
Effect of Glycated Hemoglobin (HbA1c) and Duration of Disease on Lung Functions in Type 2 Diabetic Patients

 ,
,
Abstract
:1. Introduction
2. Subjects ad Methods
2.1. Exclusion Criteria
2.2. Measurements of HbA1c
2.3. Spirometry
2.4. Statistical Analysis
3. Results
3.1. Demographic and Biochemical Characteristics
3.2. Pulmonary Function Test
3.3. Duration of Diabetes 5–10 Years (Pulmonary Function Tests)
3.4. Duration of Diabetes >10 Years and Pulmonary Function Tests
3.5. HbA1c < 8 and Pulmonary Function Tests
3.6. HbA1c > 8 and Pulmonary Function Tests
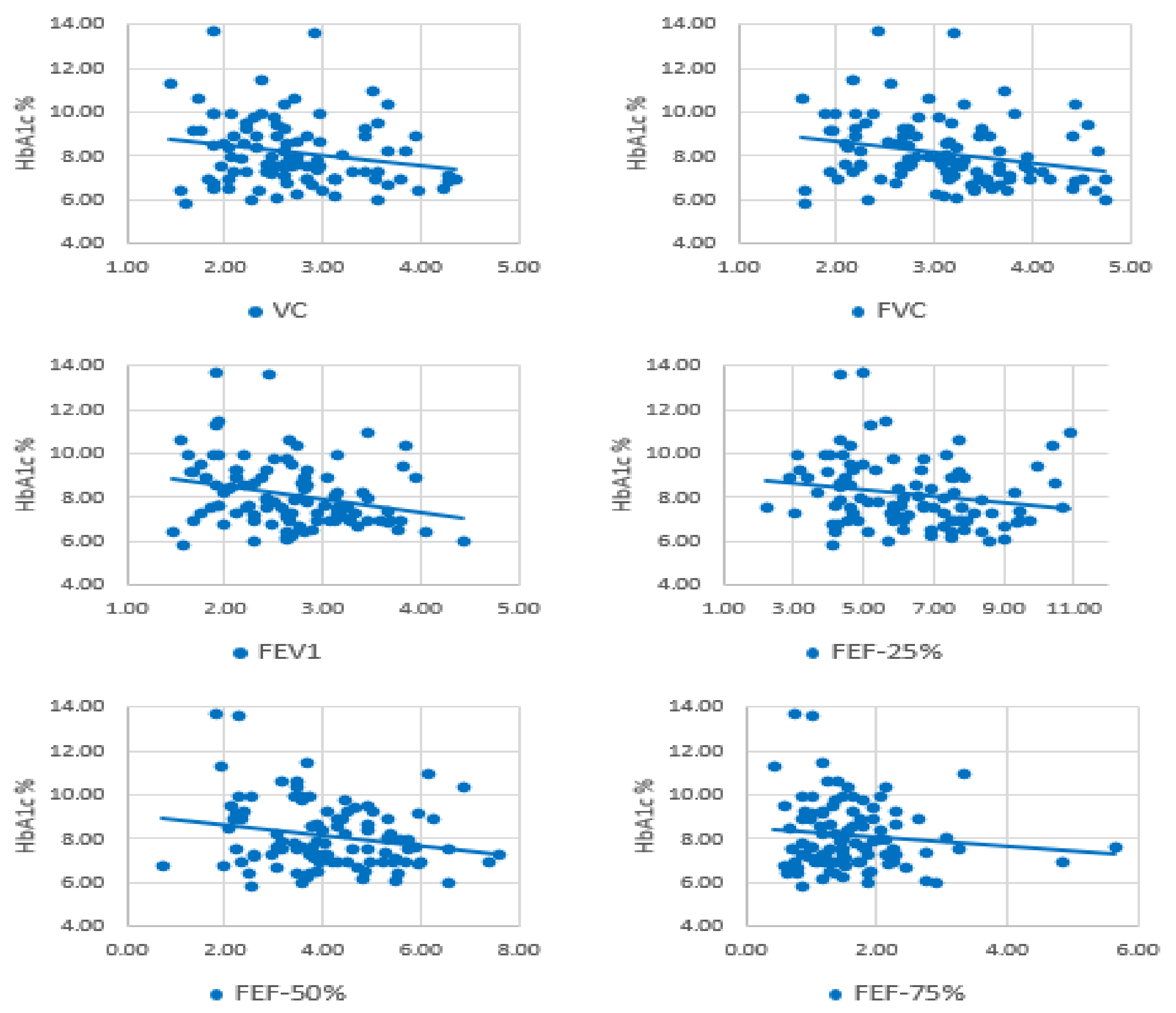
3.7. Correlation Analysis (HbA1c and Lung Function Parameters)
3.8. Correlation Analysis (Duration of Diabetes and Lung Function Parameters)
4. Discussion
Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, M.; Liu, X.; Liu, W.; Lu, Y.; Cheng, J.; Chen, Y. β cell aging and age-related diabetes. Aging 2021, 13, 7691–7706. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.; Zhong, W.; Lin, X.; Lin, S.; Lin, X.; Li, X.; Chen, T. Association between sedentary lifestyle and risks of metabolic syndrome and diabetes mellitus type 2. Zhonghua Liu Xing Bing Xue Za Zhi 2014, 35, 1235–1240. [Google Scholar] [PubMed]
- Meo, S.A.; Usmani, A.M.; Qalbani, E. Prevalence of type 2 diabetes in the Arab world: Impact of GDP and energy consumption. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 1303–1312. [Google Scholar] [PubMed]
- Meo, S.A.; Memon, A.N.; Sheikh, S.A.; Rouq, F.A.; Usmani, A.; Hassan, A.; Arian, S.A. Effect of environmental air pollution on type 2 diabetes mellitus. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 123–128. [Google Scholar]
- International Diabetes Federation (IDF.) Diabetes Atlas. Available online: https://www.idf.org/e-library/epidemiology-research/diabetes-atlas/159-idf-diabetes-atlas-ninth-edition-2019.html (accessed on 2 March 2021).
- Duwayri, Y.; Jordan, W.D. Diabetes, dysglycemia, and vascular surgery. J. Vasc. Surg. 2020, 71, 701–711. [Google Scholar] [CrossRef]
- Kitada, M.; Zhang, Z.; Mima, A.; King, G.L. Molecular mechanisms of diabetic vascular complications. J. Diabetes Investig. 2010, 1, 77–89. [Google Scholar] [CrossRef] [Green Version]
- Kolahian, S.; Leiss, V.; Nürnberg, B. Diabetic lung disease: Fact or fiction? Rev. Endocr. Metab. Disord. 2019, 20, 303–319. [Google Scholar] [CrossRef]
- Goldman, M.D. Lung Dysfunction in Diabetes. Diabetes Care 2003, 26, 1915–1918. [Google Scholar] [CrossRef] [Green Version]
- Ehrlich, S.F.; Quesenberry, C.P.; Eeden, S.K.V.D.; Shan, J.; Ferrara, A. Patients Diagnosed With Diabetes Are at Increased Risk for Asthma, Chronic Obstructive Pulmonary Disease, Pulmonary Fibrosis, and Pneumonia but Not Lung Cancer. Diabetes Care 2009, 33, 55–60. [Google Scholar] [CrossRef] [Green Version]
- Meo, S.A.; Drees, A.M.A.; Ahmed, J.; Shah, S.F.A.; Al-Regaiey, K.; Husain, A.; Al-Rubean, K. Effect of Duration of Disease on Ventilatory Function in an Ethnic Saudi Group of Diabetic Patients. J. Diabetes Sci. Technol. 2007, 1, 711–717. [Google Scholar] [CrossRef] [Green Version]
- Meo, S.A.; Aldeghaither, M.; Alnaeem, K.A.; Alabdullatif, F.S.; AlZamil, A.F.; Alshunaifi, A.I.; Alfayez, A.S.; AlMahmoud, M.; Meo, A.S.; El-Mubarak, A.H. Effect of motor vehicle pollution on lung function, fractional exhaled nitric oxide and cognitive function among school adolescents. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 8678–8686. [Google Scholar]
- Meo, S.A.; Iqbal, M.; Usmani, A.M.; Almana, A.A.; Alrashed, A.H.; Al-Regaiey, K.A. Effect of wearing cotton towel Ihram and plain Ihram on lung function among Hajj Pilgrims. Pak. J. Med. Sci. 2019, 35, 893–898. [Google Scholar] [CrossRef] [Green Version]
- Meo, S.; Abukhalaf, A.; Alomar, A.; Alessa, O.; Sumaya, O.; Meo, A. Prevalence of Prediabetes and Type 2 Diabetes Mellitus in Football Players: A Novel Multi Football Clubs Cross Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 1763. [Google Scholar] [CrossRef]
- American Diabetes Association. Classification and Diagnosis of Diabetes:Standards of Medical Care in Diabetes—2018. Diabetes Care 2017, 41, S13–S27. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Li, C.; Xu, Y.; He, B.; Hu, M.; Cao, G.; Li, L.; Wu, S.; Wang, X.; Zhang, C.; et al. Hyperglycemia and Correlated High Levels of Inflammation Have a Positive Relationship with the Severity of Coronavirus Disease 2019. Mediat. Inflamm. 2021, 2021, 1–9. [Google Scholar] [CrossRef]
- Sushil, K.; Mandira, M. Alteration of Pulmonary Functions in Male Adults with Type 2 Diabetes Mellitus. World Fam. Med. J. Middle East J. Fam. Med. 2019, 17, 4–8. [Google Scholar] [CrossRef]
- Mondal, C.; Ray, A.; Kumar, A. A study of pulmonary function tests in type 2 diabetes mellitus patients of the sub-Himalayan plain area of Darjeeling district. Int. J. Sci. Res. 2019, 8, 2277–8179. [Google Scholar]
- Zaman, S.; Mallick, S. Evaluation of pulmonary functions in type 2 diabetes mellitus and its age and gender-specific changes on the population of urban and suburban areas of Kolkata: A hospital-based study. Int. J. Sci. Res. 2018, 7, 10. [Google Scholar]
- Meo, S.A.; Al-Drees, A.M.; Arif, M.; Al-Rubean, K. Lung function in type 2 Saudi diabetic patients. Saudi Med. J. 2006, 27, 338–343. [Google Scholar]
- Díez-Manglano, J.; Samper, U.A. Pulmonary function tests in type 2 diabetes: A meta-analysis. ERJ Open Res. 2021, 7, 00371–02020. [Google Scholar] [CrossRef]
- Kumari, D.H.; Nataraj, S.M.; Devaraj, H.S. Correlation of duration of diabetes and pulmonary function tests in type 2 diabetes mellitus patients. Int. J. Biol. Med. Res. 2011, 2, 1168–1170. [Google Scholar]
- Chidri, S.; Vidya, G. Assessment of pulmonary functions in type 2 diabetes mellitus: Its correlation with glycemic control and body mass index. Natl. J. Physiol. Pharm. Pharmacol. 2020, 10, 553–556. [Google Scholar] [CrossRef]
- Anandhalakshmi, S.; Manikandan, S.; Ganeshkumar, P.; Ramachandran, C. Alveolar Gas Exchange, and Pulmonary Functions in Patients with Type II Diabetes Mellitus. J. Clin. Diagn. Res. 2013, 7, 1874–1881. [Google Scholar] [CrossRef]
- Tai, H.; Jiang, X.-L.; Yao, S.-C.; Liu, Y.; Wei, H.; Li, L.-B.; Jiao, Z.-J.; Wang, T.-Q.; Kuang, J.-S.; Jia, L.-Q. Vascular Endothelial Function as a Valid Predictor of Variations in Pulmonary Function in T2DM Patients Without Related Complications. Front. Endocrinol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Nurwidya, F.; Faisal, H.; Antariksa, B.; Yunus, F. Lung diffusion capacity disorder in indonesian patients with Type 2 diabetes mellitus and the related factors. J. Nat. Sci. Biol. Med. 2018, 9, 222. [Google Scholar] [CrossRef] [Green Version]
- Sonoda, N.; Morimoto, A.; Tatsumi, Y.; Asayama, K.; Ohkubo, T.; Izawa, S.; Ohno, Y. The association between glycemic control and lung function impairment in individuals with diabetes: The Saku study. Diabetol. Int. 2019, 10, 213–218. [Google Scholar] [CrossRef]
- Meo, S.A.; Al-Drees, A.M.; Arif, M.; Shah, F.A.; Al-Rubean, K. Assessment of respiratory muscles endurance in diabetic pa-tients. Saudi Med. J. 2006, 27, 223–226. [Google Scholar]
- Fuso, L.; Pitocco, D.; Longobardi, A.; Zaccardi, F.; Contu, C.; Pozzuto, C.; Basso, S.; Varone, F.; Ghirlanda, G.; Incalzi, R.A. Re-duced respiratory muscle strength and endurance in type 2 diabetes mellitus. Diabetes Metab. Res. Rev. 2012, 28, 370–375. [Google Scholar] [CrossRef]
- Kabitz, H.-J.; Sonntag, F.; Walker, D.; Schwoerer, A.; Walterspacher, S.; Kaufmann, S.; Beuschlein, F.; Seufert, J.; Windisch, W. Diabetic polyneuropathy is associated with respiratory muscle impairment in type 2 diabetes. Diabetologia 2007, 51, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Fang, Y.; Guo, X.; Gao, Q.; Ye, H.; Guan, S. Diaphragm dysfunction and expressions of calcium regulatory proteins in diabetic rats. J. South. Med. Univ. 2013, 33, 177–181. [Google Scholar]
- Sugimoto, K.; Ikegami, H.; Takata, Y.; Katsuya, T.; Fukuda, M.; Akasaka, H.; Tabara, Y.; Osawa, H.; Hiromine, Y.; Rakugi, H. Glycemic Control and Insulin Improve Muscle Mass and Gait Speed in Type 2 Diabetes: The MUSCLES-DM Study. J. Am. Med. Dir. Assoc. 2021, 22, 834–838. [Google Scholar] [CrossRef]
- Zheng, H.; Wu, J.; Jin, Z.; Yan, L.-J. Potential Biochemical Mechanisms of Lung Injury in Diabetes. Aging Dis. 2017, 8, 7–16. [Google Scholar] [CrossRef] [Green Version]
- McKeever, T.M.; Weston, P.J.; Hubbard, R.; Fogarty, A. Lung Function and Glucose Metabolism: An Analysis of Data from the Third National Health and Nutrition Examination Survey. Am. J. Epidemiol. 2005, 161, 546–556. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Ma, Y.; Tong, X.; Zhang, Y.; Fan, H. Diabetes Mellitus Contributes to Idiopathic Pulmonary Fibrosis: A Review from Clinical Appearance to Possible Pathogenesis. Front. Public Health 2020, 8, 8. [Google Scholar] [CrossRef]
- Klein, O.L.; Krishnan, J.A.; Glick, S.; Smith, L.J. Systematic review of the association between lung function and Type 2 diabetes mellitus. Diabet. Med. 2010, 27, 977–987. [Google Scholar] [CrossRef]
- Ofulue, A.F.; Thurlbeck, W.M. Experimental Diabetes and the Lung: II. In Vivo Connective Tissue Metabolism. Am. Rev. Respir. Dis. 1988, 138, 284–289. [Google Scholar] [CrossRef]
- Weynand, B.; Jonckheere, A.; Frans, A.; Rahier, J. Diabetes mellitus Induces a Thickening of the Pulmonary Basal Lamina. Respiration 1999, 66, 14–19. [Google Scholar] [CrossRef]
- Fogarty, A.W.; Jones, S.; Britton, J.R.; Lewis, S.A.; McKeever, T.M. Systemic inflammation and decline in lung function in a general population: A prospective study. Thorax 2007, 62, 515–520. [Google Scholar] [CrossRef] [Green Version]
- Hancox, R.J.; Poulton, R.; Greene, J.M.; Filsell, S.; McLachlan, C.R.; Rasmussen, F.; Taylor, D.R.; Williams, M.J.A.; Williamson, A.; Sears, M.R. Systemic inflammation and lung function in young adults. Thorax 2007, 62, 1064–1068. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Parameters | Diabetic Group (n = 101) | Control Group (n = 101) | p-Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Age (years) | 55.50 ± 5.99 | 54.88 ± 6.76 | 0.489 |
| Height (cm) | 166.02 ± 6.44 | 166.11 ± 6.04 | 0.919 |
| Weight (kg) | 68.84 ± 4.64 | 68.21 ± 5.77 | 0.653 |
| BMI (kg/m2) | 25.04 ± 2.11 | 24.34 ± 1.33 | 0.319 |
| HbA1c (%) | 8.19 ± 1.48 | 6.01 ± 0.24 | <0.001 * |
| Fasting Blood Glucose (mmol/L) | 9.12 ± 3.12 | 5.21 ± 0.11 | <0.001 * |
| Parameters | Diabetic Group (n = 14) | Control Group (n = 14) | p-Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| VC (L) | 2.85 ± 0.65 | 3.09 ± 0.56 | 0.303 |
| FVC (L) | 3.15 ± 0.66 | 3.47 ± 0.59 | 0.189 |
| FEV1 (L/Sec) | 2.75 ± 0.63 | 2.98 ± 0.47 | 0.278 |
| FEV1/FVC Ratio (%) | 88.98 ± 6.23 | 87.65 ± 5.21 | 0.548 |
| PEFR (L/Sec) | 6.88 ± 1.82 | 7.12 ± 1.67 | 0.720 |
| FEF-25% (L/Sec) | 6.49 ± 1.96 | 6.77 ± 1.53 | 0.672 |
| FEF-50% (L/Sec) | 4.52 ± 1.79 | 4.76 ± 1.06 | 0.907 |
| FEF-75% (L/Sec) | 1.71 ± 1.11 | 1.66 ± 0.69 | 0.673 |
| Parameters | Diabetic Group (n = 26) | Control Group (n = 26) | p-Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| VC (L) | 2.72 ± 0.80 | 2.91 ± 0.56 | 0.328 |
| FVC (L) | 3.08 ± 0.91 | 3.34 ± 0.79 | 0.283 |
| FEV1 (L/Sec) | 2.58 ± 0.75 | 2.96 ± 0.71 | 0.068 |
| FEV1/FVC Ratio (%) | 86.39 ± 6.79 | 91.47 ± 5.97 | 0.006 * |
| PEFR (L/Sec) | 6.55 ± 2.28 | 7.14 ± 2.15 | 0.345 |
| FEF-25% (L/Sec) | 6.05 ± 2.24 | 6.83 ± 1.95 | 0.184 |
| FEF-50% (L/Sec) | 3.60 ± 1.29 | 4.90 ± 1.30 | 0.001 * |
| FEF-75% (L/Sec) | 1.35 ± 0.61 | 1.93 ± 0.74 | 0.003 * |
| Parameters | Diabetic Group (n = 61) | Control Group (n = 61) | p-Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| VC (L) | 2.64 ± 0.60 | 2.85 ± 0.62 | 0.055 |
| FVC (L) | 3.07 ± 0.75 | 3.29 ± 0.78 | 0.106 |
| FEV1 (L/Sec) | 2.64 ± 0.61 | 2.90 ± 0.68 | 0.029 * |
| FEV1/FVC Ratio (%) | 89.25 ± 7.14 | 91.35 ± 6.12 | 0.311 |
| PEFR (L/Sec) | 6.56 ± 1.97 | 7.08 ± 1.94 | 0.805 |
| FEF-25% (L/Sec) | 6.31 ± 1.88 | 6.80 ± 1.85 | 0.636 |
| FEF-50% (L/Sec) | 4.23 ± 1.26 | 4.73 ± 1.40 | 0.483 |
| FEF-75% (L/Sec) | 1.62 ± 0.80 | 1.86 ± 0.74 | 0.747 |
| Parameters | Diabetic Group (n = 58) | Control Group (n = 58) | p-Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| VC (L) | 2.78 ± 0.67 | 8.94 ± 0.71 | 0.309 |
| FVC (L) | 3.24 ± 0.75 | 3.34 ± 0.76 | 0.502 |
| FEV1 (L/Sec) | 2.77 ± 0.63 | 2.95 ± 0.65 | 0.145 |
| FEV1/FVC Ratio (%) | 88.04 ± 6.85 | 91.32 ± 5.69 | 0.006 * |
| PEFR (L/Sec) | 6.94 ± 1.86 | 7.15 ± 1.98 | 0.542 |
| FEF-25% (L/Sec) | 6.58 ± 1.81 | 6.87 ± 1.84 | 0.394 |
| FEF-50% (L/Sec) | 4.29 ± 1.41 | 4.85 ± 1.36 | 0.034 * |
| FEF-75% (L/Sec) | 1.63 ± 0.92 | 1.95 ± 0.81 | 0.053 |
| Parameters | Diabetic Group (n = 43) | Control Group (n = 43) | p-Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| VC (L) | 2.56 ± 0.64 | 2.98 ± 0.57 | 0.002 * |
| FVC (L) | 2.87 ± 0.76 | 3.39 ± 0.75 | 0.002 * |
| FEV1 (L/Sec) | 2.46 ± 0.63 | 2.99 ± 0.65 | 0.001 * |
| FEV1/FVC Ratio (%) | 89.06 ± 7.11 | 91.00 ± 5.82 | 0.175 |
| PEFR (L/Sec) | 6.16 ± 2.17 | 7.20 ± 2.01 | 0.024 * |
| FEF-25% (L/Sec) | 5.86 ± 2.12 | 6.96 ± 1.99 | 0.015 * |
| FEF-50% (L/Sec) | 3.86 ± 1.30 | 4.92 ± 1.53 | 0.001 * |
| FEF-75% (L/Sec) | 1.47 ± 0.62 | 1.94 ± 0.79 | 0.003 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maan, H.B.; Meo, S.A.; Al Rouq, F.; Meo, I.M.U.; Gacuan, M.E.; Alkhalifah, J.M. Effect of Glycated Hemoglobin (HbA1c) and Duration of Disease on Lung Functions in Type 2 Diabetic Patients. Int. J. Environ. Res. Public Health 2021, 18, 6970. https://doi.org/10.3390/ijerph18136970
Maan HB, Meo SA, Al Rouq F, Meo IMU, Gacuan ME, Alkhalifah JM. Effect of Glycated Hemoglobin (HbA1c) and Duration of Disease on Lung Functions in Type 2 Diabetic Patients. International Journal of Environmental Research and Public Health. 2021; 18(13):6970. https://doi.org/10.3390/ijerph18136970
Chicago/Turabian StyleMaan, Hawra Bin, Sultan Ayoub Meo, Fawziah Al Rouq, Imran Muhammad Umar Meo, Milagros E. Gacuan, and Joud Mohammed Alkhalifah. 2021. "Effect of Glycated Hemoglobin (HbA1c) and Duration of Disease on Lung Functions in Type 2 Diabetic Patients" International Journal of Environmental Research and Public Health 18, no. 13: 6970. https://doi.org/10.3390/ijerph18136970