and Cognitive Occupational Therapy (FaCoT) Intervention for Improving Daily Functioning and Participation of Individuals with Mild Stroke: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 15: 7988. https://doi.org/10.3390/ijerph18157988