
A Systematic Review on the Efficacy of Vaporized Hydrogen Peroxide as a Non-Contact Decontamination System for Pathogens Associated with the Dental Environment



Abstract
:1. Introduction
2. Objective
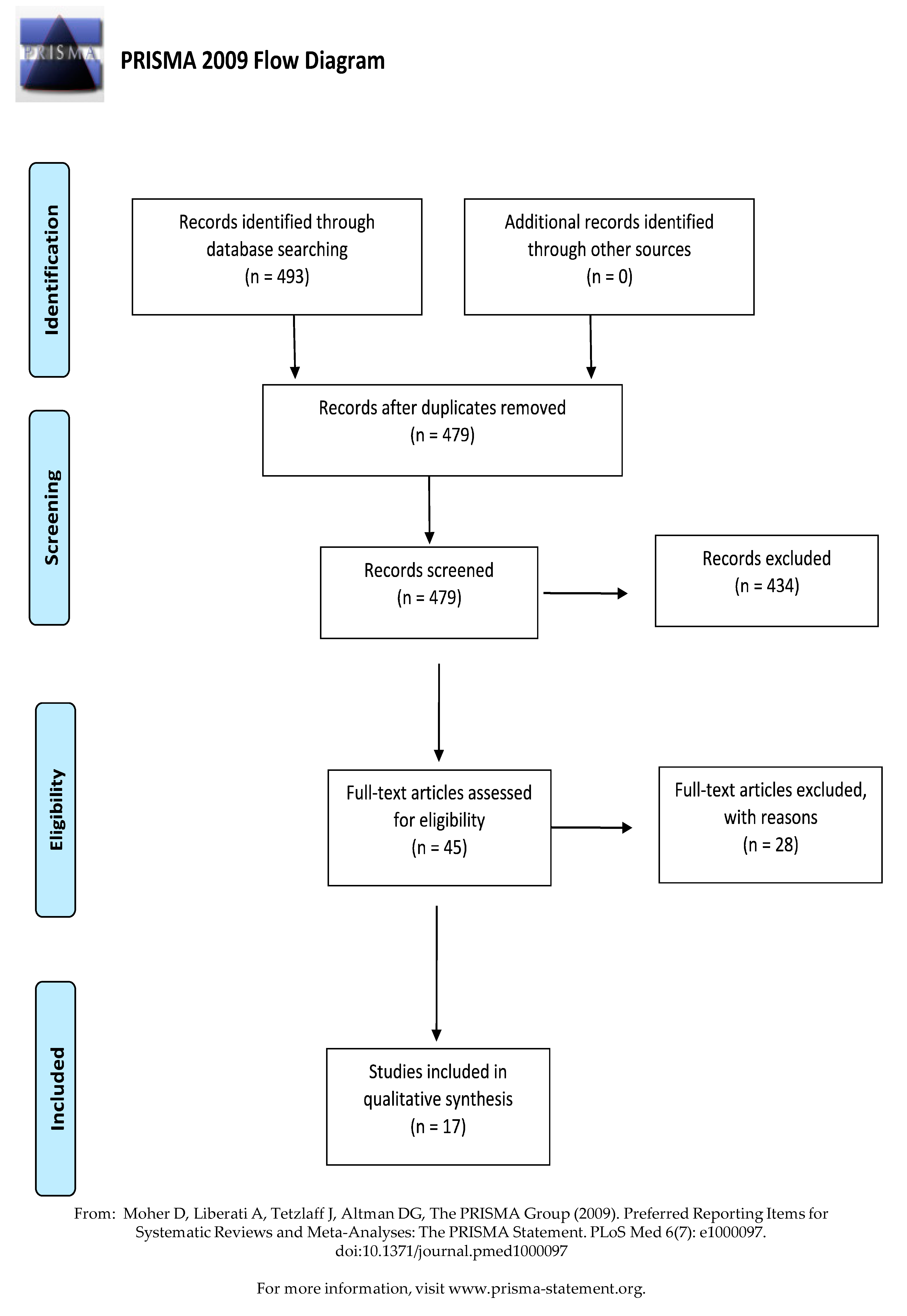
3. Methods
- −
- To what log kill are the pathogens that play a role in dentistry eliminated by VHP fogging?
- −
- What VHP fogging disinfection methods could be effective in the dental environment?
3.1. PICOS Statement
3.2. Search Strategy
3.3. Eligibility Criteria
3.4. Study Selection
3.5. Data Extraction
3.6. Control Measures
3.7. Quality Assessment
4. Results
4.1. Search Results
4.2. Characteristics of the Included Studies
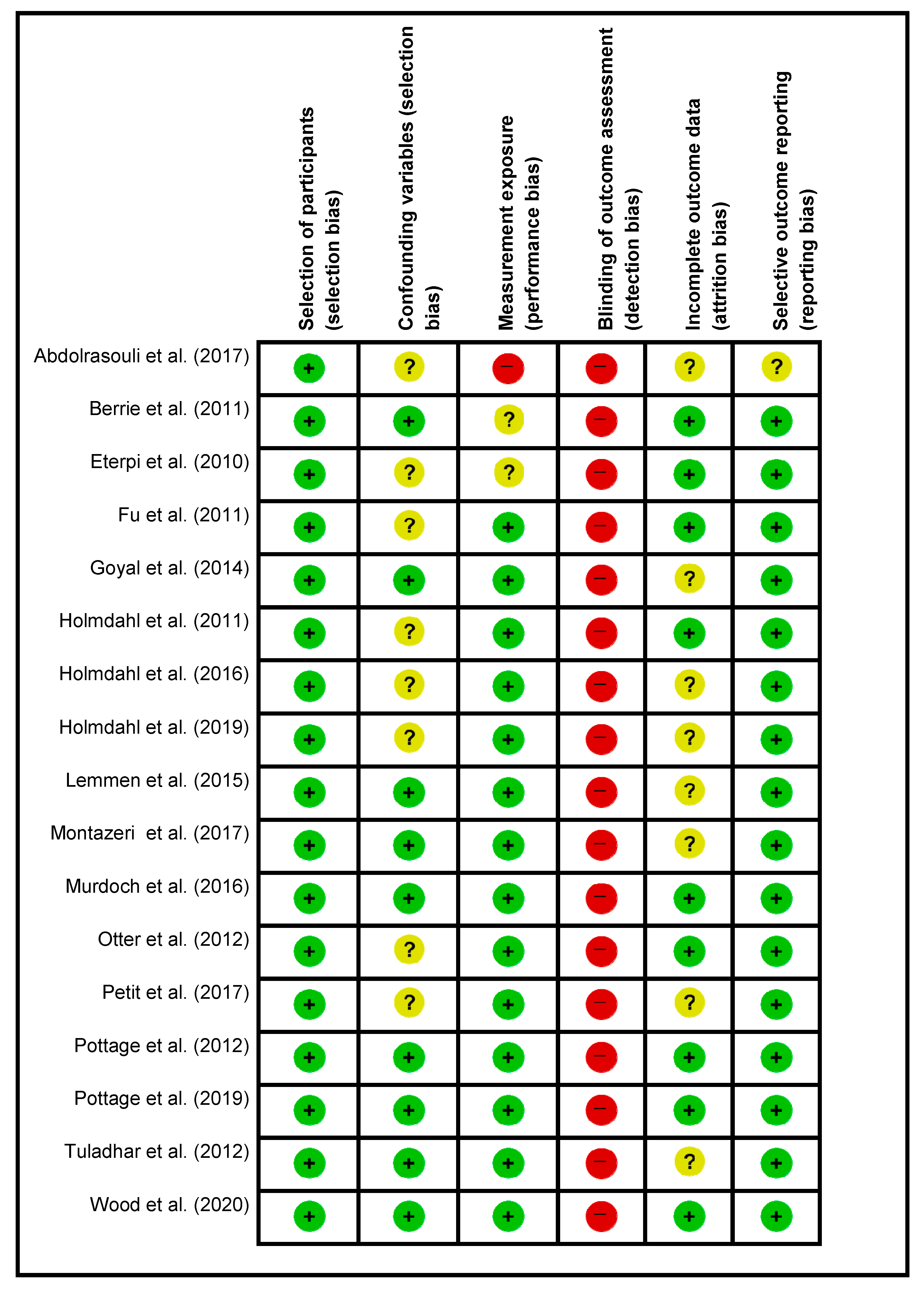
4.3. Risk of Bias in the Included Studies
4.4. Characteristics of VHP Decontamination on Pathogens
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Ali, S.; Muzslay, M.; Bruce, M.; Jeanes, A.; Moore, G.; Wilson, A.P.R. Efficacy of two hydrogen peroxide vapour aerial decontamination systems for enhanced disinfection of meticillin-resistant Staphylococcus aureus, Klebsiella pneumoniae and Clostridium difficile in single isolation rooms. J. Hosp. Infect. 2016, 93, 70–77. [Google Scholar] [CrossRef]
- Schelenz, S.; Hagen, F.; Rhodes, J.L.; Abdolrasouli, A.; Chowdhary, A.; Hall, A.; Ryan, L.; Shackelton, J.; Trimlett, R.; Meis, J.F.; et al. First hospital outbreak of the globally emerging Candida auris in a European Hospital. Antimicrob. Resist. Infect. Control 2016, 5, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarano, A.; Inchingolo, F.; Lorusso, F. Environmental Disinfection of a Dental Clinic during the Covid-19 Pandemic: A Narrative Insight. BioMed Res. Int. 2020. [Google Scholar] [CrossRef] [PubMed]
- Otter, J.A.; Mepham, S.; Athan, B.; Mack, D.; Smith, R.; Jacobs, M.; Hobkins, S. Terminal decontamination of the Royal Free London’s high-level isolation unit after a case of Ebola virus disease using hydrogen peroxide vapour. Am. J. Infect. Control 2015, 44, 233–235. [Google Scholar] [CrossRef]
- Falag, M.E.; Thomaidis, P.C.; Kotsantis, I.K.; Sgouros, K.; Samonis, G.; Karageorgopoulos, D.E. Airborne hydrogen peroxide for disinfection of the hospital environment and infection control: A systematic review. J. Hosp. Infect. 2011, 78, 171–177. [Google Scholar] [CrossRef]
- Chan, H.T.; White, P.; Sheorey, H.; Cocks, J.; Waters, M.-J. Evaluation of the biological efficacy of hydrogen peroxide vapour decontamination in wards of an Australian hospital. J. Hosp. 2011, 79, 125–128. [Google Scholar] [CrossRef]
- Tysiąc-Miśta, M.; Dubiel, A.; Brzoza, K.; Burek, M.; Pałkiewicz, K. Air disinfection procedures in the dental office during the covid-19 pandemic. Med. Pracy 2021, 72. [Google Scholar] [CrossRef]
- French, G.L.; Otter, J.A.; Shannon, K.P.; Adams, N.M.T.; Watling, D.; Parks, M.J. Tackling contamination of the hospital environment by methicillin-resistant Staphylococcus aureus (MRSA): A comparison between conventional terminal cleaning and hydrogen peroxide vapour decontamination. J. Hosp. Infect. 2004, 57, 31–37. [Google Scholar] [CrossRef]
- Rogers, J.V.; Richter, W.R.; Shaw, M.Q.; Choi, Y.W. Vapour-phase hydrogen peroxide inactivates Yersinia pestis dried on polymers, steel, and glass surfaces. Lett. Appl. Microbiol. 2008, 47, 279–285. [Google Scholar] [CrossRef]
- Blazejewski, C.; Wallet, F.; Rouzé, A.; Le Guern, R.; Ponthieux, S.; Salleron, J.; Nseir, S. Efficiency of hydrogen peroxide in improving disinfection of ICU rooms. Crit. Care 2015, 19, 30. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Abdolrasouli, A.; Armstrong-James, D.; Ryan, L.; Schelenz, S. In vitro efficacy of disinfectants utilised for skin decolonisation and environmental decontamination during a hospital outbreak with Candida auris. Mycoses 2017, 60, 758–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eterpi, M.; McDonnell, G.; Thomas, V. Decontamination efficacy against Mycoplasma. Lett. Appl. Microbiol. 2010, 52, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.Y.; Gent, P.; Kumar, V. Efficacy, efficiency and safety aspects of hydrogen peroxide vapour and aerosolized hydrogen peroxide room disinfection systems. J. Hosp. Infect. 2012, 80, 199–205. [Google Scholar] [CrossRef]
- Holmdahl, T.; Lanbeck, P.; Wullt, M.; Walder, M.H. A head-to-head comparison of hydrogen peroxide vapor and aerosol room decontamination systems. Infect. Control Hosp. Epidemiol. 2011, 32, 831–836. [Google Scholar] [CrossRef]
- Holmdahl, T.; Walder, M.; Uzcátegui, N.; Odenholt, I.; Lanbeck, P.; Medstrand, P.; Widell, A. Hydrogen peroxide vapor decontamination in a patient room using feline calicivirus and murine norovirus as surrogate markers for human norovirus. Infect. Control Hosp. Epidemiol. 2016, 37, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Holmdahl, T.; Odenholt, I.; Riesbeck, K.; Medstrand, P.; Widell, A. Hydrogen peroxide vapour treatment inactivates norovirus but has limited effect on post-treatment viral RNA levels. Infect. Dis. 2019, 51, 197–205. [Google Scholar] [CrossRef]
- Otter, J.A.; Yezlia, S.; French, G.L. Impact of the suspending medium on susceptibility of meticillin-resistant Staphylococcus aureus to hydrogen peroxide vapour decontamination. J. Hosp. Infect. 2012, 82, 213–215. [Google Scholar] [CrossRef]
- Petit, B.M.; Almeida, F.C.; Uchiyama, T.R.; Lopes, F.O.C.; Tino, K.H.; Chewins, J. Evaluating the efficacy of hydrogen peroxide vapour against foot-and-mouth disease virus within a BSL4 biosafety facility. Lett. Appl. Microbiol. 2017, 65, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Tuladhara, E.; Terpstrac, P.; Koopmansa, M.; Duizera, E. Virucidal efficacy of hydrogen peroxide vapour disinfection. J. Hosp. Infect. 2012, 80, 110–115. [Google Scholar] [CrossRef]
- Goyala, S.M.; Chandera, Y.; Yezlib, S.; Otter, J.A. Evaluating the virucidal efficacy of hydrogen peroxide vapour. J. Hosp. Infect. 2014, 86, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Lemmen, S.; Scheithauer, S.; Häfner, H.; Yezli, S.; Mohr, M.; Otter, J.A. Evaluation of hydrogen peroxide vapor for the inactivation of nosocomial pathogens on porous and nonporous surfaces. Am. J. Infect. Control 2015, 43, 82–85. [Google Scholar] [CrossRef]
- Murdoch, L.E.; Bailey, L.; Banham, E.; Watson, F.; Adams, N.M.T.; Chewins, J. Evaluating different concentrations of hydrogen peroxidein an automated room disinfection system. Lett. Appl. Microbiol. 2016, 63, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Montazeri, N.; Manuel, C.; Moorman, E.; Khatiwada, J.R.; Williams, L.L.; Jaykus, L.A. Virucidal Activity of Fogged Chlorine Dioxide- and Hydrogen Peroxide-Based Disinfectants against Human Norovirus and Its Surrogate, Feline Calicivirus, on Hard-to-Reach Surfaces. Front. Microbiol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Berrie, E.; Andrews, L.; Yezli, S.; Otter, J.A. Hydrogen peroxide vapour (HPV) inactivation of adenovirus. Lett. Appl. Microbiol. 2011, 52, 555–558. [Google Scholar] [CrossRef]
- Pottage, T.; Lewis, S.; Lansley, A.; Fraser, S.; Hendon-Dunn, C.; Bacon, J.; Ngabo, D.; Parks, S.R.; Bennett, A.M. Hazard Group 3 agent decontamination using hydrogen peroxide vapour in a class III microbiological safety cabinet. J. Appl. Microbiol. 2019, 128, 116–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, J.P.; Richter, W.; Sunderman, M.; Worth-Calfee, M.; Serre, S.; Mickelsen, L. Evaluating the Environmental Persistence and Inactivation of MS2 Bacteriophage and the Presumed Ebola Virus Surrogate Phi6 Using Low Concentration Hydrogen Peroxide Vapor. Environ. Sci. Technol. 2020, 54, 3581–3590. [Google Scholar] [CrossRef] [Green Version]
- Pottage, T.; Macken, S.; Walker, J.T.; Bennett, A.M. Meticillin-resistant Staphylococcus aureus is more resistant to vaporized hydrogen peroxide than commercial Geobacillus stearothermophilus biological indicators. J. Hosp. Infect. 2012, 80, 41–45. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Database | Search Terms |
|---|---|
| DOAJ | Hydrogen peroxide vapor OR Hydrogen peroxide vapor OR vaporized hydrogen peroxide (VHP), producing system OR Hydrogen peroxide fogger OR hydrogen peroxide in vitro AND ( decontamination or disinfection ) |
| Ebscohost | Hydrogen peroxide vapor OR Hydrogen peroxide vapour OR VHP producing system OR Hydrogen peroxide fogger OR hydrogen peroxide in vitro AND (decontamination or disinfection ) |
| Pubmed | (((((Hydrogen peroxide vapor) OR (Hydrogen peroxide vapour)) OR (HPV producing system)) OR (Hydrogen peroxide fogger)) OR (Hydrogen peroxide fog)) AND (decontamination) |
| Scopus | (((((Hydrogen peroxide vapor) OR (Hydrogen peroxide vapour)) OR (HPV producing system)) OR (Hydrogen peroxide fogger)) OR (Hydrogen peroxide fog)) AND (decontamination) |
| Sceilio | (((((Hydrogen peroxide vapor) OR (Hydrogen peroxide vapour)) OR (HPV producing system)) OR (Hydrogen peroxide fogger)) OR (Hydrogen peroxide fog)) AND (decontamination) |
| Web of Science | (Hydrogen peroxide vapo?r* OR HPV producing system* AND Enterococcus faecalis AND Candida albicans AND decontamination) |
| Characteristics | n or n (%) |
|---|---|
| Publication Year | n = 17 |
| 2010 | 1 (0.05) |
| 2011 | 3 (0.17) |
| 2012 | 3 (0.17) |
| 2014 | 1 (0.05) |
| 2015 | 1 (0.05) |
| 2016 | 2 (0.11) |
| 2017 | 3 (0.17) |
| 2019 | 2 (0.11) |
| 2020 | 1 (0.05) |
| Location | n = 17 |
| United Kingdom | 8 (0.47) |
| Sweden | 3 (0.17) |
| USA | 2 (0.11) |
| Brazil | 1 (0.05) |
| France | 1 (0.05) |
| Germany | 1 (0.05) |
| The Netherlands | 1 (0.05) |
| Hydrogen Peroxide Vapourizing machine | (n = 19) or n% of total machines |
| Aeroclave | 1 (0.05) |
| Bioquell | 1 (0.05) |
| Bioquell BQ-50 | 1 (0.05) |
| Bioquell Clarus C | 2 (0.10) |
| Bioquell Clarus L | 1 (0.05) |
| Bioquell Clarus R | 3 (0.15) |
| Bioquell Clarus S | 1 (0.05) |
| Bioquell Q10 | 4 (0.21) |
| Liquid Verne Veiling equipment | 1 (0.05) |
| Sterinis aHP | 1 (0.05) |
| Steris La Calhene VHP | 1 (0.05) |
| Steris VHP | 1 (0.05) |
| Sterinis system SR2 | 1 (0.05) |
| Assessed Pathogen: | n or n% of total pathogens |
| Candida | (n = 34) |
| Various Candida species | 34 (100) |
| Bacteria | (n = 27) |
| Acholeplasma laidlawii | 1 (0.03) |
| Acinetobacter baumannii | 1 (0.03) |
| Bacillus anthracis (Ames) spores | 1 (0.03) |
| Brucella abortus | 1 (0.03) |
| Burkholderia pseudomallei | 1 (0.03) |
| Clostridium difficile | 1 (0.03) |
| Escherichia coli | 1 (0.03) |
| Geobacillus stearothermophilus biological indicators | 9 (0.33) |
| MDR Acinetobacter baumannii | 1 (0.03) |
| Methicillin-resistant Staphylococcus aureus (MRSA) | 5 (0.18) |
| Mycoplasma pneumoniae | 1 (0.03) |
| Mycoplasma gallisepticum | 1 (0.03) |
| Mycobacterium tuberculosis | 1 (0.03) |
| Vancomycin- resistant Enterococcus (VRE) | 1 (0.03) |
| Yersinia pestis | 1 (0.03) |
| Virus | n = 21 |
| Adenovirus | 2 (0.09) |
| Avian influenza virus (AIV) | 1 (0.04) |
| Escherichia virus MS2 | 1 (0.04) |
| Feline Calicivirus | 3 (0.14) |
| Foot and mouth disease (FMDV) | 1 (0.04) |
| Human adenovirus type 1 | 1 (0.04) |
| Human norovirus | 3 (0.14) |
| Influenza A virus (H1N1) | 1 (0.04) |
| Murine norovirus (MNV) | 3 (0.14) |
| Pseudomonas virus phi6 | 1 (0.04) |
| Poliovirus | 1 (0.04) |
| Rotavirus | 1 (0.04) |
| Swine influenza virus (SwIV) | 1 (0.04) |
| Transmissible Gastroenteritis coronavirus of pigs (TGEV) | 1 (0.04) |
| Characteristics: | |
| Method of inoculation | n = 29, n% of total surfaces |
| Sabouraud’s dextrose agar and fabric | 2 (0.06) |
| Stainless steel 10 mm-diameter discs/coupon | 5 (0.17) |
| Stainless steel 3 mm-diameter discs/coupon | 1 (0.03) |
| Stainless steel 2.2 cm × 2.5 cm disc | 1 (0.03) |
| Tyvek-pouched stainless steel disc/coupon | 5 (0.17) |
| Plastic plates | 2 (0.06) |
| Steel embossing tape 2.5 cm × 5 cm | 1 (0.03) |
| Roller bottle | 1 (0.03) |
| Unspecified stainless steel/coupon | 4 (0.14) |
| Gauze | 1 (0.03) |
| Glass | 1 (0.03) |
| Painted joint tape | 1 (0.03) |
| Wood | 2 (0.06) |
| Ceramic tile | 1 (0.03) |
| N95 Filter medium | 1 (0.03) |
| Efficacy: Log kill | |
| >8 log | 1 |
| >6 log | 4 |
| >4 log | 4 |
| >3 log | 2 |
| <2 log | 2 |
| 1.3–3.5 log reduction | 1 |
| Log reduction not specified | 4 |
| Author | Country of Study | Aim/Objective | Pathogen Used | Methodology:-Hydrogen Peroxide Concentration | Blinding and Controls | Sample Hanling and Contamination Prevention | Failed Experiments and Data/Results Not Presented | Pathogens Placed on Material | Outcome (Level of Bio-Decontamination) |
|---|---|---|---|---|---|---|---|---|---|
| A Abdolrasouli et al. 2017 | United Kingdom | In vitro evaluation of the efficacy of VHP on standard and outbreak C. auris. | 34 different yeast isolates: 4 strains (Candida albicans, Candida tropicalis, Candida krusei, Candida parapsilosis) 28 outbreak isolates of C. auris | Bioquell machine, No H2O2 liquid concentration, performed following manufacture instructions. 8 g of H2O2/m3. | No blinding. One C. aurus control plate with no exposure to VHP. Six yeast-free control wells. No BI used. Done in triplicate. Wells of pathogen grown in a 96-well plate and desiccated, sealed, and kept at 4 °C until exposure to VHP. Viability was then assessed on SDA with C. auris control plate. | Did not state how long after fogging well plates were closed to prevent contamination. | One Indian C. auris and a specific Indian strain not named. Non-exposed C. auris. Candida species and VHP exposed C. aurus survive in a desiccated state. Data not shown. | Well plates. | Data provided evidence that C. auris (and other Candida species) are effectively killed with a 96.6–100% by H2O2 vaporization. |
| E Berrie et al. 2011 | United Kingdom | In vitro efficacy of inactivation of recombinant adenovirus by VHP. | Dried recombinant adenovirus (Ad5GFP) | Bioquell Clarus S machine, 60 mL of 30% H2O2 liquid concentration, performed dwell time 45 min. Whole VHP cycle 3 h | Exposed and non-exposed samples to VHP. BI (Biological Indicator) indicators used. The experiment is one disc per dilution and repeated in triplicate | Immediately after the experiment, the samples were transferred to a sterile microbiological safety cabinet. | One to two logs of pathogen lost due to drying or recovery method compared to wet reference samples compared to experiment two at the titer. Viability reduction data explained in the article. | Stainless steel 10-mm-diameter discs. | Data provided evidence that Adenovirus are effectively killed with a 7.6 to 9.4 log kill by H2O2 vaporization. |
| M Eterpi et al. 2010 | France & United Kingdom | In vitro evaluation of the efficacy of VHP and cold VHP sterilization against Mycoplasma. | Mycoplasma gallisepticum, M. pneumoniae, and A. laidlawii | VHP100 Steris machine. 30% H2O2 liquid concentration. Three cycles 1200 ppm/15 min; 400–500 ppm/60 min; 180–200 ppm/4 h. | No blinding. VHP unexposed samples kept under a laminar flow hood in sealed Petri dishes for the same time cycle and managed the same as exposed coupons. No BI used. Six treated samples with each method and repeated for times. | Samples were transferred to an SP4-glucose broth immediately after VHP exposure. | Less than one log of pathogen lost due to drying or recovery method as described by Nagatomo et al. 2001 with loss due to recovery ≤0.5 log. Neutralization an additional ≤0.5 log. Viability reduction data explained in the article. | Stainless steel coupons of 1 cm × 3 cm. | Data provided evidence that Mycoplasma is effective with a >4 log kill by H2O2 vaporization. |
| T. Y. Fu et al. 2011 | United Kingdom | Compare the efficacy, efficiency of VHP and aHP. | Methicillin-resistant Staphylococcus aureus (MRSA), Clostridium difficile and Acinetobacter baumannii. | Bioquell Clarus R machine. 30% H2O2 liquid. SR2 Sterinis machine with a 5% H2O2 liquid and silver ion (50 ppm) and orthophosphoric acid (<50 ppm), dose 6 mL/m3 recommended by the manufacturer. | No blinding. Both exposed and non-exposed to VHP. BI used. Four cycles per machine with each cycle consisting of three unexposed VHP/aHP and three dry VHP/aHP discs for water, 3% BSA (Bovine Serum Albumin) and 10% BSA. The control was cycled separately over four cycles. | Did not state how long after fogging discs were transferred to prevent contamination, nor the overnight drying to prevent contamination. | No pathogens lost or contaminated samples were described or considered in the methodology. All data presented. | Stainless steel discs with a diameter of 10 mm. | The VHP system achieved a greater level of biological inactivation between 4–6 log for most locations than the aHP system 1–5 log depending on the pathogen. |
| Goyal et al. 2014 | United Kingdom | Evaluate the in vitro efficacy of three volumes of VHP on selected viruses with surface contamination. | FCV as a surrogate of human norovirus, TGEV as a surrogate for the SARS virus, human adenovirus type 1, AIV (A/chicken/Maryland/ 2007[H9N9]) and SwIV (A/swine/Minnesota/2010 [H3N2]). | Bioquell Clarus L machine. 35% H2O2 liquid. Hydrogen peroxide at 2 mL/min for 1, 2, 5 min followed by 1.5 mL/min or 15 min equating to the following different volumes: 25, 27, and 33 mL with the treatment time between 2–3 h for the completed cycle. | No blinding. Non-VHP exposed inoculated discs at room temperature. Four BI were exposed to the VHP in corners of the environmental chamber. Positive BI control was not exposed to VHP. 8% Fetal Bovine Serum (FBS) served as soiling present in the culture medium. Each experiment had inoculated discs exposed to each vaporized volume of VHP and one disc not exposed to VHP. | Discs are left to dry in a biosafety cabinet to prevent contamination. After VHP the discs including the non-exposed control discs were transferred immediately to the environmental chamber for titration. | Data was determined concerning the control disc. This allows direct comparison to the test and control discs having the same log loss, making the comparison more accurate. But also leads to not knowing what the log loss of viral load is. Loss of virus log particles during the methodology of drying and recovery. Not calculated | 10 mm stainless steel discs. | VHP was virucidal for viruses assessed dried on surfaces, suggesting that VHP can be considered for the disinfection of virus-contaminated surfaces based on the 8% FBS surface contamination. |
| Holmdahl et al. 2011 | Sweden | Comparison of VHP and aHP to BI in various locations. | BI with G. stearothermophilus | Steris VHP machine. 5% H2O2 liquid. 6 mL/m3 with 100–150 ppm. Bioquell Q10 machine. 35% H2O2 liquid. 900 mL per test and results in 6.6 g/m3. 338 ppm peak, 3 h. | No blinding. BI was used as control. | BI in Tyvek pouches | Direct comparison of two machines on BI. All results presented. | BI stainless steel disc placed in various locations in the room. | All results presented for the same areas assessed for the two machines. VHP showed a 100% negative result while aHP presented with multiple positive results, the inconsistency with the aHP was 10% kill (100 ppm) followed by two cycles of 79% kill, with the ppm in cycles 2 and 3 being 130 and >150 ppm respectively. |
| Holmdahl et al. 2016 | Sweden | Evaluate the efficacy of VHP in six locations for two virus pathogens with surface contamination. | FCV, feline permissive cell line (FCWF). MNV and permissive murine cell line (RAW 264.7) | Bioquell Q10 machine. As per the manufacturer. No H2O2 liquid concentration. Gassing time 40–50 min, dwell time 15 min. VHP ppm range 474–505 ppm with a total cycle time of 3 h. | Virus prepared in triplicate in well plates. Two inoculated plates and BI not VHP exposed two areas of the control room. BI exposed at all the positions with VHP next to virus inoculated plates. Each VHP exposure experiment was repeated in triplicate. | Well plates left to dry at room temperature under a hood for 2 h and stored. | Loss of virus log particles during the methodology of drying and recovery were calculated. | Well plates | VHP was virucidal for viruses assessed dried on surfaces, suggesting that VHP can be considered for the disinfection of virus-contaminated surfaces based on the 10% FBS surface contamination. |
| Holmdahl et al. 2019 | Sweden | Assess norovirus viability of cytopathic the effect after VHP. | Two human norovirus field strains, genogroup I and II. Murine norovirus. | Bioquell Q10 machine. No H2O2 liquid concentration. 860 ppm VHP for 33 min gassing and 55 min dwell. This resulted in 205 g of H2O2 used. | No blinding. BI and mock samples with no VHP exposure. | Virus samples dried in 35 mm diameter wells of six-well plates mock and VHP treated samples. | Data was determined concerning the lowest detection limit of 10−0.5. This allows direct comparison to the test and control discs having the same log loss, making the comparison more accurate. But also leads to not knowing what the log loss of viral load is. | Well pates | BI deactivated and norovirus log 5 kill. |
| Lemmen et al. 2015 | Germany | Efficacy of VHP on five pathogens dried onto various hard surfaces. | MDR MRSA and MDR VRE, MDR A baumannii. BI as proxy for D. difficile | Bioquell Q10 machine. 30% H2O2 liquid. Three cycles were performed. The dose of 11.2 g/m3 achieved after 50–52 min until hydrogen peroxide was 500–600 ppm. 20 min dwell time. | No blinding. BI used. Four of each material inoculated with the pathogen and distributed in four locations exposed to VHP and the same number not exposed to VHP as controls. BI placed in 4 corners of the room and 3 challenge locations. | Kept on a sterile basis until experiment and after VHP exposure transferred to a sterile glass tube with 1 mL distilled water. | Lost pathogens are known and presented in the article and mean log reduction is calculated. | Stainless steel discs, gauze | VHP inactivated all spore BI (>6 log10 reduction), and no MRSA, VRE, or MDR A baumannii were recovered from the stainless steel and cotton carriers (>4–5 log10 reduction, depending on the starting inoculum). VHP was equally effective at all carrier locations. No difference in efficacy |
| Montazeri et al. 2017 | USA | Inactivation of human norovirus after VHP exposure. | FCV. Outbreak human NoV GI.6 and GII.4. | AeroClave System 3110. 7.5% H2O2 liquid. No air handling unit during vapor process, at end of cycle turned on for 20 min. 7.1–15.9 mL/m3 was achieved, with 5 min dwell time following the manufacturer’s recommendation. Then the air handling unit was switched on for 20 min. | No blinding. No BI used. 7 locations in BSL-3 laboratory assessed with VHP. Inoculated coupons not exposed to VHP were outside the laboratory for the duration of the experiment. | Air-dried in a biosafety hood. And used immediately for the experiment. After the experiment, the samples were transferred to PBS tubes. | Data was determined to the control disc. This allows direct comparison to the test and control discs having the same log loss, making the comparison more accurate. But also leads to not knowing what the log loss of viral load is. | Stainless steel embossing tape | No trend was observed for human NoV GI.6 reduction as a function of H2O2-based disinfectant formulation concentration. However, increasing the concentration from 7.1 to 12.4 mL/m3 enhanced viral genomic copy number reduction for GII.4 |
| Murdoch et al. 2016 | United Kingdom | Assess the application of three different liquid concentrations for VHP. | MRSA and Geobacillus stearothermophilus | Bioquell BQ50 machine. 5, 10, and 35% H2O2. 640 g hydrogen peroxide over 40 min and 200 min dwell time. | No blinding labeled containers. BI used. Positive and negative controls. Every 10 min throughout the experiment a BI was exposed for 10 min. | All specimens were placed in labeled 30 mL containers. | No pathogens lost or contaminated samples were described or considered in the methodology. All data presented. | Stainless steel discs | 35% hydrogen peroxide is ideal. |
| Otter et al. 2012 | United Kingdom | Efficacy of VHP against methicillin-resistant Staphylococcus aureus on various surfaces. | MRSA | Bioquell Clarus R machine. No H2O2 liquid concentration. VHP mean concentration 134 ppm. | No blinding. No BI used. Control discs were not VHP exposed. The experiment ran in triplicate per period for each contaminant material. | Air-dried in the test room air, then VHP exposure and immediately enumerated. | No pathogens lost or contaminated samples were described or considered in the methodology. All data presented. | Stainless steel discs | Relative susceptibility to VHP was 10% BSA < TSB < 3% BSA = water. At a ppm achieved and >75 min exposure, no MRSA was recovered on the discs. |
| Petit et al. 2017 | Brazil | Efficacy of VHP against foot-and-mouth disease. | Three serotypes of Foot-and-mouth disease virus (FMDV) | Bioquell Clarus R machine. 35% H2O2 liquid. 115 min. VHP injection time 75 min, 40 min dwell time. | No blinding. No validated BI manufactured by VHP producers. Positive controls of three serotypes. Three replicate cycles of 15 BI produced from FMDV for VHP exposure. Five samples for each viral serotype were produced. One plosive control per serotype for the duration of the experiment was stored in a refrigerator. | Dried in class 2 biological safety cabinet. | No pathogens lost or contaminated samples were described or considered in the methodology. All data presented. | Inside the cap of the polypropylene cryogenic tube. | Three FMDV serotypes showed full inactivation. |
| Pottage et al. 2012 | United Kingdom | Comparison of log kill of BI vs MRSA after VHP exposure. | G. stearothermophilus and MRSA | A Steris VHP-1000ARD machine. 35% H2O2 liquid. 750 ppm maintained in chamber. | No blinding. Random removal of VHP exposed samples. 18 MRSA and 18 BI indicators placed in sterile Petri dishes and VHP exposed for pre-determined periods. Three unexposed stainless steel discs of each pathogen were used. | Inoculated stainless steel discs air-dried for 1 h. | No pathogens lost or contaminated samples were described or considered in the methodology. All data presented. | BI on stainless steel discs sealed in Tyvek packages. | BI greater log kill than MRSA for the same periods of exposure. |
| Pottage et al. 2019 | United Kingdom | Efficacy of VHP on dried bacteria. | Bacillus anthracis (Ames) spores, Brucella abortus, Burkholderia pseudomallei, Escherichia coli, Mycobacterium tuberculosis and Yersinia pestis. | Bioquell Clarus C machine. 35% H2O2 liquid. 90 min cycle. | No blinding. Three controls tied in double plastic bags to determine the loss of log pathogen. 3 control samples were used as the start pathogen load. 12 produced BI for each VHP run to allow triplicate exposure. Three control BI from a VHP manufacturer used per VHP cycle. | Dried in a biological cabinet for 1 h. | No pathogens lost or contaminated samples were described or considered in the methodology. All data presented. | Stainless steel coupons in Petri dishes | This study demonstrates that VHP can inactivate a range of HG3 agents at high concentrations with associated organic matter, but M. tuberculosis showed increased resistance to the process. |
| Tuladhar et al. 2012 | The Netherlands | Virucidal efficacy of VHP against respiratory and enteric viruses on various materials. | Poliovirus, human norovirus genogroup II.4 (GII.4), murine norovirus 1, rotavirus, adenovirus, and influenza A (H1N1) virus. | Boneco 7131 machine. 12% H2O2 liquid. 120–134 ppm at a flow rate of 2.3 L/h. | No validated BI manufactured by VHP producers. Triplicate samples per virus were performed twice. Control samples were not VHP exposed. | Dried in a biohazard cabinet. | No pathogens lost or contaminated samples were described or considered in the methodology. All data presented. | Stainless steel, framing panel, and gauze carriers. | VHP effective against pathogens assessed. |
| Wood et al. 2020 | USA | Assess the decontamination efficacy of VHP on phages. | Bacteriophage viruses, MS2 and Phi6 | Humidifier with 3 or 8% H2O2 liquid generated to 25 ppm. Bioquell Clarus C machine. 35% H2O2 liquid. 25 ppm and 400 ppm generated. | No validated BI manufactured by VHP producers. Inoculated samples, not VHP exposed, and inoculated samples VHP exposed. Two blank samples. Completed in triplicate. | Samples made and dried in a biosafety cabinet. After the experiment coupons were sealed and transferred to the biosafety cabinet. | No pathogens lost or contaminated samples were described or considered in the methodology. All data presented. | Stainless steel, glass, tile, N95 mask material, painted joint tape, wood. | Extrapolating from these results for both an enveloped and non-enveloped virus, we would expect LCHP would be a viable decontamination option for EBOV for relatively clean surfaces |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, R.; Mulder, R. A Systematic Review on the Efficacy of Vaporized Hydrogen Peroxide as a Non-Contact Decontamination System for Pathogens Associated with the Dental Environment. Int. J. Environ. Res. Public Health 2021, 18, 4748. https://doi.org/10.3390/ijerph18094748
Ahmed R, Mulder R. A Systematic Review on the Efficacy of Vaporized Hydrogen Peroxide as a Non-Contact Decontamination System for Pathogens Associated with the Dental Environment. International Journal of Environmental Research and Public Health. 2021; 18(9):4748. https://doi.org/10.3390/ijerph18094748
Chicago/Turabian StyleAhmed, Rukshana, and Riaan Mulder. 2021. "A Systematic Review on the Efficacy of Vaporized Hydrogen Peroxide as a Non-Contact Decontamination System for Pathogens Associated with the Dental Environment" International Journal of Environmental Research and Public Health 18, no. 9: 4748. https://doi.org/10.3390/ijerph18094748