
Barriers and Facilitators for Physical Activity in Adults with Type 2 Diabetes Mellitus: A Scoping Review


Abstract
:1. Introduction
2. Aim
3. Methods Design
3.1. Identifying the Research Question
3.2. Identifying Relevant Studies
3.3. Study Selection
3.4. Charting the Data
3.5. Collating, Summarizing, and Reporting Results
4. Results
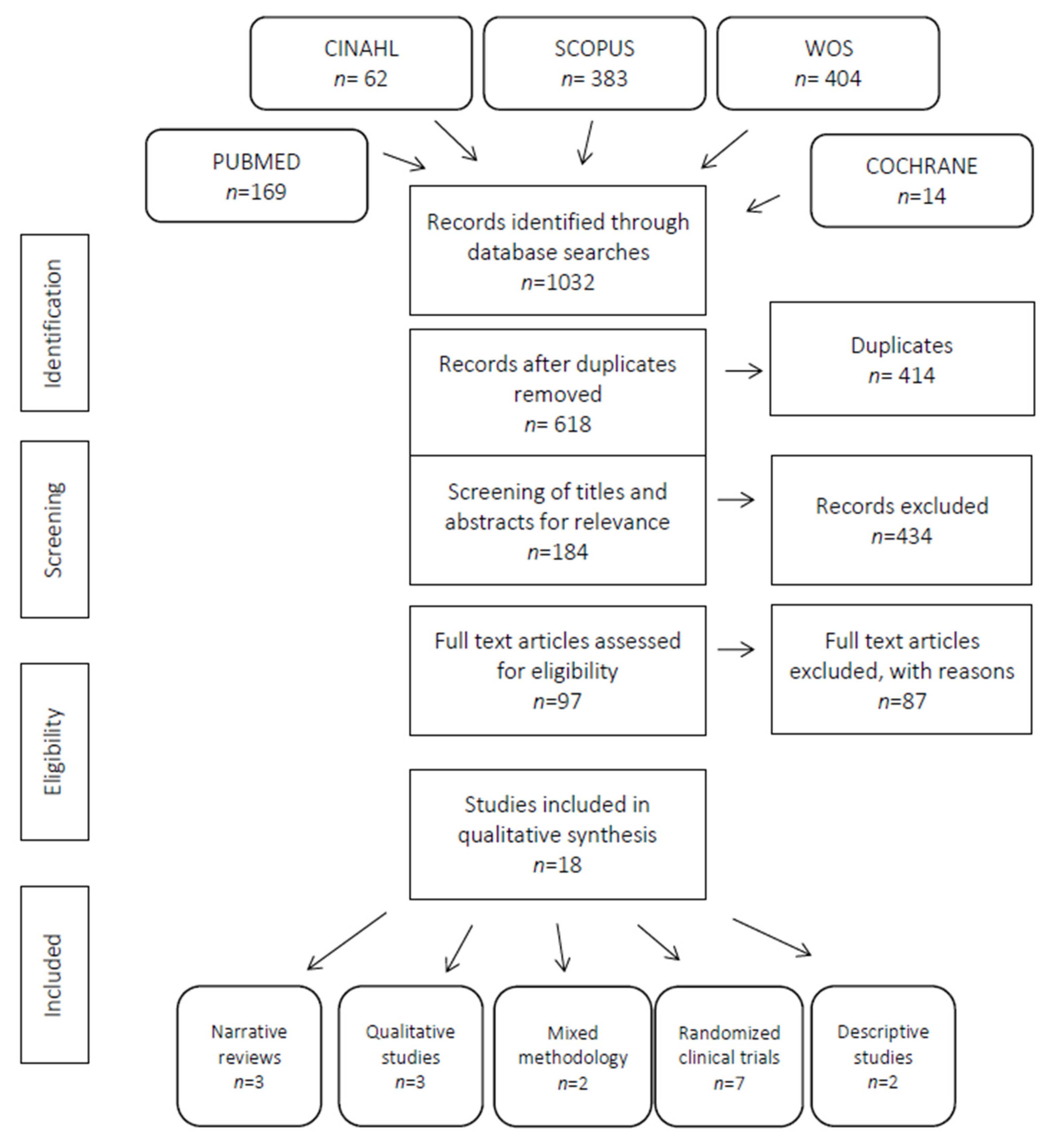
4.1. Identification and Selection of Relevant Papers
4.2. Risk of Bias, Validity, and Methodological Quality
4.3. Factors That Influence the Performance of Physical Activity in Adults with Type 2 Diabetes Mellitus
5. Discussion
5.1. Socio-Demographic Characteristics
5.2. Personal Component
5.3. Motivation Component
5.4. Social Component
5.5. Mental Component
5.6. Clinical Component
5.7. Self-Efficacy Component
6. Strengths and Limitations of the Review
7. Conclusions
Implications for Practice
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- WHO. Diabetes. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 8 September 2019).
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aranceta-Bartrina, J.; Pérez-Rodrigo, C.; Alberdi-Aresti, G.; Ramos-Carrera, N.; Lázaro-Masedo, S. Prevalencia de obesidad general y obesidad abdominal en la población adulta española (25–64 años) 2014–2015: Estudio ENPE. Rev. Española Cardiol. 2016, 69, 579–587. [Google Scholar] [CrossRef]
- Islam, S.M.S.; Lechner, A.; Ferrari, U.; Laxy, M.; Seissler, J.; Brown, J.; Niessen, L.W.; Holle, R. Healthcare use and expenditure for diabetes in Bangladesh. BMJ Glob. Health 2017, 2, e000033. [Google Scholar] [CrossRef] [Green Version]
- Ortiz, M.; Ortiz, E.; Gatica, A.; Gómez, D. Factores Psicosociales Asociados a la Adherencia al Tratamiento de la Diabetes Mellitus Tipo 2. Ter. Psicol. 2011, 29, 5–11. [Google Scholar] [CrossRef]
- Broadbent, E.; Donkin, L.; Stroh, J.C. Illness and Treatment Perceptions Are Associated With Adherence to Medications, Diet, and Exercise in Diabetic Patients. Diabetes Care 2011, 34, 338–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, E.H.B.; Katon, W.; Von Korff, M.; Rutter, C.; Simon, G.E.; Oliver, M.; Ciechanowski, P.; Ludman, E.J.; Bush, T.; Young, B. Relationship of depression and diabetes self-care, medication adherence, and preventive care. Diabetes Care 2004, 27, 2154–2160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cradock, K.A.; Ólaighin, G.; Finucane, F.M.; Gainforth, H.L.; Quinlan, L.R.; Ginis, K.A.M. Behaviour change techniques targeting both diet and physical activity in type 2 diabetes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Márquez, J.; Ramón, G.; Márquez, J. Actualidad en ejercicio y diabetes tipo 2 (I). Arch. Med. Deporte 2011, 28, 113–120. [Google Scholar]
- Oliveira, C.; Simões, M.; Carvalho, J.; Ribeiro, J. Combined exercise for people with type 2 diabetes mellitus: A systematic review. Diabetes Res. Clin. Pract. 2012, 98, 187–198. [Google Scholar] [CrossRef]
- Yang, P.; Oh, P. Predicting Aerobic Fitness Improvements after Participation in a Hybrid Supervised and Home-Based Exercise Program in People with Type 2 Diabetes. Can. J. Diabetes 2013, 37, 388–393. [Google Scholar] [CrossRef]
- Chan, A.W.K.; Chair, S.Y.; Lee, D.T.F.; Leung, D.Y.P.; Sit, J.W.H.; Cheng, H.Y.; Taylor-Piliae, R.E. Tai Chi exercise is more effective than brisk walking in reducing cardiovascular disease risk factors among adults with hypertension: A randomised controlled trial. Int. J. Nurs. Stud. 2018, 88, 44–52. [Google Scholar] [CrossRef]
- Centis, E.; Trento, M.; Cas, A.D.; Pontiroli, A.E.; De Feo, P.; Bruno, A.; Sasdelli, A.S.; Arturi, F.; Strollo, F.; Kreutzenberg, S.V.D.; et al. Stage of change and motivation to healthy diet and habitual physical activity in type 2 diabetes. Acta Diabetol. 2014, 51, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Vähäsarja, K.; Salmela, S.; Villberg, J.; Rintala, P.; Vanhala, M.; Saaristo, T.; Peltonen, M.; Keinänen-Kiukaanniemi, S.; Korpi-Hyövälti, E.; Kujala, U.M.; et al. Perceived need to increase physical activity levels among adults at high risk of type 2 diabetes. A cross-sectional analysis within a community-based diabetes prevention project FIN-D2D. BMC Public Health 2012, 12, 514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caetano, I.R.C.E.S.; Santiago, L.M.; Marques, M. Impact of written information on control and adherence in type 2 diabetes. Rev. Assoc. Médica Bras. 2018, 64, 140–147. [Google Scholar] [CrossRef] [Green Version]
- Alonso-Domínguez, R.; Gómez-Marcos, M.A.; Patino-Alonso, M.C.; Sánchez-Aguadero, N.; Agudo-Conde, C.; Castaño-Sánchez, C.; García-Ortiz, L.; Recio-Rodríguez, J.I. Effectiveness of a multifactorial intervention based on an application for smartphones, heart-healthy walks and a nutritional workshop in patients with type 2 diabetes mellitus in primary care (EMID): Study protocol for a randomised controlled trial. BMJ Open 2017, 7, e016191. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Domínguez, R.; Patino-Alonso, M.C.; Sánchez-Aguadero, N.; García-Ortiz, L.; Recio-Rodríguez, J.I.; Gómez-Marcos, M.A. Effect of a multifactorial intervention on the increase in physical activity in subjects with type 2 diabetes mellitus: A randomized clinical trial (EMID Study). Eur. J. Cardiovasc. Nurs. 2019, 18, 399–409. [Google Scholar] [CrossRef]
- Koponen, A.M.; Simonsen, N.; Suominen, S.B. Success in increasing physical activity (PA) among patients with type 2 diabetes: A self-determination theory perspective. Health Psychol. Behav. Med. 2018, 6, 104–119. [Google Scholar] [CrossRef] [Green Version]
- Miller, S.T.; Marolen, K. Physical Activity-Related Experiences, Counseling Expectations, Personal Responsibility, and Altruism among Urban African American Women with Type 2 Diabetes. Diabetes Educ. 2012, 38, 229–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koponen, A.M.; Simonsen, N.; Laamanen, R.; Suominen, S.B. Health-care climate, perceived self-care competence, and glycemic control among patients with type 2 diabetes in primary care. Health Psychol. Open 2015, 2. [Google Scholar] [CrossRef] [Green Version]
- Uchino, B.N. Social support and health: A review of physiological processes potentially underlying links to disease outcomes. J. Behav. Med. 2006, 29, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Van Dyck, D.; De Greef, K.; Deforche, B.; Ruige, J.; Tudor-Locke, C.E.; Kaufman, J.-M.; Owen, N.; De Bourdeaudhuij, I. Mediators of physical activity change in a behavioral modification program for type 2 diabetes patients. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortier, M.S.; Duda, J.L.; Guerin, E.; Teixeira, P.J. Promoting physical activity: Development and testing of self-determination theory-based interventions. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira, P.J.; Carraça, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef] [Green Version]
- Koponen, A.M.; Simonsen, N.; Suominen, S.B. Determinants of physical activity among patients with type 2 diabetes: The role of perceived autonomy support, autonomous motivation and self-care competence. Psychol. Health Med. 2016, 22, 332–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez-Zúñiga, B.; Pousada, M.; Hernandez, M.M.; Colberg, S.; Gabarrón, E.; Armayones, M. The Online Big Blue Test for Promoting Exercise: Health, Self-Efficacy, and Social Support. Telemed. J. e-Health 2015, 21, 852–859. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Meca, J. Cómo Realizar Una Revisión Sistemática y un Meta-análisis. Aula Abierta. 2010. Available online: https://dialnet.unirioja.es/descarga/articulo/3316651.pdf (accessed on 24 November 2019).
- Alharbi, M.; Gallagher, R.; Neubeck, L.; Bauman, A.; Prebill, G.; Kirkness, A.; Randall, S. Exercise barriers and the relationship to self-efficacy for exercise over 12 months of a lifestyle-change program for people with heart disease and/or diabetes. Eur. J. Cardiovasc. Nurs. 2017, 16, 309–317. [Google Scholar] [CrossRef]
- Balducci, S.; Sacchetti, M.; Haxhi, J.; Orlando, G.; Zanuso, S.; Cardelli, P.; Cavallo, S.; D’Errico, V.; Ribaudo, M.C.; Biase, N.D.; et al. The Italian Diabetes and Exercise Study 2 (IDES-2): A long-term behavioral intervention for adoption and maintenance of a physically active lifestyle. Trials 2015, 16, 569. [Google Scholar] [CrossRef] [Green Version]
- Bekele, H.; Asefa, A.; Getachew, B.; Belete, A.M. Barriers and Strategies to Lifestyle and Dietary Pattern Interventions for Prevention and Management of TYPE-2 Diabetes in Africa, Systematic Review. J. Diabetes Res. 2020, 2020, 1–14. [Google Scholar] [CrossRef]
- Gallé, F.; Di Onofrio, V.; Cirella, A.; Di Dio, M.; Miele, A.; Spinosa, T.; Liguori, G. Improving Self-Management of Type 2 Diabetes in Overweight and Inactive Patients Through an Educational and Motivational Intervention Addressing Diet and Physical Activity: A Prospective Study in Naples, South Italy. Diabetes Ther. 2017, 8, 875–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laranjo, L.; Neves, A.L.; Costa, A.; Ribeiro, R.T.; Couto, L.; Sá, A.B. Facilitators, barriers and expectations in the self-management of type 2 diabetes—a qualitative study from Portugal. Eur. J. Gen. Pract. 2015, 21, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Liebreich, T.; Plotnikoff, R.C.; Courneya, K.S.; Boulé, N. Diabetes NetPLAY: A physical activity website and linked email counselling randomized intervention for individuals with type 2 diabetes. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, N.; Ferrer, H.B.; Tyrer, F.; Wray, P.; Farooqi, A.; Davies, M.J.; Khunti, K. Barriers and Facilitators to Healthy Lifestyle Changes in Minority Ethnic Populations in the UK: A Narrative Review. J. Racial Ethn. Health Disparities 2017, 4, 1107–1119. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, S.K.; Hemmestad, L.; Macdonald, C.S.; Langberg, H.; Valentiner, L.S. Motivation and Barriers to Maintaining Lifestyle Changes in Patients with Type 2 Diabetes after an Intensive Lifestyle Intervention (The U-TURN Trial): A Longitudinal Qualitative Study. Int. J. Environ. Res. Public Health 2020, 17, 7454. [Google Scholar] [CrossRef]
- Richardson, C.R.; Buis, L.R.; Janney, A.W.; Goodrich, D.E.; Sen, A.; Hess, M.L.; Mehari, K.S.; Fortlage, L.A.; Resnick, P.J.; Zikmund-Fisher, B.J.; et al. An online community improves adherence in an internet-mediated walking program. Part 1: Results of a randomized controlled trial. J. Med. Internet Res. 2010, 12, e71. [Google Scholar] [CrossRef]
- Schneider, K.L.; Panza, E.; Handschin, B.; Ma, Y.; Busch, A.M.; Waring, M.E.; Appelhans, B.M.; Whited, M.C.; Keeney, J.; Kern, D.; et al. Feasibility of Pairing Behavioral Activation with Exercise for Women With Type 2 Diabetes and Depression: The Get It Study Pilot Randomized Controlled Trial. Behav. Ther. 2016, 47, 198–212. [Google Scholar] [CrossRef] [Green Version]
- Soderlund, P.D. Effectiveness of motivational interviewing for improving physical activity self-management for adults with type 2 diabetes: A review. Chronic Illn. 2018, 14, 54–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wycherley, T.P.; Mohr, P.; Noakes, M.; Clifton, P.M.; Brinkworth, G.D. Self-reported facilitators of, and impediments to maintenance of healthy lifestyle behaviours following a supervised research-based lifestyle intervention programme in patients with type 2 diabetes. Diabet. Med. 2012, 29, 632–639. [Google Scholar] [CrossRef]
- Collins, T.C.; Lunos, S.; Ahluwalia, J.S. Self-efficacy is associated with walking ability in persons with diabetes mellitus and peripheral arterial disease. Vasc. Med. 2010, 15, 189–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CASPe|Programa de Habilidades en Lectura Crítica EspañolCritical Appraisal Skills Programme Español. Available online: http://www.redcaspe.org/ (accessed on 10 December 2019).
- Terechenko, N.; Baute, A.; Zamonsky, J. Adherencia al tratamiento en pacientes con Diagnóstico de Diabetes Mellitus Tipo II. Miomed. Fam. Comunitaria 2014, 10, 20–33. [Google Scholar]
- Mendes, R.; Dias, E.; Gama, A.; Castelo-Branco, M.; Themudo-Barata, J.L. Prática de exercício físico e níveis de atividade física habitual em doentes com diabetes tipo 2–estudo piloto em Portugal. Rev. Port. Endocrinol. Diabetes Metab. 2013, 8, 9–15. [Google Scholar] [CrossRef] [Green Version]
- La Osa, A.P.-D.; Villaquirán-Hurtado, A.; Jácome-Velasco, S.; Galvis-Fernández, B.; Granados-Vidal, Y.A. Actividad física en pacientes con diabetes mellitus tipo 2 y relación con características sociodemográficas, clínicas y antropométricas. Univ. Salud 2017, 20, 72–81. [Google Scholar] [CrossRef] [Green Version]
- Figueroa, A.; Quingalombo, G. Correlación Entre las Barreras para Realizar Actividad Física y el Nivel de Hemoglobina Glicosilada a1c en Pacientes Diabéticos que Acuden a la Clínica de Diabetes del Hospital Vozandes de abril a junio de 2017 Usando la Herramienta “Percepción de Barrera. Pontificia Universidad Católica del Ecuador. Available online: http://repositorio.puce.edu.ec/handle/22000/13730 (accessed on 12 June 2020).
- Blanchard, C.; Arthur, H.M.; Gunn, E. Self-efficacy and outcome expectations in cardiac rehabilitation: Associations with women’s physical activity. Rehabil. Psychol. 2015, 60, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.J.; Silva, M.N.; Mata, J.; Palmeira, A.L.; Markland, D. Motivation, self-determination, and long-term weight control. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granados, J.; Gutiérrez, C.; González, L.; Masso, A. Ayudando al paciente diabético con actividad física. Rev. Digit. Act. Física Deporte 2018, 2, 134–139. [Google Scholar]
- Papín, C.; Martín, R.; González, X. Descripción del tipo de motivación de pacientes con diabetes tipo 2 para realizar actividad física. RIdEC 2018, 11, 8–45. [Google Scholar]
- Dabaghi, P.; Dashti, S.; Tofangchiha, S. The effectiveness of training program based on protective motivation theory on improving nutritional behaviors and physical activity in military patients with type 2 diabetes mellitus. J. Fam. Med. Prim. Care 2020, 9, 3328–3332. [Google Scholar] [CrossRef]
- Alarcón-Mora, C.; Veracruzana, M.I.D.S.P.D.L.U.; Hernández-Barrera, L.; Argüelles-Nava, V.; Campos-Uscanga, Y.; Pública, M.I.N.D.S. Social support and its association with diet self-care in patients with diabetes. Liberabit Rev. Peru. Psicol. 2017, 23, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Kadirvelu, A.; Sadasivan, S.; Ng, S.H. Social support in type II diabetes care: A case of too little, too late. Diabetes Metab. Syndr. Obes. Targets Ther. 2012, 5, 407–417. [Google Scholar] [CrossRef] [Green Version]
- Daneta, A.; Prieto, M.; Gamboa, E.; de Retana Garcia, L.O.; March, J. Peer training for patients with diabetes mellitus A quantitative and qualitative evaluation in the Basque Country and Andalusia. Aten. Primaria 2016, 58, 507–517. [Google Scholar]
- Salinero-Fort, M.A.; Gómez-Campelo, P.; Andrés-Rebollo, F.J.S.; Cárdenas-Valladolid, J.; Abánades-Herranz, J.C.; Pau, E.C.D.S.; Chico-Moraleja, R.M.; Beamud-Victoria, D.; De Miguel-Yanes, J.M.; Jimenez-Garcia, R.; et al. Prevalence of depression in patients with type 2 diabetes mellitus in Spain (the DIADEMA Study): Results from the MADIABETES cohort. BMJ Open 2018, 8, e020768. [Google Scholar] [CrossRef] [PubMed]
- Semenkovich, K.; Brown, M.E.; Svrakic, D.M.; Lustman, P.J. Depression in Type 2 Diabetes Mellitus: Prevalence, Impact, and Treatment. Drugs 2015, 75, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Bair, M.J.; Brizendine, E.J.; Ackermann, R.T.; Shen, C.; Kroenke, K.; Marrero, D.G. Prevalence of pain and association with quality of life, depression and glycaemic control in patients with diabetes. Diabet. Med. 2010, 27, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social Foundations of thought and Action; SAGE Publications Ltd.: New Delhi, India, 1986; pp. 23–28. [Google Scholar]
- Adam, J.; Folds, L. Depression, Self-efficacy, and Adherence in Patients with Type 2 Diabetes. J. Nurse Pract. 2014, 10, 646–652. [Google Scholar] [CrossRef]


{kind=link}
| 1. exercise | 11. barrier |
| 2. physical activity | 12. facilitator |
| 3. fitness | 13. adherence |
| 4. 1 or 2 or 3 | 14. compliance |
| 5. diabetes mellitus type 2 | 15. nonadherence |
| 6. habits change | 16. noncompliance |
| 7. habits modification | 17. motivation |
| 8. habits choice | 18. 11 or 12 or 13 or 14 or 15 or 16 or 17 |
| 9. lifestyle change | 19. 4 and 5 and 10 and 18 |
| 10. 6 or 7 or 8 or 9 |
| Author(s), Year of Publication | Study Location | Study Population | Methodology | Theory | Intervention/Tolls (Web, Interview, Primary Care) | Motivation (Email, Motivational Interview) |
|---|---|---|---|---|---|---|
| [30] Alharbi, M., Gallagher, R., Neubeck, L., Bauman, A., et al. 2016 | Australia | n = 134 | Quantitative (randomized controlled trial) and qualitative (semi-structured interviews) | Bandura | 1 h group-based supervised structured exercise twice a week and four 90 min group-based information sessions. Then, 3 telephone follow-up calls over the following 8 months | NO |
| [31] Balducci, S., Sacchetti, M., Haxhi, J., Orlando, G., Zanuso, S., et al. 2015 | Italy | n = 300 | Randomized controlled trial | Social cognitive theory and health belief model | Intervention in the INT group consisted of aggregated behavioral-change techniques once-a-year for 3 years. Theoretical, individual, face-to-face counseling sessions and practical exercise | Efforts are designed to convince the patient that regular PA is the pre-eminent cure for DM2 and to understand the positive expectations the individual patients had of this change in behavior |
| [32] Bekele, H., Asefa, A., Getachew, B., Belete, A.M. | Africa | - | Systematic Review | PICO. The levels of evidence and the quality guides of articles and research papers were evaluated based on the Johns Hopkins Method of Research Evidence Appraisal Tool. | No | No |
| [13] Centis, E., Trento, M., Dei Cas, A., et al. 2014 | Italy | n = 1353 consecutive outpatients with DM2 | Not specified. Use of questionnaires. Descriptive analysis | Prochaska’s model | Face-to-face questionnaire | Motivation to change was tested by the EMME-3 questionnaire for diet and PA |
| [30] Collins, T., Lunos, S., Ahluwalia, J. 2010 | USA | n = 145 subjects with chronic disease (DM1 or DM2 or peripheral arterial disease) | Randomized clinical trial, cross-sectional study | Social Cognitive Theory | Questionnaires, treadmill walking, six-minute walk test | Walking intervention to improve distance at 6 months in individuals with DM2 and peripheral arterial disease |
| [33] Gallé, F., Di Onofrio, V., Cirella, A., et al. 2017 | Italy | n = 130 Overweight and inactive patients with DM2 | Neither experimental nor controlled. Pre-post, prospective | No | 1-h training group sessions performed two times per week and short-form 12 questionnaire | Motivational program, a nutrition program, and an exercise program |
| [26] Gómez-Zúñiga, B., Pousada, M., Hernandez, M., et al. 2015 | USA | n = 3916 people with diabetes completed the BBT (BIG BLUE TEST) | Not specified. RCT | No | Web site (shares his or her experience by collecting own data and answering some questions through the Web) | No |
| [18] Koponen, A.M., Simonsen, N., Suominen, S. 2018 | Finland | n = 256 | Observational, cross-sectional mail survey | Self-determination theory perspective | Interviews with successful and unsuccessful participants | Studied autonomous motivation but did not apply any interventions to increase it |
| [34] Laranjo, L., Neves, A., Costa, A., et al. 2015 | Portugal | n = 16 Patients with type 2 DM were recruited at the Portuguese Diabetes Association outpatient clinic | Qualitative | No | Three video-recorded focus groups. Pre-tested interview guide | No |
| [35] Liebreich, T., Plotnikoff, R.C., Courneya, K.S., et al. 2009 | Canada | n = 49 | Prospective. 2-arm randomized controlled trial. Control/intervention groups | Social Cognitive Theory (SCT) | Web site | Individualized emails were sent on a weekly basis, providing general feedback on the specific topic of the week, progress, and motivation. |
| [19] Miller, S., Marolen, K. 2012 | USA | n = 22 African women with DM2. Two focus groups of 11 participants | Qualitative | Trans-theoretical Model of Behavior Change | Focus group | No |
| [36] Patel, N., Ferrer Harriet, B., Tyrer, F., et al. 2017 | UK | - | Narrative review | Emergent (‘berry picking’) model of information retrieval | No | No |
| [37] Schmidt, S.K., Hemmestad, L., Macdonald, C.S., Langberg, H., Valentiner, L.S. | Denmark | n = 6 (qualitative) | Longitudinal Qualitative Study | Health belief model (HBM), self-determination theory (SDT) and relevant research on the topic | Two rounds of in-depth, semi-structured interviews, conducted in August 2016 and February 2017 | No |
| [38] Richardson, C.R., Buis, L.R., Janney, A.W., et al. 2010 | USA | n = 324 | 2-arm randomized controlled trial | Bandura’s social-cognitive theory and social influence theories including social learning theory | Web page | Individually tailored motivational messages |
| [39] Schneider, K., Panza, E., Handschin, B., Ma, Y., et al. 2016 | USA | n = 20 | Randomization. | Linear mixed models: Littell, Stroup, Milliken, Wolfinger, and Schabenberger | Orientation session and 38 group exercise classes over 24 weeks | No |
| [40] Soderlund, P.D. 2018 | USA | - | Review: type not specified | No | PRISMA | MI proficient counselors who emphasize that PA self-management may help foster PA behavior change |
| [22] Van Dyck, D., De Greef, K., Deforche, B., et al. 2011 | Belgium | n = 143 | Randomized controlled trial | Social cognitive theory of Bandura + Prochaska’s trans-theoretical model de and self-determination theory | Baseline questionnaire administered in patients’ homes by a psychologist (IPAQ). The subject was provided with a pedometer. Follow-up by telephone | There was no increase in autonomous motivation towards physical activity in this study group, although our intervention also incorporated self-determination theory constructs |
| [41] Wycherley, T., Mohr, P., Noakes, M., et al. 2012 | Australia | n = 106 participants commenced and 84 completed the initial 16-week research based supervised lifestyle intervention program. Of the 81 participants invited, 3(37%) completed the 1-year follow-up | Not specified, but it was a non-randomized controlled trial and qualitative study | Standardized open-ended telephone interview | Getting involved in a structured exercise program may lead to improvements that may intrinsically motivate and facilitate exercise participation in the longer term | No |
| Author(s), Year of Publication | Conditioning Factors: Barriers | Conditioning Factors: Facilitators |
|---|---|---|
| [30] Alharbi, M., Gallagher, R., Neubeck, L., Bauman, A., et al. 2016 | The most common barriers were lack of motivation (40.3%), lack of time overall (30.6%), and lack of time due to family commitments (17.2%). Baseline self-efficacy, depressive symptoms, being female, overweight, and having coronary heart disease | No |
| [31] Balducci, S., Sacchetti, M., Haxhi, J., Orlando, G., Zanuso, S., et al. 2015 | Barriers that are outside the patient’s own control include lack of specific knowledge on the part of both physicians and exercise trainers and lack of dedicated facilities | No |
| [32] Bekele, H., Asefa, A., Getachew, B., Belete, A.M. 2020 | Barriers included the poor knowledge, the perception that exercise potentially exacerbates illness, lack of an exercise partner, specific locations away from home, the rainy season in Africa, criticism by others, and lack of support from the partner, health professionals, family members, and friends. Lack of knowledge and education, poverty and cost, population changes, and lack of access to healthcare | No |
| [13] Centis, E., Trento, M., Dei Cas, A., et al. 2014 | Older age and longer disease duration, Higher motivation to change was recorded in the area of diet compared to that of AF | Higher educational level, self-efficacy was higher in males |
| [42] Collins, T., Lunos, S., Ahluwalia, J. 2010 | Walking alone or in rainy or cold weather | Self-efficacy, motivation |
| [33] Gallé, F., Di Onofrio, V., Cirella, A., et al. 2017 | Physical barriers (disorders, excessive weight, hypoglycemic crisis), psychophysical barriers (laziness, lack of companions, of physician recommendations, low importance attributed to physical activity, feeling unable to exercise) and environmental barriers (lack of time, of green areas, of a gym close by, of equipment at home) | Personal trainer, higher educational level, women |
| [26] Gómez-Zúñiga, B., Pousada, M., Hernandez, M., et al. 2015 | Less social support, DM1 fear of hypoglycemia | Social norms, self-efficacy |
| [18] Koponen, A.M., Simonsen, N., Suominen, S. 2018 | Poor health, stress, and insulin medication slightly, higher age, poor health, and social support | Autonomous motivation, self-care competence and perceived autonomy support correlated |
| [34] Laranjo, L., Neves, A., Costa, A., et al. 2015 | Lack of motivation and willpower, and not having created the habit of exercising. To a lesser degree: fatigue, muscle and joint pain, lack of information regarding the specific types of physical activities, lack of family or friend support. Themes PA: Decisional, Fatigue, Pain and Co-morbidities | Information and knowledge translation, as well as family and social ties |
| [35] Liebreich, T., Plotnikoff, R.C., Courneya, K.S., et al. 2009 | No | Information accessed through the virtual library, and therefore increased their physical activity as well |
| [19] Miller, S., Marolen, K. 2012 | Lack of motivation, laziness, competing priorities | Social support, motivation |
| [36] Patel, N., Ferrer Harriet, B., Tyrer, F., et al. 2017 | Car travel, racial harassment, or abuse when exercising and, for women, expectations to remain in the home, fear for personal safety, lack of same gender venues and concerns over the acceptability of wearing ‘western’ exercise clothing | Weight gain might compromise family/carer responsibilities, desire to be healthy, DM2 diagnosis, and exercise classes held in ‘safe’ environments such as places of worship |
| [37] Schmidt, S.K., Hemmestad, L., Macdonald, C.S., Langberg, H., Valentiner, L.S. 2020 | No | Five motivating factors were identified: achievement of results (reduce their daily medicine intake and live an overall healthier life), social support and relatedness (with help from the coaches, they developed skill and confidence in exercising), support from health care professionals and identification with acceptance of lifestyle (displayed signs of the new lifestyle being part of their lives and self-image) |
| [38] Richardson, C.R., Buis, L.R., Janney, A. W, et al. 2010 | Participants with low baseline social support for physical activity used the online community features more than participants with high baseline social support | Participants in both arms who reported having social support at the end of the study were more likely to increase their step counts. More posts written, and pages viewed correlated with greater reported motivation to increase walking |
| [39] Schneider, K., Panza, E., Handschin, B., Ma, Y., et al. 2016 | Pain, general exercise barriers and symptoms of major depression, comorbid depression and inadequately controlled diabetes | Family, social support |
| [40] Soderlund, P.D. 2018 | Time within the healthcare setting | (1) counselors focused on a minimal number of DM2 self-management behaviors (2) MI counselors should emphasize either the frequency or duration of MI sessions (3) MI proficient counselors MI may be more effective when counselors prioritize a minimal number of target behaviors over the course of a few sessions |
| [22] Van Dyck, D., De Greef, K., Deforche, B., et al. 2011 | Self-efficacy towards physical activity barriers was not a mediator during the intervention period (short-term), but only after the intervention ended (intermediate-term) | Positive social norms and modeling from family. Coping with relapse, defined as the ability to avoid and cope with relapse-inducing situations. Sport partner. Social support from family did not mediate short-term physical activity changes but was the most consistent mediator of intermediate-term changes of physical activity |
| [41] Wycherley, T., Mohr, P., Noakes, M., et al. 2012 | Undertaking moderate to high intensity exercise and overcoming the initial challenge of doing exercise | Supervised exercise training during the program indicated access to appropriate programs/facilities, more affordable gym membership and having a personal trainer /motivator. the motivation derived from the general improvements they experienced during the program, encouragement and troubleshooting efforts of the staff, personal persistence and, less commonly, the motivating effects of having lost weight and achieved improvements in diabetes control. Support from staff |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vilafranca Cartagena, M.; Tort-Nasarre, G.; Rubinat Arnaldo, E. Barriers and Facilitators for Physical Activity in Adults with Type 2 Diabetes Mellitus: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 5359. https://doi.org/10.3390/ijerph18105359
Vilafranca Cartagena M, Tort-Nasarre G, Rubinat Arnaldo E. Barriers and Facilitators for Physical Activity in Adults with Type 2 Diabetes Mellitus: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(10):5359. https://doi.org/10.3390/ijerph18105359
Chicago/Turabian StyleVilafranca Cartagena, Mireia, Glòria Tort-Nasarre, and Esther Rubinat Arnaldo. 2021. "Barriers and Facilitators for Physical Activity in Adults with Type 2 Diabetes Mellitus: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 10: 5359. https://doi.org/10.3390/ijerph18105359
APA StyleVilafranca Cartagena, M., Tort-Nasarre, G., & Rubinat Arnaldo, E. (2021). Barriers and Facilitators for Physical Activity in Adults with Type 2 Diabetes Mellitus: A Scoping Review. International Journal of Environmental Research and Public Health, 18(10), 5359. https://doi.org/10.3390/ijerph18105359