
Favorable Lip and Oral Cancer Mortality-to-Incidence Ratios in Countries with High Human Development Index and Expenditures on Health

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Epidemiology of Lip and Oral Cancer According to the Regions
3.2. Epidemiology and Parameters of the Development and Health Expenditure of Lip and Oral Cancer in the Selected Countries
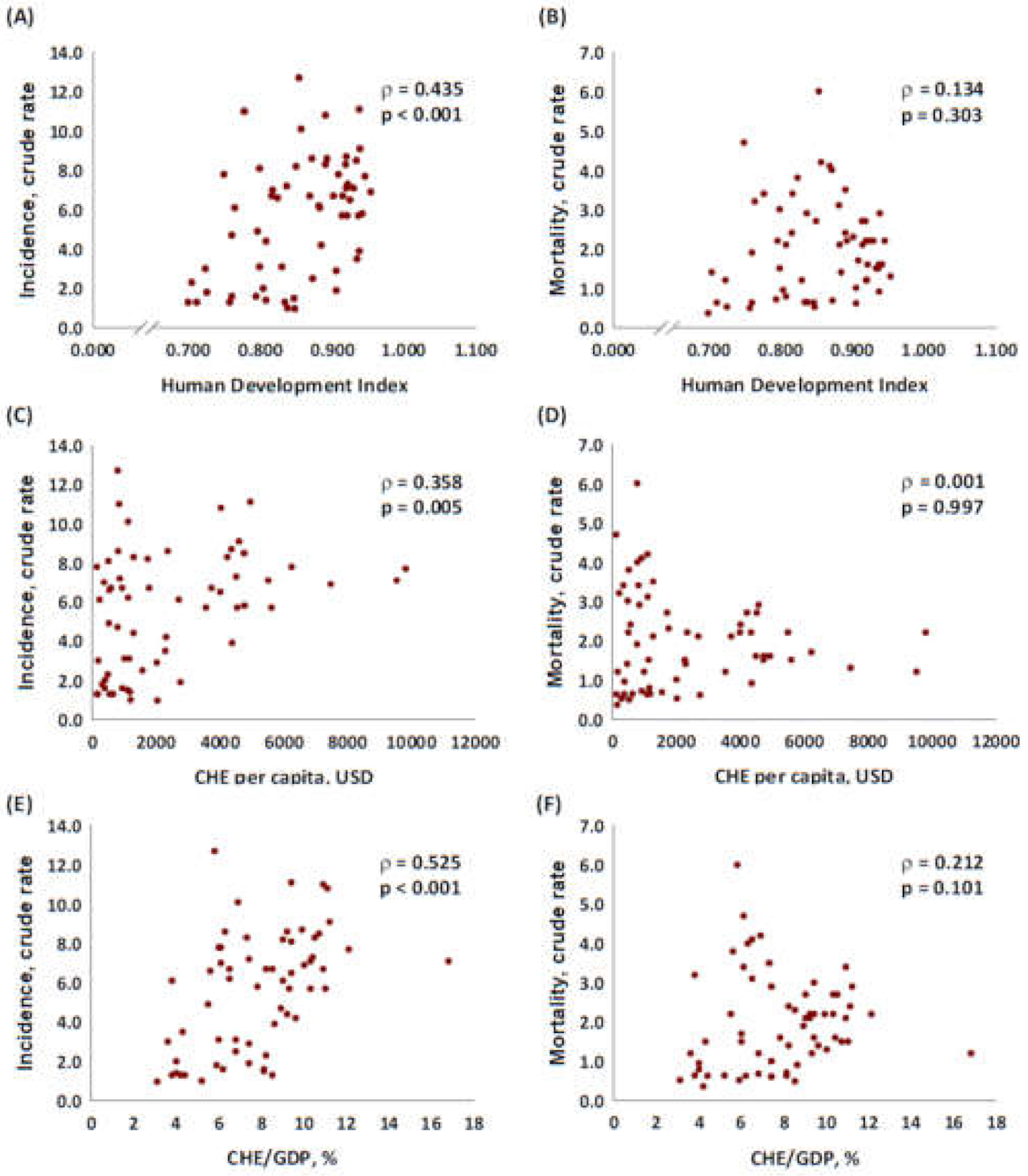
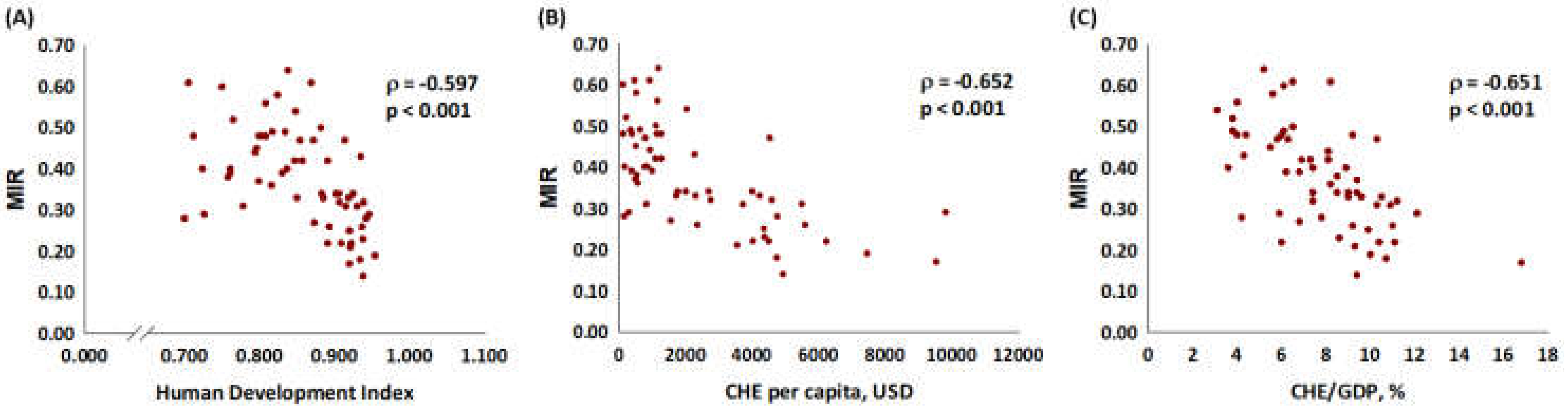
3.3. Association between MIR and Parameters of the Development and Health Expenditures in the Selected Countries
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. Cancer Rehabil. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Ghantous, Y.; Abu Elnaaj, I. Global incidence and risk factors of oral cancer. Harefuah 2017, 156, 645–649. [Google Scholar] [PubMed]
- Dhanuthai, K.; Rojanawatsirivej, S.; Thosaporn, W.; Kintarak, S.; Subarnbhesaj, A.; Darling, M.; Kryshtalskyj, E.; Chiang, C.-P.; Shin, H.-I.; Choi, S.-Y.; et al. Oral cancer: A multicenter study. Med. Oral Patol. Oral Cir. Bucal 2018, 23, e23–e29. [Google Scholar] [CrossRef] [PubMed]
- LeHew, C.W.; Weatherspoon, D.J.; Peterson, C.E.; Goben, A.; Reitmajer, K.; Sroussi, H.; Kaste, L.M. The Health System and Policy Implications of Changing Epidemiology for Oral Cavity and Oropharyngeal Cancers in the United States From 1995 to 2016. Epidemiol. Rev. 2017, 39, 132–147. [Google Scholar] [CrossRef] [Green Version]
- Kumar, M.; Nanavati, R.; Modi, T.G.; Dobariya, C. Oral cancer: Etiology and risk factors: A review. J. Cancer Res. Ther. 2016, 12, 458–463. [Google Scholar] [CrossRef]
- Yanik, E.L.; Katki, H.A.; Silverberg, M.J.; Manos, M.M.; Engels, E.A.; Chaturvedi, A.K. Leukoplakia, Oral Cavity Cancer Risk, and Cancer Survival in the U.S. Elderly. Cancer Prev. Res. (Phila) 2015, 8, 857–863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jitender, S.; Warnakulasuriya, S. Screening for oral cancer. J. Exp. Ther. Oncol. 2016, 11, 303–307. [Google Scholar]
- Kravietz, A.; Angara, P.; Le, M.; Sargi, Z. Disparities in Screening for Head and Neck Cancer: Evidence from the NHANES, 2011-2014. Otolaryngol. Head Neck Surg. 2018, 159, 683–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaidar-Person, O.; Gil, Z.; Billan, S. Precision medicine in head and neck cancer. Drug Resist. Updat. 2018, 40, 13–16. [Google Scholar] [CrossRef]
- Cheraghlou, S.; Schettino, A.; Zogg, C.K.; Jodson, B.L. Changing prognosis of oral cancer: An analysis of survival and treatment between 1973 and 2014. Laryngoscope 2018, 128, 2762–2769. [Google Scholar] [CrossRef]
- Shah, J.P.; Gil, Z. Current concepts in management of oral cancer—Surgery. Oral Oncol. 2009, 45, 394–401. [Google Scholar] [CrossRef] [Green Version]
- D’Cruz, A.K.; Vaish, R.; Dhar, H. Oral cancers: Current status. Oral Oncol. 2018, 87, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.J.; Choi, J.S.; Swanson, M.S.; Kokot, N.C.; Brown, T.N.; Yan, G.; Sinha, U.K. Association of Race/Ethnicity, Stage, and Survival in Oral Cavity Squamous Cell Carcinoma: A SEER Study. OTO Open 2019, 3, 2473974X19891126. [Google Scholar] [CrossRef]
- Farhood, Z.; Simpson, M.; Ward, G.M.; Walker, R.J.; Osazuwa-Peters, N. Does anatomic subsite influence oral cavity cancer mortality? A SEER database analysis. Laryngoscope 2019, 129, 1400–1406. [Google Scholar] [CrossRef] [PubMed]
- Gaubatz, M.E.; Bukatko, A.R.; Simpson, M.C.; Polednik, K.M.; Boakye, E.A.; Varvares, M.A.; Osazuwa-Peters, N. Racial and socioeconomic disparities associated with 90-day mortality among patients with head and neck cancer in the United States. Oral Oncol. 2019, 89, 95–101. [Google Scholar] [CrossRef]
- Agarwal, P.; Agrawal, R.R.; Jones, E.A.; Devaiah, A.K. Social determinants of health and oral cavity cancer treatment and survival: A competing risk analysis. Laryngoscope 2019. [Google Scholar] [CrossRef]
- Inverso, G.; Mahal, B.A.; Aizer, A.A.; Donoff, R.B.; Chuang, S.-K. Health Insurance Affects Head and Neck Cancer Treatment Patterns and Outcomes. J. Oral Maxillofac. Surg. 2016, 74, 1241–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghantous, Y.; Yaffi, V.; Abu-Elnaaj, I. Oral cavity cancer: Epidemiology and early diagnosis. Refuat Hapeh Vehashinayim (1993) 2015, 32, 55–63, 71. [Google Scholar]
- Akinkugbe, A.A.; Garcia, D.T.; Brickhouse, T.H.; Mosavel, M. Lifestyle risk factor related disparities in oral cancer examination in the U.S: A population-based cross-sectional study. BMC Public Health 2020, 20, 153. [Google Scholar] [CrossRef]
- Choi, E.; Lee, S.; Nhung, B.C.; Suh, M.; Park, B.; Jun, J.K.; Choi, K.S. Cancer mortality-to-incidence ratio as an indicator of cancer management outcomes in Organization for Economic Cooperation and Development countries. Epidemiol. Health 2017, 39, e2017006. [Google Scholar] [CrossRef]
- Eberth, J.M.; Zahnd, W.E.; Adams, S.A.; Friedman, D.B.; Wheeler, S.B.; Hébert, J.R. Mortality-to-incidence ratios by US Congressional District: Implications for epidemiologic, dissemination and implementation research, and public health policy. Prev. Med. 2019, 129, 105849. [Google Scholar] [CrossRef] [PubMed]
- Sunkara, V.; Hébert, J.R. The colorectal cancer mortality-to-incidence ratio as an indicator of global cancer screening and care. Cancer 2015, 121, 1563–1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.L.; Wang, S.-C.; Ho, C.-J.; Kao, Y.-L.; Hsieh, T.-Y.; Chen, W.-J.; Chen, C.-J.; Wu, P.-R.; Ko, J.-L.; Lee, H.; et al. Prostate Cancer Mortality-To-Incidence Ratios Are Associated with Cancer Care Disparities in 35 Countries. Sci. Rep. 2017, 7, 40003. [Google Scholar] [CrossRef] [Green Version]
- Sung, W.W.; Wang, S.-C.; Hsieh, T.-Y.; Ho, C.-J.; Huang, C.-Y.; Kao, Y.-L.; Chen, W.-J.; Chen, S.-L. Favorable mortality-to-incidence ratios of kidney Cancer are associated with advanced health care systems. BMC Cancer 2018, 18, 792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.C.; Sung, W.-W.; Kao, Y.-L.; Hsieh, T.-Y.; Chen, W.-J.; Chen, S.-L.; Chang, H.-R. The gender difference and mortality-to-incidence ratio relate to health care disparities in bladder cancer: National estimates from 33 countries. Sci. Rep. 2017, 7, 4360. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.Y.; Au, K.-K.; Chen, S.-L.; Wang, S.-C.; Liao, C.-Y.; Hsu, H.-H.; Sung, W.-W.; Wang, Y.-C. Unfavorable Mortality-To-Incidence Ratio of Lung Cancer Is Associated with Health Care Disparity. Int. J. Environ. Res. Public Health 2018, 15, 2889. [Google Scholar] [CrossRef] [Green Version]
- International Agency for Research on Cancer. Personal habits and indoor combustions. Volume 100 E. A review of human carcinogens. IARC Monogr. Eval. Carcinog. Risks Hum. 2012, 100 Pt E, 1–538. [Google Scholar]
- Song, H.; Wan, Y.; Xu, Y.Y. Betel quid chewing without tobacco: A meta-analysis of carcinogenic and precarcinogenic effects. Asia Pac. J. Public Health 2015, 27, Np47–Np57. [Google Scholar] [CrossRef] [PubMed]
- Guha, N.; Warnakulasuriya, S.; Vlaanderen, J.; Straif, K. Betel quid chewing and the risk of oral and oropharyngeal cancers: A meta-analysis with implications for cancer control. Int. J. Cancer 2014, 135, 1433–1443. [Google Scholar] [CrossRef]
- Fidler, M.M.; Bray, F.; Soerjomataram, I. The global cancer burden and human development: A review. Scand. J. Public Health 2018, 46, 27–36. [Google Scholar] [CrossRef] [Green Version]
- Mehrotra, R.; Gupta, D.K. Exciting new advances in oral cancer diagnosis: Avenues to early detection. Head Neck Oncol. 2011, 3, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina, M.A.; Cheung, M.C.; Perez, E.A.; Byrne, M.M.; Franceschi, D.; Moffat, F.L.; Livingstone, A.S.; Goodwin, W.J.; Gutierrez, J.C.; Koniaris, L.G. African American and poor patients have a dramatically worse prognosis for head and neck cancer: An examination of 20,915 patients. Cancer 2008, 113, 2797–2806. [Google Scholar] [CrossRef]
- Asadzadeh Vostakolaei, F.; Karim-Kos, H.E.; Janssen-Heijnen, M.L.G.; Visser, O.; Verbeek, A.L.M.; Kiemeney, L. The validity of the mortality to incidence ratio as a proxy for site-specific cancer survival. Eur. J. Public Health 2011, 21, 573–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amit, M.; Yen, T.-C.; Liao, C.-T.; Chaturvedi, P.; Agarwal, J.P.; Kowalski, L.P.; Ebrahimi, A.; Clark, J.R.; Kreppel, M.; Zöller, J.; et al. Improvement in survival of patients with oral cavity squamous cell carcinoma: An international collaborative study. Cancer 2013, 119, 4242–4248. [Google Scholar] [CrossRef]
- Li, C.C.; Shen, Z.; Bavarian, R.; Yang, F.; Bhattacharya, A. Oral Cancer: Genetics and the Role of Precision Medicine. Dent. Clin. North. Am. 2018, 62, 29–46. [Google Scholar] [CrossRef]
- Ellis, L.; Belot, A.; Rachet, B.; Coleman, M.P. The Mortality-to-Incidence Ratio Is Not a Valid Proxy for Cancer Survival. J. Glob. Oncol. 2019, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| New Cases | Deaths | MIR | |||||
|---|---|---|---|---|---|---|---|
| Region | Number | CR | ASR | Number | CR | ASR | |
| Africa | 13,324 | 1.0 | 1.7 | 9066 | 0.7 | 1.2 | 0.71 |
| Asia | 220,810 | 4.9 | 4.2 | 124,900 | 2.8 | 2.4 | 0.57 |
| Europe | 57,737 | 8.0 | 4.3 | 21,834 | 3.0 | 1.6 | 0.38 |
| Latin America and the Caribbean | 18,525 | 2.9 | 2.6 | 7050 | 1.1 | 1.0 | 0.38 |
| North America | 25,354 | 7.1 | 4.2 | 4424 | 1.2 | 0.7 | 0.17 |
| Oceania | 4163 | 10.2 | 7.5 | 895 | 2.2 | 1.5 | 0.22 |
| Country | HDI | CHE | Incidence | Mortality | MIR | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Per Capita | % of GDP | Number | CR | ASR | Number | CR | ASR | |||
| Argentina | 0.830 | 998 | 6.8 | 1357 | 3.1 | 2.5 | 512 | 1.2 | 0.9 | 0.39 |
| Australia | 0.938 | 4934 | 9.4 | 2682 | 11.1 | 6.9 | 378 | 1.6 | 0.9 | 0.14 |
| Austria | 0.914 | 4536 | 10.3 | 488 | 5.7 | 3.0 | 232 | 2.7 | 1.4 | 0.47 |
| Bahrain | 0.838 | 1190 | 5.2 | 16 | 1.0 | 1.5 | 10 | 0.6 | 1.0 | 0.64 |
| Belarus | 0.817 | 352 | 6.1 | 653 | 7.0 | 4.1 | 316 | 3.4 | 2.0 | 0.49 |
| Belgium | 0.919 | 4228 | 10.5 | 923 | 8.3 | 4.7 | 305 | 2.7 | 1.4 | 0.33 |
| Brazil | 0.761 | 780 | 8.9 | 9902 | 4.7 | 4.0 | 3965 | 1.9 | 1.6 | 0.40 |
| Bulgaria | 0.816 | 572 | 8.2 | 459 | 6.7 | 3.4 | 164 | 2.4 | 1.2 | 0.36 |
| Canada | 0.922 | 4508 | 10.4 | 2633 | 7.3 | 3.9 | 594 | 1.6 | 0.8 | 0.22 |
| Chile | 0.847 | 1102 | 8.1 | 275 | 1.5 | 1.1 | 113 | 0.6 | 0.4 | 0.42 |
| Colombia | 0.761 | 374 | 6.2 | 775 | 1.6 | 1.4 | 308 | 0.6 | 0.5 | 0.39 |
| Costa Rica | 0.794 | 929 | 8.1 | 78 | 1.6 | 1.2 | 35 | 0.7 | 0.5 | 0.44 |
| Croatia | 0.837 | 852 | 7.4 | 291 | 7.2 | 3.8 | 117 | 2.9 | 1.5 | 0.40 |
| Cuba | 0.778 | 826 | 10.9 | 1238 | 11.0 | 6.2 | 380 | 3.4 | 1.8 | 0.31 |
| Cyprus | 0.873 | 1563 | 6.8 | 29 | 2.5 | 1.6 | 8 | 0.7 | 0.5 | 0.27 |
| Czechia | 0.891 | 1284 | 7.3 | 859 | 8.3 | 4.3 | 361 | 3.5 | 1.8 | 0.42 |
| Denmark | 0.930 | 5497 | 10.3 | 397 | 7.1 | 3.8 | 125 | 2.2 | 1.1 | 0.31 |
| Ecuador | 0.758 | 530 | 8.5 | 217 | 1.3 | 1.2 | 82 | 0.5 | 0.5 | 0.38 |
| Egypt | 0.700 | 157 | 4.2 | 1295 | 1.3 | 1.6 | 352 | 0.4 | 0.4 | 0.28 |
| Estonia | 0.882 | 1112 | 6.5 | 79 | 6.2 | 3.3 | 40 | 3.1 | 1.7 | 0.50 |
| Fiji | 0.724 | 175 | 3.6 | 27 | 3.0 | 2.9 | 11 | 1.2 | 1.2 | 0.40 |
| Finland | 0.925 | 4005 | 9.4 | 348 | 6.5 | 3.0 | 116 | 2.2 | 0.9 | 0.34 |
| France | 0.891 | 4026 | 11.1 | 6815 | 10.8 | 6.2 | 1516 | 2.4 | 1.3 | 0.22 |
| Germany | 0.939 | 4592 | 11.2 | 7271 | 9.1 | 4.4 | 2311 | 2.9 | 1.3 | 0.32 |
| Iceland | 0.938 | 4375 | 8.6 | 13 | 3.9 | 2.3 | 3 | 0.9 | 0.5 | 0.23 |
| Ireland | 0.942 | 4757 | 7.8 | 275 | 5.8 | 3.7 | 74 | 1.6 | 0.9 | 0.28 |
| Israel | 0.906 | 2756 | 7.4 | 155 | 1.9 | 1.4 | 51 | 0.6 | 0.4 | 0.32 |
| Italy | 0.883 | 2700 | 9.0 | 3500 | 6.1 | 2.7 | 1184 | 2.1 | 0.9 | 0.34 |
| Jamaica | 0.726 | 294 | 5.9 | 52 | 1.8 | 1.5 | 15 | 0.5 | 0.4 | 0.29 |
| Japan | 0.915 | 3733 | 10.9 | 8138 | 6.7 | 2.8 | 2496 | 2.1 | 0.7 | 0.31 |
| Kuwait | 0.808 | 1169 | 4.0 | 59 | 1.4 | 2.0 | 33 | 0.8 | 1.1 | 0.56 |
| Latvia | 0.854 | 784 | 5.8 | 239 | 12.7 | 6.8 | 113 | 6.0 | 3.2 | 0.47 |
| Lithuania | 0.869 | 923 | 6.5 | 188 | 6.7 | 3.7 | 114 | 4.1 | 2.3 | 0.61 |
| Luxembourg | 0.909 | 6236 | 6.0 | 45 | 7.8 | 4.8 | 10 | 1.7 | 1.0 | 0.22 |
| Malaysia | 0.804 | 386 | 4.0 | 640 | 2.0 | 2.0 | 302 | 1.0 | 1.0 | 0.48 |
| Malta | 0.885 | 2304 | 9.6 | 18 | 4.2 | 1.9 | 6 | 1.4 | 0.4 | 0.33 |
| Mauritius | 0.796 | 506 | 5.5 | 62 | 4.9 | 3.3 | 28 | 2.2 | 1.5 | 0.45 |
| Netherlands | 0.934 | 4746 | 10.7 | 1418 | 8.5 | 4.4 | 257 | 1.5 | 0.7 | 0.18 |
| New Zealand | 0.921 | 3554 | 9.3 | 264 | 5.7 | 3.4 | 58 | 1.2 | 0.7 | 0.21 |
| Norway | 0.954 | 7464 | 10.0 | 362 | 6.9 | 3.7 | 68 | 1.3 | 0.7 | 0.19 |
| Oman | 0.834 | 636 | 3.8 | 65 | 1.3 | 2.0 | 31 | 0.6 | 1.1 | 0.49 |
| Philippines | 0.712 | 127 | 4.4 | 1372 | 1.3 | 1.6 | 673 | 0.6 | 0.8 | 0.48 |
| Poland | 0.872 | 797 | 6.3 | 3203 | 8.6 | 4.8 | 1505 | 4.0 | 2.2 | 0.47 |
| Portugal | 0.850 | 1722 | 9.0 | 817 | 8.2 | 4.3 | 269 | 2.7 | 1.4 | 0.33 |
| Qatar | 0.848 | 2030 | 3.1 | 26 | 1.0 | 2.0 | 14 | 0.5 | 1.4 | 0.54 |
| Russian Federation | 0.824 | 524 | 5.6 | 9340 | 6.6 | 4.0 | 5443 | 3.8 | 2.3 | 0.58 |
| Serbia | 0.799 | 491 | 9.4 | 701 | 8.1 | 4.9 | 261 | 3.0 | 1.7 | 0.37 |
| Singapore | 0.935 | 2280 | 4.3 | 199 | 3.5 | 1.9 | 85 | 1.5 | 0.8 | 0.43 |
| Slovakia | 0.857 | 1108 | 6.9 | 541 | 10.1 | 6.0 | 224 | 4.2 | 2.5 | 0.42 |
| Slovenia | 0.902 | 1772 | 8.5 | 135 | 6.7 | 3.5 | 47 | 2.3 | 1.1 | 0.34 |
| South Africa | 0.705 | 471 | 8.2 | 1328 | 2.3 | 2.7 | 829 | 1.4 | 1.7 | 0.61 |
| South Korea | 0.906 | 2013 | 7.4 | 1467 | 2.9 | 1.6 | 507 | 1.0 | 0.5 | 0.34 |
| Spain | 0.893 | 2354 | 9.2 | 3843 | 8.6 | 4.0 | 969 | 2.2 | 1.0 | 0.26 |
| Sweden | 0.937 | 5600 | 11.0 | 556 | 5.7 | 2.8 | 145 | 1.5 | 0.7 | 0.26 |
| Switzerland | 0.946 | 9818 | 12.1 | 639 | 7.7 | 4.0 | 184 | 2.2 | 1.1 | 0.29 |
| Thailand | 0.765 | 217 | 3.8 | 4169 | 6.1 | 3.8 | 2159 | 3.2 | 2.0 | 0.52 |
| Trinidad and Tobago | 0.799 | 1146 | 6.0 | 42 | 3.1 | 2.2 | 20 | 1.5 | 1.1 | 0.48 |
| Ukraine | 0.750 | 125 | 6.1 | 3358 | 7.8 | 4.4 | 2058 | 4.7 | 2.8 | 0.60 |
| United Kingdom | 0.920 | 4356 | 9.9 | 5645 | 8.7 | 4.9 | 1443 | 2.2 | 1.1 | 0.25 |
| United States of America | 0.920 | 9536 | 16.8 | 22715 | 7.1 | 4.2 | 3830 | 1.2 | 0.7 | 0.17 |
| Uruguay | 0.808 | 1281 | 9.2 | 149 | 4.4 | 2.9 | 70 | 2.1 | 1.3 | 0.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sung, W.-W.; Hsu, Y.-C.; Dong, C.; Chen, Y.-C.; Chao, Y.-C.; Chen, C.-J. Favorable Lip and Oral Cancer Mortality-to-Incidence Ratios in Countries with High Human Development Index and Expenditures on Health. Int. J. Environ. Res. Public Health 2021, 18, 6012. https://doi.org/10.3390/ijerph18116012
Sung W-W, Hsu Y-C, Dong C, Chen Y-C, Chao Y-C, Chen C-J. Favorable Lip and Oral Cancer Mortality-to-Incidence Ratios in Countries with High Human Development Index and Expenditures on Health. International Journal of Environmental Research and Public Health. 2021; 18(11):6012. https://doi.org/10.3390/ijerph18116012
Chicago/Turabian StyleSung, Wen-Wei, Yong-Chen Hsu, Chen Dong, Ying-Ching Chen, Yu-Chi Chao, and Chih-Jung Chen. 2021. "Favorable Lip and Oral Cancer Mortality-to-Incidence Ratios in Countries with High Human Development Index and Expenditures on Health" International Journal of Environmental Research and Public Health 18, no. 11: 6012. https://doi.org/10.3390/ijerph18116012