
Effect of Different Exercise Methods on Non-Alcoholic Fatty Liver Disease: A Meta-Analysis and Meta-Regression


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategies
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
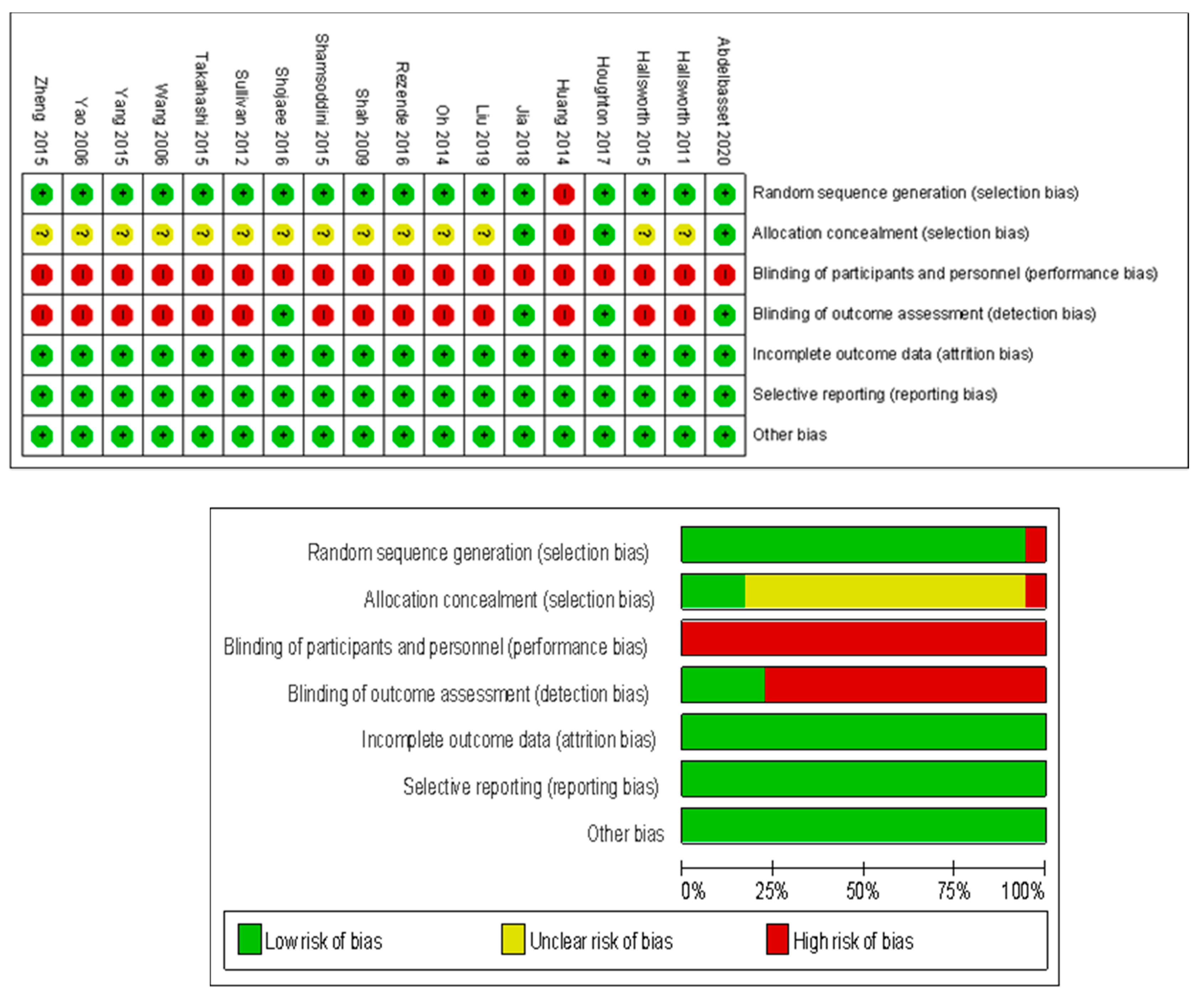
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Literature Retrieval
3.2. Basic Characteristics of Included Studies
3.3. Quality Assessment of Included Studies
3.4. Meta-Analysis and Publication Bias Evaluation
3.4.1. Meta-Analysis and Publication Bias Evaluation of TG
3.4.2. Meta-Analysis and Publication Bias Evaluation of TC
3.4.3. Meta-Analysis and Publication Bias Evaluation of LDL
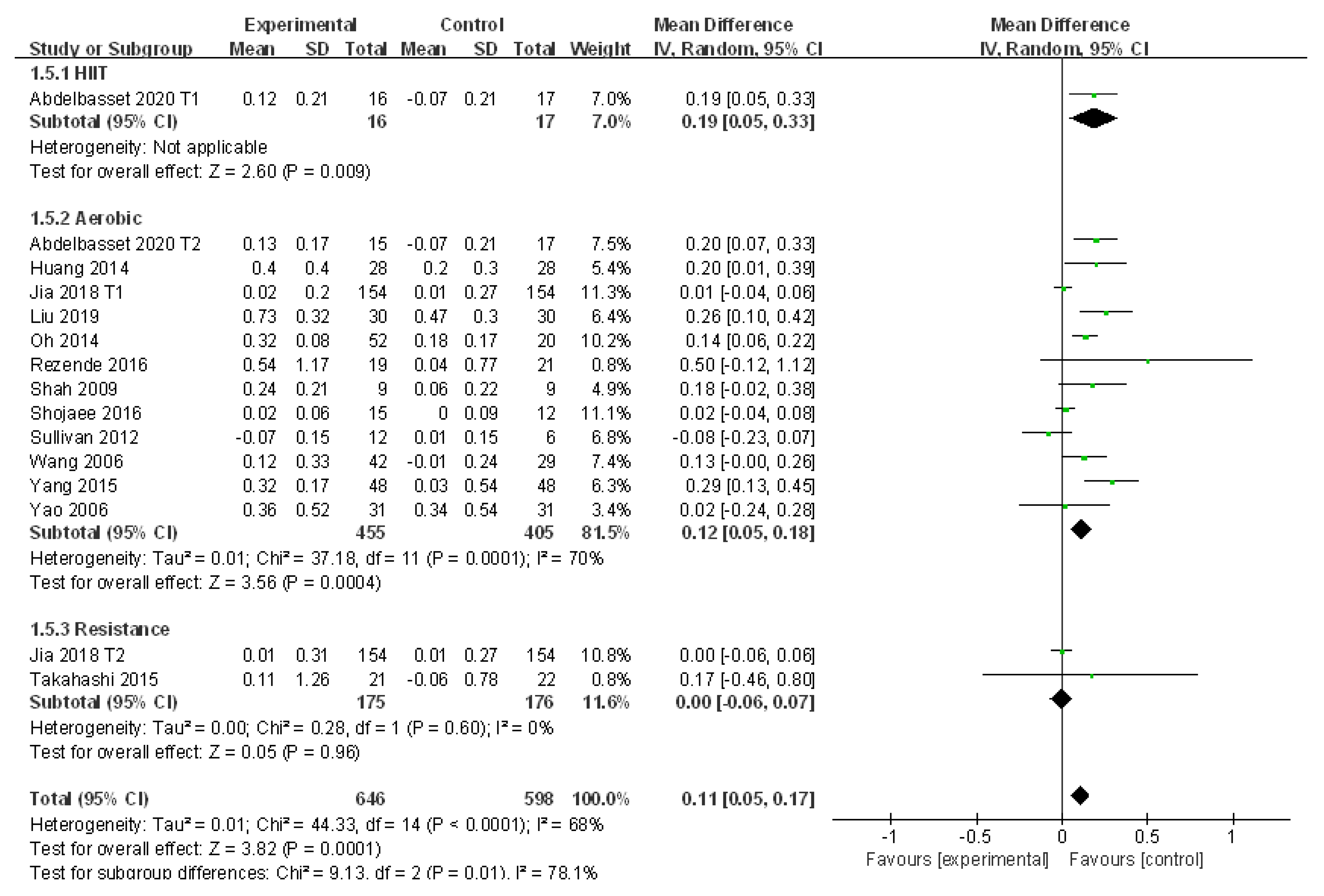
3.4.4. Meta-Analysis and Publication Bias Evaluation of HDL
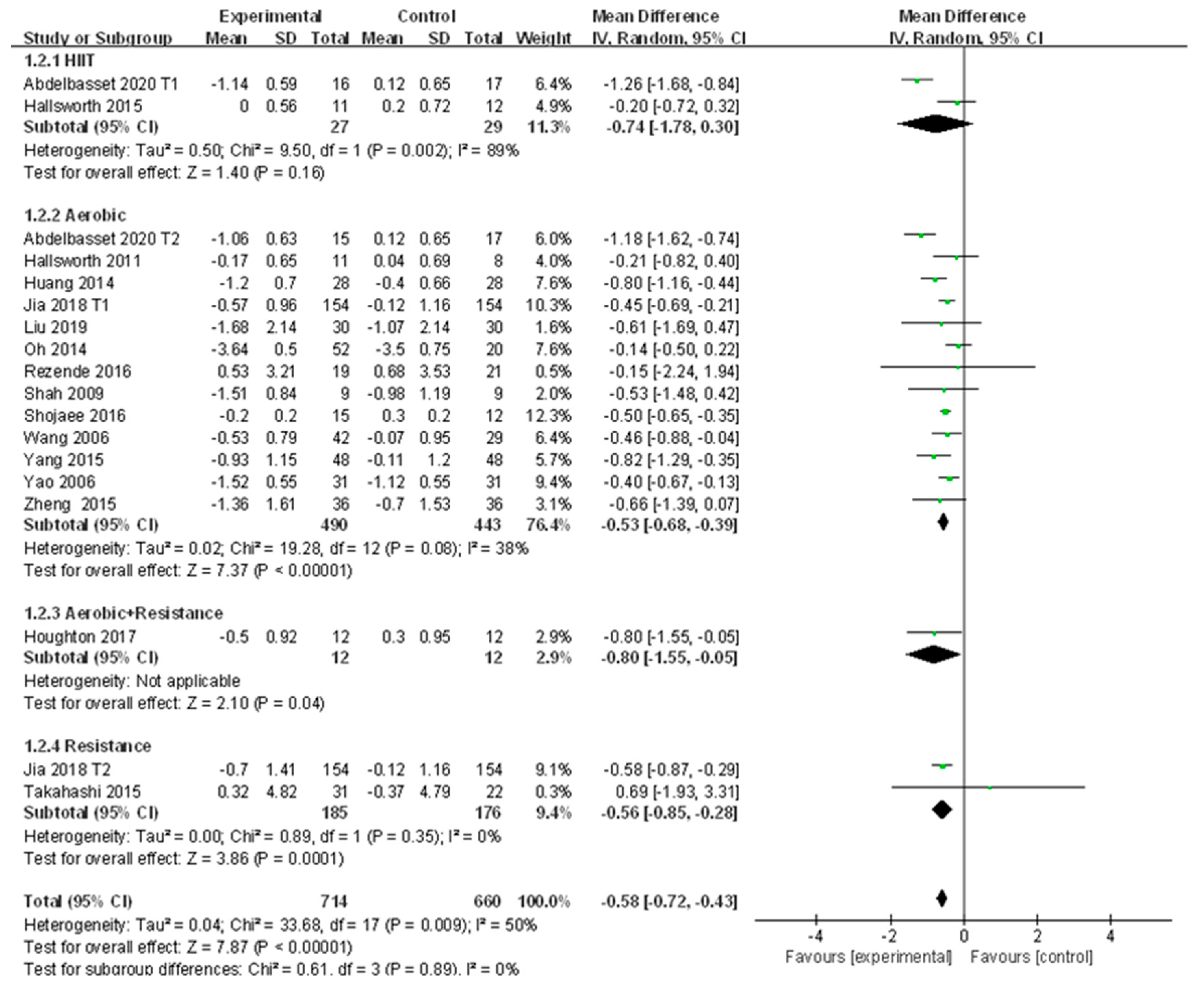
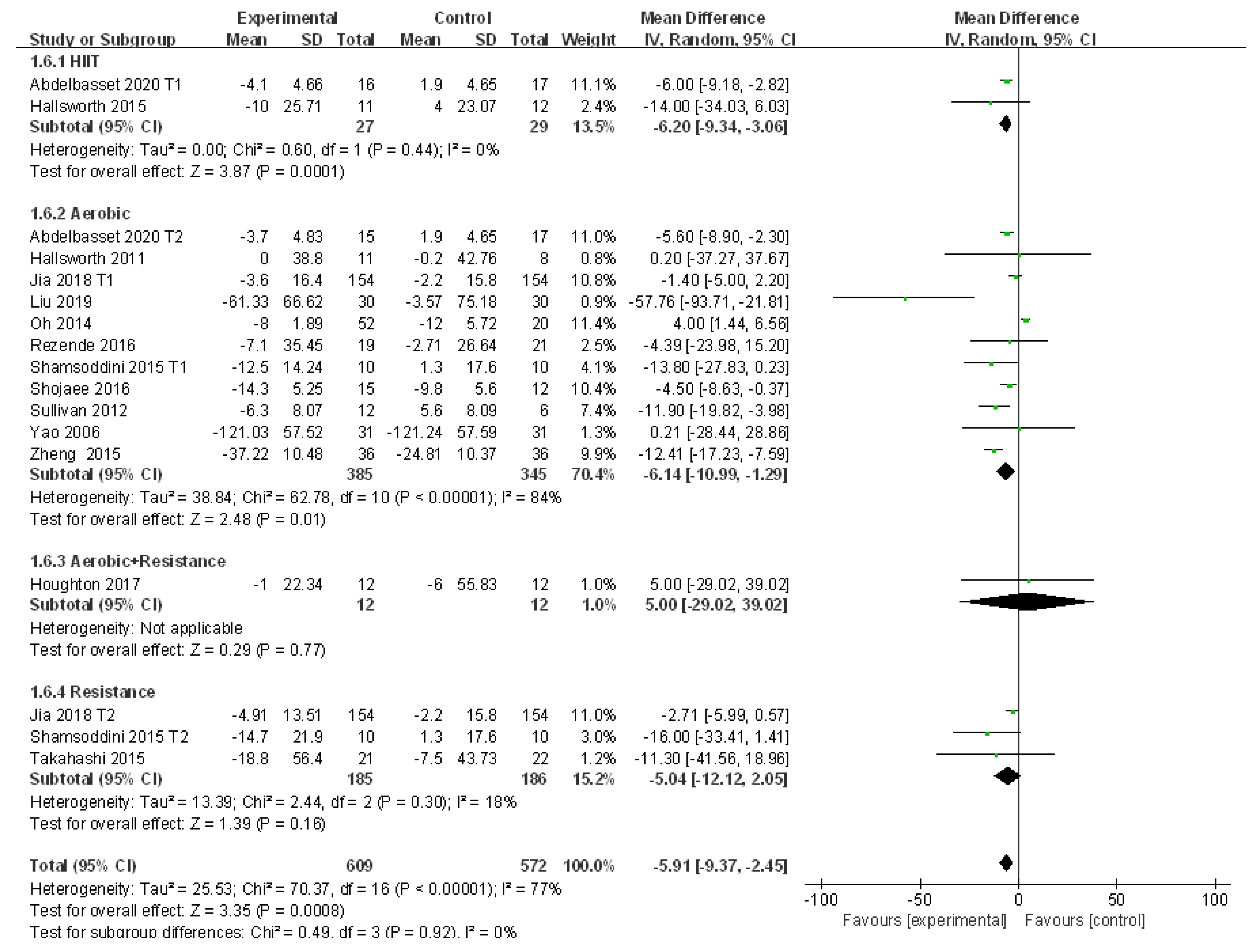
3.4.5. Meta-Analysis and Publication Bias Evaluation of ALT
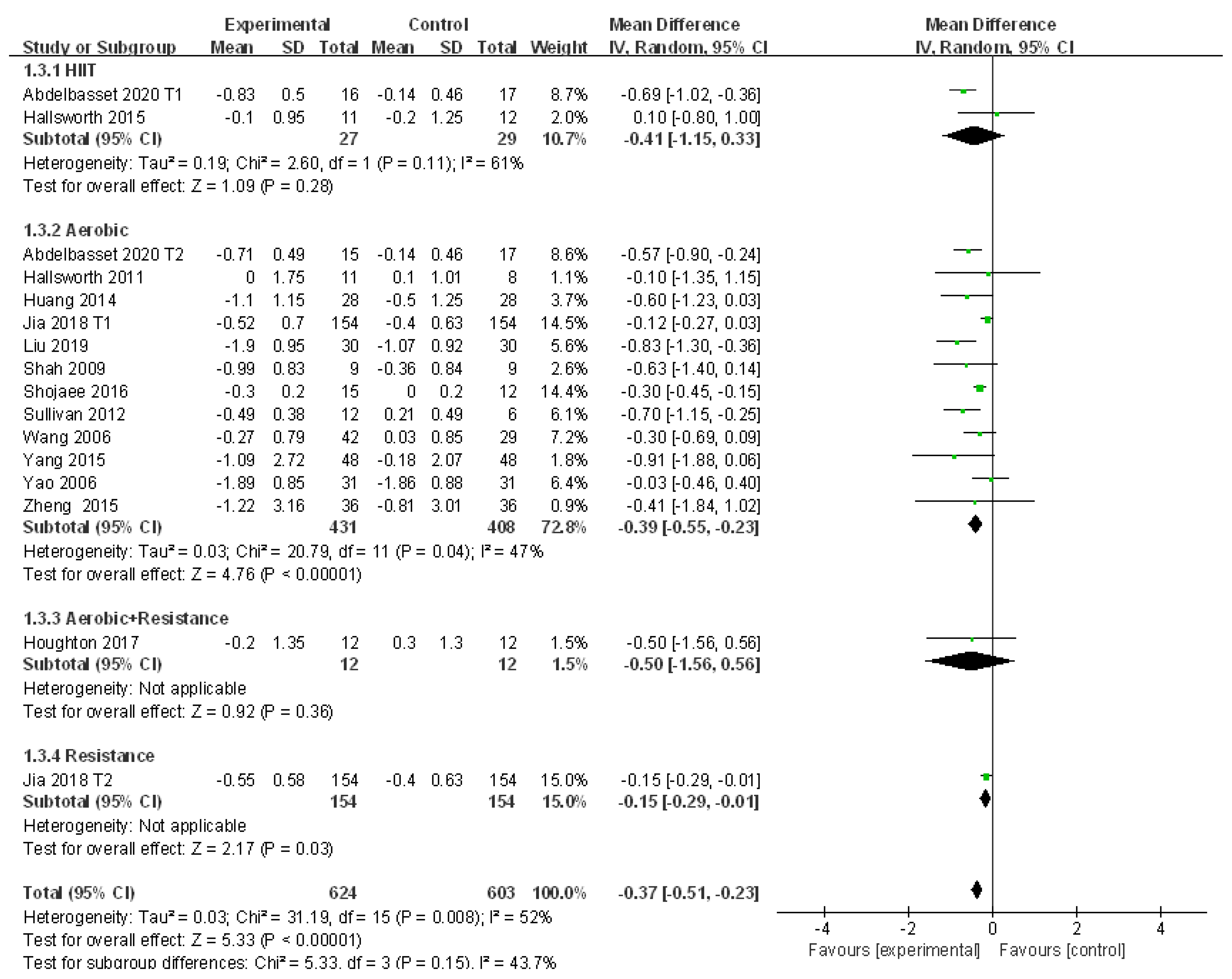
3.4.6. Meta-Analysis and Publication Bias Evaluation of AST
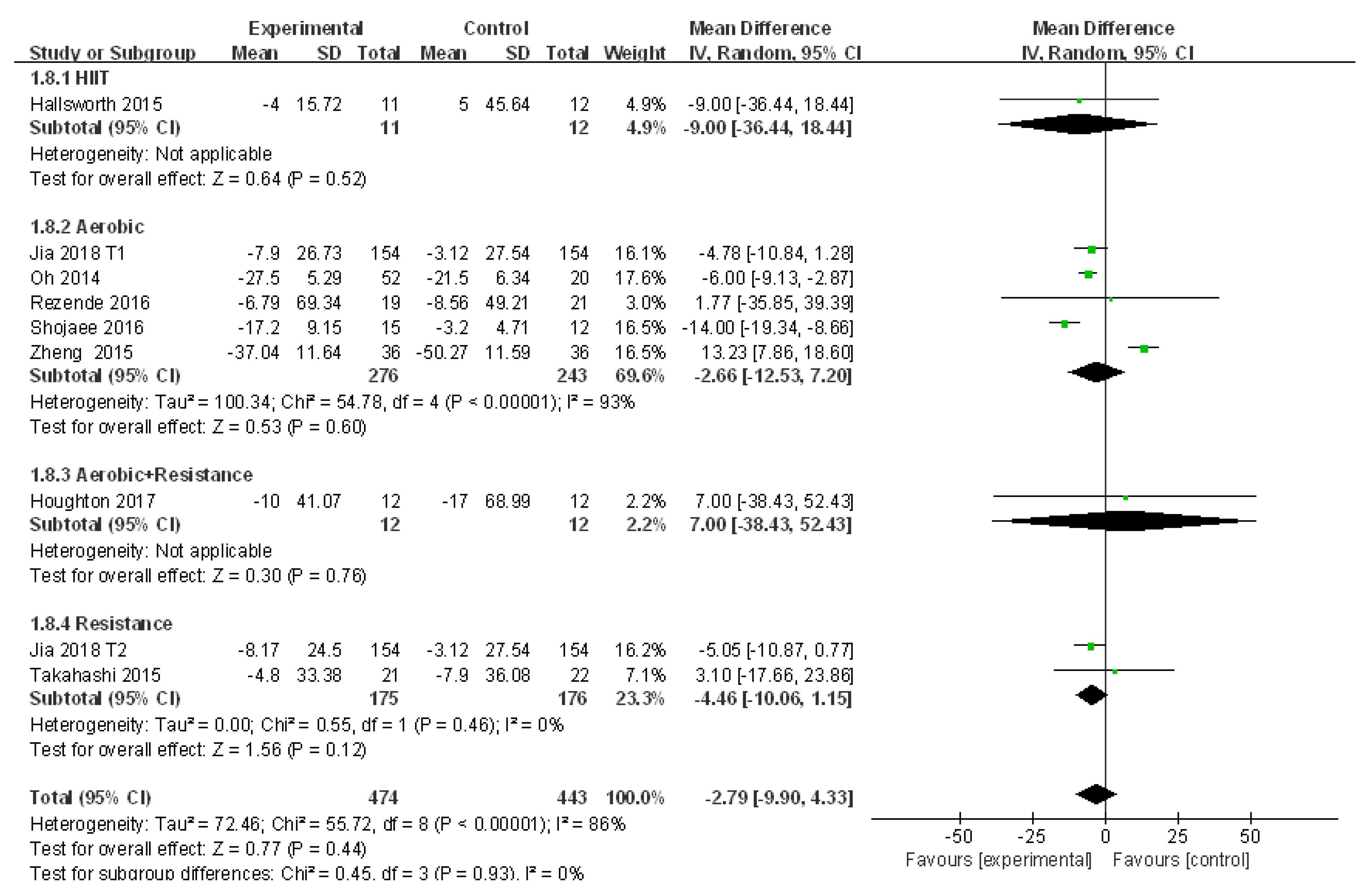
3.4.7. Meta-Analysis and Publication Bias Evaluation of GGT
3.4.8. Meta-Analysis and Publication Bias Evaluation of BMI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thorn, S.R.; Baquero, K.C.; Newsom, S.A.; El Kasmi, K.C.; Bergman, B.C.; Shulman, G.I.; Grove, K.L.; Friedman, J.E. Early Life Exposure to Maternal Insulin Resistance Has Persistent Effects on Hepatic NAFLD in Juvenile Nonhuman Primates. Diabetes 2014, 63, 2702–2713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Del Campo, J.; Gallego-Durán, R.; Gallego, P.; Grande, L. Genetic and Epigenetic Regulation in Nonalcoholic Fatty Liver Disease (NAFLD). Int. J. Mol. Sci. 2018, 19, 911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Zhou, F.; Wang, W.; Zhang, X.; Ji, Y.; Zhang, P.; She, Z.; Zhu, L.; Cai, J.; Li, H. Epidemiological Features of NAFLD From 1999 to 2018 in China. Hepatology 2020, 71, 1851–1864. [Google Scholar] [CrossRef] [PubMed]
- Estes, C.; Anstee, Q.M.; Arias-Loste, M.T.; Bantel, H.; Bellentani, S.; Caballeria, J.; Colombo, M.; Craxi, A.; Crespo, J.; Day, C.P.; et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J. Hepatol. 2018, 69, 896–904. [Google Scholar] [CrossRef]
- Shu, J.R.; Li, A.Q.; Liu, Q. Epidemiology of nonalcoholic fatty liver disease and related risk factors. J. Clin. Hepatol. 2019, 35, 2085–2090. [Google Scholar]
- Chalasani, N.; Younossi, Z.; LaVine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.C.; Jia, W. Research progress of exercise prescription for nonalcoholic fatty liver disease. Occup. Health 2020, 36, 569–572. [Google Scholar]
- Keating, S.E.; Hackett, D.A.; George, J.; Johnson, N.A. Exercise and non-alcoholic fatty liver disease: A systematic review and meta-analysis. J. Hepatol. 2012, 57, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Hallsworth, K.; Thoma, C.; Hollingsworth, K.G.; Cassidy, S.; Anstee, Q.M.; Day, C.P.; Trenell, M.I. Modified high-intensity interval training reduces liver fat and improves cardiac function in non-alcoholic fatty liver disease: A randomized controlled trial. Clin. Sci. 2015, 129, 1097–1105. [Google Scholar] [CrossRef]
- Oh, S.; Tanaka, K.; Tsujimoto, T.; So, R.; Shida, T.; Shoda, J. Regular Exercise Coupled to Diet Regimen Accelerates Reduction of Hepatic Steatosis and Associated Pathological Conditions in Nonalcoholic Fatty Liver Disease. Metab. Syndr. Relat. Disord. 2014, 12, 290–298. [Google Scholar] [CrossRef]
- Abdel Basset, W.K.; Tantawy, S.A.; Kamel, D.M.; Alqahtani, B.A.; Elnegamy, T.E.; Soliman, G.S.; Ibrahim, A.A. Effects of high-intensity interval and moderate-intensity continuous aerobic exercise on diabetic obese patients with nonalcoholic fatty liver disease. Medicine 2020, 99, e19471. [Google Scholar] [CrossRef]
- Jia, G.Y.; Han, T.; Gao, L.; Wang, L.; Wang, S.C.; Yang, L.; Zhang, J.; Guan, Y.Y.; Yan, N.N.; Yu, H.Y.; et al. Effect of aerobic exercise and resistance exercise in hnproving non-alcoholic fatty fiver disease: A randomized controlled trial. Chin. J. Hepatol. 2018, 26, 34–41. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Updated Guidance for Trusted Systematic Reviews: A New Edition of the Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Database of Systematic Reviews; John Wiley & Sons: Oxford, UK, 2019; Volume 10, p. ED000142. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Hallsworth, K.; Fattakhova, G.; Hollingsworth, K.G.; Thoma, C.; Moore, S.; Taylor, R.; Day, C.P.; I Trenell, M. Resistance exercise reduces liver fat and its mediators in non-alcoholic fatty liver disease independent of weight loss. Gut 2011, 60, 1278–1283. [Google Scholar] [CrossRef]
- Rezende, R.E.; Duarte, S.M.; Stefano, J.T.; Roschel, H.; Gualano, B.; Pinto, A.L.D.S.; Vezozzo, D.C.; Carrilho, F.J.; Oliveira, C.P. Randomized clinical trial: Benefits of aerobic physical activity for 24 weeks in postmenopausal women with nonalcoholic fatty liver disease. Menopause 2016, 23, 876–883. [Google Scholar] [CrossRef]
- Shah, K.; Stufflebam, A.; Hilton, T.N.; Sinacore, D.R.; Klein, S.; Villareal, D.T. Diet and Exercise Interventions Reduce Intrahepatic Fat Content and Improve Insulin Sensitivity in Obese Older Adults. Obesity 2009, 17, 2162–2168. [Google Scholar] [CrossRef] [Green Version]
- Shamsoddini, A.; Sobhani, V.; Chehreh, M.E.G.; Alavian, S.M.; Zaree, A. Effect of Aerobic and Resistance Exercise Training on Liver Enzymes and Hepatic Fat in Iranian Men with Nonalcoholic Fatty Liver Disease. Zahedan J. Res. Med Sci. 2015, 15, e31434. [Google Scholar] [CrossRef] [Green Version]
- Shojaee-Moradie, F.; Cuthbertson, D.J.; Barrett, M.; Jackson, N.C.; Herring, R.; Thomas, E.L.; Bell, J.; Kemp, G.J.; Wright, J.; Umpleby, A.M. Exercise Training Reduces Liver Fat and Increases Rates of VLDL Clearance but not VLDL Production in NAFLD. J. Clin. Endocrinol. Metab. 2016, 101, 4219–4228. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, S.; Kirk, E.P.; Mittendorfer, B.; Patterson, B.W.; Klein, S. Randomized trial of exercise effect on intrahepatic triglyceride content and lipid kinetics in nonalcoholic fatty liver disease. Hepatology 2011, 55, 1738–1745. [Google Scholar] [CrossRef] [Green Version]
- Huang, K.; Lu, H.Y.; Yang, J.Q. Exercise therapy combined with dietary regulation on fatty liver effect of lowering blood pressure and regulating lipid in patients with hypertension. Chin. Hepatol. 2014, 19, 525–527. [Google Scholar]
- Liu, F. Effects of aerobic exercise on liver function and blood lipids in patients with non-alcoholic fatty liver effect analysis. Chin. Foreign Med Res. 2019, 17, 147–148. [Google Scholar] [CrossRef]
- Wang, Y. Intervention Effects of Aerobic Exercise on Nonalcoholic Fatty Liver Disease; Beijing Sport University: Beijing, China, 2006. [Google Scholar]
- Yang, Y.H.; Wang, F.L.; Mao, J.J. Comprehensive exploration on the effectiveness of aerobic exercise for patients with non-alcoholic fatty liver. Mod. Pract. Med. 2015, 27, 1055–1057. [Google Scholar] [CrossRef]
- Yao, Z.L.; Zhu, C.C.; Wan, X.Q. Clinical research of Xuezhikang joint sport in treatment of steatohepatitis who had symptom. China J. Mod. Med. 2006, 16, 253–256. [Google Scholar] [CrossRef]
- Zheng, Y.C.; Chen, L.; Lu, F.L.; Yan, Q.Q. Observation of the clinical effect of exercise therapy on non-alcoholic fatty liver. Chin. Hepatol. 2015, 20, 51–53. [Google Scholar]
- Houghton, D.; Thoma, C.; Hallsworth, K.; Cassidy, S.; Hardy, T.; Burt, A.D.; Tiniakos, D.; Hollingsworth, K.G.; Taylor, R.; Day, C.P.; et al. Exercise Reduces Liver Lipids and Visceral Adiposity in Patients With Nonalcoholic Steatohepatitis in a Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2017, 15, 96–102.e3. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, A.; Abe, K.; Usami, K.; Imaizumi, H.; Hayashi, M.; Okai, K.; Kanno, Y.; Tanji, N.; Watanabe, H.; Ohira, H. Simple Resistance Exercise helps Patients with Non-alcoholic Fatty Liver Disease. Int. J. Sports Med. 2015, 36, 848–852. [Google Scholar] [CrossRef] [PubMed]
- Orci, L.A.; Gariani, K.; Oldani, G.; Delaune, V.; Morel, P.; Toso, C. Exercise-based Interventions for Nonalcoholic Fatty Liver Disease: A Meta-analysis and Meta-regression. Clin. Gastroenterol. Hepatol. 2016, 14, 1398–1411. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.T.; Zheng, J.; Peng, H.W.; Cai, X.L.; Pan, X.T.; Li, H.Q.; Hong, Q.Z.; Peng, X.E. Physical activity intervention for non-diabetic patients with non-alcoholic fatty liver disease: A meta-analysis of randomized controlled trials. BMC Gastroenterol. 2020, 20, 66. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Mou, Z.Y.; Zhai, J.X.; Zong, H.X.; Zhao, X.D. Study on stata software in investigating publication bias in meta-analysis. Mod. Prev. Med. 2009, 9, 1115–1118. [Google Scholar]
- Abdelbasset, W.K.; Tantawy, S.A.; Kamel, D.M.; Alqahtani, B.A.; Soliman, G.S. A randomized controlled trial on the effectiveness of 8-week high-intensity interval exercise on intrahepatic triglycerides, visceral lipids, and health-related quality of life in diabetic obese patients with nonalcoholic fatty liver disease. Medicine 2019, 98, e14918. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, B.; Schrauwen-Hinderling, V.B.; Jelenik, T.; Gemmink, A.; Sparks, L.M.; Havekes, B.; Bruls, Y.; Dahlmans, D.; Roden, M.; Hesselink, M.K.; et al. Exercise training reduces intrahepatic lipid content in people with and people without nonalcoholic fatty liver. Am. J. Physiol. Metab. 2018, 314, E165–E173. [Google Scholar] [CrossRef]
- Takahashi, H.; Kotani, K.; Tanaka, K.; Egucih, Y.; Anzai, K. Therapeutic Approaches to Nonalcoholic Fatty Liver Disease: Exercise Intervention and Related Mechanisms. Front. Endocrinol. 2018, 9, 9. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Research Object | Intervention | Diet | Drug | Outcomes | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Participants | Gender (m/f) | Age | Exercise Type | Intensity | Duration (min) | Frequency (n/week) | Duration (week) | |||||
| Abdelbasset | 2020 | T1 16 | 10/6 | 54.4 ± 5.8 | HIIT | 80–85% VO2max | 40 | 3 | 8 | ①②③④⑤⑥ | ||
| T2 15 | 8/7 | 54.9 ± 4.7 | Aerobic | 60–70% VO2max | 40–50 | 3 | 8 | |||||
| C 16 | 9/7 | 55.2 ± 4.3 | No exercise | |||||||||
| Hallsworth | 2011 | T 11 | Aerobic | 60% HRM | 45–60 | 3 | 8 | ①②③⑥ | ||||
| C 8 | No exercise | |||||||||||
| Hallsworth | 2015 | T 11 | 11/0 | 54 ± 10 | HIIT | 30–40 | 3 | 12 | ①②③⑥⑦⑧ | |||
| C 12 | 12/0 | 52 ± 12 | No exercise | |||||||||
| Houghton | 2017 | T 12 | 12/0 | 54 ± 12 | Aerobic + Resistance | 45–60 | 3 | 12 | ①②③⑥⑦⑧ | |||
| C 12 | 12/0 | 51 ± 16 | No exercise | |||||||||
| Huang | 2014 | T 28 | Aerobic | 5 | 24 | Diet | ②③④⑤ | |||||
| C 28 | No exercise | |||||||||||
| Jia | 2018 | T1 154 | 78/76 | 54.6 + 7.5 | Aerobic | 50–70% HRM | 45 | 3 | 24 | ①②③④⑤⑥⑦⑧ | ||
| T2 154 | 78/76 | 55.1 ± 7.4 | Resistance | |||||||||
| C 154 | 75/79 | 54.2 + 7.5 | No exercise | |||||||||
| Liu | 2019 | T 30 | 12/18 | 60.5 ± 8.5 | Aerobic | 60 | 4 | 16 | ②③④⑤⑥ | |||
| C 30 | 17/13 | 61.5 ± 8.2 | No exercise | |||||||||
| Oh | 2014 | T 52 | 52/0 | 49.1 ± 1.3 | Aerobic | >40% HRM | 90 | 3 | 12 | Diet | ②④⑤⑥⑦⑧ | |
| C 20 | 20/0 | 53.2 ± 2.1 | No exercise | |||||||||
| Rezende | 2016 | T 19 | 19/0 | 56.2 ± 7.8 | Aerobic | 30–50 | 2 | 24 | ①②④⑤⑥⑦⑧ | |||
| C 21 | 21/0 | 54.5 ± 8.9 | No exercise | |||||||||
| Shah | 2009 | T 9 | 2/7 | 68.5 ± 1.3 | Aerobic | 90 | 3 | 24 | Diet | ②③④⑤ | ||
| C 9 | 3/6 | 68.6 ± 1.1 | No exercise | |||||||||
| Shamsoddini | 2015 | T1 10 | 10/0 | 39.7 ± 6.3 | Aerobic | 60% HRM | 45 | 3 | 8 | ①⑥⑦ | ||
| T2 10 | 10/0 | 45.9 ± 7.3 | Resistance | 45 | ||||||||
| C 10 | 10/0 | 45.8 ± 7.3 | No exercise | |||||||||
| Shojaee | 2016 | T 15 | 15/0 | 52.4 ± 2.2 | Aerobic | 40–60% HRM | 60 | 4 | 16 | ①②③④⑤⑥⑦⑧ | ||
| C 12 | 12/0 | 52.8 ± 3.0 | No exercise | |||||||||
| Sullivan | 2012 | T 12 | 4/8 | 48.6 ± 2.2 | Aerobic | 45–55% HRM | 30–60 | 5 | 16 | ①②③④⑤⑥ | ||
| C 6 | 1/5 | 47.5 ± 3.1 | No exercise | |||||||||
| Takahashi | 2015 | T 31 | 9/22 | 55.5 ± 13.2 | Resistance | 20–30 | 3 | 12 | ①②④⑤⑥⑦⑧ | |||
| C 32 | 10/12 | 51.4 ± 14.8 | No exercise | |||||||||
| Wang | 2006 | T 32 | 14/28 | 51.9 ± 7.7 | Aerobic | 60 | 3 | 12 | Drug | ①②③④⑤ | ||
| C 29 | 11/18 | 49.2 ± 8.7 | No exercise | |||||||||
| Yang | 2015 | T 48 | 41/7 | 47.1 ± 3.9 | Aerobic | 60 | 3 | 24 | ①②③④⑤ | |||
| C 48 | 42/6 | 48.4 ± 4.8 | No exercise | |||||||||
| Yao | 2006 | T 31 | Aerobic | 40 | 7 | 12 | Drug | ②③⑤⑥⑦ | ||||
| C 31 | No exercise | |||||||||||
| Zheng | 2015 | T 36 | 22/14 | 42.3 ± 10.3 | Aerobic | 60–75% HRM | 40–90 | 4 | 24 | Drug | ①②③④⑥⑦⑧ | |
| C 36 | 22/14 | 43.2 ± 9.5 | No exercise | |||||||||
| Research Factors | Regression Coefficients | 95% CI | t | p |
|---|---|---|---|---|
| publication year | −0.066 | −0.128~−0.003 | −2.29 | 0.041 |
| sample size | 0.001 | −0.001~0.004 | 1.25 | 0.234 |
| intervention time | −0.009 | −0.046~0.028 | −0.55 | 0.596 |
| diet | −0.002 | −0.061~0.057 | −0.07 | 0.942 |
| medication | 0.031 | −0.043~0.104 | 0.91 | 0.380 |
| Research Factors | Regression Coefficients | 95%CI | t | p |
|---|---|---|---|---|
| publication year | −0.046 | −0.092~−0.001 | −2.28 | 0.045 |
| sample size | 0.002 | −0.000~0.003 | 1.83 | 0.096 |
| intervention time | −0.006 | −0.047~0.035 | −0.35 | 0.735 |
| diet | 0.037 | −0.044~0.118 | 1.02 | 0.330 |
| medication | 0.023 | −0.027~0.074 | 1.02 | 0.332 |
| Research Factors | Regression Coefficients | 95%CI | t | p |
|---|---|---|---|---|
| publication year | −0.047 | −0.112~−0.019 | −1.62 | 0.139 |
| sample size | 0.001 | −0.000~0.002 | 1.40 | 0.194 |
| intervention time | −0.014 | −0.039~0.011 | −1.25 | 0.244 |
| diet | 0.091 | −0.057~0.124 | 6.18 | 0.000 |
| medication | 0.021 | −0.024~0.066 | 1.06 | 0.318 |
| Research Factors | Regression Coefficients | 95% CI | t | p |
|---|---|---|---|---|
| publication year | 0.024 | −0.001~−0.048 | 2.20 | 0.055 |
| sample size | −0.001 | −0.002~0.000 | −2.01 | 0.076 |
| intervention time | 0.007 | −0.007~0.022 | 1.11 | 0.297 |
| diet | −0.013 | −0.033~0.006 | −1.54 | 0.159 |
| medication | 0.021 | −0.024~0.066 | −1.23 | 0.249 |
| Research Factors | Regression Coefficients | 95% CI | t | p |
|---|---|---|---|---|
| publication year | 0.612 | −0.754~−1.979 | 0.99 | 0.345 |
| sample size | −0.000 | −0.043~0.043 | 0.00 | 1.000 |
| intervention time | 0.319 | −0.548~1.186 | 0.81 | 0.435 |
| diet | −1.375 | −2.172~−0.577 | −3.79 | 0.003 |
| medication | 0.962 | −0.034~1.959 | 2.13 | 0.057 |
| Research Factors | Regression Coefficients | 95%CI | t | p |
|---|---|---|---|---|
| publication year | −2.941 | −5.084~−0.798 | −3.36 | 0.015 |
| sample size | 0.013 | −0.014~0.040 | 1.19 | 0.278 |
| intervention time | 0.633 | −0.428~1.693 | 1.46 | 0.195 |
| diet | 0.307 | −0.141~−0.754 | 1.68 | 0.144 |
| medication | 2.574 | −1.162~3.987 | 4.46 | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiong, Y.; Peng, Q.; Cao, C.; Xu, Z.; Zhang, B. Effect of Different Exercise Methods on Non-Alcoholic Fatty Liver Disease: A Meta-Analysis and Meta-Regression. Int. J. Environ. Res. Public Health 2021, 18, 3242. https://doi.org/10.3390/ijerph18063242
Xiong Y, Peng Q, Cao C, Xu Z, Zhang B. Effect of Different Exercise Methods on Non-Alcoholic Fatty Liver Disease: A Meta-Analysis and Meta-Regression. International Journal of Environmental Research and Public Health. 2021; 18(6):3242. https://doi.org/10.3390/ijerph18063242
Chicago/Turabian StyleXiong, Yingzhe, Qingwen Peng, Chunmei Cao, Zujie Xu, and Bing Zhang. 2021. "Effect of Different Exercise Methods on Non-Alcoholic Fatty Liver Disease: A Meta-Analysis and Meta-Regression" International Journal of Environmental Research and Public Health 18, no. 6: 3242. https://doi.org/10.3390/ijerph18063242