
Long-Term Exposure to Fine and Coarse Particulate Matter and COVID-19 Incidence and Mortality Rate in Chile during 2020

 , ,
, ,
Abstract
:1. Background
2. Materials and Methods
2.1. Study Design and Population
2.2. Variables and Sources of Information
2.2.1. Health Variables
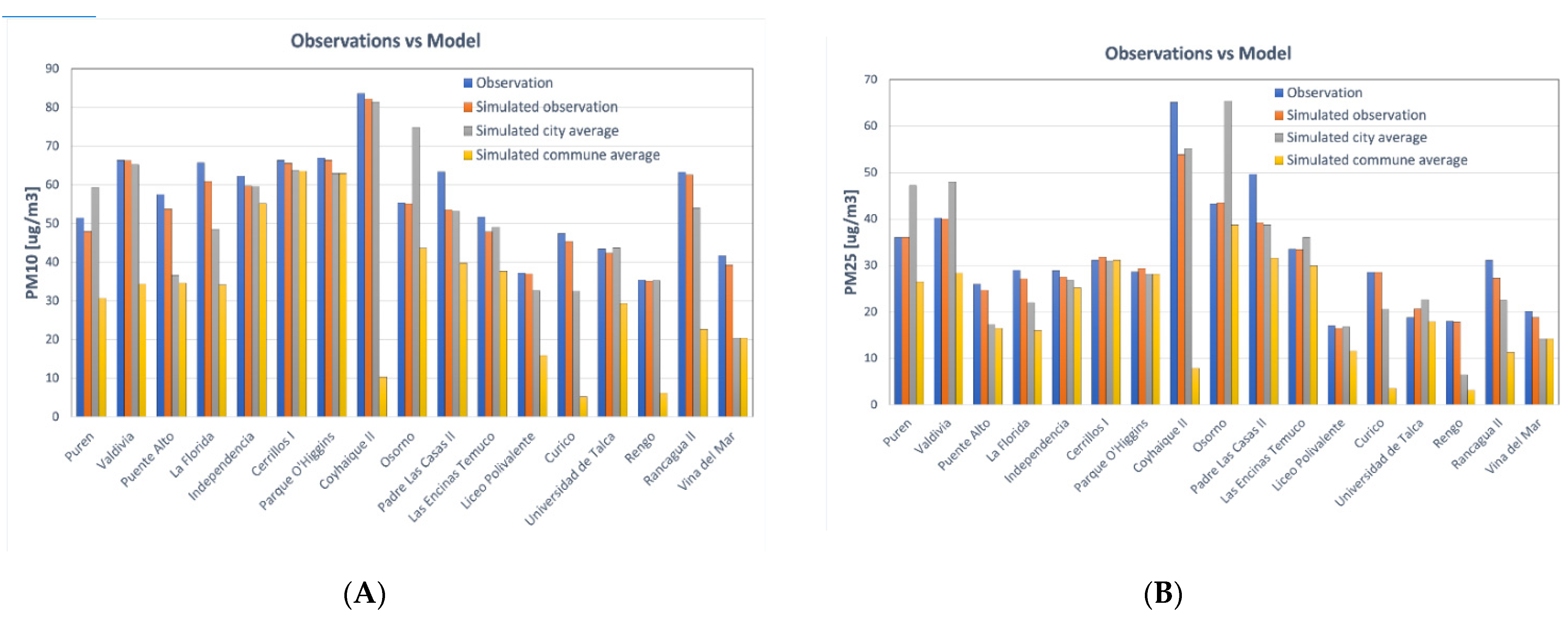
2.2.2. Air Pollution
2.2.3. Confounders
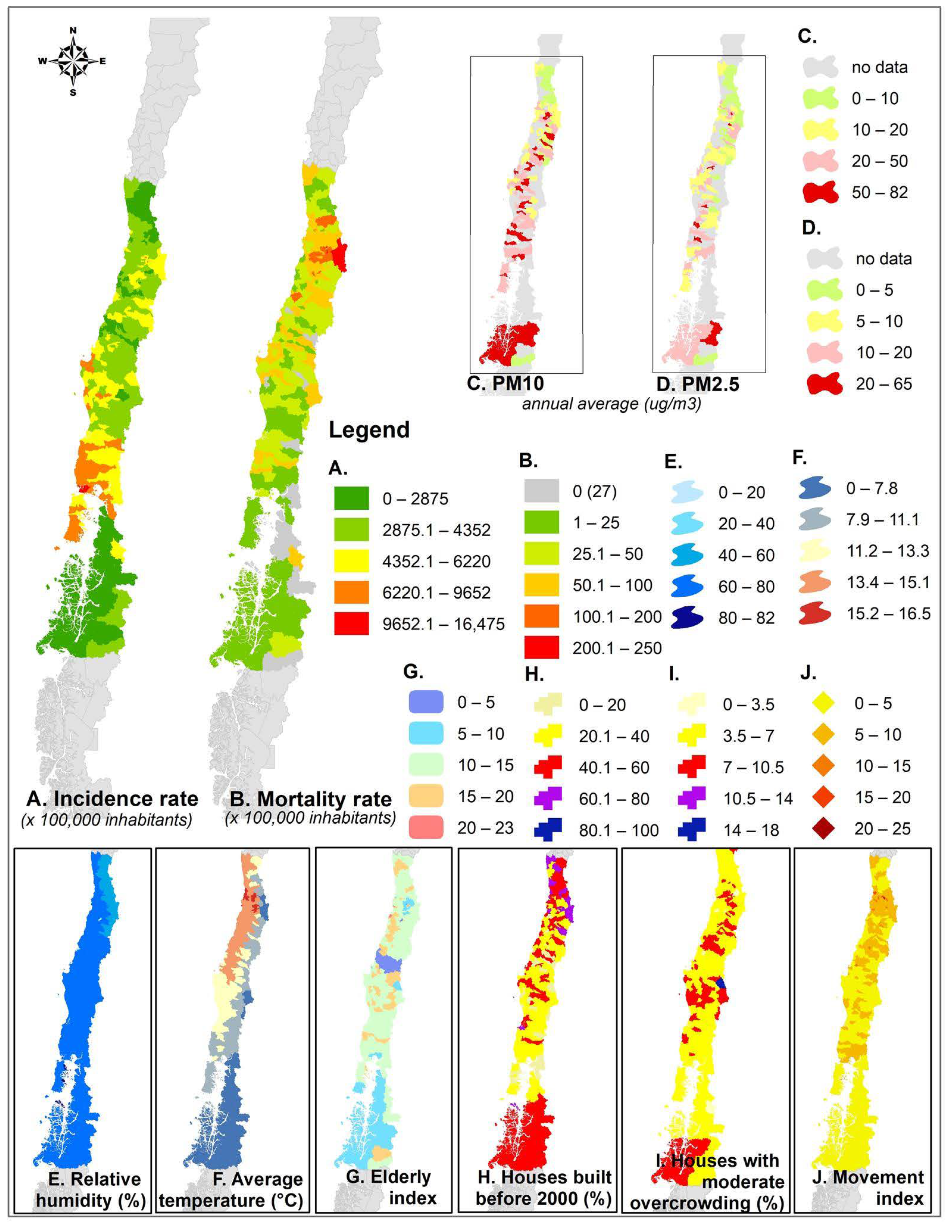
- Temperature and humidity: The average annual air temperature and relative humidity from 1980–2010 were obtained from ARClim, which is an open-source meteorological dataset [30]. This dataset was chosen due to its official endorsement given by the Chilean Ministry of Environment, and because its spatial resolution (5 × 5 km) provides data for all 188 communes.
- Elderly index: Proportion of the elderly population (65 years old or more) for 2020 based on projections of the 2017 Census.
- Self-report of health: Proportion of the population that have declared absence of chronic or acute diseases, based on the National Socioeconomic Characterization Survey [31]. The reported illnesses include hypertension, diabetes, myocardial infarction, stroke, chronic obstructive pulmonary disease, asthma, thyroid disease, cancer, and lupus.
- Percentage of houses with moderate overcrowding: Number of houses with moderate overcrowding out of the total number of houses in each commune. The overcrowding corresponds to the ratio of the number of people to the number of bedrooms. Moderate overcrowding is defined as 2.5 to 4.9 people per bedroom [32].
- Percentage of houses built before 2000: Number of houses built before 2000 out of each commune’s total number of houses. Homes built before 2000 were not subject to the thermal standard considered in the first stage of regulations associated with thermal insulation of housing [32].
- Mobility index: Sum of the internal and external mobility indexes. The internal index is a measure of the number of trips that occur within a commune, whereas the latter corresponds to the number of trips made outside of the commune. Both indexes were summed and normalized by the population of the administrative unit [33].
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- COVID-19 Map-Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 16 May 2021).
- Center for Disease Control and Prevention CDC Symptoms of COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html (accessed on 16 May 2021).
- Pearce, N.; Lawlor, D.A.; Brickley, E.B. Comparisons between countries are essential for the control of COVID-19. Int. J. Epidemiol. 2020, 49, 1059–1062. [Google Scholar] [CrossRef]
- Wei, Y.Y.; Wang, R.R.; Zhang, D.W.; Tu, Y.H.; Chen, C.S.; Ji, S.; Li, C.X.; Li, X.Y.; Zhou, M.X.; Cao, W.S.; et al. Risk factors for severe COVID-19: Evidence from 167 hospitalized patients in Anhui, China. J. Infect. 2020, 81, e89–e92. [Google Scholar] [CrossRef]
- Gao, F.; Zheng, K.I.; Wang, X.B.; Sun, Q.F.; Pan, K.H.; Wang, T.Y.; Chen, Y.P.; Targher, G.; Byrne, C.D.; George, J.; et al. Obesity Is a Risk Factor for Greater COVID-19 Severity. Diabetes Care 2020, 43, E72–E74. [Google Scholar] [CrossRef]
- Hamer, M.; Kivimäki, M.; Gale, C.R.; Batty, G.D. Lifestyle risk factors, inflammatory mechanisms, and COVID-19 hospitalization: A community-based cohort study of 387,109 adults in UK. Brain Behav. Immun. 2020, 87, 184–187. [Google Scholar] [CrossRef]
- Woodby, B.; Arnold, M.M.; Valacchi, G. SARS-CoV-2 infection, COVID-19 pathogenesis, and exposure to air pollution: What is the connection? Ann. N. Y. Acad. Sci. 2021, 1486, 15–38. [Google Scholar] [CrossRef]
- Frontera, A.; Cianfanelli, L.; Vlachos, K.; Landoni, G.; Cremona, G. Severe air pollution links to higher mortality in COVID-19 patients: The “double-hit” hypothesis. J. Infect. 2020, 81, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Sanhueza, P.A.; Torreblanca, M.A.; Diaz-Robles, L.A.; Schiappacasse, L.N.; Silva, M.P.; Astete, T.D. Particulate air pollution and health effects for cardiovascular and respiratory causes in Temuco, Chile: A wood-smoke-polluted urban area. J. Air Waste Manag. Assoc. 2009, 59, 1481–1488. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [Green Version]
- Sicard, P.; Khaniabadi, Y.O.; Perez, S.; Gualtieri, M.; De Marco, A. Effect of O3, PM10 and PM2.5 on cardiovascular and respiratory diseases in cities of France, Iran and Italy. Environ. Sci. Pollut. Res. 2019, 26, 32645–32665. [Google Scholar] [CrossRef]
- Bourdrel, T.; Annesi-Maesano, I.; Alahmad, B.; Maesano, C.N.; Bind, M.A. The impact of outdoor air pollution on covid-19: A review of evidence from in vitro, animal, and human studies. Eur. Respir. Rev. 2021, 30, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Bhaskar, A.; Chandra, J.; Braun, D.; Cellini, J.; Dominici, F. Air pollution, SARS-CoV-2 transmission, and COVID-19 outcomes: A state-of-the-science review of a rapidly evolving research area. medRxiv 2020. [Google Scholar] [CrossRef]
- Wu, X.; Nethery, R.C.; Benjamin, M.; Ma, S.; Braun, D.; Dominici, F.; Gamble, C.J. Exposure to air pollution and COVID-19 mortality in the United States. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Travaglio, M.; Popovic, R.; Yu, Y.; Santos Leal, N.; Martins, L.M. Links between air pollution and COVID-19 in England. Environ. Pollut. 2021, 268, 115859. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; University, F.; China, S.; Liu, Z.; Med, B.; Meng, X.; Kan, H.; Wang, W. Ambient nitrogen dioxide pollution and spread ability of COVID-19 in Chinese cities. Ecotoxicol. Environ. Saf. 2021, 208, 111421. [Google Scholar] [CrossRef]
- Coker, E.S.; Cavalli, L.; Fabrizi, E.; Guastella, G.; Lippo, E.; Parisi, M.L.; Pontarollo, N.; Rizzati, M.; Varacca, A.; Vergalli, S. The Effects of Air Pollution on COVID-19 Related Mortality in Northern Italy. Environ. Resour. Econ. 2020, 76, 611–634. [Google Scholar] [CrossRef] [PubMed]
- Das, K.; Chatterjee, N. Das Examine the impact of weather and ambient air pollutant parameters on daily case of COVID-19 in India. medRxiv 2020. [Google Scholar] [CrossRef]
- Zhu, Y.; Xie, J.; Huang, F.; Cao, L. Association between short-term exposure to air pollution and COVID-19 infection: Evidence from China. Sci. Total Environ. 2020, 727, 138704. [Google Scholar] [CrossRef]
- Fernández-Raga, M.; Díaz-Marugán, L.; García Escolano, M.; Bort, C.; Fanjul, V. SARS-CoV-2 viability under different meteorological conditions, surfaces, fluids and transmission between animals. Environ. Res. 2021, 192. [Google Scholar] [CrossRef]
- Correa-Araneda, F.; Ulloa-Yañez, A.; Núñez, D.; Boyero, L.; Tonin, A.; Cornejo, A.; Urbina, M.; Díaz, M.E.; Figueroa-Muñoz, G.; Esse, C. Environmental determinants of COVID-19 transmission across a wide climatic gradient in Chile. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- World Health Organization Coronavirus Disease (COVID-19): How Is It Transmitted? Available online: https://www.who.int/news-room/q-a-detail/coronavirus-disease-covid-19-how-is-it-transmitted (accessed on 24 May 2021).
- World Bank World Bank East Asia and Pacific Economic Update. April 2020: East Asia and Pacific in the Time of COVID-19; World Bank: Washington, DC, USA, 2020. [Google Scholar]
- Ministerio de Ciencia. Gobierno de Chile Base de Datos COVID-19. Available online: https://www.minciencia.gob.cl/covid19/ (accessed on 1 March 2021).
- Instituto Nacional de Estadísticas. Chile Proyecciones de Población. Available online: https://www.ine.cl/estadisticas/sociales/demografia-y-vitales/proyecciones-de-poblacion (accessed on 24 May 2021).
- Mazzeo, A.; Huneeus, N.; Ordoñez, C.; Orfanoz-Cheuquelaf, A.; Menut, L.; Mailler, S.; Valari, M.; Denier Van Der Gon, H.; Gallardo, L.; Muñoz, R.; et al. Impact of residential combustion and transport emissions on air pollution in Santiago during winter. Atmos. Environ. 2018, 190, 195–208. [Google Scholar] [CrossRef]
- Lapere, R.; Mailler, S.; Menut, L.; Huneeus, N. Pathways for wintertime deposition of anthropogenic light-absorbing particles on the Central Andes cryosphere. Environ. Pollut. 2021, 272, 115901. [Google Scholar] [CrossRef]
- Lapere, R.; Menut, L.; Mailler, S.; Huneeus, N. Soccer games and record-breaking PM2.5 pollution events in Santiago, Chile. Atmos. Chem. Phys. 2020, 20, 4681–4694. [Google Scholar] [CrossRef] [Green Version]
- Trewhela, B.; Huneeus, N.; Munizaga, M.; Mazzeo, A.; Menut, L.; Mailler, S.; Valari, M.; Ordoñez, C. Analysis of exposure to fine particulate matter using passive data from public transport. Atmos. Environ. 2019, 215, 116878. [Google Scholar] [CrossRef]
- Ministerio del Medio Ambiente del Gobierno de Chile Atlas de Riesgos Climáticos desarrollado por el Centro de Investigación del Clima y la Resiliencia (CR2) y el Centro de Cambio Global (CCG-Universidad Católica de Chile). Available online: https://arclim.mma.gob.cl. (accessed on 1 March 2021).
- Ministerio de Desarrollo Social y Familia Encuesta de Caracterización Socioeconómica Nacional CASEN 2017. Available online: http://observatorio.ministeriodesarrollosocial.gob.cl/encuesta-casen (accessed on 24 May 2021).
- Ministerio de Vivienda y Urbanismo Estadísticas Habitacionales. Observatorio Urbano. Available online: https://www.observatoriourbano.cl/estadisticas-habitacionales/ (accessed on 24 May 2021).
- Instituto de Data Science de la Universidad del Desarrollo Bravo, Loreto, and Ferres, Leo. The IM (Mobility Index) dataset, electronic dataset, UDD and Ministry of Science, Chile. 2020. Available online: https://github.com/MinCiencia/Datos-COVID19/tree/master/output/producto33 (accessed on 24 May 2021).
- Cole, M.A.; Ozgen, C.; Strobl, E. Air Pollution Exposure and Covid-19 in Dutch Municipalities. Environ. Resour. Econ. 2020, 76, 581–610. [Google Scholar] [CrossRef] [PubMed]
- Contini, D.; Costabile, F. Does Air Pollution Influence COVID-19 Outbreaks? Atmosphere 2020, 11, 377. [Google Scholar] [CrossRef] [Green Version]
- Frontera, A.; Martin, C.; Vlachos, K.; Sgubin, G. Regional air pollution persistence links to COVID-19 infection zoning. J. Infect. 2020, 81, 318. [Google Scholar] [CrossRef] [PubMed]
- Pramanik, M.; Udmale, P.; Bisht, P.; Chowdhury, K.; Szabo, S.; Pal, I. Climatic factors influence the spread of COVID-19 in Russia. Int. J. Environ. Health Res. 2020, 1–16. [Google Scholar] [CrossRef]
- Gupta, A.; Banerjee, S.; Das, S. Significance of geographical factors to the COVID-19 outbreak in India. Model. Earth Syst. Environ. 2020, 6, 2645–2653. [Google Scholar] [CrossRef]
- Patel, A. Preventing COVID-19 Amid Public Health and Urban Planning Failures in Slums of Indian Cities. World Med. Health Policy 2020, 12, 266–273. [Google Scholar] [CrossRef]
- Morawska, L.; Tang, J.W.; Bahnfleth, W.; Bluyssen, P.M.; Boerstra, A.; Buonanno, G.; Cao, J.; Dancer, S.; Floto, A.; Franchimon, F.; et al. How can airborne transmission of COVID-19 indoors be minimised? Environ. Int. 2020, 142, 105832. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Mean | St. Deviation | Min | Max | |
|---|---|---|---|---|---|
| Incidence × 100,000 inhabitants | 188 | 4501 | 1423 | 1786 | 9071 |
| Mortality × 100,000 inhabitants | 188 | 71 | 56 | 0 | 250 |
| Annual average PM2.5, μg/m3 | 188 | 16 | 10 | 2 | 65 |
| Annual average PM10, μg/m3 | 188 | 24 | 18 | 3 | 81 |
| Elderly index, % | 188 | 13 | 3 | 4 | 23 |
| Self-reported health, % | 188 | 73 | 4 | 57 | 85 |
| Houses with moderate overcrowding, % | 188 | 6 | 2 | 1 | 12 |
| Houses built before 2000, % | 188 | 45 | 16 | 11 | 88 |
| Mobility index | 188 | 7 | 3 | 0 | 30 |
| Average temperature, °C | 188 | 13 | 2 | 5 | 16 |
| Relative humidity, % | 188 | 67 | 7 | 48 | 79 |
| Crude Models | Adjusted Models | |||||
|---|---|---|---|---|---|---|
| IRR | 95%CI | p-Value | IRR | 95%CI | p-Value | |
| Annual average PM2.5, μg/m3 | 1.015 | 1.011–1.019 | <0.001 | 1.012 | 1.008–1.017 | <0.001 |
| Elderly index, % | 0.989 | 0.975–1.004 | 0.155 | |||
| Self-reported health, % | 1.007 | 0.998–1.016 | 0.115 | |||
| Houses with moderate overcrowding, % | 1.043 | 1.018–1.068 | 0.001 | |||
| Houses built before 2000, % | 1.000 | 0.998–1.003 | 0.769 | |||
| Mobility index | 0.997 | 0.982–1.012 | 0.666 | |||
| Average temperature, °C | 0.997 | 0.977–1.017 | 0.742 | |||
| Relative humidity, % | 1.012 | 1.006–1.018 | <0.001 | |||
| Annual average PM10, μg/m3 | 1.009 | 1.006–1.011 | <0.001 | 1.009 | 1.007–1.011 | <0.001 |
| Elderly index, % | 0.985 | 0.972–0.999 | 0.041 | |||
| Self-reported health, % | 1.003 | 0.995–1.012 | 0.472 | |||
| Houses with moderate overcrowding, % | 1.038 | 1.015–1.063 | 0.001 | |||
| Houses built before 2000, % | 0.999 | 0.997–1.002 | 0.627 | |||
| Mobility index | 0.998 | 0.983–1.012 | 0.759 | |||
| Average temperature, °C | 0.988 | 0.969–1.007 | 0.224 | |||
| Relative humidity, % | 1.015 | 1.009 | <0.001 | |||
| Crude Models | Adjusted Models | |||||
|---|---|---|---|---|---|---|
| IRR | 95%CI | p-Value | IRR | 95%CI | p-Value | |
| Annual average PM2.5, μg/m3 | 1.022 | 1.011–1.033 | <0.001 | 1.004 | 0.996–1.011 | 0.361 |
| Elderly index, % | 0.984 | 0.956–1.013 | 0.271 | |||
| Self-reported health, % | 0.998 | 0.980–1.016 | 0.834 | |||
| Houses with moderate overcrowding, % | 1.035 | 0.986–1.086 | 0.161 | |||
| Houses built before 2000, % | 1.011 | 1.005–1.016 | <0.001 | |||
| Mobility index | 1.004 | 0.969–1.039 | 0.842 | |||
| Average temperature, °C | 1.154 | 1.111–1.198 | <0.001 | |||
| Relative humidity, % | 0.958 | 0.946–0.970 | <0.001 | |||
| Annual average PM10, μg/m3 | 1.018 | 1.012–1.023 | <0.001 | 1.003 | 0.999–1.008 | 0.144 |
| Elderly index, % | 0.982 | 0.954–1.011 | 0.221 | |||
| Self-reported health, % | 0.997 | 0.979–1.015 | 0.707 | |||
| Houses with moderate overcrowding, % | 1.031 | 0.983–1.082 | 0.210 | |||
| Houses built before 2000, % | 1.010 | 1.005–1.016 | <0.001 | |||
| Mobility index | 1.003 | 0.969–1.038 | 0.860 | |||
| Average temperature, °C | 1.149 | 1.106.1.194 | <0.001 | |||
| Relative humidity, % | 0.959 | 0.947–0.970 | <0.001 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valdés Salgado, M.; Smith, P.; Opazo, M.A.; Huneeus, N. Long-Term Exposure to Fine and Coarse Particulate Matter and COVID-19 Incidence and Mortality Rate in Chile during 2020. Int. J. Environ. Res. Public Health 2021, 18, 7409. https://doi.org/10.3390/ijerph18147409
Valdés Salgado M, Smith P, Opazo MA, Huneeus N. Long-Term Exposure to Fine and Coarse Particulate Matter and COVID-19 Incidence and Mortality Rate in Chile during 2020. International Journal of Environmental Research and Public Health. 2021; 18(14):7409. https://doi.org/10.3390/ijerph18147409
Chicago/Turabian StyleValdés Salgado, Macarena, Pamela Smith, Mariel A. Opazo, and Nicolás Huneeus. 2021. "Long-Term Exposure to Fine and Coarse Particulate Matter and COVID-19 Incidence and Mortality Rate in Chile during 2020" International Journal of Environmental Research and Public Health 18, no. 14: 7409. https://doi.org/10.3390/ijerph18147409