
Effect of the COVID-19 Pandemic on Medical Student Career Perceptions: Perspectives from Medical Students in China


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Design
2.2. Measures
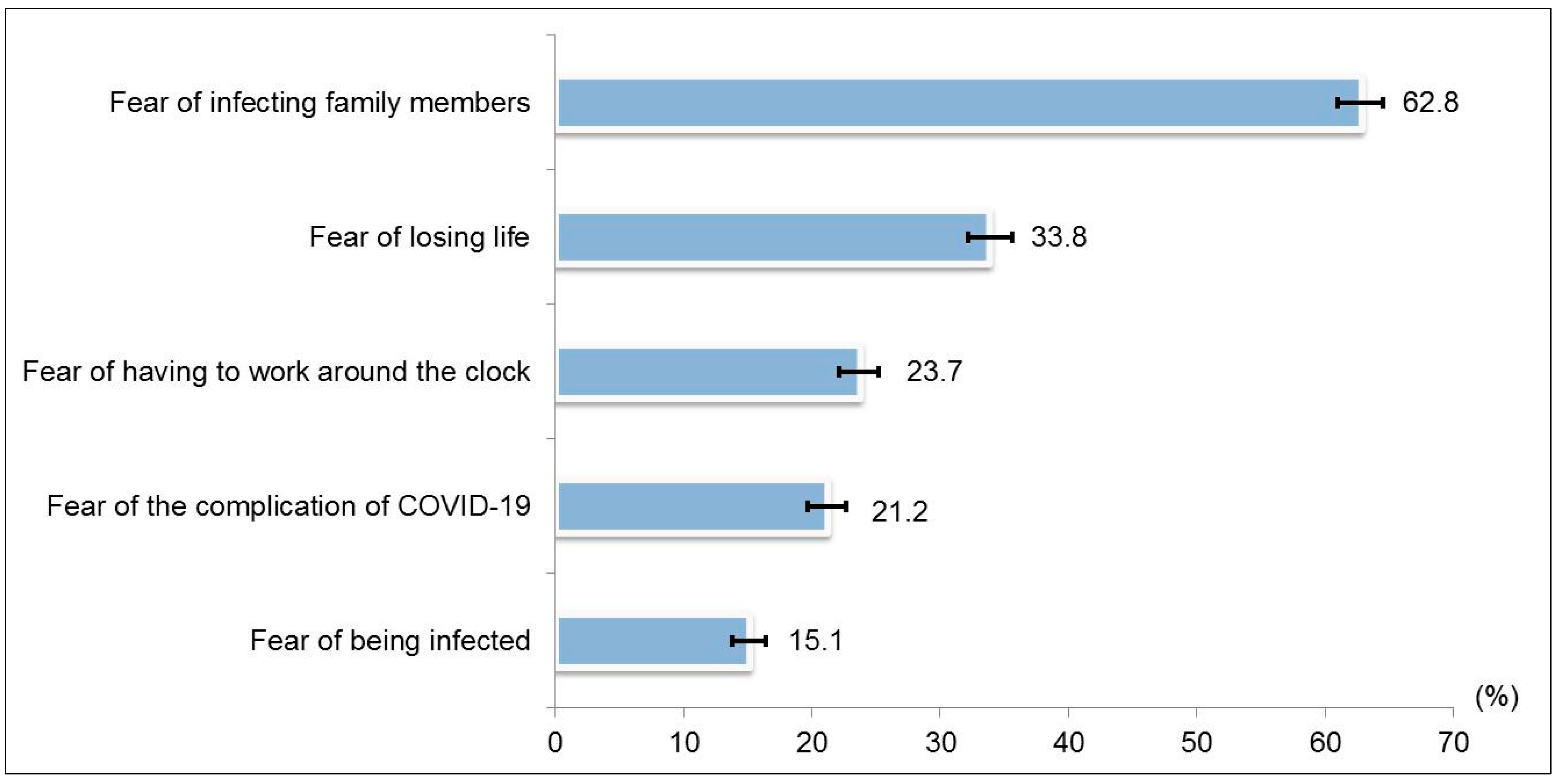
2.2.1. Perceived Fear of COVID-19
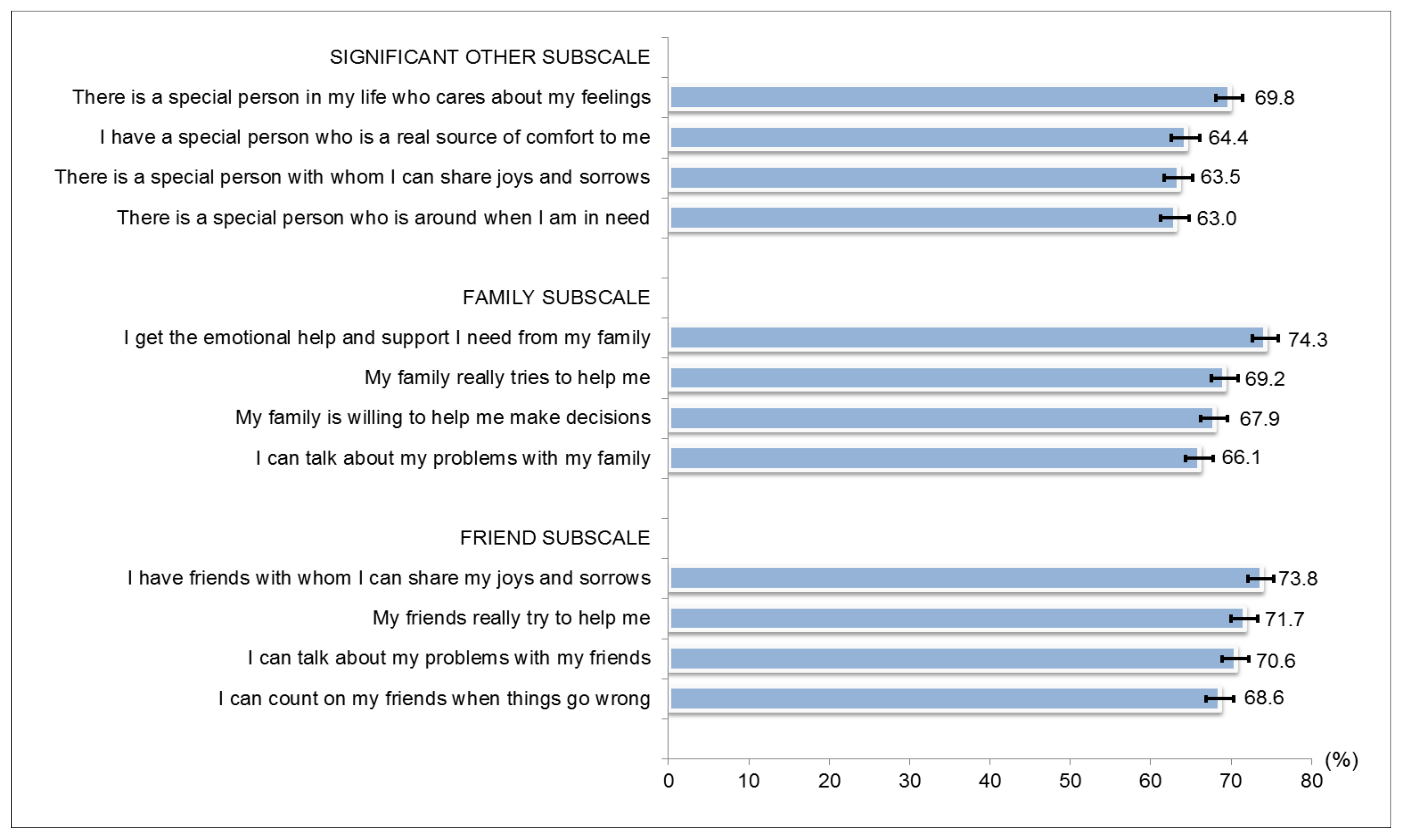
2.2.2. Multidimensional Scale of Perceived Social Support (MSPSS)
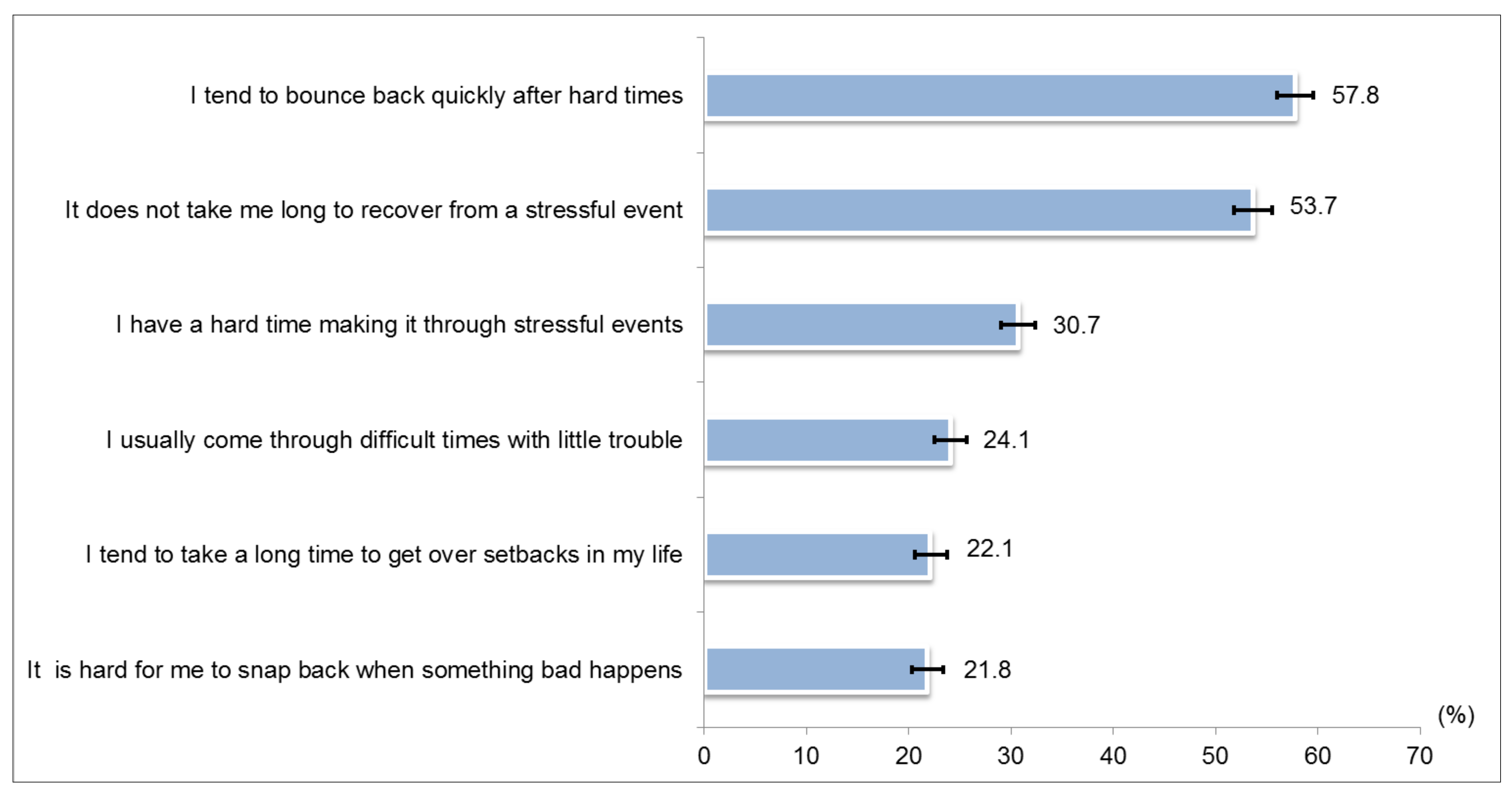
2.2.3. Brief Resilience Scale (BRS)
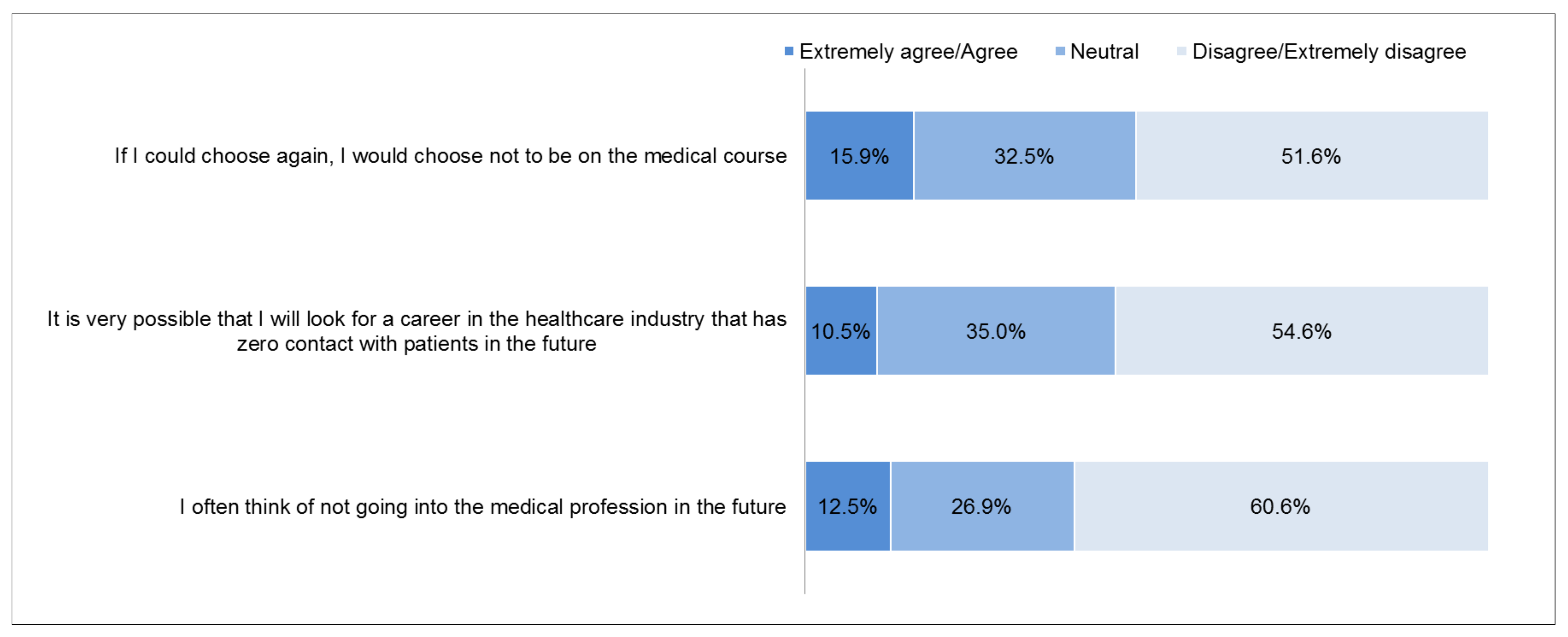
2.2.4. Attitudes towards the Medical Profession
2.2.5. Turnover Intention Scale
2.3. Statistical Analyses
2.4. Ethical Considerations
3. Results
3.1. Perceived Fear of COVID-19
3.2. Multidimensional Scale of Perceived Social Support (MSPSS)
3.3. Brief Resilience Scale (BRS)
3.4. Attitudes towards the Medical Profession
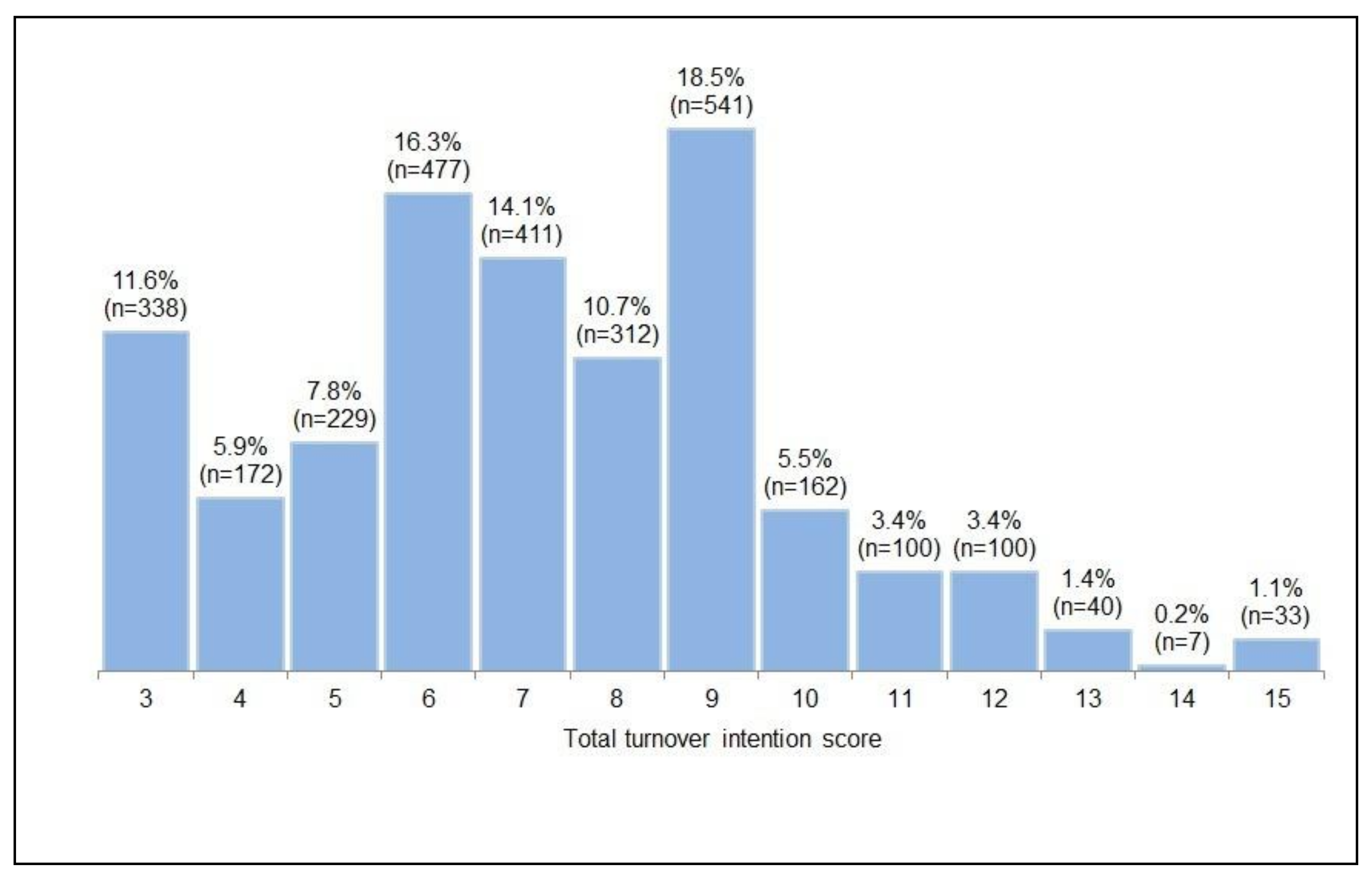
3.5. Turnover Intention Scale
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Weekly Epidemiological Update—29 December 2020. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update---29-december-2020 (accessed on 14 January 2021).
- Bielicki, J.A.; Duval, X.; Gobat, N.; Goossens, H.; Koopmans, M.; Tacconelli, E.; van der Werf, S. Monitoring approaches for health-care workers during the COVID-19 pandemic. Lancet Infect. Dis. 2020, 20, e261–e267. [Google Scholar] [CrossRef]
- Ahmed, H.; Carmody, J.B. On the Looming Physician Shortage and Strategic Expansion of Graduate Medical Education. Cureus 2020, 12, e9216. [Google Scholar] [CrossRef] [PubMed]
- Lien, S.S.; Kosik, R.O.; Fan, A.P.; Huang, L.; Zhao, X.; Chang, X.; Wang, Y.; Chen, Q. 10-year trends in the production and attrition of Chinese medical graduates: An analysis of nationwide data. Lancet 2016, 388, S11. [Google Scholar] [CrossRef]
- Wu, Q.; Zhao, L.; Ye, X.-C. Shortage of healthcare professionals in China. BMJ 2016, 354, i4860. [Google Scholar] [CrossRef]
- Sun, S.; Xie, Z.; Yu, K.; Jiang, B.; Zheng, S.; Pan, X. COVID-19 and healthcare system in China: Challenges and progression for a sustainable future. Glob. Health 2021, 17, 1–8. [Google Scholar] [CrossRef]
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; Kamath, A.; Parepalli, S.A.; Brown, G.; Iharchane, S.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5, e003097. [Google Scholar] [CrossRef]
- Giménez-Espert, M.D.C.; Prado-Gascó, V.; Soto-Rubio, A. Psychosocial Risks, Work Engagement, and Job Satisfaction of Nurses During COVID-19 Pandemic. Front. Public Health 2020, 8, 566896. [Google Scholar] [CrossRef]
- Zhang, S.X.; Chen, J.; Jahanshahi, A.A.; Alvarez-Risco, A.; Dai, H.; Li, J.; Patty-Tito, R.M. Succumbing to the COVID-19 Pandemic—Healthcare Workers Not Satisfied and Intend to Leave Their Jobs. Int. J. Ment. Health Addict. 2021, 7, 1–10. [Google Scholar] [CrossRef]
- Labrague, L.J.; Santos, J.A.A. Fear of COVID-19, psychological distress, work satisfaction and turnover intention among frontline nurses. J. Nurs. Manag. 2021, 29, 395–403. [Google Scholar] [CrossRef]
- Khattak, S.R.; Saeed, I.; Rehman, S.U.; Fayaz, M. Impact of Fear of COVID-19 Pandemic on the Mental Health of Nurses in Pakistan. J. Loss Trauma 2020, 1–15. [Google Scholar] [CrossRef]
- Sanghera, J.; Pattani, N.; Hashmi, Y.; Varley, K.F.; Cheruvu, M.S.; Bradley, A.; Burke, J.R. The impact of SARS-CoV-2 on the mental health of healthcare workers in a hospital setting—A Systematic Review. J. Occup. Health 2020, 62, e12175. [Google Scholar] [CrossRef]
- Sun, J.; Ma, J.; Hu, G.; Zhao, Q.; Yuan, C.; Si, W.; Zhang, X.; Liu, Y. Welfare, wellness, and job satisfaction of Chinese physicians: A national survey of public tertiary hospitals in China. Int. J. Health Plan. Manag. 2017, 32, 270–284. [Google Scholar] [CrossRef]
- He, R.; Liu, J.; Zhang, W.-H.; Zhu, B.; Zhang, N.; Mao, Y. Turnover intention among primary health workers in China: A systematic review and meta-analysis. BMJ Open 2020, 10, e037117. [Google Scholar] [CrossRef]
- Duan, X.; Ni, X.; Shi, L.; Zhang, L.; Ye, Y.; Mu, H.; Li, Z.; Liu, X.; Fan, L.; Wang, Y. The impact of workplace violence on job satisfaction, job burnout, and turnover intention: The mediating role of social support. Health Qual. Life Outcomes 2019, 17, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.H.; Kim, J.K. Factors Influencing Turnover Intention in Clinical Nurses: Compassion Fatigue, Coping, Social Support, and Job Satisfaction. J. Korean Acad. Nurs. Adm. 2016, 22, 562–569. [Google Scholar] [CrossRef]
- Srivastava, S.; Madan, P. The relationship between resilience and career satisfaction: Trust, political skills and organizational identification as moderators. Aust. J. Career Dev. 2020, 29, 44–53. [Google Scholar] [CrossRef]
- Yu, M.; Lee, H. Impact of resilience and job involvement on turnover intention of new graduate nurses using structural equation modeling. Jpn. J. Nurs. Sci. 2018, 15, 351–362. [Google Scholar] [CrossRef]
- Zou, G.; Shen, X.; Tian, X.; Liu, C.; Li, G.; Kong, L.; Li, P. Correlates of psychological distress, burnout, and resilience among Chinese female nurses. Ind. Health 2016, 54, 389–395. [Google Scholar] [CrossRef] [Green Version]
- RistiĆ, D.I.; Hinić, D.; Banković, D.; Kočović, A.; Ristić, I.; Rosić, G.; Ristić, B.; MilovanoviĆ, D.; JanjiĆ, V.; JovanoviĆ, M.; et al. Levels of stress and resilience related to the COVID -19 pandemic among academic medical staff in Serbia. Psychiatry Clin. Neurosci. 2020, 74, 604–605. [Google Scholar] [CrossRef]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Pers. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Chou, K.-L. Assessing Chinese adolescents’ social support: The multidimensional scale of perceived social support. Pers. Individ. Differ. 2000, 28, 299–307. [Google Scholar] [CrossRef]
- Wang, Y.; Wan, Q.; Huang, Z.; Huang, L.; Kong, F. Psychometric Properties of Multi-Dimensional Scale of Perceived Social Support in Chinese Parents of Children with Cerebral Palsy. Front. Psychol. 2017, 8, 2020. [Google Scholar] [CrossRef] [Green Version]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.M.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- The Ohio State University. Brief Resilience Scale (BRS). Available online: https://ogg.osu.edu/media/documents/MB%20Stream/Brief%20Resilience%20Scale.pdf (accessed on 15 January 2021).
- Coelho, G.L.D.H.; Hanel, P.H.P.; Cavalcanti, T.M.; Rezende, A.T.; Gouveia, V.V. Brief Resilience Scale: Testing its factorial structure and invariance in Brazil. Univ. Psychol. 2016, 15, 397. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Liu, Y. The salary of physicians in Chinese public tertiary hospitals: A national cross-sectional and follow-up study. BMC Health Serv. Res. 2018, 18, 1–9. [Google Scholar] [CrossRef]
- Lo, D.; Wu, F.; Chan, M.; Chu, R.; Li, D. A systematic review of burnout among doctors in China: A cultural perspective. Asia Pac. Fam. Med. 2018, 17, 3. [Google Scholar] [CrossRef] [Green Version]
- Camman, C.; Fichman, M.; Jenkins, D.; Klesh, J. The Organizational Assessment Questionnaire; University of Michigan: Ann Arbor, MI, USA, 1979; Unpublished Manuscript; Available online: https://www.scirp.org/(S(i43dyn45teexjx455qlt3d2q))/reference/ReferencesPapers.aspx?ReferenceID=2018239 (accessed on 15 January 2021).
- Katz, M.H. Multivariable Analysis: A Practical Guide for Clinicians and Public Health Researchers; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; John Wiley & Sons: New York, NY, USA, 2013. [Google Scholar]
- Szmyd, B.; Bartoszek, A.; Karuga, F.; Staniecka, K.; Błaszczyk, M.; Radek, M. Medical Students and SARS-CoV-2 Vaccination: Attitude and Behaviors. Vaccines 2021, 9, 128. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Hu, D.; Kong, Y.; Li, W.; Han, Q.; Zhang, X.; Zhu, L.X.; Wan, S.W.; Liu, Z.; Shen, Q.; Yang, J.; et al. Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large-scale cross-sectional study. EClinicalMedicine 2020, 24, 100424. [Google Scholar] [CrossRef]
- Szmyd, B.; Karuga, F.; Bartoszek, A.; Staniecka, K.; Siwecka, N.; Bartoszek, A.; Błaszczyk, M.; Radek, M. Attitude and Behaviors towards SARS-CoV-2 Vaccination among Healthcare Workers: A Cross-Sectional Study from Poland. Vaccines 2021, 9, 218. [Google Scholar] [CrossRef]
- Zheng, L.; Wang, X.; Zhou, C.; Liu, Q.; Li, S.; Sun, Q.; Wang, M.; Zhou, Q.; Wang, W. Analysis of the Infection Status of Healthcare Workers in Wuhan During the COVID-19 Outbreak: A Cross-sectional Study. Clin. Infect. Dis. 2020, 71, 2109–2113. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Lei, W.; Xu, F.; Liu, H.; Yu, L. Emotional responses and coping strategies in nurses and nursing students during Covid-19 outbreak: A comparative study. PLoS ONE 2020, 15, e0237303. [Google Scholar] [CrossRef] [PubMed]
- Zamani-Alavijeh, F.; Dehkordi, F.R.; Shahry, P. Perceived social support among students of medical sciences. Electron. Physician 2017, 9, 4479–4488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, C.; Siddiq, A.A.; Aida, S.; Zainal, N.; Koh, O. Validation of the Malay version of the Multidimensional Scale of Perceived Social Support (MSPSS-M) among a group of medical students in Faculty of Medicine, University Malaya. Asian J. Psychiatry 2010, 3, 3–6. [Google Scholar] [CrossRef]
- Jordan, R.K.; Shah, S.S.; Desai, H.; Tripi, J.; Mitchell, A.; Worth, R.G. Variation of stress levels, burnout, and resilience throughout the academic year in first-year medical students. PLoS ONE 2020, 15, 0240667. [Google Scholar] [CrossRef]
- Fung, S.-F. Validity of the Brief Resilience Scale and Brief Resilient Coping Scale in a Chinese Sample. Int. J. Environ. Res. Public Health 2020, 17, 1265. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, K.; Moutray, M.; Moore, C. Career motivation in nursing students and the perceived influence of significant others. J. Adv. Nurs. 2010, 66, 404–412. [Google Scholar] [CrossRef]
- Ozbay, F.; Johnson, D.C.; Dimoulas, E.; Morgan, C.A., III; Charney, D.; Southwick, S. Social support and resilience to stress: From neurobiology to clinical practice. Psychiatry (Edgmont) 2007, 4, 35. [Google Scholar]
- Hostinar, C.E.; Gunnar, M.R. Social Support Can Buffer Against Stress and Shape Brain Activity. AJOB Neurosci. 2015, 6, 34–42. [Google Scholar] [CrossRef]
- Foster, K.; Roche, M.; Rn, J.G.; Furness, T. Workplace stressors, psychological well-being, resilience, and caring behaviours of mental health nurses: A descriptive correlational study. Int. J. Ment. Health Nurs. 2020, 29, 56–68. [Google Scholar] [CrossRef]
- Irshad, M.; Khattak, S.A.; Hassan, M.M.; Majeed, M.; Bashir, S. Withdrawn: How perceived threat of Covid-19 causes turnover intention among Pakistani nurses: A moderation and mediation analysis. Int. J. Ment. Health Nurs. 2021, 30, 350. [Google Scholar] [CrossRef]
- Thompson, G.; McBride, R.B.; Hosford, C.C.; Halaas, G. Resilience Among Medical Students: The Role of Coping Style and Social Support. Teach. Learn. Med. 2016, 28, 174–182. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|---|
| Total Turnover Score | Total Turnover Score 7–15 vs. 3–6 | ||||
| N (%) | 3–6 (n = 1216) | 7–15 (n = 1706) | p-Value | OR (95% CI) | |
| Gender | |||||
| Male | 1367 (46.8) | 547 (40.0) | 820 (60.0) | 0.106 | |
| Female | 1555 (53.2) | 669 (43.0) | 886 (57.0) | ||
| Ethnicity | |||||
| Han | 2837 (97.1) | 1184 (41.7) | 1653 (58.3) | 0.503 | |
| Others | 85 (2.9) | 32 (37.6) | 53 (62.4) | ||
| Birthplace | |||||
| Urban | 1269 (43.4) | 567 (44.7) | 702 (55.3) | 0.004 | Reference |
| Rural | 1653 (56.6) | 649 (39.3) | 1004 (60.7) | 1.16 (0.98–1.37) | |
| Year of study | |||||
| Year 1 | 793 (27.1) | 449 (56.6) | 344 (43.4) | Reference | |
| Year 2 | 1017 (34.8) | 404 (39.7) | 613 (60.3) | 1.72 (1.41–2.10) *** | |
| Year 3 | 454 (15.5) | 178 (39.2) | 276 (60.8) | p < 0.001 | 1.77 (1.37–2.28) *** |
| Year 4 | 452 (15.5) | 143 (31.6) | 309 (68.4) | 2.34 (1.80–3.03) *** | |
| Year 5 | 206 (7.0) | 42 (20.4) | 164 (79.6) | 3.88 (2.62–5.73) *** | |
| Household monthly income (CNY) | |||||
| Less than 4000 | 673 (23.0) | 242 (36.0) | 431 (64.0) | 1.07 (0.85–1.36) | |
| 4000–9999 | 1437 (49.2) | 623 (43.4) | 814 (56.6) | 0.003 | 0.94 (0.77–1.14) |
| 10,000 and above | 812 (27.8) | 351 (43.2) | 461 (56.8) | Reference | |
| Fear of COVID-19 | |||||
| Total fear score | |||||
| 0–5 | 1326 (45.4) | 626 (47.2) | 700 (52.8) | p < 0.001 | Reference |
| 6–15 | 1596 (54.6) | 590 (37.0) | 1006 (63.0) | 1.39 (1.78–1.63) *** | |
| Multidimensional Scale of Perceived Social Support (MSPSS) | |||||
| Significant other subscale | |||||
| 1.00–5.00 | 1433 (49.0) | 431 (30.1) | 1002 (69.9) | p < 0.001 | 1.47 (1.17–1.84) ** |
| 5.01–7.00 | 1489 (51.0) | 785 (52.7) | 704 (47.3) | Reference | |
| Family subscale | |||||
| 1.00–5.00 | 1243 (42.5) | 365 (29.4) | 878 (70.6) | p < 0.001 | 1.47 (1.18–1.83) ** |
| 5.01–7.00 | 1679 (57.5) | 851 (50.7) | 828 (49.3) | Reference | |
| Friend subscale | |||||
| 1.00–5.00 | 1367 (46.8) | 416 (30.4) | 951 (69.6) | p < 0.001 | 1.42 (1.14–1.77) ** |
| 5.01–7.00 | 1555 (53.2) | 800 (51.4) | 755 (48.6) | Reference | |
| Brief Resilience Scale (BRS) | |||||
| Total BRS score | |||||
| Low resilience score (1.00–2.99) | 595 (20.4) | 183 (30.8) | 412 (69.2) | p < 0.001 | 1.44 (1.17–1.77) *** |
| Normal/high resilience (3.00–5.00) | 2327 (79.6) | 1033 (44.4) | 1294 (55.6) | Reference | |
| Attitudes towards medical profession | |||||
| Doctor is not a profession of high social status and reputation | |||||
| Strongly agree/agree | 1137 (38.9) | 309 (27.2) | 828 (72.8) | p < 0.001 | 2.26 (1.90–2.68) *** |
| Strongly disagree/disagree | 1785 (61.1) | 907 (50.8) | 878 (49.2) | Reference | |
| The contributions and sacrifices made by doctors far outweigh their incomes | |||||
| Strongly agree/agree | 2460 (84.2) | 951 (38.7) | 1509 (61.3) | p < 0.001 | 1.66 (1.29–2.13) |
| Strongly disagree/disagree | 462 (15.8) | 265 (57.4) | 197 (42.6) | Reference | |
| Doctors often experience long working hours with tremendous workload | |||||
| Strongly agree/agree | 2704 (92.5) | 1113 (41.2) | 1591 (58.8) | 0.086 | 0.83 (0.59–1.17) |
| Strongly disagree/disagree | 218 (7.5) | 103 (47.2) | 115 (52.8) | Reference | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, C.Z.; Lin, Y.; Alias, H.; Hu, Z.; Wong, L.P. Effect of the COVID-19 Pandemic on Medical Student Career Perceptions: Perspectives from Medical Students in China. Int. J. Environ. Res. Public Health 2021, 18, 5071. https://doi.org/10.3390/ijerph18105071
Cai CZ, Lin Y, Alias H, Hu Z, Wong LP. Effect of the COVID-19 Pandemic on Medical Student Career Perceptions: Perspectives from Medical Students in China. International Journal of Environmental Research and Public Health. 2021; 18(10):5071. https://doi.org/10.3390/ijerph18105071
Chicago/Turabian StyleCai, Carla Zi, Yulan Lin, Haridah Alias, Zhijian Hu, and Li Ping Wong. 2021. "Effect of the COVID-19 Pandemic on Medical Student Career Perceptions: Perspectives from Medical Students in China" International Journal of Environmental Research and Public Health 18, no. 10: 5071. https://doi.org/10.3390/ijerph18105071