
Barriers to, and Facilitators of, Exercising in Fitness Centres among Adults with and without Physical Disabilities: A Scoping Review

 , ,
, ,
Abstract
:1. Background
2. Methods
2.1. Methodological Design
2.2. Step 1—Identifying the Research Question
2.3. Step 2—Identifying Relevant Studies
Search Strategy
2.4. Step 3—Study Selection
2.5. Step 4—Charting the Data (Data Extraction Process)
- Descriptive studies (e.g., questionnaires)—if more than 50% of the respondents stated the factor as a barrier or a facilitator;
- Regression/correlation analysis—a significant result according to the definition in the paper;
- Factor analysis—a significant result according to the definition in the paper.
- Qualitative data:
- Papers with a results section—barriers or facilitators described in the results or conclusion sections;
- ‘Grey literature’ without a results section—if barriers or facilitators were described in the text.
2.6. Step 5 Collating, Summarising, and Reporting the Results
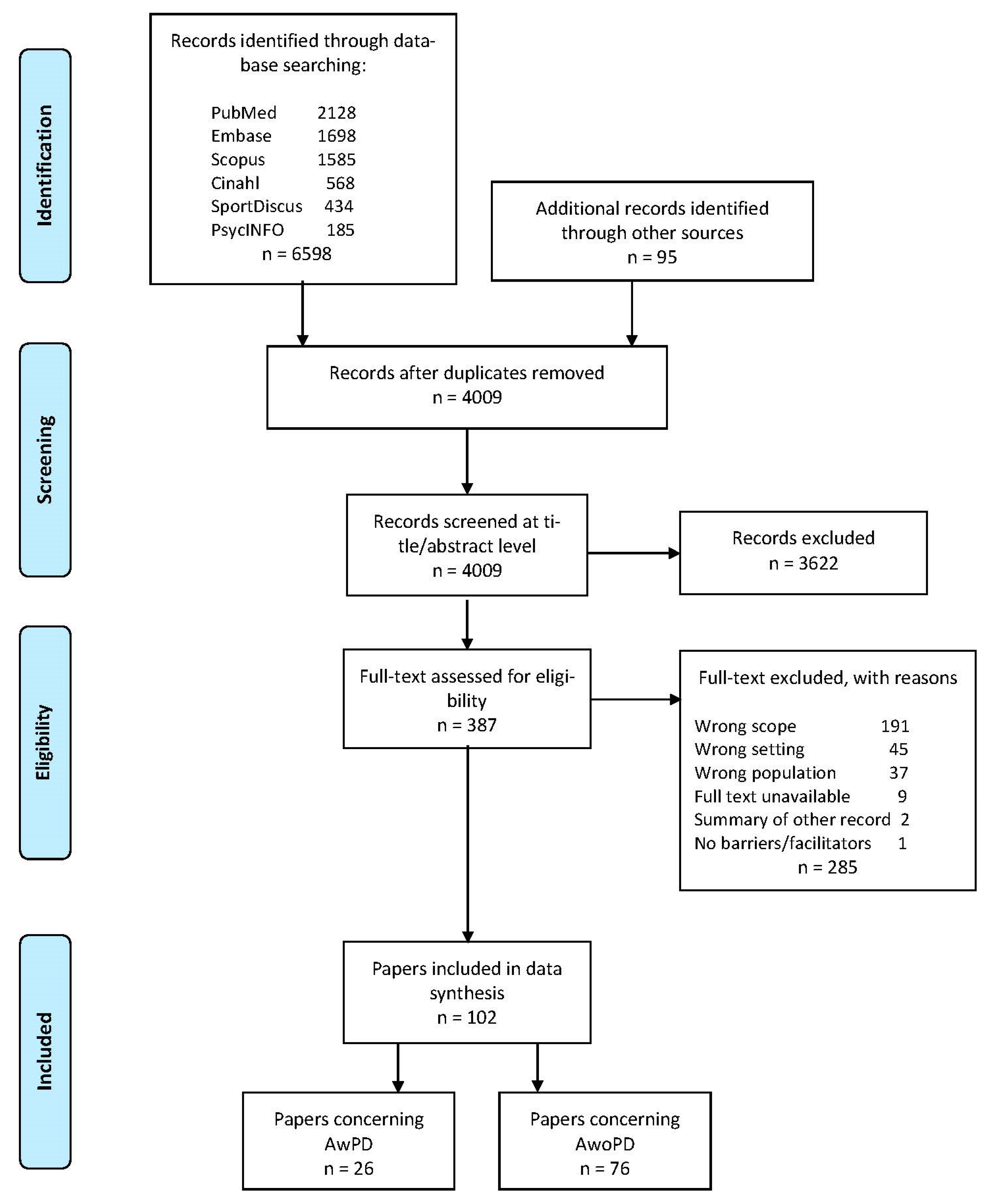
3. Results
3.1. Numerical Summary


{kind=link}
| Type of Paper | AwPD Reference Number | n | % | AwoPD Reference Number | n | % | |
|---|---|---|---|---|---|---|---|
| Scientific | Quantitative studies | [44,45,46,47,50,55,62] | 7 | 27 | [69,74,75,76,77,80,81,82,83,85,86,87,90,91,92,93,94,98,100,103,108,110,118,119,120,122,123,125,133,134,135,136,137,139,140] | 36 | 47 |
| Qualitative studies | [11,51,58,59,60] | 5 | 19 | [66,70,79,84,88,99,102,105,106,107,113,117,121,126,130] | 15 | 20 | |
| Mixed method studies | [43] | 1 | 4 | [71,72,114,115,124,132,138] | 7 | 9 | |
| Systematic reviews | [26] | 1 | 4 | ||||
| Reviews/opinion papers | [61] | 1 | 4 | ||||
| Theses | [89,116] | 2 | 3 | ||||
| Grey | Conference papers | [48] | 1 | 4 | [68] | 1 | 1 |
| Conference poster | [101] | 1 | 1 | ||||
| Guidelines | [49,52,53,56,64,65] | 6 | 23 | ||||
| Reports | [67,95,96,111,112] | 5 | 7 | ||||
| Magazine articles | [54,57,63] | 3 | 11 | [78,97,104,109,131] | 5 | 7 | |
| Newspaper articles | [42] | 1 | 4 | [73,127,128,129] | 4 | 5 | |
| In total | 26 | 100 | 76 | 100 |
3.2. Descriptive Summary
3.2.1. Adults with Physical Disabilities (AwPD)—Barriers and Facilitators
| 1. The Fitness Centre Setting (18 Papers) | 2. The Fitness Centre User Characteristics (6 Papers) | 3. The Fitness Instructor’s/Staff Characteristics (7 Papers) | 4. The Fitness Centre User—Instructor/Management Relationship (9 Papers) | 5. The Fitness/Exercise Characteristics (5 Papers) | 6. Other Relationships (7 Papers) |
|---|---|---|---|---|---|
Poor transportation options [11,26,42,45,50,52,55]
| Lack of knowledge about accessible and available facilities [11]
| Lack of skilled instructors [11,26,43,45,50,52,53]
| Management not being actively inclusive [11,43,52,53,56,57,62]
| Lack of tailored classes/ adaptive programs [11,26,42,46,52]
| Stigma from non-disabled members leading to direct psycho-emotional disablism [51,52,53,59,60]
|
Poor accessibility to the fitness centre and bathrooms/locker rooms [11,26,44,45,47,50,51,52,53,55,57,58,59,61,62,63]
| High costs [11,42]
| Negative attitudes resulting in direct psycho-emotional disablism [11,43,52,53,59,60]
| Negotiations about body ideals, rights and power [58]
| ||
Unsuitable fitness equipment [11,26,45,47,48,50,52,55,57,59,63]
| Negative feelings about fitness [11,51,58,59,60]
| Lack of knowledge leading to unprofessional assistance [56,60]
| Lack of support from friends and families [11]
|
| 1. The Fitness Centre Setting (14 Papers) | 2. The Fitness Centre User Characteristics (2 Papers) | 3. The Fitness Instructor’s/Staff Characteristics (9 Papers) | 4. The Fitness Centre User—Instructor/Management Relationship (8 Papers) | 5. The Fitness/Exercise Characteristics (7 Papers) | 6. Other Relationships (5 Papers) |
|---|---|---|---|---|---|
| Universal design/good accessibility [11,44,47,49,53,54,56,57,65]
| Benefits from exercising [60]
| Specially trained staff [11,43,44,50,55,56,58,64]
| Correct guidance and assistance from instructors [56]
| Tailored exercise programs to people with physical disabilities [47,53,55,56,57,63,64]
| The fitness centre as a social arena [51,58,59,60,63]
|
Specialised fitness equipment [11,44,45,47,52,56,57,63,64]
| Positive experiences related to fitness [59,60]
| Respectful communication [11,49,56]
| Inclusive and tolerant environment [51,56,58,60]
| ||
Use of checklists to improve accessibility [49,56,61]
| Membership/low costs [11,44,50,55,56]
|
3.2.2. Adults without Physical Disabilities (AwoPD)—Barriers and Facilitators
| 1. The Fitness Centre Setting (8 Papers) | 2. The Fitness Centre User Characteristics (22 Papers) | 3. The Fitness Instructor’s/Staff Characteristics (4 Papers) | 4. The Fitness Centre User—Instructor/Management Relationship (6 Papers) | 5. The Fitness/Exercise Characteristics (2 Papers) | 6. Other Relationships (8 Papers) |
|---|---|---|---|---|---|
Long transportation time/distance to fitness centre [69,71,126]
| Dislike of the fitness culture [70,97,99,113,122,123,131]
| Lack of professional guidance [70,106,107,122]
| Negative staff attitudes [79,97,107,120,122]
| Uninteresting/boring exercises [115,117]
| Lack of social connections [113,115]
|
Unattractive fitness facilities [71,100,113,122,123,131]
| Lack of knowledge [70,71,84,90,104,113,123]
| Body ideals and physical performance [97,115,122]
| Lack of support from health authorities [113]
| ||
Individual priorities [70,71,73,80,85,90,95,96,99,105,111,112,113,116,117,123,126]
| Not fitting in [71,78,113,116,122,128,131]
|
| 1. The Fitness Centre Setting (18 Papers) | 2. The Fitness Centre User Characteristics (43 Papers) | 3. The Fitness Instructor’s/Staff Characteristics (15 Papers) | 4. The Fitness Centre User—Instructor/Management Relationship (13 Papers) | 5. The Fitness/Exercise Characteristics (14 Papers) | 6. Other Relationships (21 Papers) |
|---|---|---|---|---|---|
Easy access [67,70,71,87,91,102,110,114,117,132]
| Health and body appearance [66,67,68,70,73,75,79,84,86,90,95,96,99,102,105,110,111,112,113,114,115,117,121,125,126,127,128,129,130,132,133]
| The ideal instructor [70,71,72,73,74,100,102,103,106,107,110,117,124,131,138]
| Comfortable atmosphere [66,76,94,115,124]
| Fitness classes [70,100,101,110,117,126,127,129,131]
| Social connections [66,70,71,81,84,88,97,102,105,113,114,115,117,121,124,126,132,134,138,139,140]
|
Pleasant fitness environment [88,91,98,109,110,124,127,129,131,132,141]
| Positive mind and feelings [68,70,73,79,84,86,89,90,95,96,99,102,110,111,112,114,115,117,118,126,130,132]
| Soft values [74,94,97,113,115,124,126,138]
| Individual focus/goal [76,104,108,110,116,138]
| ||
Feeling comfortable in the fitness centre [67,70,71,72,92,93,94,99,110,113,114,115,119,121,131,132,137]
| Membership [66,76,83,135,136]
| ||||
Low costs [70,71,77,91,113,114]
|
3.3. Comparative Analysis
| Adults with Physical Disabilities (AwPD) | Adults without Physical Disabilities (AwPD) | |||
|---|---|---|---|---|
| Context Factor Categories | Barriers (Table 3) | Facilitators (Table 4) | Barriers (Table 5) | Facilitators (Table 6) |
| 1. The Fitness Centre Setting | Poor transportation options (7) Poor accessibility to the fitness centre and bathrooms/locker rooms (16) Unsuitable fitness equipment (11) | Universal design/good accessibility (9) Specialised fitness equipment (9) Use of checklists to improve accessibility (3) | Long transportation time/distance to fitness centre (3) Unattractive fitness facilities (6) | Easy access (10) Pleasant fitness environment (11) |
| 2. The Fitness Centre User Characteristics | Lack of knowledge about accessible and available facilities (1) High costs (2) Negative feelings about fitness (5) | Benefits from exercising (1) Positive experiences related to fitness (2) | Dislike of the fitness culture (7) Lack of knowledge (7) Individual priorities (17) | Health and body appearance (31) Positive mind and feelings (22) Feeling comfortable in the fitness centre (17) Low costs (6) |
| 3. The Fitness Instructor’s/Staff Characteristics | Lack of skilled instructors (7) | Specially trained staff (8) Respectful communication (3) | Lack of professional guidance (4) | The ideal instructor (15) |
| 4. The Fitness Centre User —Instructor/Management Relationship | Management not being actively inclusive (7) Negative attitudes resulting in direct psycho-emotional disablism (6) Unprofessional assistance (2) | Correct guidance and assistance from instructors (1) Inclusive and tolerant environment (4) Membership/low costs (5) | Negative staff attitudes (5) Body ideals and physical performance (3) | Comfortable atmosphere (5) Soft values (8) Membership (5) |
| 5. The Fitness/Exercise Characteristics | Lack of tailored classes/adaptive programs (5) | Tailored exercise programs to people with physical disability (7) | Uninteresting/boring exercises (2) | Fitness classes (9) Individual focus/goal (6) |
| 6. Other Relationships | Stigma from non-disabled members leading to direct psycho-emotional disablism (5) Negotiations about body ideals, rights and power (1) Lack of support from friends and family (5) | The fitness centre as a social arena (5) | Lack of social connections (2) Lack of support from health authorities (1) Not fitting in (7) | Social connections (21) |
4. Discussion
Method—Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AwPD | Adults with physical disabilities |
| AwoPD | Adults without physical disabilities |
| PCC mnemonic | Population, Concept and Context |
| WHO | World Health Organization |
References
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide Trends in Insufficient Physical Activity from 2001 to 2016: A Pooled Analysis of 358 Population-Based Surveys with 19 Million Participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases: 2013–2020; World Health Organization: Geneva, Switzerland, 2013; ISBN 978-92-4-150623-6. [Google Scholar]
- Danish Health Authority. Danskernes sundhed: Den nationale sundhedsprofil 2017. In The health of Danish Citizens: The Danish National Health Profile 2017; Danish Health Authority: Copenhagen, Denmark, 2018; ISBN 978-87-7104-956-5. [Google Scholar]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of Exercise Is a Major Cause of Chronic Diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, B.K.; Saltin, B. Exercise as Medicine—Evidence for Prescribing Exercise as Therapy in 26 Different Chronic Diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 26 June 2020).
- World Health Organization. Global Recommendations on Physica006C Activity for Health; World Health Organization: Geneva, Switzerland, 2010; ISBN 978-92-4-159997-9. [Google Scholar]
- World Health Organization. 10 Facts on Physical Activity. Available online: http://www.who.int/features/factfiles/physical_activity/en/ (accessed on 30 July 2018).
- Krahn, G.L.; Walker, D.K.; Correa-De-Araujo, R. Persons With Disabilities as an Unrecognized Health Disparity Population. Am. J. Public Health 2015, 105, 198–206. [Google Scholar] [CrossRef]
- Carroll, D.D.; Courtney-Long, E.A.; Stevens, A.C.; Sloan, M.L.; Lullo, C.; Visser, S.N.; Fox, M.H.; Armour, B.S.; Campbell, V.A.; Brown, D.R.; et al. Vital Signs: Disability and Physical Activity—United States, 2009–2012. MMWR. Morb. Mortal. Wkly. Rep. 2014, 63, 7. [Google Scholar]
- Rimmer, J.H.; Riley, B.; Wang, E.; Rauworth, A.; Jurkowski, J. Physical Activity Participation among Persons with Disabilities. Am. J. Prev. Med. 2004, 26, 419–425. [Google Scholar] [CrossRef]
- Ginis, K.A.M.; Ma, J.K.; Latimer-Cheung, A.E.; Rimmer, J.H. A Systematic Review of Review Articles Addressing Factors Related to Physical Activity Participation among Children and Adults with Physical Disabilities. Health Psychol. Rev. 2016, 10, 478–494. [Google Scholar] [CrossRef]
- Strain, T.; Wijndaele, K.; Garcia, L.; Cowan, M.; Guthold, R.; Brage, S.; Bull, F.C. Levels of Domain-Specific Physical Activity at Work, in the Household, for Travel and for Leisure among 327 789 Adults from 104 Countries. Br. J. Sports Med. 2020, 54, 1488–1497. [Google Scholar] [CrossRef]
- Sassatelli, R. Fitness Culture: Gyms and the Commercialisation of Discipline and Fun. In Consumption and Public Life; Palgrave Macmillan: London, UK, 2010; ISBN 978-0-230-50749-4. [Google Scholar]
- Burgess, T. Fitness Is the World’s Biggest Sport; Les Mills International: Auckland, New Zealand, 2013. [Google Scholar]
- Rodriguez, M. 2019 IHRSA Global Report: Key Findings. What’s New In Fitness (WNiF) Magazine. 2019. Available online: https://whatsnewinfitness.com.au/ihrsa-2019-global-report-key-findings (accessed on 25 June 2021).
- Deloitte. European Health & Fitness Market Report 2020; Europe Active: Bruxelles, Belgium, 2020. [Google Scholar]
- Hedblom, C. The Body Is Made to Move: Gym and Fitness Culture in Sweden; Stockholm Studies in Social Anthropology; Acta Universitatis Stockholmiensis: Stockholm, Sweden, 2009; ISBN 978-91-86071-20-2. [Google Scholar]
- Andreasson, J.; Johansson, T. The Global Gym: Gender, Health and Pedagogies; Palgrave Macmillan: London, UK, 2014; ISBN 978-1-137-34661-2. [Google Scholar]
- English Federation of Disability Sport. Motivate Me: Understanding What Motivates and Appeals to Disabled People to Take Part in Sport and Physical Activity; English Federation of Disability Sport: Loughborough, England, 2014. [Google Scholar]
- Kirkegaard, K.L. Fitnessculture.dk: The History of the Fitness Sector, the Active Participants and the Commercialisation of Non-Elite Sport. Ph.D Thesis, Department of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, Denmark, 2012. [Google Scholar]
- Mosley, P.E. Bigorexia: Bodybuilding and Muscle Dysmorphia. Eur. Eat. Disord. Rev. 2009, 17, 191–198. [Google Scholar] [CrossRef]
- Almeida, C.; Vieira Borba, V.; Santos, L. Orthorexia Nervosa in a Sample of Portuguese Fitness Participants. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2018, 23, 443–451. [Google Scholar] [CrossRef]
- Gwizdek, K.; Brzęk, A.; Bąk-Sosnowska, M.; Dittfeld, A.; Knapik, A.; Ziaja, D. The Use of Steroids by Gym Athletes: An Attempt to Diagnose the Problem Scale and Possible Causes. J. Sports Med. Phys. Fit. 2018, 58, 880–888. [Google Scholar] [CrossRef]
- Wazaify, M.; Bdair, A.; Al-Hadidi, K.; Scott, J. Doping in Gymnasiums in Amman: The Other Side of Prescription and Nonprescription Drug Abuse. Subst. Use Misuse 2014, 49, 1296–1302. [Google Scholar] [CrossRef]
- Calder, A.; Sole, G.; Mulligan, H. The Accessibility of Fitness Centers for People with Disabilities: A Systematic Review. Disabil. Health J. 2018, 11, 525–536. [Google Scholar] [CrossRef]
- Chan, D.M.; Zoellick, M.R.B. World Report on Disability; World Health Organization (WHO): Geneva, Switzerland, 2011; p. 24. [Google Scholar]
- Herazo-Beltrán, Y.; Pinillos, Y.; Vidarte, J.; Crissien, E.; Suarez, D.; García, R. Predictors of Perceived Barriers to Physical Activity in the General Adult Population: A Cross-Sectional Study. Braz. J. Phys. Ther. 2017, 21, 44–50. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for Conducting Systematic Scoping Reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Khalil, H.; Peters, M.; Godfrey, C.M.; McInerney, P.; Soares, C.B.; Parker, D. An Evidence-Based Approach to Scoping Reviews. Worldviews Evid. Based Nurs. 2016, 13, 118–123. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Soares, C.B.; Khalil, H.; Parker, D. Chapter 11: Scoping reviews. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Peters, M.D.J.; Godfrey, C.M.; McInerney, P.; Soares, C.B.; Khalil, H.; Parker, D. The Joanna Briggs Institute Reviewers’ Manual 2015: Methodology for JBI Scoping Reviews; The Joanna Briggs Institute: Adelaide, South Australia, 2015. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping Studies: Advancing the Methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Nikolajsen, H.; Sandal, L.F.; Juhl, C.; Troelsen, J.; Juul-Kristensen, B. Barriers and Facilitators for Fitness Centre Participation among Adult People with or without Physical Disabilities: A Systematic Scoping Review Protocol. Zenodo 2018. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Blasi, Z.; Harkness, E.; Ernst, E.; Georgiou, A.; Kleijnen, J. Influence of Context Effects on Health Outcomes: A Systematic Review. Lancet 2001, 357, 757–762. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001; ISBN 978-92-4-154542-6. [Google Scholar]
- Canadian Agency for Drugs and Technologies in Health (CADTH) Grey Matters: A Practical Tool for Searching Health-Related Grey Literature. Available online: https://cadth.ca/resources/finding-evidence/grey-matters (accessed on 5 September 2018).
- Allen, J.E. An exercise in frustration. Los Angeles Times-Southern California Edition, 10 September 2001; S1–S6. [Google Scholar]
- Anderson, C.; Grant, R.L.; Hurley, M.V. Exercise Facilities for Neurologically Disabled Populations—Perceptions from the Fitness Industry. Disabil. Health J. 2017, 10, 157–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arbour-Nicitopoulos, K.P.; Ginis, K.A.M. Universal Accessibility of “Accessible” Fitness and Recreational Facilities for Persons with Mobility Disabilities. Adapt. Phys. Act. Q. 2011, 28, 1–15. [Google Scholar] [CrossRef]
- Dolbow, D.R.; Figoni, S.F. Accommodation of Wheelchair-Reliant Individuals by Community Fitness Facilities. Spinal Cord 2015, 53, 515–519. [Google Scholar] [CrossRef] [Green Version]
- Fullerton, A.; Macdonald, M.; Brown, A.; Ho, P.-L.; Martin, J.; Tang, A.; Sibley, K.M.; McIlroy, W.E.; Brooks, D. Survey of Fitness Facilities for Individuals Post-Stroke in the Greater Toronto Area. Appl. Physiol. Nutr. Metab. 2008, 33, 713–719. [Google Scholar] [CrossRef]
- Gross, J.; Kroll, T.; Morris, J. Accessibility of Fitness Centres for People with Disabilities in a Region in North East Scotland. Public Health 2013, 127, 782–784. [Google Scholar] [CrossRef]
- Hurley, S.L.; Axelson, P.W. Universal Design of Fitness Equipment Criteria to Meet the New Department of Justice Accessibility Requirements. In Proceedings of the Rehabilitation Engineering and Assistive Technology Society of North America (RESNA) Annual conference, Baltimore, MD, USA, 28 June–3 July 2012; Beneficial Designs, Inc.: Minden, NV, USA, 2012; p. 4. [Google Scholar]
- Facts for Fitness Centers Information Sheet: Making Your Health & Fitness Center a Welcoming Facility; Inclusive Fitness Coalition: Durango, CO, USA, 2015.
- Johnson, M.; Stoelzle, H.; Finco, K.; Foss, S.; Carstens, K. ADA Compliance and Accessibility of Fitness Facilities in Western Wisconsin. Top. Spinal Cord Inj. Rehabil. 2012, 18, 340–353. [Google Scholar] [CrossRef]
- Johnston, K.R.; Goodwin, D.L.; Leo, J. Understanding Dignity: Experiences of Impairment in an Exercise Facility. Adapt. Phys. Act. Q 2015, 32, 106–124. [Google Scholar] [CrossRef]
- Kailes, J.I. Using a Fitness Center Does Not. Have to Be an Exercise in Frustration: Tips for People with Mobility and Visual Disabilities; Center for Disability Issues and the Health Profession, Western University of Health Sciences: London, Canada, 2008. [Google Scholar]
- Lockett, M. Information Package on AIMFREE Accessibility Instruments Measuring Fitness and Recreation Environments; KT4TT Center, University of Buffalo: Buffalo, NY, USA, 2011; p. 9. [Google Scholar]
- McDonnell, A.B. Family-Friendly Locker Rooms: As the Demographics in Your Facility Change to Include More Families and Older Adults, Catering to Their Locker Room Needs May Be to Your Advantage. Fit. Manag. 2002, 18, 44–47. [Google Scholar]
- Nary, D.; Froehlich, A.K.; White, G. Accessibility of Fitness Facilities for Persons with Physical Disabilities Using Wheelchairs. Top. Spinal Cord Inj. Rehabil. 2000, 6, 87–98. [Google Scholar] [CrossRef]
- North Carolina Office on Disability and Health; The Center for Universal Design. Removing Barriers to Health Clubs and Fitness Facilities—A Guide for Accommodating All Members, Including People with Disabilities and Older Adults; The University of North Carolina: Chapel Hill, NC, USA, 2008. [Google Scholar]
- Rauworth, A. Designing a Fitness Facility for All. ACMS’s Certified News, 2006; 4, 6–8. [Google Scholar]
- Richardson, E.V.; Smith, B.; Papathomas, A. Crossing Boundaries: The Perceived Impact of Disabled Fitness Instructors in the Gym. Psychol. Sport Exerc. 2017, 29, 84–92. [Google Scholar] [CrossRef] [Green Version]
- Richardson, E.V.; Smith, B.; Papathomas, A. Collective Stories of Exercise: Making Sense of Gym Experiences With Disabled Peers. Adapt. Phys. Act. Q 2017, 34, 276–294. [Google Scholar] [CrossRef]
- Richardson, E.V.; Smith, B.; Papathomas, A. Disability and the Gym: Experiences, Barriers and Facilitators of Gym Use for Individuals with Physical Disabilities. Disabil. Rehabil. 2017, 39, 1950–1957. [Google Scholar] [CrossRef] [Green Version]
- Riley, B.B.; Rimmer, J.H.; Wang, E.; Schiller, W.J. A Conceptual Framework for Improving the Accessibility of Fitness and Recreation Facilities for People with Disabilities. J. Phys. Act. Health 2008, 5, 158–168. [Google Scholar] [CrossRef]
- Rimmer, J.H.; Padalabalanarayanan, S.; Malone, L.A.; Mehta, T. Fitness Facilities Still Lack Accessibility for People with Disabilities. Disabil. Health J. 2017, 10, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Swoyer, J.O. Equality of the Fitness Centres: Are All Fitness Centres Created Equal? The Exceptional Parent: Chesterfield County, VA, USA, 2008. [Google Scholar]
- Tolle, H.; Rapacz, A.; Weintraub, B.; Shogren, C.; Harkema, S.J.; Gibson, J.L. Establishing the NeuroRecovery Network Community Fitness and Wellness Facilities: Multi-Site Fitness Facilities Provide Activity-Based Interventions and Assessments for Evidence-Based Functional Gains in Neurologic Disorders. Disabil. Rehabil. 2018, 40, 3086–3093. [Google Scholar] [CrossRef]
- United States Access Board. Accessible Sports Facilities: A Summary of Accessibility Guidelines for Recreation Facilities; United states access board: Washington, DC, USA, 2003. [Google Scholar]
- Andreasson, J.; Tugetam, Å.; Bergman, P. Keeping Death at Bay through Health Negotiation: Older Adults’ Understanding of Health and Life within Gym and Fitness Culture. Act. Adapt. Aging 2016, 40, 200–218. [Google Scholar] [CrossRef]
- Asserhøj, T.L. Danes’ Fitness Habits and Use of Commercial Sports Offers [Danskernes Fitnessvaner Og Brug Af Kommercielle Idrætstilbud]; The Danish Institute for Sports Studies [Idrættens Analyseinstitut]: Copenhagen, Denmark, 2017. [Google Scholar]
- Athanasopoulou, P.; Oikonomou, K.; Douvis, I.; Skalkos, J. Consumer Behaviour in Fitness Centers: A Typologi of Customers. In Proceedings of the Session 10: Competitive Papers: Sports Marketing, Liverpool, UK, 7 July 2011. [Google Scholar]
- Berke, E.M.; Ackermann, R.T.; Lin, E.H.; Diehr, P.H.; Maciejewski, M.L.; Williams, B.; Patrick, M.B.; LoGerfo, J.P. Distance as a Barrier to Using a Fitness-Program Benefit for Managed Medicare Enrollees. J. Aging Phys. Act. 2006, 14, 313–323. [Google Scholar] [CrossRef]
- Bethancourt, H.J.; Rosenberg, D.E.; Beatty, T.; Arterburn, D.E. Barriers to and Facilitators of Physical Activity Program Use among Older Adults. Clin. Med. Res. 2014, 12, 10–20. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.C.; Volberding, J.; Baghurst, T.; Sellers, J. Faculty/Staff Perceptions of a Free Campus Fitness Facility. Int. J. Workplace Health Manag. 2014, 7, 156–170. [Google Scholar] [CrossRef]
- Brown, T.C.; Volberding, J.; Baghurst, T.; Sellers, J. Comparing Current Fitness Center Members’ Perceptions of the Motivational Climate with Non-Members. Glob. Health Promot. 2017, 24, 5–13. [Google Scholar] [CrossRef]
- Brownfield, P. Setting his own pace in the gym rat race. Los Angeles Times-Southern California Edition, 7 January 2002; S1–S6. [Google Scholar]
- Campos, F.; Martins, F.; Simões, V.; Franco, S. Fitness Participants Perceived Quality by Age and Practiced Activity. J. Phys. Educ. Sport 2017, 17, 698–704. [Google Scholar]
- Caudwell, K.M.; Keatley, D.A. The Effect of Men’s Body Attitudes and Motivation for Gym Attendance. J. Strength Cond. Res. 2016, 30, 2550–2556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choitz, P.; Johnson, M.P.; Berhane, Z.; Lefever, G.; Anderson, J.K.; Eiser, A.R. Urban Fitness Centers: Removing Barriers to Promote Exercise in Underserved Communities. J. Health Care Poor Underserved 2010, 21, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Courneya, K.S.; Estabrooks, P.A.; Nigg, C.R. A Simple Reinforcement Strategy for Increasing Attendance at a Fitness Facility. Health Educ. Behav. 1997, 24, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Cyr, A.; Munroe-Chandler, K.; Gammage, K. Might Plight: The Social Anxiety Felt by Men in the Weightlifting Environment. ACSM’S Health Fit. J. 2019, 23, 14–18. [Google Scholar] [CrossRef]
- Doğan, C. Training at the Gym, Training for Life: Creating Better Versions of the Self Through Exercise. Eur. J. Psychol. 2015, 11, 442–458. [Google Scholar] [CrossRef]
- Emeterio, I.C.S.; García-Unanue, J.; Iglesias-Soler, E.; Felipe, J.L.; Gallardo, L. Prediction of Abandonment in Spanish Fitness Centres. Eur. J. Sport Sci. 2019, 19, 217–224. [Google Scholar] [CrossRef]
- Evans, M.B.; Graupensperger, S.; Benson, A.J.; Eys, M.; Hastings, B.; Gottschall, J.S. Groupness Perceptions and Basic Need Satisfaction: Perceptions of Fitness Groups and Experiences within Club Environments. Group Dyn. Theory Res. Pract. 2019, 23, 1–15. [Google Scholar] [CrossRef]
- Evans, M.B.; Shanahan, E.; Leith, S.; Litvak, N.; Wilson, A.E. Living for Today or Tomorrow? Self-Regulation amidst Proximal or Distal Exercise Outcomes. Appl. Psychol. Health Well Being 2019, 11, 304–327. [Google Scholar] [CrossRef]
- Faulkner, G.; Dale, L.P.; Lau, E. Examining the Use of Loyalty Point Incentives to Encourage Health and Fitness Centre Participation. Prev. Med. Rep. 2019, 14, 100831. [Google Scholar] [CrossRef] [PubMed]
- Fieril, K.P.; Olsén, M.F.; Glantz, A.; Larsson, M. Experiences of Exercise during Pregnancy among Women Who Perform Regular Resistance Training: A Qualitative Study. Phys. Ther. 2014, 94, 1135–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fredslund, E.K.; Leppin, A. Can the Easter Break Induce a Long-Term Break of Exercise Routines? An Analysis of Danish Gym Data Using a Regression Discontinuity Design. BMJ Open 2019, 9, e024043. [Google Scholar] [CrossRef] [Green Version]
- Gjestvang, C.; Stensrud, T.; Haakstad, L.A.H. Are Changes in Physical Fitness, Body Composition and Weight Associated with Exercise Attendance and Dropout among Fitness Club Members? Longitudinal Prospective Study. BMJ Open 2019, 9, e027987. [Google Scholar] [CrossRef] [Green Version]
- Harada, K.; Shibata, A.; Ishii, K.; Liao, Y.; Oka, K. Perceived and Objectively Measured Access to Strength-Training Facilities and Strength-Training Behavior. Ann. Behav. Med. 2014, 48, 120–124. [Google Scholar] [CrossRef]
- Heinrich, K.M.; Carlisle, T.; Kehler, A.; Cosgrove, S.J. Mapping Coaches’ Views of Participation in CrossFit to the Integrated Theory of Health Behavior Change and Sense of Community. Fam. Community Health 2017, 40, 24–27. [Google Scholar] [CrossRef] [Green Version]
- Hosek, P.P. Self-Motivation and Exercise Adherence in Adult Women. Ph.D. Thesis, University of Houston, Houston, TX, USA, May 1997. [Google Scholar]
- Hurrell, R.M. Factors Associated with Regular Exercise. Percept. Mot. Ski. 1997, 84, 871–874. [Google Scholar] [CrossRef]
- Jang, W.Y.; Choi, K. Factors Influencing Choice When Enrolling at a Fitness Center. Soc. Behav. Pers. 2018, 46, 1043–1056. [Google Scholar] [CrossRef]
- Jekauc, D.; Völkle, M.; Wagner, M.O.; Mess, F.; Reiner, M.; Renner, B. Prediction of Attendance at Fitness Center: A Comparison between the Theory of Planned Behavior, the Social Cognitive Theory, and the Physical Activity Maintenance Theory. Front. Psychol. 2015, 6, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Kaushal, N.; Rhodes, R.E.; Meldrum, J.T.; Spence, J.C. The Role of Habit in Different Phases of Exercise. Br. J. Health Psychol. 2017, 22, 429–448. [Google Scholar] [CrossRef] [PubMed]
- Kaushal, N.; Rhodes, R. Exercise Habit Formation in New Gym Members: A Longitudinal Study. J. Behav. Med. 2015, 38, 652–663. [Google Scholar] [CrossRef] [PubMed]
- Kirkegaard, K.L. Part 2: Portray of the active fitness customers: Motives for training, satisfaction and self-reported health [Delrapport 2: Portræt af de aktive fitnesskunder: Træningsmotiver, tilfredshed og selvvurderet sundhed]. In Health for Millions [Sundhed for Millioner]; The Danish Institute for Sports Studies [Idrættens Analyseinstitut]: Copenhagen, Denmark, 2009; ISBN 978-87-92120-16-8. [Google Scholar]
- Kirkegaard, K.L.; Østerlund, K. Part 5: Fitness culture between sports club and business: Active fitness users motives for training, satisfaction and self-reported health [Delrapport 5: Fitnesskultur mellem forening og forretning: Aktive fitnessudøveres træningsmotiver, tilfredshed og selvvurderede sundhed]. In Health for Millions [Sundhed for Millioner]; The Danish Institute for Sports Studies [Idrættens Analyseinstitut]: Copenhagen, Denmark, 2010; ISBN 978-87-92120-24-3. [Google Scholar]
- Klein, J. Make a Positive Connection. Am. Fit. 2002, 20, 35. [Google Scholar]
- Kruisselbrink, L.D.; Dodge, A.M.; Swanburg, S.L.; MacLeod, A.L. Influence of Same-Sex and Mixed-Sex Exercise Settings on the Social Physique Anxiety and Exercise Intentions of Males and Females. J. Sport Exerc. Psychol. 2004, 26, 616. [Google Scholar] [CrossRef]
- Larson, H.K.; McFadden, K.; McHugh, T.L.F.; Berry, T.R.; Rodgers, W.M. You Can’t Always Get What You Want: Expectations, Outcomes, and Adherence of New Exercisers. Qual. Res. Sport Exerc. Health 2017, 9, 389–402. [Google Scholar] [CrossRef]
- León-Quismondo, J.; García-Unanue, J.; Burillo, P. Service Perceptions in Fitness Centers: IPA Approach by Gender and Age. Int J. Environ. Res. Public Health 2020, 17, 2844. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Fernandez, J.; Staniland, B.; Sanchez, I.; Iturriaga, T.; Ayuso, M.; Horton, E.; Mann, S.; Liguori, G.; Atkinson, L.; Jimenez, A. A Weekly Structured Physical Activity Program Enhances Short-Term Retention Of Middle-Aged Adult Fitness Centre Users: 284 Board #125 May 30 9: 30 AM–11: 00 AM. Med. Sci. Sports Exerc. 2018, 50, 55. [Google Scholar] [CrossRef]
- Lübcke, A.; Martin, C.; Hellström, K. Older Adults’ Perceptions of Exercising in a Senior Gym. Act. Adapt. Aging 2012, 36, 131–146. [Google Scholar] [CrossRef]
- Malek, M.H.; Nalbone, D.P.; Berger, D.E.; Coburn, J.W. Importance of Health Science Education for Personal Fitness Trainers. J. Strength Cond. Res. 2002, 16, 19–24. [Google Scholar]
- Manning, K.M.; Chmelo, E.; Yates, B.A.; Conteh, P.; Morey, M. Adopting a Functional Fitness Approach to Membership. J. Act. Aging 2019, 18, 74–79. [Google Scholar]
- Martin, P.; McCann, T.V. Exercise and Older Women’s Wellbeing. Contemp. Nurse 2005, 20, 169–179. [Google Scholar] [CrossRef]
- Melton, D.I.; Dail, T.K.; Katula, J.A.; Mustian, K.M. The Current State of Personal Training: Managers’ Perspectives. J. Strength Cond. Res. 2010, 24, 3173–3179. [Google Scholar] [CrossRef]
- Melton, D.I.; Katula, J.A.; Mustian, K.M. The Current State of Personal Training: An Industry Perspective of Personal Trainers in a Small Southeast Community. J. Strength Cond. Res. 2008, 22, 883–889. [Google Scholar] [CrossRef] [Green Version]
- Middelkamp, J.; van Rooijen, M.; Wolfhagen, P.; Steenbergen, B. The Effects of Two Self-Regulation Interventions to Increase Self-Efficacy and Group Exercise Behavior in Fitness Clubs. J. Sports Sci. Med. 2016, 15, 358–364. [Google Scholar] [PubMed]
- Milner, C. Equipping Your Fitness Centre for Older Adults. Fit. Bus. Can. 2005, 6, 58–59. [Google Scholar]
- Mullen, S.P.; Whaley, D.E. Age, Gender, and Fitness Club Membership: Factors Related to Initial Involvement and Sustained Participation. Int. J. Sport Exerc. Psychol. 2010, 8, 24–35. [Google Scholar] [CrossRef]
- Østerlund, K.; Kirkegaard, K.L. Part 4 Fitness centers within company sports—Portray of the active fitness users: Motives for training, satisfaction and self-reported health [Delrapport 4: Fitnesscentre i firmaidrætten—Portræt af de aktive medlemmer: Træningsmotiver, tilfredshed og selvvurderet sundhed]. In Health for Millions [Sundhed for Millioner]; The Danish Institute for Sports Studies [Idrættens Analyseinstitut]: Copenhagen, Denmark, 2010; ISBN 978-87-92120-29-8. [Google Scholar]
- Østerlund, K.; Kirkegaard, K.L. Part 3: Fitness in sports clubs/associations—Portray of the active fitness users: Motives for training, satisfaction and self-reported health [Delrapport 3 Foreningsfitness—Portæt af de aktive medlemmer: Træningsmotiver, tilfredshed og selvvurderet sundhed]. In Health for Millions [Sundhed for Millioner]; The Danish Institute for Sports Studies [Idrættens Analyseinstitut]: Copenhagen, Denmark, 2010; ISBN 978-87-92120-26-7. [Google Scholar]
- Pettigrew, S.; Burton, E.; Farrier, K.; Hill, A.M.; Bainbridge, L.; Lewin, G.; Airey, P.; Hill, K. A Typology of Factors Influencing Seniors’ Participation in Strength Training in Gyms and Fitness Centers. J. Aging Phys. Act. 2018, 26, 492–498. [Google Scholar] [CrossRef]
- Rabiee, F.; Robbins, A.; Khan, M. Gym for Free: The Short-Term Impact of an Innovative Public Health Policy on the Health and Wellbeing of Residents in a Deprived Constituency in Birmingham, UK. Health Educ. J. 2015, 74, 691–704. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, R.L.; Overgaard, C.; Bøggild, H.; Thomsen, L.L.H. An Explorative Evaluation Study of the Mechanisms Underlying a Community-based Fitness Centre in Denmark—Why Do Residents Participate and Keep up the Healthy Activities? Health Soc. Care Community 2018, 26, 898–907. [Google Scholar] [CrossRef] [PubMed]
- Rekieta, S.K. Exercise Relapse Prevention: The Efficacy of a Motivational Interview Intervention. Ph.D. Thesis, University of Memphis, Memphis, TN, USA, 2002. [Google Scholar]
- Riseth, L.; Nøst, T.H.; Nilsen, T.I.L.; Steinsbekk, A. Long-Term Members’ Use of Fitness Centers: A Qualitative Study. BMC Sports Sci. Med. Rehabil. 2019, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.; Teixeira, D.S.; Neiva, H.P.; Cid, L.; Monteiro, D. The Bright and Dark Sides of Motivation as Predictors of Enjoyment, Intention, and Exercise Persistence. Scand. J. Med. Sci. Sports 2020, 30, 787–800. [Google Scholar] [CrossRef]
- Rodrigues, F.; Teixeira, D.S.; Cid, L.; Monteiro, D. Have You Been Exercising Lately? Testing the Role of Past Behavior on Exercise Adherence. J. Health Psychol. 2019, 135910531987824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, F.; Teixeira, D.S.; Cid, L.; Machado, S.; Monteiro, D. The Role of Dark-side of Motivation and Intention to Continue in Exercise: A Self-determination Theory Approach. Scand. J. Psychol. 2019, 60, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.L.K.; Østergren, P.; Cormie, P.; Ragle, A.-M.; Sønksen, J.; Midtgaard, J. “Kicked out into the Real World”: Prostate Cancer Patients’ Experiences with Transitioning from Hospital-Based Supervised Exercise to Unsupervised Exercise in the Community. Support. Care Cancer 2019, 27, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Schvey, N.A.; Sbrocco, T.; Bakalar, J.L.; Ress, R.; Barmine, M.; Gorlick, J.; Pine, A.; Stephens, M.; Tanofsky-Kraff, M. The Experience of Weight Stigma among Gym Members with Overweight and Obesity. Stigma Health 2017, 2, 292–306. [Google Scholar] [CrossRef]
- Schwetschenau, H.M.; O’Brien, W.H.; Cunningham, C.J.L.; Jex, S.M. Barriers to Physical Activity in an On-Site Corporate Fitness Center. J. Occup. Health Psychol. 2008, 13, 371–380. [Google Scholar] [CrossRef]
- Souza, B.J.; Ebbeck, V. Perspectives on Increasing Positive Attitudes Toward Larger Members in Fitness Centers. J. Appl. Sport Psychol. 2018, 30, 96–118. [Google Scholar] [CrossRef]
- Sperandei, S.; Vieira, M.C.; Reis, A.C. Adherence to Physical Activity in an Unsupervised Setting: Explanatory Variables for High Attrition Rates among Fitness Center Members. J. Sci. Med. Sport 2016, 19, 916–920. [Google Scholar] [CrossRef]
- Springer, J.B.; Lamborn, S.D.; Pollard, D.M. Maintaining Physical Activity over Time: The Importance of Basic Psychological Need Satisfaction in Developing the Physically Active Self. Am. J. Health Promot. 2013, 27, 284–293. [Google Scholar] [CrossRef]
- Stein, J. Bodywork. A swing toward families: Gyms are taking a fresh look at classes for kids and parents to encourage old and young to plan their exercise time together. Los Angeles Times-Southern California Edition, 17 June 2003; F7. [Google Scholar]
- Stein, J. Bodywork. Bracing for the attack of the gym “Newbies”. Los Angeles Times-Southern California Edition, 17 June 2003; F1–F5. [Google Scholar]
- Stenson, J. Workout partners: Health clubs and videos are incorporating kids into routines so time-strapped parents can strollercize, lift weights or do yoga with children in tow. Los Angeles Times-Southern California Edition, 14 June 2005; F9. [Google Scholar]
- Stewart, B.; Smith, A.C.T. The Significance of Critical Incidents in Explaining Gym Use amongst Adult Populations. Qual. Res. Sport Exerc. Health 2014, 6, 45–61. [Google Scholar] [CrossRef]
- Strelsand, B. No Six-Packs here, Please. U.S. News World Rep. 2007, 142, 66–67. [Google Scholar]
- Thomson, D.; McAdoo, K. An Exploration into the Development of Motivation to Exercise in a Group of Male UK Regular Gym Users. Int. J. Sport Exerc. Psychol. 2016, 14, 414–429. [Google Scholar] [CrossRef]
- Ulseth, A.-L.B. New Opportunities—Complex Motivations: Gender Differences in Motivation for Physical Activity in the Context of Sports Clubs and Fitness Centers. Int. J. Appl. Sports Sci. 2008, 20, 44–66. [Google Scholar]
- Unger, J.B.; Johnson, C.A. Social Relationships and Physical Activity in Health Club Members. Am. J. Health Promot. 1995, 9, 340–343. [Google Scholar] [CrossRef] [PubMed]
- Van der Swaluw, K.; Lambooij, M.S.; Mathijssen, J.J.P.; Schipper, M.; Zeelenberg, M.; Berkhout, S.; Polder, J.J.; Prast, H.M. Commitment Lotteries Promote Physical Activity Among Overweight Adults—A Cluster Randomized Trial. Ann. Behav. Med. 2018, 52, 342–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Swaluw, K.; Lambooij, M.S.; Mathijssen, J.J.P.; Schipper, M.; Zeelenberg, M.; Berkhout, S.; Polder, J.J.; Prast, H.M. Physical Activity after Commitment Lotteries: Examining Long-Term Results in a Cluster Randomized Trial. J. Behav. Med. 2018, 41, 483–493. [Google Scholar] [CrossRef] [Green Version]
- Vlachopoulos, S.P.; Neikou, E. A Prospective Study of the Relationships of Autonomy, Competence, and Relatedness with Exercise Attendance, Adherence, and Dropout. J. Sports Med. Phys. Fit. 2007, 47, 475–482. [Google Scholar]
- Wayment, H.A.; McDonald, R.L. Sharing a Personal Trainer: Personal and Social Benefits of Individualized, Small-Group Training. J. Strength Cond. Res. 2017, 31, 3137–3145. [Google Scholar] [CrossRef]
- Whiteman-Sandland, J.; Hawkins, J.; Clayton, D. The Role of Social Capital and Community Belongingness for Exercise Adherence: An Exploratory Study of the CrossFit Gym Model. J. Health Psychol. 2018, 23, 1545–1556. [Google Scholar] [CrossRef]
- Wininger, S.R. Instructors’ and Classroom Characteristics Associated with Exercise Enjoyment by Females. Percept. Mot. Ski. 2002, 94, 395–398. [Google Scholar] [CrossRef]
- Yin, Z. Setting for Exercise and Concerns about Body Appearance of Women Who Exercise. Percept. Mot. Ski. 2001, 93, 851–855. [Google Scholar] [CrossRef]
- Sharon-David, H.; Siekanska, M.; Tenenbaum, G. Are Gyms Fit for All? A Scoping Review of the Barriers and Facilitators to Gym-Based Exercise Participation Experienced by People with Physical Disabilities. Perform. Enhanc. Health 2020, 100170. [Google Scholar] [CrossRef]
- Rimmer, J.H. The Conspicuous Absence of People with Disabilities in Public Fitness and Recreation Facilities: Lack of Interest or Lack of Access? Am. J. Health Promot. 2005, 19, 327–329. [Google Scholar] [CrossRef] [PubMed]
- Calder, A.M.; Mulligan, H.F. Measurement Properties of Instruments That Assess Inclusive Access to Fitness and Recreational Sports Centers: A Systematic Review. Disabil. Health J. 2014, 7, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Reeve, D. Psycho-emotional disablism and internalised oppression. In Disabling Barriers—Enabling Environments; Swain, J., French, S., Barnes, C., Thomas, C., Eds.; SAGE: Los Angeles, CA, USA, 2014; ISBN 978-1-4462-5898-9. [Google Scholar]
- Morgan, F.; Battersby, A.; Weightman, A.L.; Searchfield, L.; Turley, R.; Morgan, H.; Jagroo, J.; Ellis, S. Adherence to Exercise Referral Schemes by Participants—What Do Providers and Commissioners Need to Know? A Systematic Review of Barriers and Facilitators. BMC Public Health 2016, 16, 227. [Google Scholar] [CrossRef] [PubMed]
- The National Center on Health, Physical Activity and Disability (NCHPAD). Community Health Inclusion Sustainability Planning Guide An. Addendum to A Sustainability Planning Guide for Healthy Communities; The National Center on Health, Physical Activity and Disability (NCHPAD): Birmingham, UK, 2014. [Google Scholar]
| Context Factor Categories | Description | |
|---|---|---|
| 1 | The Fitness Centre Setting | The physical environment in the specific fitness centre/gym, e.g., surrounding area, buildings, room arrangement, and fitness equipment. |
| 2 | The Fitness Centre User Characteristics | The ‘personal factors’ according to ICF [40] combined with their physical ability, e.g., bodily performance and the individual participant’s opinions and feelings. |
| 3 | The Fitness Instructor’s/Staff Characteristics | The front-line personnel in the fitness centre and their qualifications, e.g., knowledge, education, appearance, communication skills, and courtesy, etc. |
| 4 | The Fitness Centre User—Instructor/Management Relationship | The direct or indirect interaction between the participant and the instructor/management who represent the fitness centre as a whole with respect to personal relations, teaching, and prejudices when interacting as a representative of the specific fitness centre, together with the rules, policies, membership terms and conditions, artefacts, culture, and the atmosphere of the place. |
| 5 | The Fitness/Exercise Characteristics | The different types of fitness exercises and how they are performed, e.g., individual exercising, types of classes, planning, specific exercises, etc. |
| 6 | Other Relationships | The relationship or direct and indirect interactions with other people than the staff in the fitness centre, e.g., strangers, familiar faces, friends and family, or personal assistants. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikolajsen, H.; Sandal, L.F.; Juhl, C.B.; Troelsen, J.; Juul-Kristensen, B. Barriers to, and Facilitators of, Exercising in Fitness Centres among Adults with and without Physical Disabilities: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 7341. https://doi.org/10.3390/ijerph18147341
Nikolajsen H, Sandal LF, Juhl CB, Troelsen J, Juul-Kristensen B. Barriers to, and Facilitators of, Exercising in Fitness Centres among Adults with and without Physical Disabilities: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(14):7341. https://doi.org/10.3390/ijerph18147341
Chicago/Turabian StyleNikolajsen, Helene, Louise Fleng Sandal, Carsten Bogh Juhl, Jens Troelsen, and Birgit Juul-Kristensen. 2021. "Barriers to, and Facilitators of, Exercising in Fitness Centres among Adults with and without Physical Disabilities: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 14: 7341. https://doi.org/10.3390/ijerph18147341