
Psychosocial Correlates of Suicidal Behavior among Adolescents under Confinement Due to the COVID-19 Pandemic in Aguascalientes, Mexico: A Cross-Sectional Population Survey

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Population
2.2. Constructs and Measurements
2.2.1. Suicidal Behaviors Schedule
2.2.2. Questionnaire of Attachment Evaluation CAMIR-R
2.2.3. Problem-Oriented Screening Instrument for Teenagers (POSIT)
2.2.4. Center for Epidemiologic Studies of Depression Scale CESD-R
2.2.5. Beck Anxiety Inventory BAI
2.2.6. Beck’s Hopelessness Scale HS-UAA 18
2.2.7. Trait Meta-Mood Scale TMMS-24
2.2.8. Rosenberg Self-Esteem Scale
2.2.9. Sociodemographic Characteristics
2.3. Data Collection and Analysis Procedure
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Iob, E.; Steptoe, A.; Fancourt, D. Abuse, self-harm and suicidal ideation in the UK during the COVID-19 pandemic. Br. J. Psychiatry 2020, 217, 543–546. [Google Scholar] [CrossRef] [PubMed]
- John, A.; Okolie, C.; Eyles, E.; Webb, R.T.; Schmidt, L.; McGuiness, L.A.; Olorisade, B.K.; Arensman, E.; Hawton, K.; Kapur, N.; et al. The impact of the COVID-19 pandemic on self-harm and suicidal behaviour: A living systematic review. F1000Research 2020, 9, 1097. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Preventing Suicide: A Global Imperative. 2014. Available online: https://www.who.int/mental_health/suicide-prevention/world_report_2014/en/ (accessed on 16 March 2021).
- Franklin, J.C.; Ribeiro, J.D.; Fox, K.R.; Bentley, K.H.; Kleiman, E.M.; Huang, X.; Musacchio, K.M.; Jaroszewski, A.C.; Chang, B.P.; Nock, M.K. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychol. Bull. 2017, 143, 187–232. [Google Scholar] [CrossRef] [PubMed]
- Pollock, N.J. Place, the Built Environment, and Means Restriction in Suicide Prevention. Int. J. Environ. Res. Public Health 2019, 16, 4389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, A.; Pirkis, J.; Gunnell, D.; Appleby, L.; Morrissey, J. Trends in suicide during the covid-19 pandemic. BMJ 2020, 371, m4352. [Google Scholar] [CrossRef]
- Ivey-Stephenson, A.Z.; Demissie, Z.; Crosby, A.E.; Stone, D.M.; Gaylor, E.; Wilkins, N.; Lowry, R.; Brown, M. Suicidal Ideation and Behaviors Among High School Students—Youth Risk Behavior Survey, United States, 2019. MMWR Suppl. 2020, 69, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Rahman, M.; Islam, R.; Karim, M.; Hasan, M.; Jesmin, S.S. Suicidal behavior among school-going adolescents in Bangladesh: Findings of the global school-based student health survey. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 55, 1491–1502. [Google Scholar] [CrossRef]
- Soto-Sanz, V.; Piqueras, J.A.; García-Olcina, M.; Rivera-Riquelme, M.; Rodríguez-Marín, J.; Alonso, J. Relación Entre Conducta Suicida Y Síntomas Interiorizados En Niños Y Adolescentes. Psicol. Conduct. 2020, 28, 5–18. Available online: https://dialnet.unirioja.es/servlet/articulo?codigo=7376910 (accessed on 24 March 2021).
- Uddin, R.; Burton, N.W.; Maple, M.; Khan, S.R.; Khan, A. Suicidal ideation, suicide planning, and suicide attempts among adolescents in 59 low-income and middle-income countries: A population-based study. Lancet Child Adolesc. Health 2019, 3, 223–233. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Suicide in the World: Global Health Estimates. 2019. Available online: https://apps.who.int/iris/handle/10665/326948 (accessed on 25 March 2021).
- World Health Organization. SDG Target 3.4, Indicator 3.4.2 Suicide Mortality Rate. Available online: https://unstats.un.org/sdgs/metadata?Text=&Goal=3&Target=3.4 (accessed on 25 March 2021).
- Turecki, G.; Brent, D.A.; Gunnell, D.; O’Connor, R.C.; Oquendo, M.A.; Pirkis, J.; Stanley, B.H. Suicide and suicide risk. Nat. Rev. Dis. Prim. 2019, 5, 1–22. [Google Scholar] [CrossRef]
- Cha, C.B.; Franz, P.J.; Guzmán, E.M.; Glenn, C.R.; Kleiman, E.M.; Nock, M.K. Annual Research Review: Suicide among youth—epidemiology, (potential) etiology, and treatment. J. Child Psychol. Psychiatry 2017, 59, 460–482. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.B.; Munroe, S.; Gray, K.; Porta, G.; Douaihy, A.; Marsland, A.; Brent, D.; Melhem, N.M. The role of substance use, smoking, and inflammation in risk for suicidal behavior. J. Affect. Disord. 2019, 243, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Conejero, I.; Nobile, B.; Olié, E.; Courtet, P. How Does COVID-19 Affect the Neurobiology of Suicide? Curr. Psychiatry Rep. 2021, 23, 1–13. [Google Scholar] [CrossRef]
- Glenn, C.R.; Lanzillo, E.C.; Esposito, E.C.; Santee, A.C.; Nock, M.K.; Auerbach, R.P. Examining the Course of Suicidal and Nonsuicidal Self-Injurious Thoughts and Behaviors in Outpatient and Inpatient Adolescents. J. Abnorm. Child Psychol. 2017, 45, 971–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nock, M.K.; Green, J.G.; Hwang, I.; McLaughlin, K.A.; Sampson, N.A.; Zaslavsky, A.M.; Kessler, R.C. Prevalence, Correlates, and Treatment of Lifetime Suicidal Behavior Among Adolescents. JAMA Psychiatry 2013, 70, 300–310. [Google Scholar] [CrossRef] [Green Version]
- Miranda-Mendizabal, A.; Castellví, P.; Parés-Badell, O.; Alayo, I.; Almenara, J.; Alonso, I.; Blasco, M.J.; Cebrià, A.; Gabilondo, A.; Gili, M.; et al. Gender differences in suicidal behavior in adolescents and young adults: Systematic review and meta-analysis of longitudinal studies. Int. J. Public Health 2019, 64, 265–283. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Estadística y Geografía. Defunciones por Suicidio por Entidad Federativa de Residencia Habitual de la Persona Fallecida Según Sexo, 2010 a 2019. Available online: https://www.inegi.org.mx/app/tabulados/interactivos/?pxq=Mortalidad_Mortalidad_07_8627c147-473c-4c63-9967-56664e612f40 (accessed on 22 March 2021).
- Instituto Nacional de Estadística y Geografía. Estadísticas a Propósito del día Mundial Para la Prevención del Suicidio: Datos Nacionales. Comunicado de Prensa INEGI. Available online: https://www.inegi.org.mx/contenidos/saladeprensa/aproposito/2020/suicidios2020_Nal.pdf (accessed on 22 March 2021).
- Instituto Nacional de Estadística y Geografía. Estadísticas a Propósito del día Mundial de la Prevenció del Suicidio (10 DE SEPTIEMBRE): Datos Nacionales. Comunicado de Prensa 455/19. Available online: https://www.inegi.org.mx/contenidos/saladeprensa/aproposito/2019/suicidios2019_Nal.pdf (accessed on 23 March 2021).
- Reger, M.A.; Stanley, I.H.; Joiner, T.E. Suicide Mortality and Coronavirus Disease 2019—A Perfect Storm? JAMA Psychiatry 2020, 77, 1093–1094. [Google Scholar] [CrossRef] [Green Version]
- Hermosillo-De-La-Torre, A.E.; González-Forteza, C.; Rivera-Heredia, M.E.; Méndez-Sánchez, C.; González-Betanzos, F.; Palacios-Salas, P.; Jiménez, A.; Wagner, F.A. Understanding suicidal behavior and its prevention among youth and young adults in Mexico. Prev. Med. 2020, 138, 106177. [Google Scholar] [CrossRef]
- The World Medical Association. WMA Declaration of Helsinki-Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 22 March 2021).
- González-Forteza, C.; Juárez-López, C.E.; Jiménez, A.; Montejo-León, L.; Rodríguez-Santisbón, U.R.; Wagner, F.A. Suicide behavior and associated psychosocial factors among adolescents in Campeche, Mexico. Prev. Med. 2017, 105, 206–211. [Google Scholar] [CrossRef]
- González-Forteza, C.; Ramos, L.L.; Caballero, M.Á.G.; Wagner, F.A.E. Correlatos psicosociales de depresión, ideación e intento suicida en adolescentes mexicanos. Psicothema 2003, 15, 524–532. Available online: https://reunido.uniovi.es/index.php/PST/article/view/8053 (accessed on 23 March 2021).
- Gonzalez-Forteza, C.; Alvarez-Ruiz, M.; Saldaña-Hernández, A.; Carreño-García, S.; Chávez-Hernández, A.-M.; Pérez-Hernández, R. PREVALENCE OF DELIBERATE SELF-HARM IN TEENAGE STUDENTS IN THE STATE OF GUANAJUATO, MEXICO: 2003. Soc. Behav. Pers. Int. J. 2005, 33, 777–792. [Google Scholar] [CrossRef] [Green Version]
- Díez-Gómez, A.; Pérez-Albéniz, A.; Sebastián-Enesco, C.; Fonseca-Pedrero, E. Suicidal Behavior in Adolescents: A Latent Class Analysis. Int. J. Environ. Res. Public Health 2020, 17, 2820. [Google Scholar] [CrossRef] [PubMed]
- Arenas-Monreal, L.; Hidalgo-Solórzano, E.; Chong-Escudero, X.; la Cruz, J.A.D.; González-Cruz, N.L.; Pérez-Matus, S.; Valdez-Santiago, R. Suicidal behaviour in adolescents: Educational interventions in Mexico. Health Soc. Care Community 2021, 2021, 1–8. [Google Scholar] [CrossRef]
- Balluerka, N.; Lacasa, F.; Gorostiaga, A.; Muela, A.; Pierrehumbert, B. Versión reducida del cuestionario CaMir (CaMir-R) para la evaluación del apego. Psicothema 2011, 23, 486–494. Available online: http://diposit.ub.edu/dspace/handle/2445/124587 (accessed on 15 March 2021). [PubMed]
- Pierrehumbert, B.; Karmaniola, A.; Sieye, A.; Meister, C.; Miljkovitch, R.; Halfon, O. Les modèles de relations: Développement d’un autoquestionnaire d’attachement pour adultes. Psychiatr. l’Enfant 1996, 39, 161–206. [Google Scholar]
- Main, M. Epilogue. Attachment theory: Eighteen points with suggestions for future studies. In Handbook of Attachment: Theory, Research, and Clinical Applications; Cassidy, J., Shaver, P.R., Eds.; Guilford P: New York, NY, USA, 1999; pp. 845–887. [Google Scholar]
- Lacasa, F.; Muela, A. Guía para la aplicación e interpretación del cuestionario de apego CaMir-R. Rev. Psicopatol. Salud Ment. Niño Adolesc. 2014, 24, 83–93. [Google Scholar] [CrossRef]
- Mariño, M.D.C.; González-Forteza, C.; Andrade, P.; Medina-Mora, M.E. Validación de un cuestionario para detectar adolescentes con problemas por el uso de drogas. Salud Ment. 1998, 21, 27–36. Available online: http://repositorio.inprf.gob.mx/handle/123456789/5707 (accessed on 25 March 2021).
- Eaton, W.W.; Smith, C.; Ybarra, M.; Muntaner, C.; Tien, A. Center for Epidemiologic Studies Depression Scale: Review and Revision (CESD and CESD-R). In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment: Instruments for Adults, 3rd ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2004; Volume 3, pp. 363–377. [Google Scholar]
- González-Forteza, C.; Jiménez-Tapia, J.A.; Ramos-Lira, L.; Wagner, F.A. Aplicación de la Escala de Depresión del Center of Epidemiological Studies en adolescentes de la Ciudad de México. Salud Pública México 2008, 50, 292–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robles, R.; Varela, R.; Jurado, S.; Páez, F. The Mexican version of Beck Anxiety Inventory: Psychometric properties. Rev. Mex. Psicol. 2001, 18, 211–218. Available online: https://www.researchgate.net/publication/283150414_The_Mexican_version_of_Beck_Anxiety_Inventory_Psychometric_properties (accessed on 15 March 2021).
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef] [PubMed]
- La Torre, A.E.H.-D.; Méndez-Sánchez, C.; Gonzalez-Betanzos, F. Evidencias de validez factorial de la Escala de desesperanza de Beck en español con muestras clínicas y no clínicas. Acta Colomb. Psicol. 2020, 23, 148–169. [Google Scholar] [CrossRef]
- Beck, A.T.; Weissman, A.; Lester, D.; Trexler, L. The measurement of pessimism: The Hopelessness Scale. J. Consult. Clin. Psychol. 1974, 42, 861–865. [Google Scholar] [CrossRef]
- Fernandez-Berrocal, P.; Extremera, N.; Ramos, N. Validity and Reliability of the Spanish Modified Version of the Trait Meta-Mood Scale. Psychol. Rep. 2004, 94, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Salovey, P.; Mayer, J.D.; Goldman, S.L.; Turvey, C.; Palfai, T.P. Emotional attention, clarity and repair: Exploring emotional intelligence using the Trait Meta-Mood Scale. In Emotion, Disclosure and Health; Pennebaker, J.W., Ed.; American Psychological Association: Washington, DC, USA, 1995; pp. 125–154. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Jiménez Tapia, A.; Mondragón Barrios, L.; González-Forteza, C. Self-esteem, depressive symptomatology, and suicidal ideation in adolescents: Results of three studies. Salud Ment. 2007, 30, 20–26. Available online: https://www.medigraphic.com/pdfs/salmen/sam-2007/sam075d.pdf (accessed on 23 March 2021).
- Sánchez-Teruel, D.; Robles-Bello, M.A.; Camacho-Conde, J.A. Self-inflicted injuries in adolescents and young adults: A longitudinal approach. Psicothema 2020, 32, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Carroll, R.; Metcalfe, C.; Gunnell, D. Hospital Presenting Self-Harm and Risk of Fatal and Non-Fatal Repetition: Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e89944. [Google Scholar] [CrossRef] [PubMed]
- Benjet, C.; Borges, G.; Medina-Mora, M.E.; Zambrano, J.; Aguilar-Gaxiola, S. Youth mental health in a populous city of the developing world: Results from the Mexican Adolescent Mental Health Survey. J. Child Psychol. Psychiatry 2009, 50, 386–395. [Google Scholar] [CrossRef]
- Gili, M.; Castellví, P.; Vives, M.; de la Torre-Luque, A.; Almenara, J.; Blasco, M.J.; Cebrià, A.I.; Gabilondo, A.; Pérez-Ara, M.A.; Miranda-Mendizábal, A.; et al. Mental disorders as risk factors for suicidal behavior in young people: A meta-analysis and systematic review of longitudinal studies. J. Affect. Disord. 2019, 245, 152–162. [Google Scholar] [CrossRef]
- Rodríguez, S.P.; Salvador, J.H.M.; García-Alandete, J. The role of hopelessness and meaning in life in a clinical sample with non-suicidal self-injury and suicide attempts. Psicothema 2017, 29, 323–328. [Google Scholar]
- Wolfe, K.L.; Nakonezny, P.A.; Owen, V.J.; Rial, K.V.; Bs, A.P.M.; Kennard, B.D.; Emslie, G.J. Hopelessness as a Predictor of Suicide Ideation in Depressed Male and Female Adolescent Youth. Suicide Life-Threat. Behav. 2019, 49, 253–263. [Google Scholar] [CrossRef]
- De La Vega, D.; Giner, L.; Courtet, P. Suicidality in Subjects With Anxiety or Obsessive-Compulsive and Related Disorders: Recent Advances. Curr. Psychiatry Rep. 2018, 20, 26. [Google Scholar] [CrossRef]
- Herres, J.; Shearer, A.; Kodish, T.; Kim, B.; Wang, S.B.; Diamond, G.S. Differences in Suicide Risk Severity Among Suicidal Youth With Anxiety Disorders. Crisis 2019, 40, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Borges, G.; Benjet, C.; Orozco, R.; Medina-Mora, M.-E.; Menendez, D. Alcohol, cannabis and other drugs and subsequent suicide ideation and attempt among young Mexicans. J. Psychiatr. Res. 2017, 91, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Burlaka, V. Gender Differences in Suicidal Behaviors: Mediation Role of Psychological Distress between Alcohol Abuse/Dependence and Suicidal Behaviors. Arch. Suicide Res. 2017, 22, 405–419. [Google Scholar] [CrossRef]
- Poorolajal, J.; Darvishi, N. Smoking and Suicide: A Meta-Analysis. PLoS ONE 2016, 11, e0156348. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.; Koyanagi, A.; Rehm, J.; Roerecke, M.; Carvalho, A.F. Association of Tobacco Use and Exposure to Secondhand Smoke With Suicide Attempts Among Adolescents: Findings From 33 Countries. Nicotine Tob. Res. 2019, 22, 1322–1329. [Google Scholar] [CrossRef] [PubMed]
- Orri, M.; Galera, C.; Turecki, G.; Forte, A.; Renaud, J.; Boivin, M.; Tremblay, R.E.; Côté, S.M.; Geoffroy, M.-C. Association of Childhood Irritability and Depressive/Anxious Mood Profiles with Adolescent Suicidal Ideation and Attempts. JAMA Psychiatry 2018, 75, 465–473. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Psiquiatría de la Fuente Muñiz, Instituto Nacional de Salud Pública, Comisión Nacional Contra las Adicciones, Secretaría de Salud. Encuesta Nacional de Consumo de Drogas, Alcohol y Tabaco 2016–2017: Reporte de Alcohol; Villatoro Velázquez, J.A., Medina-Mora Icaza, M.E., Hernández Ávila, M., Eds.; INPRFM: Ciudad de México, Mexico, 2017; Available online: https://www.gob.mx/salud%7Cconadic/acciones-y-programas/encuesta-nacional-de-consumo-de-drogas-alcohol-y-tabaco-encodat-2016-2017-136758 (accessed on 23 March 2021).
- Soto-Sanz, V.; Piqueras, J.A.; Rodríguez-Marín, J.; Pérez-Vázquez, M.; Rodríguez-Jiménez, T.; Castellví, P.; Miranda-Mendizábal, A.; Parés-Badell, O.; Almenara, J.; Blanco, M.J.; et al. Self-esteem and suicidal behaviour in youth: A meta-analysis of longitudinal studies. Psicothema 2019, 31, 246–254. [Google Scholar]
- Johnson, J.G.; Cohen, P.; Gould, M.S.; Kasen, S.; Brown, J.; Brook, J.S. Childhood Adversities, Interpersonal Difficulties, and Risk for Suicide Attempts During Late Adolescence and Early Adulthood. Arch. Gen. Psychiatry 2002, 59, 741–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, A.; Gorodetsky, E.; Yuan, Q.; Goldman, D.; Enoch, M.-A. Interaction of FKBP5, a Stress-Related Gene, with Childhood Trauma Increases the Risk for Attempting Suicide. Neuropsychopharmacology 2010, 35, 1674–1683. [Google Scholar] [CrossRef] [Green Version]
- Van Der Vegt, E.J.M.; Van Der Ende, J.; Ferdinand, R.F.; Verhulst, F.C.; Tiemeier, H. Early Childhood Adversities and Trajectories of Psychiatric Problems in Adoptees: Evidence for Long Lasting Effects. J. Abnorm. Child Psychol. 2008, 37, 239–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nock, M.K.; Hwang, I.; Sampson, N.; Kessler, R.C.; Angermeyer, M.; Beautrais, A.; Borges, G.; Bromet, E.; Bruffaerts, R.; De Girolamo, G.; et al. Cross-National Analysis of the Associations among Mental Disorders and Suicidal Behavior: Findings from the WHO World Mental Health Surveys. PLoS Med. 2009, 6, e1000123. [Google Scholar] [CrossRef] [Green Version]
- Arsenault-Lapierre, G.; Kim, C.; Turecki, G. Psychiatric diagnoses in 3275 suicides: A meta-analysis. BMC Psychiatry 2004, 4, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumais, A.; Lesage, A.; Alda, M.; Rouleau, G.; Dumont, M.; Chawky, N.; Roy, M.; Mann, J.; Benkelfat, C.; Turecki, G. Risk Factors for Suicide Completion in Major Depression: A Case-Control Study of Impulsive and Aggressive Behaviors in Men. Am. J. Psychiatry 2005, 162, 2116–2124. [Google Scholar] [CrossRef] [PubMed]
- Séguin, M.; Lesage, A.; Turecki, G.; Bouchard, M.; Chawky, N.; Tremblay, N.; Daigle, F.; Guy, A. Life trajectories and burden of adversity: Mapping the developmental profiles of suicide mortality. Psychol. Med. 2007, 37, 1575–1583. [Google Scholar] [CrossRef]
- Artenie, A.A.; Bruneau, J.; Roy, É.; Zang, G.; Lespérance, F.; Renaud, J.; Tremblay, J.; Jutras-Aswad, D. Licit and illicit substance use among people who inject drugs and the association with subsequent suicidal attempt. Addiction 2015, 110, 1636–1643. [Google Scholar] [CrossRef] [Green Version]
- Li, C.-Q.; Zhang, J.-S.; Ma, S.; Lv, R.-R.; Duan, J.-L.; Luo, D.-M.; Yan, X.-J.; Ma, N.; Song, Y. Gender differences in self-harm and drinking behaviors among high school students in Beijing, China. BMC Public Health 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Vijayakumar, L. Suicide in women. Indian J. Psychiatry 2015, 57, 233–238. [Google Scholar] [CrossRef]
- Goldsmith, S.K.; Pellmar, T.C.; Kleinman, A.M.; Bunney, W.E. (Eds.) Reducing Suicide: A National Imperative; National Academies Press: Washington, DC, USA, 2002; Available online: http://www.nap.edu/catalog/10398.html (accessed on 18 March 2021).
- Restrepo, D.M.; Chesin, M.S.; Jeglic, E.L. The Relationship between Social Maladjustment, Childhood Abuse and Suicidal Behavior in College Students. Int. J. Psychol. Psychol. Ther. 2016, 16, 235–248. Available online: https://www.redalyc.org/pdf/560/56049049002.pdf (accessed on 23 March 2021).
- Sheftall, A.H.; Asti, L.; Horowitz, L.M.; Felts, A.; Fontanella, C.A.; Campo, J.V.; Bridge, J.A. Suicide in Elementary School-Aged Children and Early Adolescents. Pediatrics 2016, 138, e20160436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassels, M.; Baetens, I.; Wilkinson, P.; Hoppenbrouwers, K.; Wiersema, J.R.; Van Leeuwen, K.; Kiekens, G. Attachment and Non-Suicidal Self-Injury among Young Adolescents: The Indirect Role of Behavioral Problems. Arch. Suicide Res. 2019, 23, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Davaji, R.B.O.; Valizadeh, S.; Nikamal, M. The relationship between attachment styles and suicide ideation: The study of Turkmen students, Iran. Procedia Soc. Behav. Sci. 2010, 5, 1190–1194. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Total | Sample % | No Suicidal Behavior (n = 6390, 79.5%) | Self-Injuries (n = 454, 5.7%) | Low-Lethality Suicide Attempt (n = 897, 11.2%) | High-Lethality Suicide Attempt (n = 292, 3.6%) | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | wt % ** | n | wt % ** | n | wt % ** | n | wt % ** | |||
| Sex | Design-based F(2.85, 176.69) = 108.0410 p < 0.001 | |||||||||
| Male | 3910 | 48.7 | 3401 | 87.0 | 146 | 3.7 | 250 | 6.4 | 113 | 2.9 |
| Female | 4123 | 51.3 | 2989 | 72.5 | 308 | 7.5 | 647 | 15.7 | 179 | 4.3 |
| High-School Grade | Design-based F(5.32, 329.93) = 1.0650 p = 0.3810 | |||||||||
| 9th | 3029 | 37.7 | 2380 | 78.6 | 191 | 6.3 | 349 | 11.5 | 109 | 3.6 |
| 10th | 2805 | 34.9 | 2238 | 79.8 | 154 | 5.5 | 302 | 10.8 | 111 | 4.0 |
| 11th | 2199 | 27.4 | 1772 | 80.6 | 109 | 5.0 | 246 | 11.2 | 72 | 3.3 |
| Depression | Design-based F(2.70, 167.55) = 305.7240 p < 0.001 | |||||||||
| No | 6938 | 86.4 | 5910 | 85.2 | 327 | 4.7 | 539 | 7.8 | 162 | 2.3 |
| Yes | 1095 | 13.6 | 480 | 43.8 | 127 | 11.6 | 358 | 32.7 | 130 | 11.9 |
| Hopelessness | Design-based F(2.71, 167.88) = 87.7198 p < 0.001 | |||||||||
| No | 6919 | 86.1 | 5748 | 83.1 | 324 | 4.7 | 649 | 9.4 | 198 | 2.9 |
| Yes | 1114 | 13.9 | 642 | 57.6 | 130 | 11.7 | 248 | 22.3 | 94 | 8.4 |
| Anxiety (BAI) | Design-based F(6.80, 421.36) = 90.7285 p < 0.001 | |||||||||
| Minimal | 3682 | 45.8 | 3335 | 90.6 | 118 | 3.2 | 155 | 4.2 | 74 | 2.0 |
| Mild | 2314 | 28.8 | 1813 | 78.4 | 152 | 6.6 | 280 | 12.1 | 69 | 3.0 |
| Moderate | 1615 | 20.1 | 1039 | 64.3 | 138 | 8.5 | 340 | 21.1 | 98 | 6.1 |
| Severe | 422 | 5.3 | 203 | 48.1 | 46 | 10.9 | 122 | 28.9 | 51 | 12.1 |
| Past Month Use | ||||||||||
| Marijuana | Design-based F(2.40, 149.05) = 30.0118 p < 0.001 | |||||||||
| No | 7321 | 91.1 | 5926 | 81.0 | 395 | 5.4 | 761 | 10.4 | 239 | 3.3 |
| Yes | 712 | 8.9 | 464 | 65.2 | 59 | 8.3 | 136 | 19.1 | 53 | 7.4 |
| Inhalants | Design-based F(2.23, 138.04) = 8.4606 p < 0.001 | |||||||||
| No | 7639 | 95.1 | 6110 | 80.0 | 420 | 5.5 | 843 | 11.0 | 266 | 3.5 |
| Yes | 394 | 4.9 | 280 | 71.1 | 34 | 8.6 | 54 | 13.7 | 26 | 6.6 |
| Cocaine | Design-based F(2.61, 161.92) = 10.7100 p < 0.001 | |||||||||
| No | 7634 | 95.0 | 6106 | 80.0 | 425 | 5.6 | 844 | 11.1 | 259 | 3.4 |
| Yes | 399 | 5.0 | 284 | 71.2 | 29 | 7.3 | 53 | 13.3 | 33 | 8.3 |
| Methamphetamines | Design-based F(2.63, 163.20) = 7.3596 p < 0.001 | |||||||||
| No | 7685 | 95.7 | 6135 | 79.8 | 430 | 5.6 | 853 | 11.1 | 267 | 3.5 |
| Yes | 348 | 4.3 | 255 | 73.3 | 24 | 6.9 | 44 | 12.6 | 25 | 7.2 |
| Alcohol | Design-based F(2.48, 153.64) = 64.1876 p < 0.001 | |||||||||
| No | 4249 | 52.9 | 3632 | 85.5 | 190 | 4.5 | 333 | 7.8 | 94 | 2.2 |
| Yes | 3784 | 47.1 | 2758 | 72.9 | 264 | 7.0 | 564 | 14.9 | 198 | 5.2 |
| Tobacco | Design-based F(2.54, 157.18) = 90.9564 p < 0.001 | |||||||||
| No | 6502 | 80.9 | 5412 | 83.2 | 322 | 5.0 | 590 | 9.1 | 178 | 2.7 |
| Yes | 1531 | 19.1 | 978 | 63.9 | 132 | 8.6 | 307 | 20.1 | 114 | 7.5 |
| Emotional Intelligence | ||||||||||
| Emotional attention | Design-based F(4.84, 300.14) = 2.1194 p = 0.065 | |||||||||
| Adequate | 3013 | 37.5 | 2444 | 81.1 | 139 | 4.6 | 330 | 11.0 | 100 | 3.3 |
| Too little | 3864 | 48.1 | 3056 | 79.1 | 233 | 6.0 | 436 | 11.3 | 139 | 3.6 |
| Too much | 1156 | 14.4 | 890 | 77.0 | 82 | 7.1 | 131 | 11.3 | 53 | 4.6 |
| Emotional clarity | Design-based F(4.33, 268.15) = 16.3275 p < 0.001 | |||||||||
| Adequate | 2380 | 29.6 | 1989 | 83.6 | 103 | 4.3 | 220 | 9.2 | 68 | 2.9 |
| Too little | 4471 | 55.7 | 3388 | 75.8 | 292 | 6.5 | 609 | 13.6 | 182 | 4.1 |
| Too much | 1182 | 14.7 | 1013 | 85.7 | 59 | 5.0 | 68 | 5.8 | 42 | 3.6 |
| Emotional repair | Design-based F(4.91, 304.19) = 36.8942 p < 0.001 | |||||||||
| Adequate | 3124 | 38.9 | 2608 | 83.5 | 154 | 4.9 | 288 | 9.2 | 74 | 2.4 |
| Too little | 3286 | 40.9 | 2372 | 72.2 | 244 | 7.4 | 498 | 15.2 | 172 | 5.2 |
| Too much | 1623 | 20.2 | 1410 | 86.9 | 56 | 3.5 | 111 | 6.8 | 46 | 2.8 |
| Variable | Total | Mean | Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | Mean | 95% CI |
| Attachment * | ||||||||||
| Security | 8033 | 4.9 | 4.9 | 4.9, 5.0 | 4.4 | 4.3, 4.5 | 4.4 | 4.3, 4.4 | 4.3 | 4.0, 4.3 |
| Family preoccupation | 8033 | 4.2 | 4.2 | 4.2, 4.3 | 4.2 | 4.1, 4.3 | 4.3 | 4.3, 4.4 | 4.2 | 4.0, 4.3 |
| Parental interference | 8033 | 4.1 | 4.1 | 4.1, 4.1 | 4.2 | 4.1, 4.3 | 4.3 | 4.2, 4.4 | 4.2 | 4.1, 4.3 |
| Parental authority | 8033 | 5.1 | 5.2 | 5.1, 5.2 | 4.9 | 4.8, 5.0 | 5.0 | 4.9, 5.0 | 4.8 | 4.7, 4.9 |
| Parental permissiveness | 8033 | 3.4 | 3.4 | 3.4, 3.4 | 3.5 | 3.4, 3.6 | 3.5 | 3.4, 3.5 | 3.5 | 3.3, 3.6 |
| Resentment | 8033 | 3.9 | 3.8 | 3.8, 3.8 | 4.2 | 4.1, 4.3 | 4.3 | 4.3, 4.4 | 4.1 | 5.0, 4.3 |
| Childhood trauma | 8033 | 3.3 | 3.2 | 3.1, 3.2 | 3.7 | 3.6, 3.8 | 3.8 | 3.7, 3.8 | 3.7 | 3.6, 3.8 |
| POSIT * | ||||||||||
| Drugs | 8033 | 0.7 | 0.4 | 0.5, 0.5 | 1.2 | 1.0, 1.4 | 1.6 | 1.4, 1.7 | 2.0 | 1.7, 2.4 |
| Mental health | 8033 | 5.2 | 4.4 | 4.3, 4.5 | 7.8 | 7.4, 8.3 | 8.9 | 8.7, 9.2 | 8.5 | 7.9, 9.2 |
| Low self-esteem * | 8033 | 22.2 | 21.6 | 21.4, 21.7 | 24.3 | 23.9, 24.8 | 24.9 | 24.3, 25.7 | 25.0 | 24.4, 25.7 |
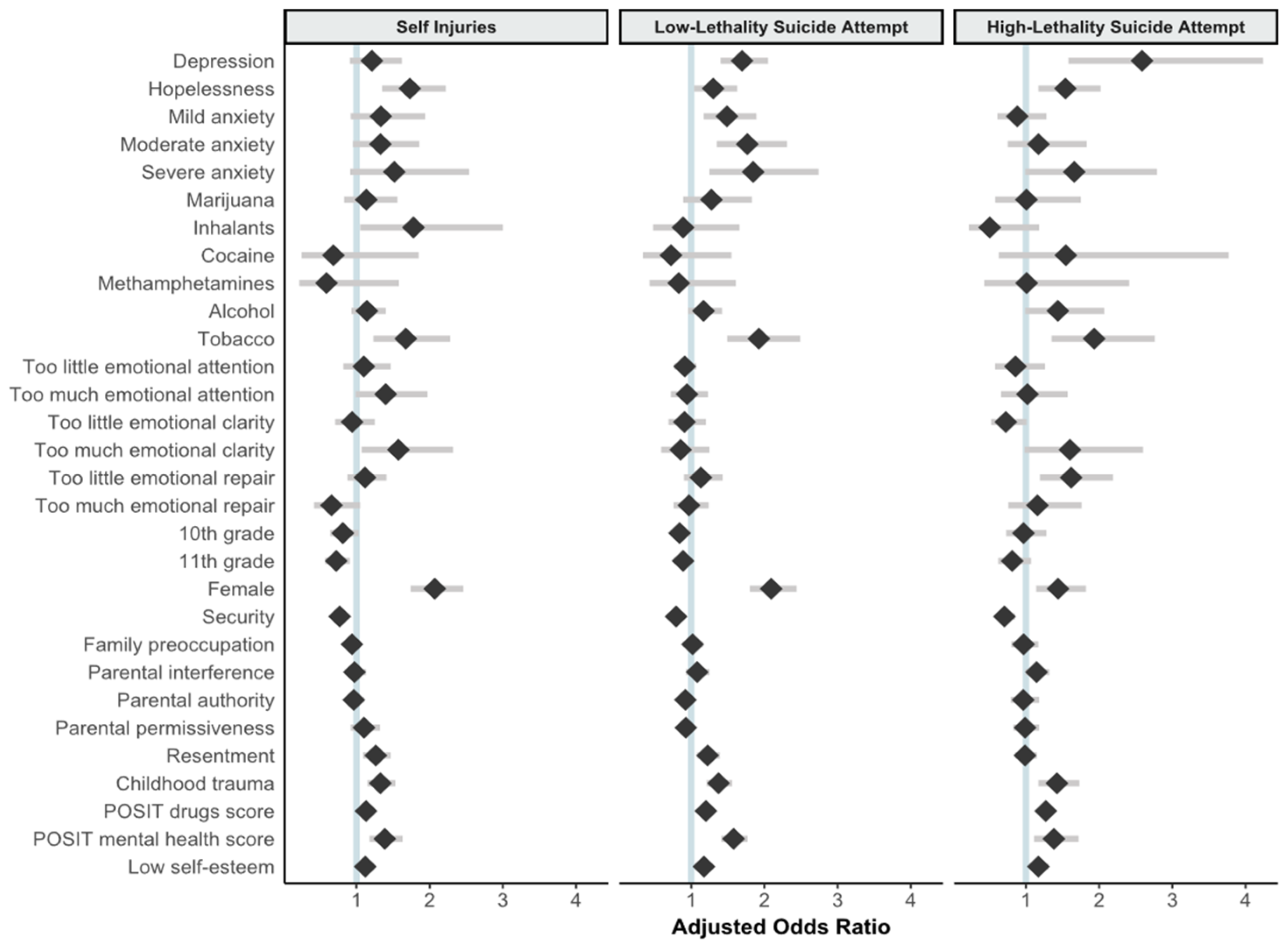
| Variable | Self-Injuries | Low-Lethality Suicide Attempt | High-Lethality Suicide Attempt | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | aOR | p | 95% CI | OR | aOR | p | 95% CI | OR | aOR | p | 95% CI | ||||
| ll | uL | ll | uL | ll | uL | ||||||||||
| Depression | |||||||||||||||
| No | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | |||||||
| Yes | 4.78 | 1.21 | 0.193 | 0.91 | 1.62 | 8.17 | 1.69 | <0.001 | 1.40 | 2.05 | 9.88 | 2.59 | <0.001 | 1.58 | 4.24 |
| Hopelessness | |||||||||||||||
| No | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | ||||||
| Yes | 3.59 | 1.73 | <0.001 | 1.35 | 2.22 | 3.42 | 1.30 | 0.024 | 1.04 | 1.63 | 4.25 | 1.54 | 0.002 | 1.17 | 2.02 |
| Anxiety (BAI) | |||||||||||||||
| Minimal | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | ||||||
| Mild | 2.37 | 1.33 | 0.129 | 0.92 | 1.94 | 3.32 | 1.49 | 0.001 | 1.17 | 1.89 | 1.72 | 0.88 | 0.503 | 0.61 | 1.28 |
| Moderate | 3.75 | 1.33 | 0.096 | 0.95 | 1.86 | 7.04 | 1.77 | <0.001 | 1.35 | 2.31 | 4.25 | 1.17 | 0.478 | 0.75 | 1.83 |
| Severe | 6.40 | 1.52 | 0.111 | 0.91 | 2.54 | 12.93 | 1.85 | 0.003 | 1.25 | 2.74 | 11.32 | 1.66 | 0.056 | 0.99 | 2.79 |
| Past Month Use | |||||||||||||||
| Marijuana | |||||||||||||||
| No | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | ||||||
| Yes | 1.91 | 1.14 | 0.427 | 0.83 | 1.56 | 2.28 | 1.28 | 0.179 | 0.89 | 1.83 | 2.83 | 1.01 | 0.981 | 0.58 | 1.75 |
| Inhalants | |||||||||||||||
| No | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | ||||||
| Yes | 1.77 | 1.78 | 0.032 | 1.05 | 3.00 | 1.4 | 0.89 | 0.708 | 0.48 | 1.66 | 2.13 | 0.51 | 0.114 | 0.22 | 1.18 |
| Cocaine | |||||||||||||||
| No | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | ||||||
| Yes | 1.47 | 0.68 | 0.449 | 0.25 | 1.85 | 1.35 | 0.72 | 0.400 | 0.34 | 1.55 | 2.74 | 1.55 | 0.334 | 0.63 | 3.77 |
| Methamphetamines | |||||||||||||||
| No | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | 1.00 | 1.00 | (referent) | |||||||
| Yes | 1.34 | 0.59 | 0.291 | 0.22 | 1.58 | 1.24 | 0.83 | 0.570 | 0.43 | 1.61 | 2.25 | 1.01 | 0.977 | 0.43 | 2.41 |
| Alcohol | |||||||||||||||
| No | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | ||||||
| Yes | 1.83 | 1.14 | 0.192 | 0.93 | 1.40 | 2.23 | 1.17 | 0.121 | 0.96 | 1.42 | 2.77 | 1.44 | 0.053 | 0.99 | 2.07 |
| Tobacco | |||||||||||||||
| No | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | ||||||
| Yes | 2.27 | 1.67 | 0.001 | 1.23 | 2.28 | 2.88 | 1.92 | < 0.001 | 1.49 | 2.49 | 3.54 | 1.93 | < 0.001 | 1.35 | 2.76 |
| Emotional intelligence | |||||||||||||||
| Emotional attention | |||||||||||||||
| Adequate | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | ||||||
| Too little | 1.34 | 1.10 | 0.509 | 0.82 | 1.47 | 1.06 | 0.91 | 0.265 | 0.77 | 1.07 | 1.11 | 0.86 | 0.424 | 0.58 | 1.26 |
| Too much | 1.62 | 1.40 | 0.053 | 0.99 | 1.97 | 1.09 | 0.94 | 0.656 | 0.72 | 1.23 | 1.46 | 1.02 | 0.925 | 0.66 | 1.57 |
| Emotional clarity | |||||||||||||||
| Adequate | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | ||||||
| Too little | 1.66 | 0.94 | 0.666 | 0.71 | 1.25 | 1.63 | 0.91 | 0.487 | 0.69 | 1.20 | 1.57 | 0.73 | 0.059 | 0.52 | 1.01 |
| Too much | 1.12 | 1.57 | 0.023 | 1.07 | 2.32 | 0.61 | 0.86 | 0.410 | 0.59 | 1.25 | 1.21 | 1.60 | 0.058 | 0.98 | 2.60 |
| Emotional repair | |||||||||||||||
| Adequate | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | ||||||
| Too little | 1.74 | 1.12 | 0.355 | 0.88 | 1.41 | 1.90 | 1.13 | 0.288 | 0.90 | 1.43 | 2.56 | 1.62 | 0.002 | 1.19 | 2.19 |
| Too much | 0.67 | 0.66 | 0.076 | 0.42 | 1.05 | 0.71 | 0.97 | 0.799 | 0.76 | 1.24 | 1.15 | 1.16 | 0.491 | 0.76 | 1.76 |
| High-School Grade | |||||||||||||||
| 9th | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | ||||||
| 10th | 0.86 | 0.81 | 0.080 | 0.64 | 1.03 | 0.92 | 0.84 | 0.043 | 0.71 | 0.99 | 1.08 | 0.97 | 0.813 | 0.73 | 1.28 |
| 11th | 0.77 | 0.72 | 0.007 | 0.57 | 0.91 | 0.95 | 0.89 | 0.101 | 0.77 | 1.02 | 0.89 | 0.81 | 0.134 | 0.62 | 1.07 |
| Sex | |||||||||||||||
| Male | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | 1.00 | 1.00 | (referent) | ||||||
| Female | 2.40 | 2.07 | <0.001 | 1.74 | 2.46 | 2.94 | 2.09 | <0.001 | 1.80 | 2.44 | 1.80 | 1.44 | 0.003 | 1.14 | 1.82 |
| Attachment * | |||||||||||||||
| Security | 0.62 | 0.77 | 0.001 | 0.66 | 0.90 | 0.61 | 0.79 | <0.001 | 0.71 | 0.89 | 0.55 | 0.71 | <0.001 | 0.59 | 0.85 |
| Family preoccupation | 1.00 | 0.94 | 0.276 | 0.84 | 1.05 | 1.16 | 1.02 | 0.770 | 0.89 | 1.16 | 0.94 | 0.97 | 0.726 | 0.80 | 1.17 |
| Parental interference | 1.15 | 0.97 | 0.710 | 0.84 | 1.13 | 1.32 | 1.08 | 0.287 | 0.93 | 1.25 | 1.14 | 1.15 | 0.066 | 0.99 | 1.32 |
| Parental authority | 0.80 | 0.96 | 0.579 | 0.84 | 1.10 | 0.83 | 0.92 | 0.184 | 0.82 | 1.04 | 0.73 | 0.96 | 0.712 | 0.79 | 1.18 |
| Parental permissiveness | 1.22 | 1.10 | 0.277 | 0.92 | 1.32 | 1.1 | 0.93 | 0.165 | 0.83 | 1.03 | 1.09 | 0.99 | 0.891 | 0.83 | 1.18 |
| Resentment | 1.79 | 1.26 | 0.003 | 1.09 | 1.47 | 2.04 | 1.22 | 0.003 | 1.08 | 1.39 | 1.59 | 0.99 | 0.868 | 0.85 | 1.15 |
| Childhood trauma | 1.93 | 1.33 | <0.001 | 1.15 | 1.53 | 2.12 | 1.37 | <0.001 | 1.21 | 1.56 | 2.02 | 1.42 | 0.001 | 1.17 | 1.73 |
| POSIT * | |||||||||||||||
| Drugs | 1.44 | 1.13 | 0.010 | 1.03 | 1.24 | 1.56 | 1.20 | <0.001 | 1.13 | 1.28 | 1.69 | 1.27 | <0.001 | 1.18 | 1.37 |
| Mental health | 2.34 | 1.39 | <0.001 | 1.18 | 1.63 | 3.06 | 1.58 | <0.001 | 1.41 | 1.77 | 2.77 | 1.38 | 0.004 | 1.11 | 1.72 |
| Low self-esteem * | 1.56 | 1.12 | 0.018 | 1.02 | 1.23 | 1.7 | 1.17 | 0.002 | 1.06 | 1.30 | 1.72 | 1.17 | 0.006 | 1.05 | 1.31 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hermosillo-de-la-Torre, A.E.; Arteaga-de-Luna, S.M.; Acevedo-Rojas, D.L.; Juárez-Loya, A.; Jiménez-Tapia, J.A.; Pedroza-Cabrera, F.J.; González-Forteza, C.; Cano, M.; Wagner, F.A. Psychosocial Correlates of Suicidal Behavior among Adolescents under Confinement Due to the COVID-19 Pandemic in Aguascalientes, Mexico: A Cross-Sectional Population Survey. Int. J. Environ. Res. Public Health 2021, 18, 4977. https://doi.org/10.3390/ijerph18094977
Hermosillo-de-la-Torre AE, Arteaga-de-Luna SM, Acevedo-Rojas DL, Juárez-Loya A, Jiménez-Tapia JA, Pedroza-Cabrera FJ, González-Forteza C, Cano M, Wagner FA. Psychosocial Correlates of Suicidal Behavior among Adolescents under Confinement Due to the COVID-19 Pandemic in Aguascalientes, Mexico: A Cross-Sectional Population Survey. International Journal of Environmental Research and Public Health. 2021; 18(9):4977. https://doi.org/10.3390/ijerph18094977
Chicago/Turabian StyleHermosillo-de-la-Torre, Alicia Edith, Stephania Montserrat Arteaga-de-Luna, Denise Liliana Acevedo-Rojas, Angélica Juárez-Loya, José Alberto Jiménez-Tapia, Francisco Javier Pedroza-Cabrera, Catalina González-Forteza, Manuel Cano, and Fernando A. Wagner. 2021. "Psychosocial Correlates of Suicidal Behavior among Adolescents under Confinement Due to the COVID-19 Pandemic in Aguascalientes, Mexico: A Cross-Sectional Population Survey" International Journal of Environmental Research and Public Health 18, no. 9: 4977. https://doi.org/10.3390/ijerph18094977