
The Moderating Role of Caregiving on Fear of COVID-19 and Post-Traumatic Stress Symptoms



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Analysis Strategy
3. Results
3.1. Sample Characteristics
3.2. Correlations between Study Variables
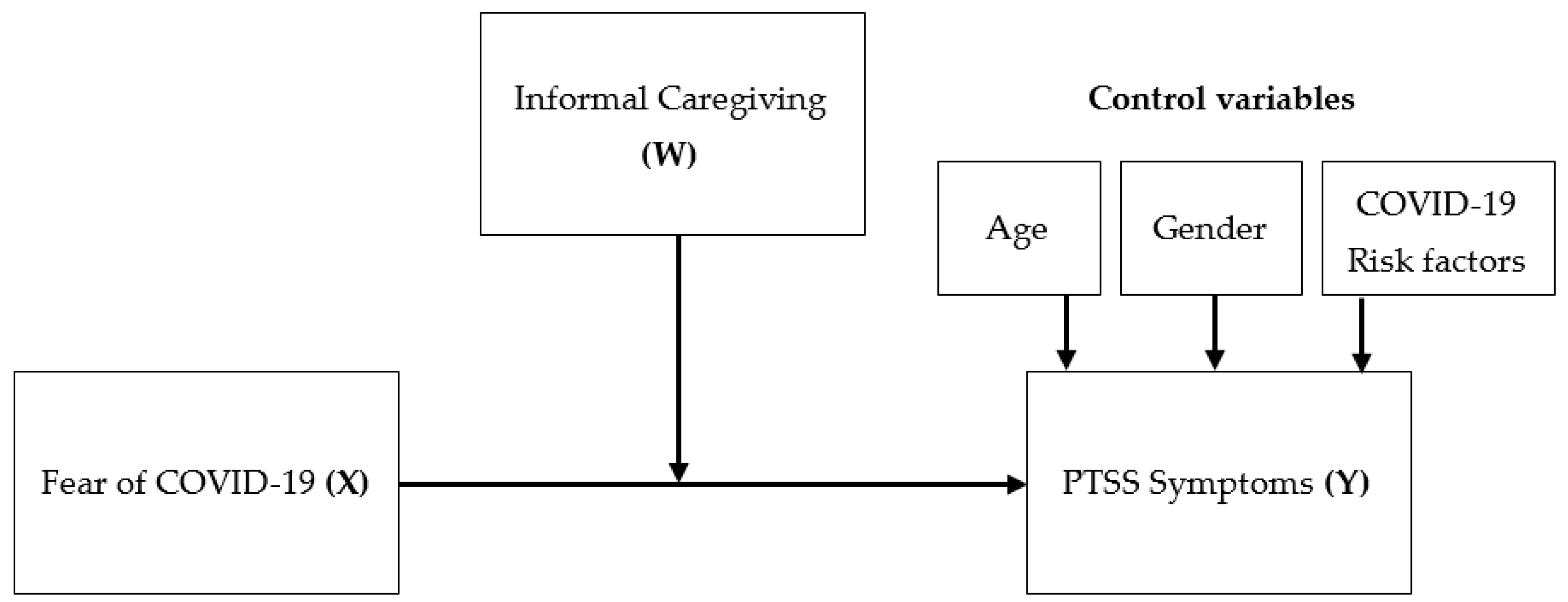
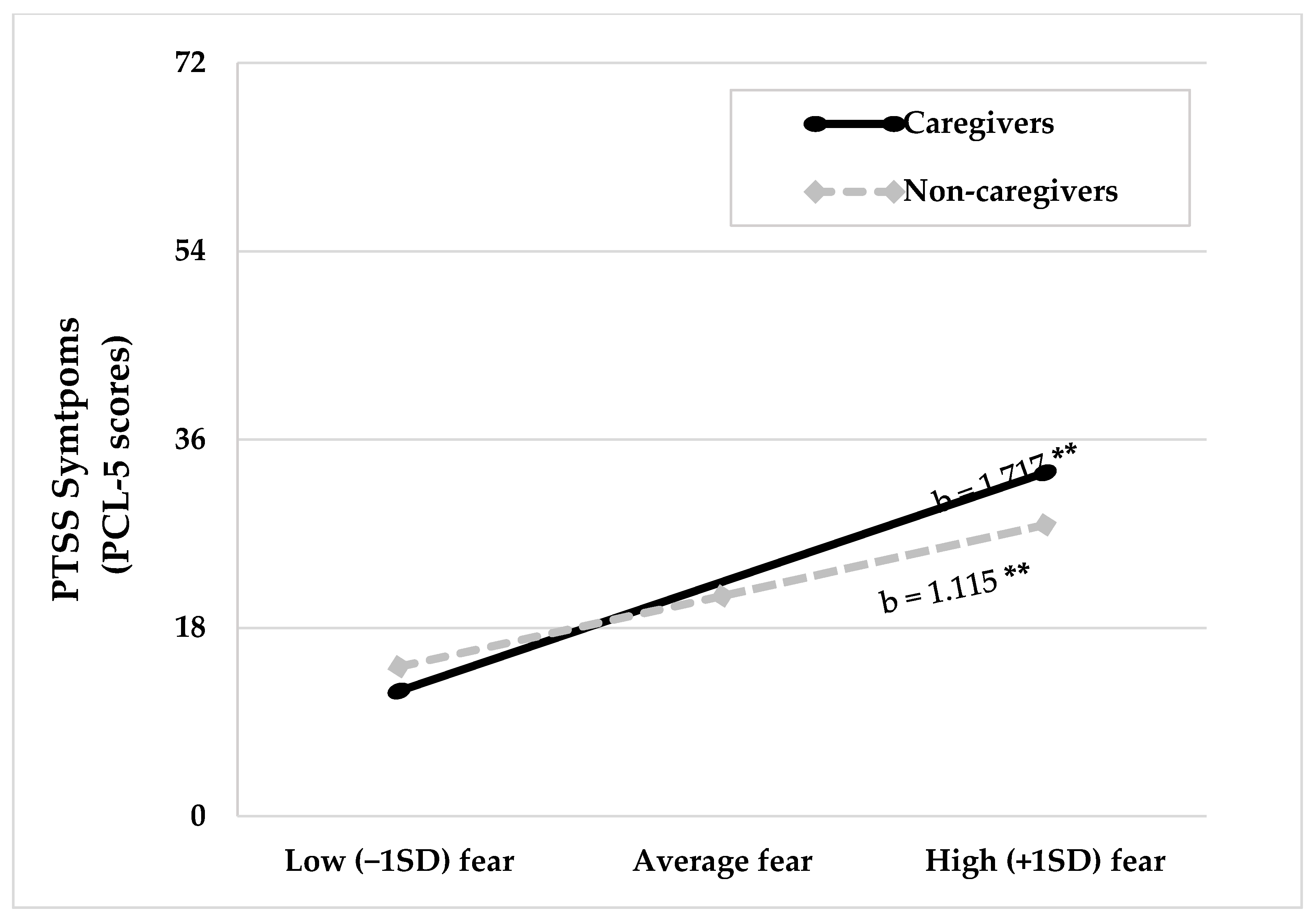
3.3. Moderation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhao, Y.-J.; Jin, Y.; Rao, W.-W.; Li, W.; Zhao, N.; Cheung, T.; Ng, C.H.; Wang, Y.-Y.; Zhang, Q.-E.; Xiang, Y.-T. The prevalence of psychiatric comorbidities during the SARS and COVID-19 epidemics: A systematic review and meta-analysis of observational studies. J. Affect. Disord. 2021, 287, 145–157. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef]
- Nikopoulou, V.A.; Holeva, V.; Parlapani, E.; Karamouzi, P.; Voitsidis, P.; Porfyri, G.-N.; Blekas, A.; Papigkioti, K.; Patsiala, S.; Diakogiannis, I. Mental health screening for COVID-19: A proposed cutoff score for the Greek version of the Fear of COVID-19 Scale (FCV-19S). Int. J. Ment. Health Addict. 2020, 1–14. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and initial validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, S. The Psychology of Pandemics: Preparing for the Next Global Outbreak of Infectious Disease; Cambridge Scholars Publishing: Newcastle upon Tyne, UK, 2019; ISBN 978-1-5275-4118-4. [Google Scholar]
- Pakpour, A.H.; Griffiths, M.D. The fear of COVID-19 and its role in preventive behaviors. J. Concurr. Disord. 2020, 2, 58–63. [Google Scholar]
- Schimmenti, A.; Starcevic, V.; Giardina, A.; Khazaal, Y.; Billieux, J. Multidimensional Assessment of COVID-19-Related Fears (MAC-RF): A theory-based instrument for the assessment of clinically relevant fears during pandemics. Front. Psychiatry 2020, 11, 748. [Google Scholar] [CrossRef] [PubMed]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R.D. Functional fear predicts public health compliance in the COVID-19 pandemic. Int. J. Ment. Health Addict. 2020, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Gruchoła, M.; Sławek-Czochra, M. “The culture of fear” of inhabitants of EU countries in their reaction to the COVID-19 pandemic—A study based on the reports of the Eurobarometer. Saf. Sci. 2021, 135, 105140. [Google Scholar] [CrossRef]
- Coco, G.L.; Gentile, A.; Bosnar, K.; Milovanović, I.; Bianco, A.; Drid, P.; Pišot, S. A cross-country examination on the fear of COVID-19 and the sense of loneliness during the first wave of COVID-19 outbreak. Int. J. Environ. Res. Public Health 2021, 18, 2586. [Google Scholar] [CrossRef]
- Bendau, A.; Petzold, M.B.; Pyrkosch, L.; Maricic, L.M.; Betzler, F.; Rogoll, J.; Große, J.; Ströhle, A.; Plag, J. Associations between COVID-19 related media consumption and symptoms of anxiety, depression and COVID-19 related fear in the general population in Germany. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Gunnell, D.; Appleby, L.; Arensman, E.; Hawton, K.; John, A.; Kapur, N.; Khan, M.; O’Connor, R.C.; Pirkis, J. COVID-19 Suicide Prevention Research Collaboration. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 468–471. [Google Scholar] [CrossRef]
- Koçak, O.; Koçak, Ö.; Younis, M. The psychological consequences of COVID-19 fear and the moderator effects of individuals’ underlying illness and witnessing infected friends and family. Int. J. Environ. Res. Public Health 2021, 18, 1836. [Google Scholar] [CrossRef]
- Mertens, G.; Gerritsen, L.; Duijndam, S.; Salemink, E.; Engelhard, I.M. Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. J. Anxiety Disord. 2020, 74, 102258. [Google Scholar] [CrossRef] [PubMed]
- Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. “Pandemic fear” and COVID-19: Mental health burden and strategies. Braz. J. Psychiatry 2020, 42, 232–235. [Google Scholar] [CrossRef] [Green Version]
- Maeng, L.Y.; Milad, M.R. Post-traumatic stress disorder: The relationship between the fear response and chronic stress. Chronic Stress 2017, 1, 2470547017713297. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, P.; Martinez, K.G. The role of stress and fear in the development of mental disorders. Psychiatr. Clin. N. Am. 2014, 37, 535–546. [Google Scholar] [CrossRef] [Green Version]
- Al Falasi, B.; Al Mazrouei, M.; Al Ali, M.; Al Dhamani, M.; Al Ali, A.; Al Kindi, M.; Dalkilinc, M.; Al Qubaisi, M.; Campos, L.; Al Tunaiji, H.; et al. Prevalence and determinants of immediate and long-term PTSD consequences of coronavirus-related (CoV-1 and CoV-2) pandemics among healthcare professionals: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 2182. [Google Scholar] [CrossRef] [PubMed]
- Salehi, M.; Amanat, M.; Mohammadi, M.; Salmanian, M.; Rezaei, N.; Saghazadeh, A.; Garakani, A. The prevalence of post-traumatic stress disorder related symptoms in Coronavirus outbreaks: A systematic-review and meta-analysis. J. Affect. Disord. 2021, 282, 527–538. [Google Scholar] [CrossRef]
- Yuan, K.; Gong, Y.-M.; Liu, L.; Sun, Y.-K.; Tian, S.-S.; Wang, Y.-J.; Zhong, Y.; Zhang, A.-Y.; Su, S.-Z.; Liu, X.-X.; et al. Prevalence of posttraumatic stress disorder after infectious disease pandemics in the twenty-first century, including COVID-19: A meta-analysis and systematic review. Mol. Psychiatry 2021, 1–17. [Google Scholar] [CrossRef]
- North, C.S.; Surís, A.M.; Pollio, D.E. A nosological exploration of PTSD and trauma in disaster mental health and implications for the COVID-19 pandemic. Behav. Sci. 2021, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Landry, C.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J. Development and initial validation of the COVID Stress Scales. J. Anxiety Disord. 2020, 72, 102232. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef] [Green Version]
- Devakumar, D.; Shannon, G.; Bhopal, S.S.; Abubakar, I. Racism and discrimination in COVID-19 responses. Lancet 2020, 395, 1194. [Google Scholar] [CrossRef]
- Taylor, S.; Landry, C.A.; Rachor, G.S.; Paluszek, M.M.; Asmundson, G.J. Fear and avoidance of healthcare workers: An important, under-recognized form of stigmatization during the COVID-19 pandemic. J. Anxiety Disord. 2020, 75, 102289. [Google Scholar] [CrossRef]
- Yuen, K.F.; Wang, X.; Ma, F.; Li, K.X. The psychological causes of panic buying following a health crisis. Int. J. Environ. Res. Public Health 2020, 17, 3513. [Google Scholar] [CrossRef]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. COVID stress syndrome: Concept, structure, and correlates. Depress. Anxiety 2020, 37, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Schimmenti, A.; Billieux, J.; Starcevic, V. The four horsemen of fear: An integrated model of understanding fear experiences during the COVID-19 pandemic. Clin. Neuropsychiatry J. Treat. Eval. 2020, 17, 41–45. [Google Scholar]
- Doshi, D.; Karunakar, P.; Sukhabogi, J.R.; Prasanna, J.S.; Mahajan, S.V. Assessing Coronavirus fear in Indian population using the fear of COVID-19 scale. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sit, S.M.-M.; Lam, T.-H.; Lai, A.Y.-K.; Wong, B.Y.-M.; Wang, M.-P.; Ho, S.-Y. Fear of COVID-19 and its associations with perceived personal and family benefits and harms in Hong Kong. Transl. Behav. Med. 2021, 11, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Solymosi, R.; Jackson, J.; Pósch, K.; Yesberg, J.A.; Bradford, B.; Kyprianides, A. Functional and dysfunctional fear of COVID-19: A classification scheme. Crime Sci. 2021, 10, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Segal, S.; Sharabany, R.; Maaravi, Y. Policymakers as safe havens: The relationship between adult attachment style, COVID-19 fear, and regulation compliance. Personal. Individ. Differ. 2021, 177, 110832. [Google Scholar] [CrossRef]
- Jørgensen, F.; Bor, A.; Petersen, M.B. Compliance without fear: Individual-level protective behaviour during the first wave of the COVID-19 pandemic. Br. J. Health Psychol. 2021, 26, 679–696. [Google Scholar] [CrossRef]
- Ng, K.Y.Y.; Zhou, S.; Tan, S.H.; Ishak, N.D.B.; Goh, Z.Z.S.; Chua, Z.Y.; Chia, J.M.X.; Chew, E.L.; Shwe, T.; Mok, J.K.Y.; et al. Understanding the psychological impact of COVID-19 pandemic on patients with cancer, their caregivers, and health care workers in Singapore. JCO Glob. Oncol. 2020, 6, 1494–1509. [Google Scholar] [CrossRef]
- Park, S.S. Caregivers’ mental health and somatic symptoms during COVID-19. J. Gerontol. Ser. B 2021, 76, e235–e240. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.; Herrera-Peco, I.; Jurado, M.; Oropesa, N.; Linares, J.G. Predictors of threat from COVID-19: A cross-sectional study in the Spanish population. J. Clin. Med. 2021, 10, 692. [Google Scholar] [CrossRef]
- Heger, D.; Korfhage, T. Care choices in Europe: To each according to his or her needs? Inq. J. Health Care Organ. Provis. Financ. 2018, 55, 46958018780848. [Google Scholar] [CrossRef] [Green Version]
- Budnick, A.; Hering, C.; Eggert, S.; Teubner, C.; Suhr, R.; Kuhlmey, A.; Gellert, P. Informal caregivers during the COVID-19 pandemic perceive additional burden: Findings from an ad-hoc survey in Germany. BMC Health Serv. Res. 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Giebel, C.; Lord, K.; Cooper, C.; Shenton, J.; Cannon, J.; Pulford, D.; Shaw, L.; Gaughan, A.; Tetlow, H.; Butchard, S.; et al. A UK survey of COVID-19 related social support closures and their effects on older people, people with dementia, and carers. Int. J. Geriatr. Psychiatry 2021, 36, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Savla, J.; Roberto, K.A.; Blieszner, R.; McCann, B.R.; Hoyt, E.; Knight, A.L. Dementia caregiving during the “Stay-at-Home” phase of COVID-19 pandemic. J. Gerontol. Ser. B 2021, 76, e241–e245. [Google Scholar] [CrossRef] [PubMed]
- Schorren, N. The Impact of COVID-19 on Wellbeing, Depression, and Physical Activity of Informal Caregivers and Non-Caregivers during Isolation. Available online: http://essay.utwente.nl/82470/ (accessed on 28 April 2021).
- Cohen, S.A.; Kunicki, Z.J.; Drohan, M.M.; Greaney, M.L. Exploring changes in caregiver burden and caregiving intensity due to COVID-19. Gerontol. Geriatr. Med. 2021, 7, 2333721421999279. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, R.; Simmons, C.; Schmidt, A.E.; Steiber, N. Care in times of COVID-19: The impact of the pandemic on informal caregiving in Austria. Eur. J. Ageing 2021, 1–11. [Google Scholar] [CrossRef]
- Kent, E.E.; Ornstein, K.A.; Dionne-Odom, J.N. The family caregiving crisis meets an actual pandemic. J. Pain Symptom Manag. 2020, 60, e66–e69. [Google Scholar] [CrossRef] [PubMed]
- Koh, Z.Y.; Law, F.; Chew, J.; Ali, N.; Lim, W.S. Impact of Coronavirus disease on persons with dementia and their caregivers: An audit study. Ann. Geriatr. Med. Res. 2020, 24, 316–320. [Google Scholar] [CrossRef]
- Cheng, S.-T.; Zhang, F. A comprehensive meta-review of systematic reviews and meta-analyses on nonpharmacological interventions for informal dementia caregivers. BMC Geriatr. 2020, 20, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Prime, H.; Wade, M.; Browne, D.T. Risk and resilience in family well-being during the COVID-19 pandemic. Am. Psychol. 2020, 75, 631–643. [Google Scholar] [CrossRef]
- Wade, M.; Prime, H.; Johnson, D.; May, S.S.; Jenkins, J.M.; Browne, D.T. The disparate impact of COVID-19 on the mental health of female and male caregivers. Soc. Sci. Med. 2021, 275, 113801. [Google Scholar] [CrossRef]
- Glaziou, P. Sampsize Home Page. Available online: Sampsize.sourceforge.net (accessed on 15 March 2021).
- Eurofound European Quality of Life Survey 2016: Quality of Life, Quality of Public Services, and Quality of Society; Publications Office of the European Union: Luxembourg, 2016.
- Espinoza, J.; Crown, K.; Kulkarni, O. A guide to chatbots for COVID-19 screening at pediatric health care facilities. JMIR Public Health Surveill. 2020, 6, e18808. [Google Scholar] [CrossRef]
- Laranjo, L.; Dunn, A.G.; Tong, H.L.; Kocaballi, A.B.; Chen, J.; Bashir, R.; Surian, D.; Gallego, B.; Magrabi, F.; Lau, A.Y.S.; et al. Conversational agents in healthcare: A systematic review. J. Am. Med. Inform. Assoc. 2018, 25, 1248–1258. [Google Scholar] [CrossRef] [Green Version]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The posttraumatic stress disorder checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Forte, G.; Favieri, F.; Tambelli, R.; Casagrande, M. COVID-19 pandemic in the Italian population: Validation of a post-traumatic stress disorder questionnaire and prevalence of PTSD symptomatology. Int. J. Environ. Res. Public Health 2020, 17, 4151. [Google Scholar] [CrossRef] [PubMed]
- Tsur, N.; Abu-Raiya, H. COVID-19-related fear and stress among individuals who experienced child abuse: The mediating effect of complex posttraumatic stress disorder. Child Abuse Negl. 2020, 110, 104694. [Google Scholar] [CrossRef]
- Bridgland, V.M.E.; Moeck, E.K.; Green, D.M.; Swain, T.L.; Nayda, D.M.; Matson, L.A.; Hutchison, N.P.; Takarangi, M.K.T. Why the COVID-19 pandemic is a traumatic stressor. PLoS ONE 2021, 16, e0240146. [Google Scholar] [CrossRef]
- Moshier, S.J.; Lee, D.J.; Bovin, M.J.; Gauthier, G.; Zax, A.; Rosen, R.C.; Keane, T.M.; Marx, B.P. An empirical crosswalk for the PTSD checklist: Translating DSM-IV to DSM-5 using a veteran sample. J. Trauma. Stress 2019, 32, 799–805. [Google Scholar] [CrossRef]
- Martínez-Lorca, M.; Martínez-Lorca, A.; Criado-Álvarez, J.J.; Armesilla, M.D.C.; Latorre, J.M. The fear of COVID-19 scale: Validation in Spanish university students. Psychiatry Res. 2020, 293, 113350. [Google Scholar] [CrossRef] [PubMed]
- Pakenham, K.I.; Landi, G.; Boccolini, G.; Furlani, A.; Grandi, S.; Tossani, E. The moderating roles of psychological flexibility and inflexibility on the mental health impacts of COVID-19 pandemic and lockdown in Italy. J. Context. Behav. Sci. 2020, 17, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Publications: New York, NY, USA, 2017; ISBN 978-1-4625-3465-4. [Google Scholar]
- Aiken, L.S.; West, S.G.; Reno, R.R. Multiple Regression: Testing and Interpreting Interactions; Sage: Thousand Oaks, CA, USA, 1991. [Google Scholar]
- Mistry, S.K.; Ali, A.R.M.M.; Akther, F.; Yadav, U.N.; Harris, M.F. Exploring fear of COVID-19 and its correlates among older adults in Bangladesh. Glob. Health 2021, 17, 1–9. [Google Scholar] [CrossRef]
- Bakioğlu, F.; Korkmaz, O.; Ercan, H. Fear of COVID-19 and positivity: Mediating role of intolerance of uncertainty, depression, anxiety, and stress. Int. J. Ment. Health Addict. 2020, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ausín, B.; González-Sanguino, C.; Castellanos, M.Á.; Muñoz, M. Gender-related differences in the psychological impact of confinement as a consequence of COVID-19 in Spain. J. Gend. Stud. 2021, 30, 29–38. [Google Scholar] [CrossRef]
- Özdin, S.; Bayrak Özdin, Ş. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef]
- Hicks, T.A.; Bountress, K.E.; Resnick, H.S.; Ruggiero, K.J.; Amstadter, A.B. Caregiver support buffers posttraumatic stress disorder symptoms following a natural disaster in relation to binge drinking. Psychol. Trauma Theory Res. Pract. Policy 2020. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Bonsaksen, T.; Heir, T.; Schou-Bredal, I.; Ekeberg, Ø.; Skogstad, L.; Grimholt, T.K. Post-Traumatic Stress disorder and associated factors during the early stage of the COVID-19 pandemic in Norway. Int. J. Environ. Res. Public Health 2020, 17, 9210. [Google Scholar] [CrossRef] [PubMed]
- Fairchild, A.J.; McQuillin, S.D. Evaluating mediation and moderation effects in school psychology: A presentation of methods and review of current practice. J. Sch. Psychol. 2010, 48, 53–84. [Google Scholar] [CrossRef] [Green Version]
- Altieri, M.; Santangelo, G. The psychological impact of COVID-19 pandemic and lockdown on caregivers of people with dementia. Am. J. Geriatr. Psychiatry 2021, 29, 27–34. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total (N = 503) | Range |
|---|---|---|
| Gender, % (n) | ||
| Male | 17.50 (88) | |
| Female | 82.50 (415) | |
| Age, M ± SD | 35.54 ± 12.79 | 18–75 |
| Educational level, % (n) | ||
| Elementary/primary | 2.40 (12) | |
| Secondary/technical | 40.60 (204) | |
| University or higher | 57.10 (287) | |
| Informal caregiving, % (n) | 16.90 (85) | |
| Fear of COVID-19 (FCVS-19), M ± SD | 18.73 ± 6.08 | 7–35 |
| Post-traumatic stress symptoms (PCL-5), M ± SD | 21.52 ± 12.78 | 0–72 |
| COVID-19 risk factors, M ± SD † | 2.31 ± 0.86 | 0–4 |
| a Potential/direct occupational exposure to COVID-19, % (n) | 13.70 (69) | |
| b Friends/relatives infected with COVID-19, % (n) | 83.50 (420) | |
| c Reported COVID-19 symptoms/diagnosis, % (n) | 45.70 (230) | |
| d Receiving psychiatric/psychological treatment, % (n) | 15.50 (78) |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| 1. Fear of COVID-19 | (0.87) | ||||||
| 2. PTSS symptoms | 0.587 ** | (0.92) | |||||
| 3. Informal Caregiving (ref. no) a | 0.162 ** | 0.175 ** | -- | ||||
| 4. Gender (ref. male) b | −0.247 ** | −0.117 ** | −0.068 | -- | |||
| 5. Age | 0.081 | −0.096 * | 0.005 | 0.012 | -- | ||
| 6. Educational level (ref. elementary) c | 0.016 | 0.041 | 0.005 | −0.078 | 0.094 * | -- | |
| 7. COVID-19 risk factors | 0.131 ** | 0.216 ** | 0.122 ** | 0.023 | −0.165 ** | −0.091 * | -- |
| Variables | B (SE) | 95% CI | p |
|---|---|---|---|
| Fear of COVID-19 | 1.115 (0.085) | [0.949, 1.282] | 0.001 ** |
| Informal caregiving | 1.341 (1.263) | [−1.141, 3.824] | 0.289 |
| Fear x Caregiving | 0.602 (0.200) | [0.209, 0.995] | 0.003 ** |
| Covariates | |||
| Gender (ref. = male) | 0.936 (1.215) | [−1.452, 3.323] | 0.442 |
| Age | −0.127 (0.036) | [−0.197, −0.057] | 0.001 ** |
| COVID-19 risk factors | 1.714 (0.538) | [0.658, 2.770] | 0.002 ** |
| Constant | 21.459 (1.969) | [17.590, 25.328] | 0.001 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carballo, J.L.; Coloma-Carmona, A.; Arteseros-Bañón, S.; Pérez-Jover, V. The Moderating Role of Caregiving on Fear of COVID-19 and Post-Traumatic Stress Symptoms. Int. J. Environ. Res. Public Health 2021, 18, 6125. https://doi.org/10.3390/ijerph18116125
Carballo JL, Coloma-Carmona A, Arteseros-Bañón S, Pérez-Jover V. The Moderating Role of Caregiving on Fear of COVID-19 and Post-Traumatic Stress Symptoms. International Journal of Environmental Research and Public Health. 2021; 18(11):6125. https://doi.org/10.3390/ijerph18116125
Chicago/Turabian StyleCarballo, José Luis, Ainhoa Coloma-Carmona, Sara Arteseros-Bañón, and Virtudes Pérez-Jover. 2021. "The Moderating Role of Caregiving on Fear of COVID-19 and Post-Traumatic Stress Symptoms" International Journal of Environmental Research and Public Health 18, no. 11: 6125. https://doi.org/10.3390/ijerph18116125