
Solitary Extramedullary Plasmacytoma Presenting as Asymptomatic Palatal Erythroplakia: Report of a Case

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
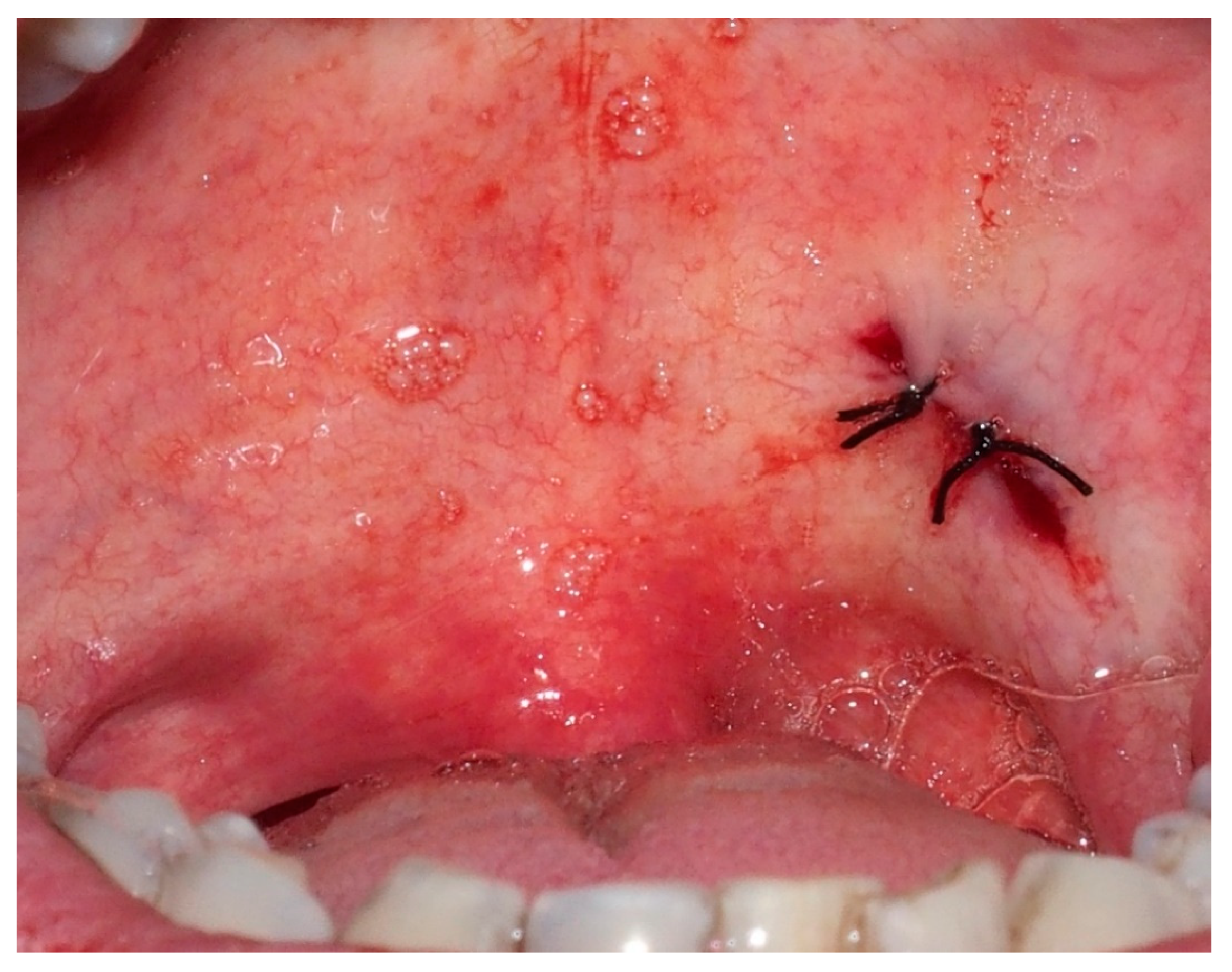
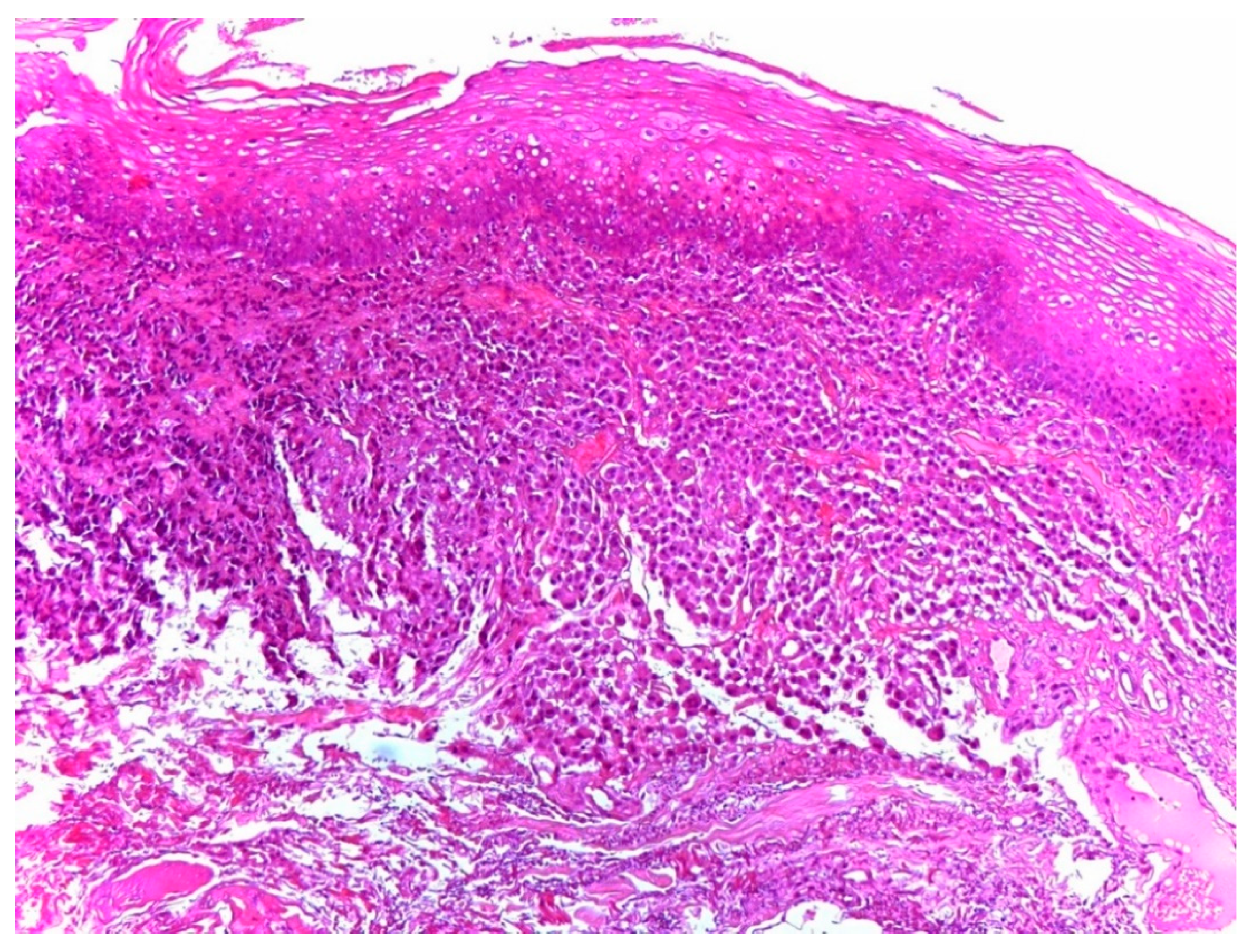
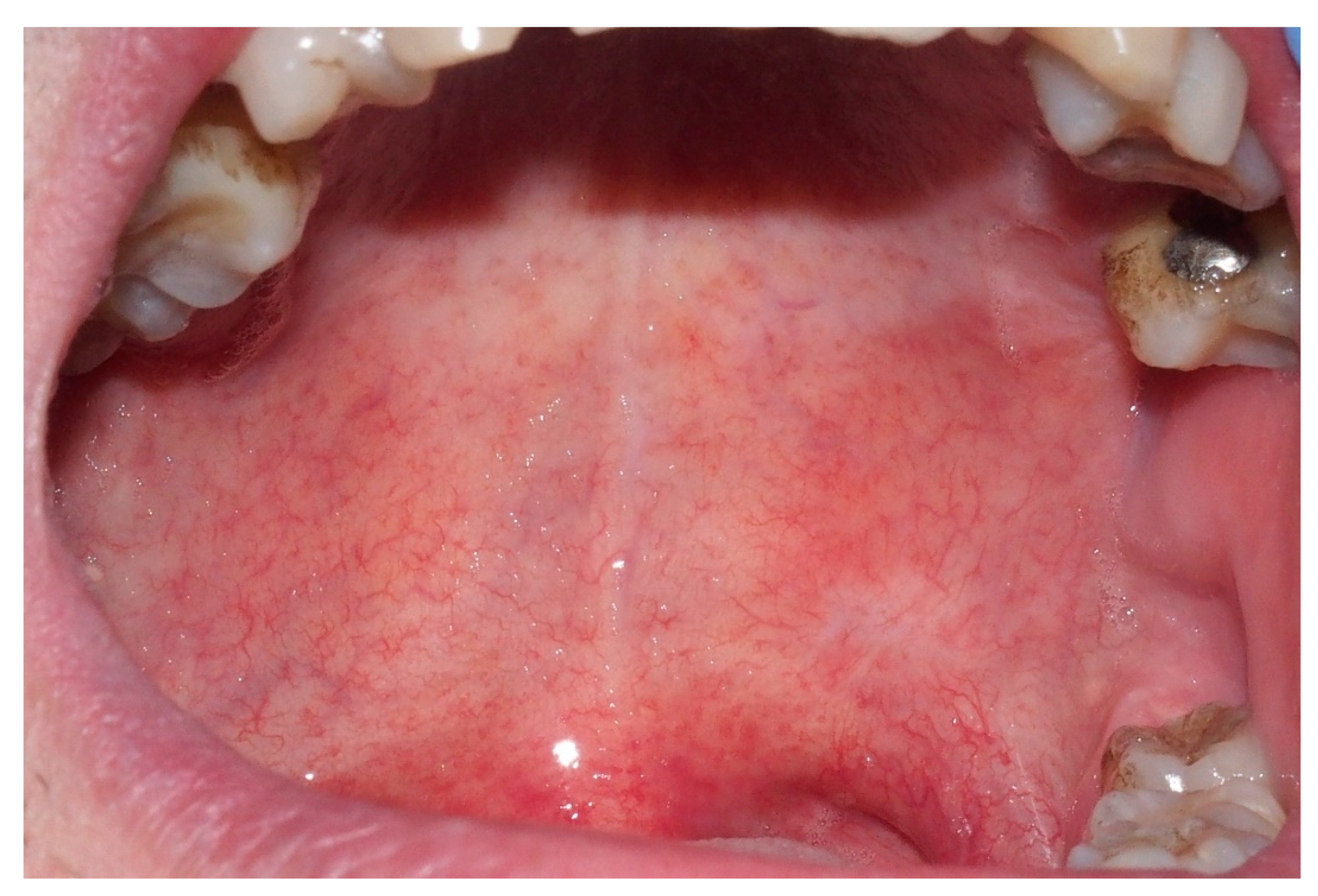
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lai, C.Y.; Hsieh, H.H.; Chen, H.K.; Chao, C.Y.; Hua, C.H.; Tai, C.J.; Bau, D.T.; Tsai, M.H.; Shih, L.C. Clinical Features of Head and Neck Solitary Extramedullary Plasmacytoma in Taiwan. In Vivo 2020, 34, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Barros, T.P.; Savilha, F.M.; Amantea, D.V.; Campolongo, G.D.; Neto, L.B.; Alves, N.; Oliveira, R.J. Plasmacytoma in the Oral Cavity: A Case Report. Int. J. Odontostomat. 2011, 5, 115–118. [Google Scholar] [CrossRef] [Green Version]
- Majumdar, S.; Raghavan, U.; Jones, N.S. Solitary Plasmacytoma and Extramedullary Plasmacytoma of the Paranasal Sinuses and Soft Palate. J. Laryngol. Otol. 2002, 116, 962–965. [Google Scholar] [CrossRef] [PubMed]
- Caers, J.; Paiva, B.; Zamagni, E.; Leleu, X.; Bladé, J.; Kristinsson, S.Y.; Touzeau, C.; Abildgaard, N.; Terpos, E.; Heusschen, R.; et al. Diagnosis Treatment and Response Assessment in Solitary Plasmacytoma: Updated Recommendations from a European Expert Panel. J. Hematol. Oncol. 2018, 11, 10. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, M.A.; Kiamours, C.; Moulopoulos, L.A. Solitary Plasmacytoma of Bone and Extramedullary Plasmacytoma. Hematol. Oncol. Clin. N. Am. 1999, 13, 1249–1257. [Google Scholar] [CrossRef]
- Gholizadeh, N.; Mehdipour, M.; Rohani, B.; Esmaeili, V. Extramedullary Plasmacytoma of the Oral Cavity in a Young Man: A Case Report. J. Dent. (Shiraz Iran) 2016, 17, 155–158. [Google Scholar]
- Kilciksiz, S.; Karakoyun-Celik, O.; Agaoglu, F.Y.; Haydaroglu, A. A Review for Solitary Plasmacytoma of Bone and Extramedullary Plasmacytoma. Sci. World J. 2012, 2012, 895765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purkayastha, A.; Sharma, N.; Suhag, V.; Lohia, N. Extramedullary Plasmacytoma of Oral Cavity: Series of Three Unusual Cases at Unusual Locations. Int. J. Oral Heal. Sci. 2016, 6, 26–29. [Google Scholar] [CrossRef]
- Webb, H.E.; Harrison, E.G.; Masson, J.K.; Remine, W.H. Solitary Extramedullary Myeloma (Plasmacytoma) of the Upper Part of the Respiratory Tract and Oropharynx. Cancer 1962, 15, 1142–1155. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Takada, K.; Kawai, N.; Hasegawa, K.; Ishikawa, T. Two Cases of Plasmacytoma in the Oral Cavity. Int. J. Oral Surg. 1976, 5, 82–91. [Google Scholar] [CrossRef]
- Susnerwala, S.S.; Shanks, J.H.; Banerjee, S.S.; Scarffe, J.H.; Farrington, W.T.; Slevin, N.J. Extramedullary Plasmacytoma of the Head and Neck Region: Clinicopathological Correlation in 25 Cases. Br. J. Cancer 1997, 75, 921–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morassi, M.L.; Trimarchi, M.; Nicolai, P.; Gregorini, G.; Maroldi, R.; Specks, U.; Facchetti, F. Cocaine, ANCA, and Wegener’s Granulomatosis. Pathologica 2001, 93, 581–583. [Google Scholar] [PubMed]
- Trimarchi, M.; Bellini, C.; Toma, S.; Bussi, M. Back-and-Forth Endoscopic Septoplasty: Analysis of the Technique and Outcomes. Int. Forum Allergy Rhinol. 2012, 2, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Biafora, M.; Bertazzoni, G.; Trimarchi, M. Maxillary Sinusitis Caused by Dental Implants Extending into the Maxillary Sinus and the Nasal Cavities. J. Prosthodont. 2014, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Trimarchi, M.; Bondi, S.; Della Torre, E.; Terreni, M.R.; Bussi, M. Palate Perforation Differentiates Cocaine-Induced Midline Destructive Lesions from Granulomatosis with Polyangiitis. Acta Otorhinolaryngol. Ital. 2017, 37, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Lanzillotta, M.; Campochiaro, C.; Trimarchi, M.; Arrigoni, G.; Gerevini, S.; Milani, R.; Bozzolo, E.; Biafora, M.; Venturini, E.; Cicalese, M.P.; et al. Deconstructing IgG4-Related Disease Involvement of Midline Structures: Comparison to Common Mimickers. Mod. Rheumatol. 2017, 27, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Della Torre, E.; Campochiaro, C.; Cassione, E.B.; Albano, L.; Gerevini, S.; Bianchi Marzoli, S.; Bozzolo, E.; Passerini, G.; Lanzillotta, M.; Terreni, M.; et al. Intrathecal Rituximab for IgG4-Related Hypertrophic Pachymeningitis. J. Neurol. Neurosurg. Psychiatry 2018, 89, 441–444. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Sex | Age | Location | No of Cases |
|---|---|---|---|---|---|---|
| Webb et al. [9] | 1962 | USA | F | 37 | Soft palate | 1 |
| Yoshimura et al. [10] | 1976 | Japan | M | 64 | Mucosa of the hard palate | 1 |
| Susnerwala et al. [11] | 1997 | UK | M | 72 | Soft palate | 1 |
| Majumdar et al. [3] | 2002 | UK | M | 54 | Soft palate, close to the uvula | 1 |
| Barros et al. [2] | 2011 | Brazil | M | 70 | Lesion in the posterior upper alveolar ridge, extending towards the palate | 1 |
| Purkayastha et al. [8] | 2016 | India | M | 44 | Hard palate | 1 |
| Gholizadeh et al. [6] | 2016 | Iran | M | 25 | Palatal side of left maxillary second and third molars | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lalla, F.; Vinciguerra, A.; Lissoni, A.; Arrigoni, G.; Lira Luce, F.; Abati, S. Solitary Extramedullary Plasmacytoma Presenting as Asymptomatic Palatal Erythroplakia: Report of a Case. Int. J. Environ. Res. Public Health 2021, 18, 3762. https://doi.org/10.3390/ijerph18073762
Lalla F, Vinciguerra A, Lissoni A, Arrigoni G, Lira Luce F, Abati S. Solitary Extramedullary Plasmacytoma Presenting as Asymptomatic Palatal Erythroplakia: Report of a Case. International Journal of Environmental Research and Public Health. 2021; 18(7):3762. https://doi.org/10.3390/ijerph18073762
Chicago/Turabian StyleLalla, Francesca, Alessandro Vinciguerra, Alessandra Lissoni, Gianluigi Arrigoni, Francesca Lira Luce, and Silvio Abati. 2021. "Solitary Extramedullary Plasmacytoma Presenting as Asymptomatic Palatal Erythroplakia: Report of a Case" International Journal of Environmental Research and Public Health 18, no. 7: 3762. https://doi.org/10.3390/ijerph18073762