
Custom-Made Foot Orthoses as Non-Specific Chronic Low Back Pain and Pronated Foot Treatment

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
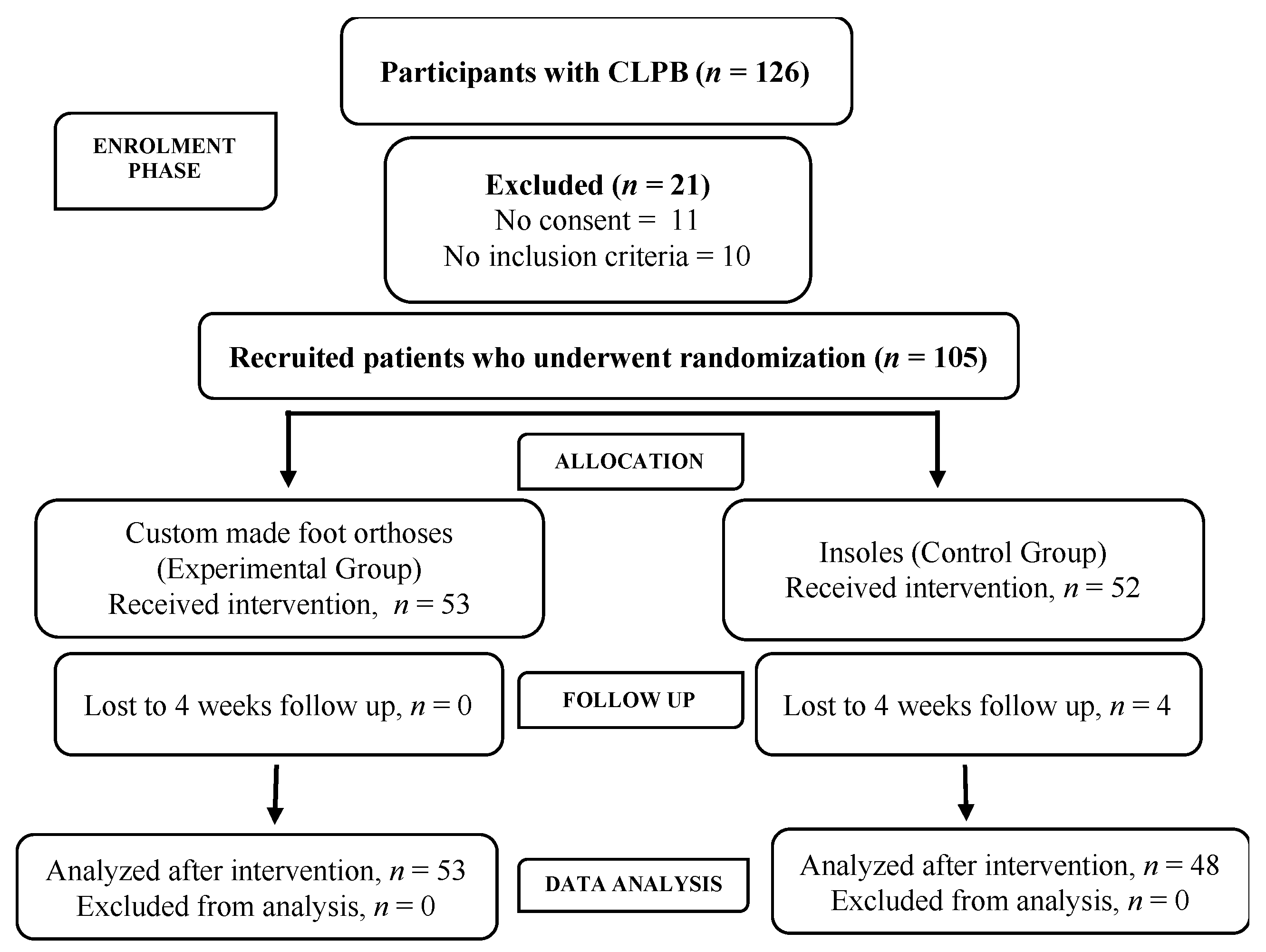
2.2. Randomisation
2.3. Recruitment
2.4. Inclusion Criteria
2.5. Exclusion Criteria
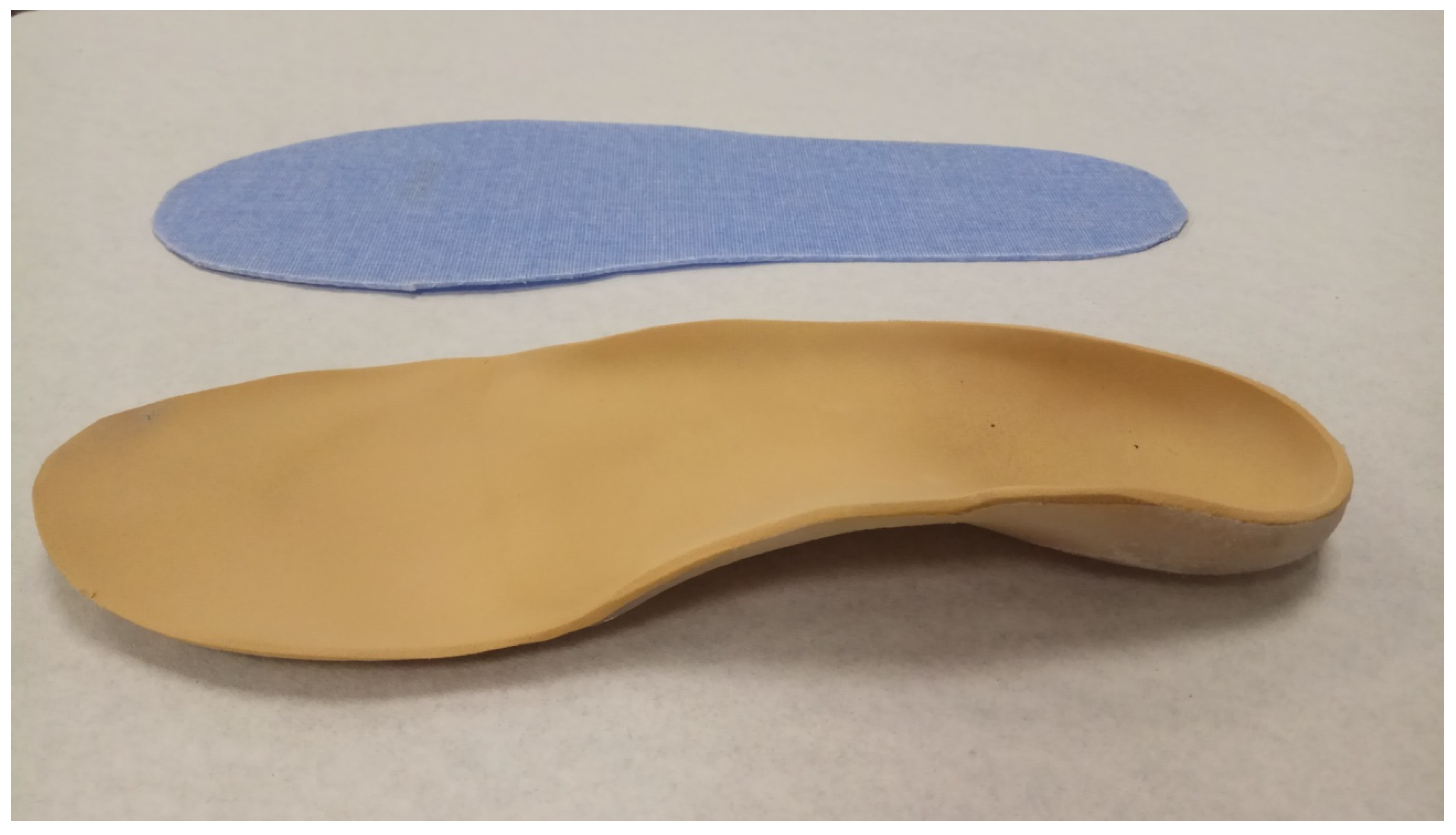
2.6. Procedure
Fabrication of Foot Orthoses
2.7. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Chuter, V.; Spink, M.; Searle, A. The effectiveness of shoe insoles for the prevention and treatment of low back pain: A systematic review and meta-analysis of randomised controlled trials. BMC Musculoskelet. Disord. 2014, 15, 140–148. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, C.B.; Maher, C.G.; Pinto, R.Z. Clinical practice guidelines for the management of non-specific low back pain in primary care: An updated overview. Eur. Spine J. 2018, 27, 2791–2803. [Google Scholar] [CrossRef] [Green Version]
- Farahpour, N.; Jafarnezhadgero, A.; Allard, P.; Majlesi, M. Muscle activity and kinetics of lower limbs during walking in pronated feet individuals with and without low back pain. J. Biomech. 2018, 39, 35–41. [Google Scholar] [CrossRef]
- Ferrari, R. Responsiveness of the short-form 36 and Oswestry disability questionnaire in chronic nonspecific low back and lower limb pain treated with customized foot orthotics. J. Manip. Physiol. Ther. B 2007, 30, 456–458. [Google Scholar] [CrossRef] [PubMed]
- Brantingham, J.W.; Lee Gilbert, J.; Sheik, J.; Globe, G. Sagittal plane blockage of the foot, ankle and hallux and foot alignment-prevalence and association with low back pain. J. Chiropr. Med. 2006, 5, 123–127. [Google Scholar] [CrossRef] [Green Version]
- Pinto, R.Z.; Souza, T.R.; Trede, R.G.; Kirkwood, R.N.; Figueiredo, E.M.; Fonseca, S.T. Bilateral and unilateral increases in calcaneal eversion affect pelvic alignment in standing position. Man Ther. 2008, 13, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Cambron, J.A.; Duarte, M.; Dexheimer, J.; Solecki, T. Shoe orthotics for the treatment of chronic low back pain: A randomized controlled pilot study. J. Manip. Physiol. Ther. 2011, 34, 254–260. [Google Scholar] [CrossRef]
- Farokmanesh, K.; Shirzadian, T.; Mahboubi, M.; Neyakan, M. Effect of foot hyperpronation on lumbar lordosis and thoracic kyphosis in standing position using 3-dimensional ultrasound-based motion analysis system. Glob. J. Health Sci. 2014, 6, 254–259. [Google Scholar] [CrossRef] [Green Version]
- O’Leary, C.; Cahill, C.; Robinson, A.; Barnes, M.; Hong, H. A systematic review: The effects of podiatrical deviations on nonspecific chronic low back pain. J. Back Musculoskelet. Rehabil. 2013, 26, 117–123. [Google Scholar] [CrossRef]
- Livingstone, L.A.; Mandingo, J.L. Bilateral rear foot asymmetry and anterior knee pain syndrome. J. Orthop. Deportes. Phys. Ther. 2003, 33, 48–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro-Méndez, A.; Munuera, P.V.; Albornoz-Cabello, M. The short-term effect of custom-made foot orthoses in subjects with excessive foot pronation and lower back pain: A randomized, double-blinded, clinical trial. Prosthet. Orthot. Int. 2013, 37, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Papúa, M.O.; Cambron, J. Foot orthotics for low back pain: The state of our understanding and recommendations for future research. Foot 2016, 26, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Rosner, A.; Conable, K.; Eldelmann, T. Influence of foot orthotics upon duration of effects of spinal manipulation in chronic back pain patients: A randomized clinical trial. J. Manip. Physiol. Ther. 2013, 37, 124–140. [Google Scholar] [CrossRef]
- Menendez, C.; Batalla, L.; Prieto, A.; Rodríguez, M.A.; Crespo, I.; Olmedillas, H. Medial tibial stress syndrome in novice and recreational runners: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 7457. [Google Scholar] [CrossRef]
- Pascual-Gutierrez, R.; Redmon, A.C.; Alcacer-Pitarch, B.; López Ros, P. Índice de postura del pie (IPP-6), versión de seis criterios. Man. Guía Usario. Podol. Clínica 2013, 14, 36–45. [Google Scholar]
- Ghasemi, M.; Koohpayehzadeh, J.; Kadkhodaei, H.; Ehsani, A. The effect of foot hyperpronation on spine alignment in standing position. Med. J. Islamic Repub. Iran 2016, 30, 466–472. [Google Scholar]
- Resende, R.A.; Kirkwood, R.N.; Deluzio, K.J.; Fonseca, T.S. Ipsilateral and contralateral foot pronation affect lower limb and trunk biomechanics of individuals with knee osteoarthritis during gait. Clin. Biomech. 2016, 7, 30–37. [Google Scholar] [CrossRef]
- Resende, A.; Deluzio, K.; Kirkwood, R.; Hassan, A.; Fonseca, S. Increased unilateral foot pronation affects lower limbs and pelvic biomechanics during walking. Gait Posture 2015, 41, 395–401. [Google Scholar] [CrossRef]
- Sahar, T.; Cohen, M.J.; Uval-Neeman, V.; Kandel, L.; Odebiyi, D.O.; Lev, I. Insoles for prevention and treatment of back pain: A systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine 2009, 34, 924–933. [Google Scholar] [CrossRef] [PubMed]
- Dananberg, H.J. Sagittal plane biomechanics. J. Am. Podiatr. Med. Assoc. 2000, 90, 47–50. [Google Scholar] [CrossRef]
- Khamis, S.; Yizhar, Z. Effect of feet hyperpronation on pelvic alignment in a standing position. Gait Posture 2007, 25, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. Declaración de la Iniciativa STROBE (Strengthening the Reporting of Observational studies in Epidemiology): Directrices para la comunicación de estudios observacionales. Gac. Sanit. 2008, 22, 144–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knutson, G.A. Anatomic and functional leg-length inequality: A review and recommendation for clinical decision-making. Part I, anatomic leg-length inequality: Prevalence, magnitude, effects and clinical significance. Chiropr. Osteopat. 2005, 20, 11–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcántara-Bumbiedro, S.; Flórez-García, M.T.; Echávarri-Pérez, C.; García-Pérez, F. Escala de incapacidad por dolor lumbar de Oswestry. Rehabilitación 2006, 40, 150–158. [Google Scholar] [CrossRef]
- Bijur, P.; Silver, W.; Gallagher, E. Reliability of the visual analog scale for measurement of acute pain. Acad. Emerg. Med. 2001, 8, 1153–1157. [Google Scholar] [CrossRef] [PubMed]
- Maughan, E.F.; Lewis, J.S. Outcome measures in chronic low back pain. Eur. Spine J. 2010, 19, 1484–1494. [Google Scholar] [CrossRef] [Green Version]
- Menz, H.; Alyssa, B.; Riskowski, J.; Howard, J.; Hannan, T. Foot posture, foot function and low back pain: The Framingham foot study. Rheumatology 2013, 53, 2275–2282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sannes, A.C.; Christensen, J.O.; Nielsen, N.B.; Gjerstad, J. The influence of age, gender and the FKBP5 genotype on subjective health complaints in the Norwegian working population. J. Psychosom. Res. 2020, 139, 110264. [Google Scholar] [CrossRef]
- Helen Reshman, K.; Mohanraj, K.G.; Vishnu Priya, V. Association between osteoporosis and gender, age, hypothyroidism, sex hormones among the middle-aged and old-age population-a survey-based analysis. Int. J. Res. Pharm. Sci. 2020, 11, 574–582. [Google Scholar] [CrossRef]
- Redmon, A.C.; Crane, Y.; Menz, H.B. Normative values for the Foot Posture Index. J. Foot Ankle Res. 2008, 31, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botte, R.R. An interpretation of the pronation syndrome and foot types of patients with low back pain. J. Am. Podiatry Assoc. 1981, 71, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Rothbart, B.A.; Estabrook, L. Excessive pronation: A major biomechanical determinant in the development of chondromalacia and pelvic lists. J. Manip. Physiol. Ther. 1988, 11, 373–379. [Google Scholar]
- Kelvin, J.; Molyneux, T.; Le Grande, M.; Castro, A.; Franz, K.; Fuss, M.D.; Azari, M. Association of Mild Leg Length Discrepancy and Degenerative Changes in the Hip Joint and Lumbar Spine. J. Manip. Physiol. Ther. 2017, 40, 301–309. [Google Scholar]
- Kim, S.C.; Yi, J.H.; Jung, S.W.; Seo, D.K. The effects of calcaneal posture on thoracolumbar alignment in a standing position. J. Phys. Ther. Sci. 2017, 2, 1993–1995. [Google Scholar] [CrossRef] [Green Version]
- Yazdani, S.; Dizji, E.; Alizadeh, F.; Hassanlouei, H. Effect of chronic idiopathic low back pain on the kinetic gait characteristics in different foot masks. J. Biomech. 2018, 79, 243–247. [Google Scholar] [CrossRef]
- Dodelin, D.; Tourny, C.; L’Hermette, M. The biomechanical effects of pronated foot function on gait. Scand. J. Med. Sci. Sport 2020, 30, 2167–2177. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Total Sample = 101 | Group | Group |
|---|---|---|---|
| Experimental n = 53 | Control n = 48 | ||
| Gender male | 48 (47.0%) | 26 (49.10%) | 22 (45.80%) |
| FPI BILATERAL PRONATED | 54 (53.50%) | 30 (56.60%) | 24 (50.0%) |
| LIMITED ANKLE ROM FLEXION | 46 (53.40%) | 32 (60.4%) | 22 (45.80%) |
| Age | 40.09 ± 15.22 | 40.64 ± 15.46 | 39.48 ± 15.09 |
| BMI | 24.01 ± 3.50 | 23.7 ± 3.00 | 24.36 ± 3.95 |
| FPI RIGHT FOOT | 6.19 ± 1.50 | 5.98 ± 1.62 | 6.42 ± 1.33 |
| FPI LEFT FOOT | 6.28 ± 1.63 | 6.57 ± 1.21 | 5.96 ± 1.97 |
| VAS/ODI | Group Time Groups | Mean SD | 95 IC | Median | Interquartile Range | p Value a | Size Effect |
|---|---|---|---|---|---|---|---|
| VAS | PRE | ||||||
| Control group | 6.50 ± 1.70 | 7.0–6.0 | 7.0 | 2 | |||
| Experimental group | 6.36 ± 1.70 | 6.8–5.9 | 6.0 | 2 | 0.505 | ||
| POST | |||||||
| Control Group | 6.54 ± 1.51 | 7.0–6.10 | 7.0 | 3 | |||
| Experimental Group | 3.02 ± 1.80 | 3.50–2.50 | 3.0 | 2 | 0.001 | 0.772 | |
| ODI | PRE | ||||||
| Control group | 18.90 ± 9.40 | 21.50–16.30 | 18.0 | 12 | |||
| Experimental group | 20.50 ± 12.50 | 23.90–17.0 | 16.0 | 23 | 0.877 | ||
| POST | |||||||
| Control Group | 21.40 ± 8.40 | 23.80–19.10 | 20.0 | 13 | |||
| Experimental Group | 7.21 ± 6.20 | 8.90–5.20 | 6.0 | 10 | 0.001 | 0.771 | |
| VAS | Control group | ||||||
| between-group differences | −0.04 ± 1.88 | 0.5–0.57 | 0.0 | 2 | 0.941 | ||
| Experimental Group | |||||||
| between-group differences | 3.34 ± 2.41 | 4.0–2.70 | 3.0 | 3 | 0.001 | 0.647 | |
| ODI | Control group | ||||||
| between-group differences | −2.51 ± 10.42 | 0.38–5.40 | 0.0 | 10 | 0.150 | ||
| Experimental Group | |||||||
| between-group differences | 13.24 ± 12.73 | 16.80–9.70 | 8.0 | 22 | 0.001 | 0.593 |
| Experimental Group | p Value b | Size Effect |
|---|---|---|
| VAS PRE/POST | 0.001 | 0.58 |
| ODI PRE/POST | 0.001 | 0.56 |
| Control Group | ||
| VAS PRE/POST | 0.999 | 0.09 |
| ODI PRE/POST | 0.136 | 0.14 |
| Gender | VAS/ODI | Time/Change | Experimental Group Mean SD | Control Group Mean SD | p Value a |
|---|---|---|---|---|---|
| MALE | VAS | PRE | 6.50 ± 1.77 | 6.52 ± 1.44 | 0.926 |
| POST | 2.81 ± 1.78 | 6.57 ± 1.40 | <0.001 | ||
| CHANGE (PRE/POST) | 3.69 ± 2.52 | −0.04 ± 1.79 | <0.001 | ||
| ODI | PRE | 21.81 ± 12.89 | 17.17 ± 9.56 | 0.330 | |
| POST | 7.38 ± 7.32 | 20.78 ± 7.83 | <0.001 | ||
| CHANGE (PRE/POST) | 14.42 ± 13.86 | −3.60 ± 10.87 | <0.001 | ||
| FAMALE | VAS | PRE | 6.22 ± 1.92 | 6.48 ± 1.60 | 0.438 |
| POST | 3.22 ± 1.84 | 6.52 ± 1.62 | <0.001 | ||
| CHANGE (PRE/POST) | 3.00 ± 2.30 | −0.03 ± 1.99 | <0.001 | ||
| ODI | PRE | 19.15 ± 12.23 | 20.28 ± 9.17 | 0.445 | |
| POST | 7.04 ± 5.03 | 21.93 ± 8.84 | <0.001 | ||
| CHANGE (PRE/POST) | 12.11 ± 11.69 | −1.65 ± 10.15 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro-Méndez, A.; Palomo-Toucedo, I.C.; Pabón-Carrasco, M.; Ramos-Ortega, J.; Díaz-Mancha, J.A.; Fernández-Seguín, L.M. Custom-Made Foot Orthoses as Non-Specific Chronic Low Back Pain and Pronated Foot Treatment. Int. J. Environ. Res. Public Health 2021, 18, 6816. https://doi.org/10.3390/ijerph18136816
Castro-Méndez A, Palomo-Toucedo IC, Pabón-Carrasco M, Ramos-Ortega J, Díaz-Mancha JA, Fernández-Seguín LM. Custom-Made Foot Orthoses as Non-Specific Chronic Low Back Pain and Pronated Foot Treatment. International Journal of Environmental Research and Public Health. 2021; 18(13):6816. https://doi.org/10.3390/ijerph18136816
Chicago/Turabian StyleCastro-Méndez, Aurora, Inmaculada Concepción Palomo-Toucedo, Manuel Pabón-Carrasco, Javier Ramos-Ortega, Juan Antonio Díaz-Mancha, and Lourdes María Fernández-Seguín. 2021. "Custom-Made Foot Orthoses as Non-Specific Chronic Low Back Pain and Pronated Foot Treatment" International Journal of Environmental Research and Public Health 18, no. 13: 6816. https://doi.org/10.3390/ijerph18136816